Introduction
Hepatocellular carcinoma (HCC) is the fifth most
common cancer and the third leading cause of cancer-related death
worldwide (1). HCC is more common in
Asia and Africa compared with western countries (2,3).
However, incidence rates of HCC in western countries have been
gradually increasing in recent years (3,4).
HCC is treated by surgical resection (RES),
radiofrequency ablation (RFA), liver transplantation, as well as
other methods. Currently, the most effective treatment option for
patients with HCC is a liver transplant; however, due to the lack
of available donors, this method is not widely used (5). As a consequence, RES is considered to
be the most popular treatment strategy for patients with resectable
tumors and good liver function (a Child-Pugh score of A or B)
(6–8). However, only 9–29% of patients with HCC
are able to tolerate surgery, either due to poor hepatic reserves
as a result of potential chronic liver disease, or due to the
multifocal distribution of tumor nodules (9–16).
RFA has been demonstrated to be safe and effective
for the treatment of patients with tumors <3 cm in size. In
addition, RFA is associated with lower mortality rates and shorter
hospital stays (17–20). However, only a small number of
randomized controlled trials (RCTs) comparing the effectiveness of
RFA and RES have been performed (21–23), and
the results are contradictory. In addition, the value of these RCTs
is limited due to a small number of samples analyzed and the wide
confidence intervals (CIs). A number of studies have concluded that
RFA is as effective as RES in the treatment of solitary and small
HCC tumors (21,24–29).
Livraghi et al (29) even
regarded RFA as the preferable treatment for small, resectable HCC
tumors (tumor size, ≤2 cm). By contrast, other studies arrived at
the opposite conclusion (18,30,31).
RES may improve long-term disease-free survival (DFS) rates, and
potentially increase overall survival (OS) rates, when compared
with RFA in a subgroup of patients with single HCC tumors >2 cm
in size and with Child-Pugh class A liver function scores. The
conflicting results of these previous studies are primarily
considered to be related to the relatively small sample sizes.
Similarly, previously published reviews and meta-analyses present
contradictory results. A number of these studies concluded that no
significant difference in death rates following treatment of HCC
using RES and RFA was observed, if disease recurrence following RFA
was detected in a timely manner and effectively treated (32,33).
However, the opposite conclusions have been drawn in other review
studies (17,34). In these studies, it was argued that
RFA did not decrease the number of overall recurrences and had no
effect on patient survival when compared with RES in a selected
group of patients. In addition, RES was superior to RFA with
regards to overall or recurrence-free survival. The contradictory
results from these studies may be due to inconsistencies between
the subjects recruited, therapeutic techniques employed and the
evaluation criteria. However, a recent systematic review concluded
that the indication for RFA as a primary treatment for patients
with early stage HCC that are eligible for RES is unclear, and
additional well-designed RCTs are required (35). Ultimately, due to the small number of
RCTs performed thus far, the heterogeneity of different studies and
the inherent limitations of meta-analyses, it is currently unclear
whether RFA or RES is more effective for the treatment of patients
with resectable HCC. Strong evidence is required to compare RFA and
RES treatment strategies. Therefore, the aim of the present study
was to conduct a meta-analysis of 13,147 patients with HCC to
compare the therapeutic effects of RFA and RES.
Materials and methods
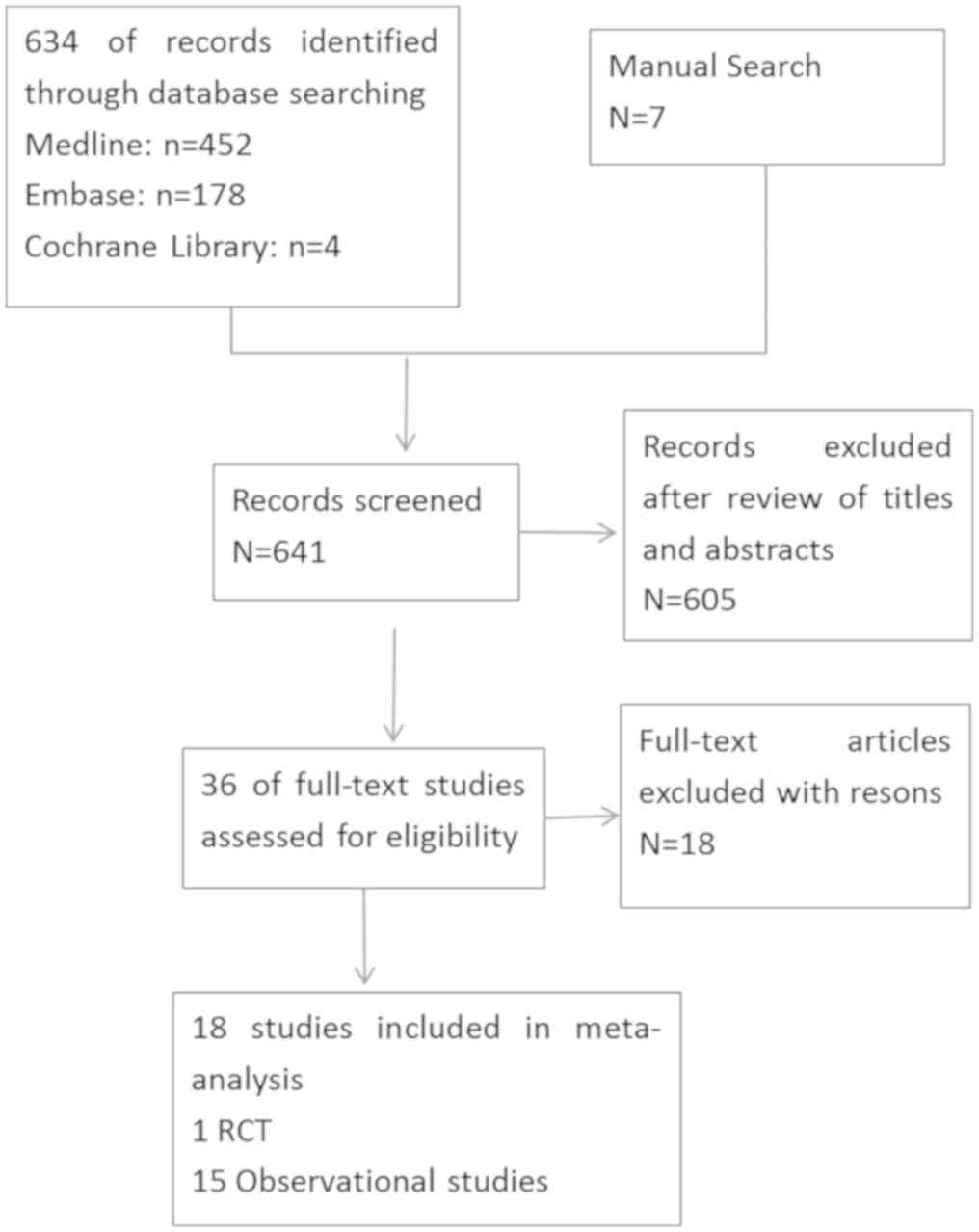
Literature search
A Medline, Embase, and Cochrane Library search was
performed for data published between January 2000 and February
2018. The following keywords were used as search criteria: ‘RFA,
radio-frequency, radio frequency or RFA’ AND ‘RES or hepatectomy’
AND ‘liver or hepatic or HCC’ with no language restrictions.
Additional studies were identified by manual searching of the
references by two reviewers.
Study selection criteria
The following selection criteria for studies were
applied: i) Those that included patients with no previous treatment
for HCC; ii) those that included patients suitable for treatment
with either RES or RFA (based on the Milan Criteria) and with liver
function Child-Pugh scores of grade A or B; iii) results for at
least one of the outcome measures, including the 1-, 3- and 5-year
OS or DFS rates; and iv) studies published in peer-reviewed
journals.
Data extraction
Data was extracted independently by two observers
and cross-checked to reach a consensus. The following parameters
were recorded: Author; journal; date of publication; geographical
region; number of patients; age; sex; liver function; tumor size;
Child-Pugh class; number of tumors; death rates; 1-, 3- and 5-year
OS rates; and 1-, 3- and 5-year DFS rates. The primary authors were
contacted to retrieve further information where necessary.
Quality assessment
The quality of the RCTs were assessed using the
Jadad Scoring system (36) and the
quality of observational studies was assessed using the
Newcastle-Ottawa Scale (NOS) (37).
Although the majority of studies included were observational
studies, these studies had high NOS scores (≥5*) and were found to
be important for directing clinical work.
Data analysis
A meta-analysis was performed according to the
recommendations of the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses guidelines. The analysis was conducted
using the STATA 12.0 statistical software and Review Manager
Version 5.1. For statistical analysis of the pooled odds ratio (OR)
for categorical variables, which correspond to the odds of an event
occurring in the treatment group (RFA), compared to the control
group (RES) was used. An OR of >1 indicates that the probability
of an outcome is more likely to occur in the treatment group, and
is considered statistically significant when P<0.05 and the 95%
CI does not include the value 1. The Mantel-Haenszel method was
used to combine the ORs for outcomes of interest to the present
study. A random-effects model, that is more robust in terms of
anticipated heterogeneity in patient and hospital-related risk
factors, was used for the meta-analysis due to the considerable
clinical heterogeneity of surgical procedures and study designs
(38,39). However, the statistical heterogeneity
in each meta-analysis was assessed using the τ2,
χ2 and I2 statistics parameters.
Heterogeneity was regarded as significant if τ2 was
>0 and if either the P-value of χ2 analysis was
<0.10 or the I2 vale was >50%. Subgroup analyses
included: i) A mean tumor size of ≤3 cm and (ii) a mean tumor size
of >3 cm.
Results
Description of the studies
Out of the 13,147 patients with HCC across 25
studies included in the current study, 6,727 were allocated to the
RFA group and 6,420 were allocated to the RES group in order to
evaluate the therapeutic effects of these treatment modalities. The
selected studies included three RCTs and 20 observational
comparative studies. The overlap in time of patients was detected
in two trials (22,40) and the non-randomly controlled trial
was excluded (40). Two trials
(21,41) were thought to have overlapping data,
as they were conducted in the same center (21); one was an RCT that recruited patients
with solitary HCC tumors ≤5 cm in diameter between November 1999
and June 2004, while the other (41)
was a retrospective study that analyzed patient data collected
between December 2003 to December 2008. As a result, only the RCT
was included in the current study (Fig.
1). Data from patients presenting with a mean tumor size of
<3 and >3 cm were divided into the subgroup analysis whenever
the author presented them independently in the study.
Outcome measures
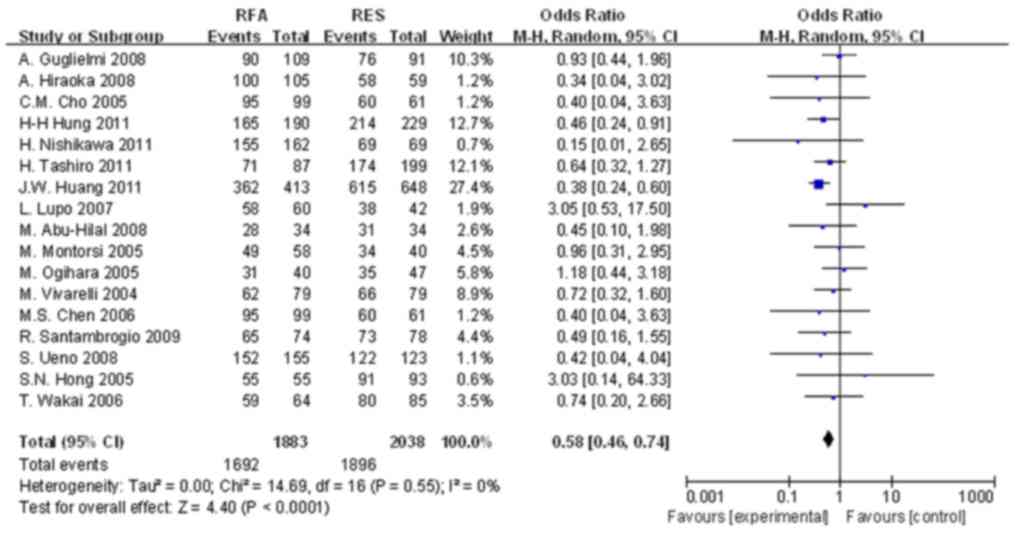
OS rates
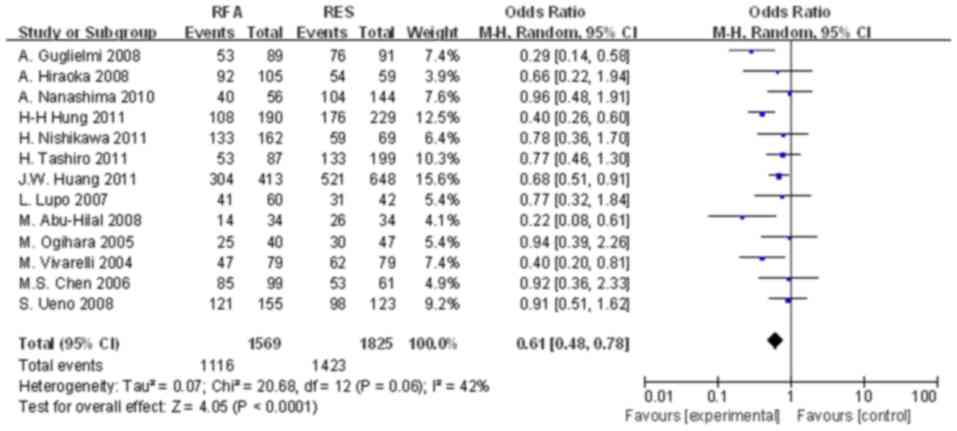
The meta-analysis results demonstrated a significant
difference in the 1-, 3- and 5-year OS rates between the two
groups. The OR of 1-year OS rates of the two groups was 0.757 (95%
CI, 0.578–0.989; P=0.042; Fig. 2).
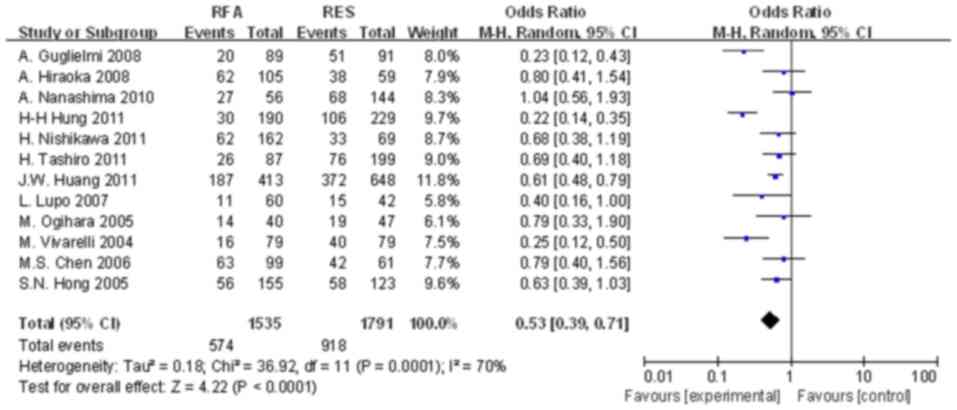
For the 3-year OS rates, the OR of the two groups was 0.530 (95%
CI, 0.401–0.700; P<0.001; Fig.
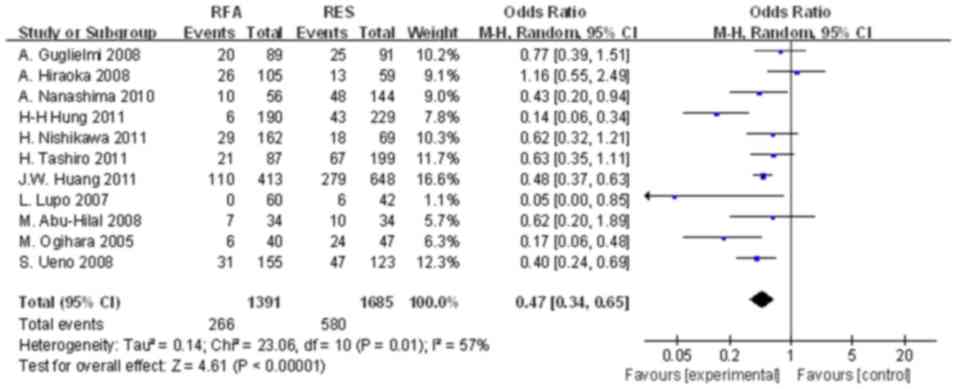
3). Finally, the OR of 5-year OS rates in the two groups was
0.566 (95% CI, 0.423–0.758; P=0.001; Fig. 4).
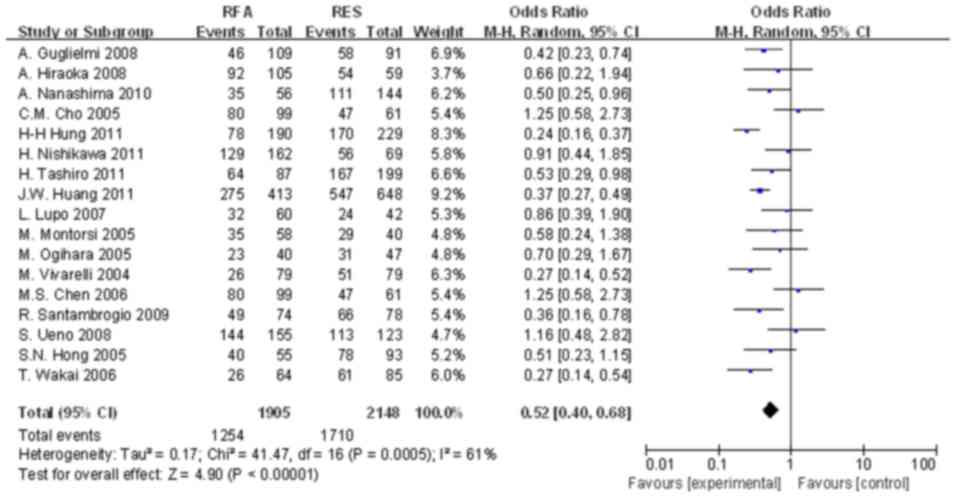
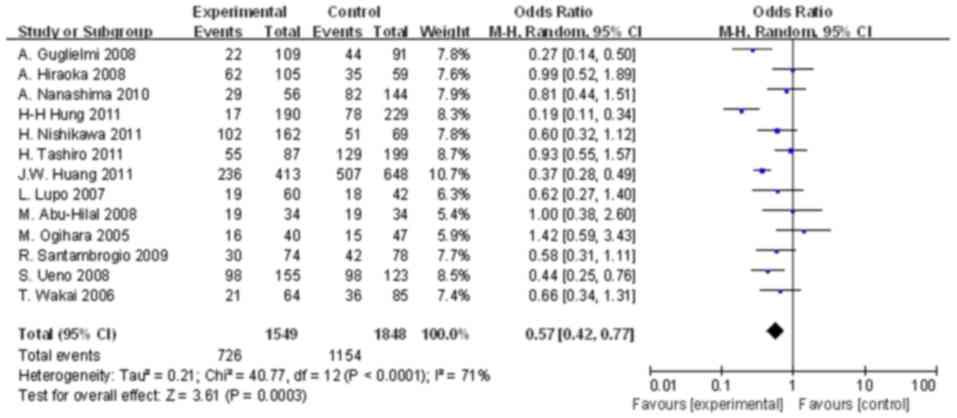
DFS rates
The results of the meta-analysis demonstrated a
significant difference in the 1-, 3- and 5-year DFS rates between
the two groups. As indicated in Fig.
5, the OR of 1-year DFS in the two groups was 0.569 (95% CI,
0.456–0.711; P<0.001). The ORs of the 3- and 5-year DFS rates
between the two groups were 0.418 (95% CI, 0.267–0.653; P<0.001)
and 0.374 (95% CI, 0.231–0.606; P<0.001), respectively (Figs. 6 and 7).
Subgroup analysis
Subgroup of mean tumor size ≤3 cm
The 3- and 5-year OS rates and the 1-, 3- and 5-year
DFS rates of the RES group of patients with HCC were significantly
higher than those of the RFA group. The 1-year OS rate of patients
in the RES group was not significantly higher than that of the RFA
group.
Subgroup of mean tumor size >3
cm
The 5-year OS rates and the 1- and 3-year DFS rates
of patients treated with RES were significantly different than the
RFA treatment group, whereas the 1- and 3-year OS rates and the
5-year DFS rate of patients treated with RES were not significantly
higher than those of the RFA treatment group.
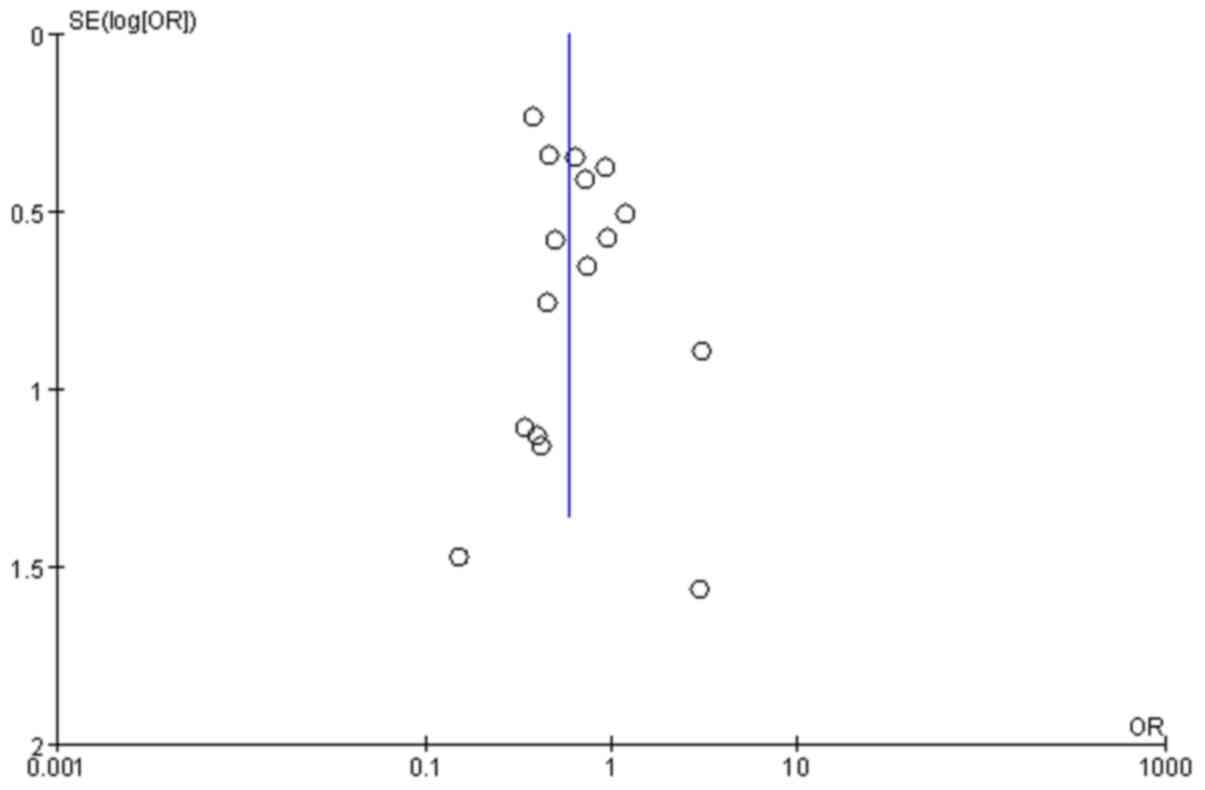
Testing for publication bias
A funnel plot was used to determine the level of
bias (Fig. 8). The funnel plot for
1-year OS rates following RFA or RES shows symmetry, which suggests
that there was no signficant publication bias. In addition, Begg
tests were performed to exclude the possibility of asymmetry in
funnel plots (continuity corrected, z =1.35, P=0.178). The results
of the Begg tests suggested that chances of publication bias were
minimal.
Discussion
At present, RES and RFA are commonly used and
regarded as the curative methods for the treatment of patients with
small HCC tumors. However, no definite consensus for which modality
is the most effective has been reached. OS and DFS are two common
primary indexes used to assess the curative effects of treatments
for patients with cancer. Each index emphasizes different factors.
DFS is a significant index that reveals the treatment effect of
therapeutic modalities employed, while OS represents the response
to the overall condition, including comprehensive treatment
modalities, the state of patient health, and other relevant factors
that influence survival. Although DFS is considered to be the more
appropriate index for evaluating the effect of the therapeutic
modalities used, in accordance with current practice, both DFS and
OS rates were used to compare the therapeutic effectiveness of RES
and RFA in the current study. The results of the meta-analysis
demonstrated that RES was superior to RFA with regards to the
survival of patients with resectable HCC. This is because the 1-,
3- and 5-year OS and DFS rates of patients treated using RFA were
generally lower than those treated with RES. RFA techniques use
thermal effects to kill tumor cells (42–44). The
ablation process is influenced by numerous factors, such as overall
energy deposition, the duration of application, electrode types or
tip length and gauge. In addition, if ablation is applied with or
without pulsed radiofrequency or cluster techniques, this may
result in instability of the required RFA therapy effect (45–47), and
may lead to higher recurrence rates. By contrast, RES has been
demonstrated to eliminate cancer nodules thoroughly and prevent
recurrence (32,48,49).
Therefore, the OS and DFS rates of patients treated using RFA are
lower than that of RES. Mulier et al (50) concluded that the short-term benefits
of using a less invasive method through the percutaneous route of
RFA does not counteract the increased long-term risk of local
recurrence (Belgium and Netherlands). Therefore, the authors of the
present study consider that RES may serve an important role in the
treatment of patients with HCC (8).
As such, clinicians treating HCC patients within the Milan criteria
should consider hepatectomy as the primary treatment option if the
patient's liver function and general condition are sufficient for
surgery (51) (Korea).
At present, RFA is frequently used as a first-line
treatment option for patients with HCC tumors as large as 5 cm
(52). It is generally considered
that the smaller the lesion, the better the effect of treatment.
Peng et al (41) demonstrated
that the OS rates, but not the recurrence-free survival rates, of
percutaneous RFA were significantly improved when compared with
those of RES in patients with HCC tumors measuring ≤2 cm. In
addition, subgroup analysis of patients with central HCC (where the
tumor is located >3 cm from the liver capsule), the OS and
recurrence-free survival rates of percutaneous RFA were improved
when compared with RES (China). This previous study provided an
explanation for the superior effect of RFA when compared with RES.
However, it did not provide an explanation for the worse relative
efficacy of RES, aside from the observation that patients treated
using this method had more severe complications. The conclusions of
this previous study contradicted the majority of other relevant
studies (18,30,31,53). Guo
et al collated and performed a meta-analysis of previous
studies to assess the outcomes of combined transcatheter arterial
chemoemobolization (TACE)-RFA vs. RES alone in patients with early
HCC and small resectable tumors. The results demonstrated that,
even though TACE-RFA showed comparable 1- and 3-year OS rates and
1-year recurrence-free rates compared with RES, this combination
was associated with significantly lower 3-year recurrence-free
survival rates compared with RES. Therefore, the authors concluded
that RES should still be considered as the primary choice of
treatment for patients with early HCC (54).
In the present study, subgroup analysis was
performed to better compare the outcomes of RES and RFA in patients
with HCC. To achieve this, patients were divided into two subgroups
based on mean tumor size (~3 cm). In the group of patients with
tumors ≤3 cm in size, those treated with RES demonstrated
significantly improved 3- and 5-year OS rates, as well as 1-, 3-
and 5-year DFS rates, compared with those treated with RFA. It was
therefore considered that if patients are in good physical
condition and have good liver function, treatment using RES may
likely increase their OS. In the group of patients with a mean
tumor size of >3 cm, those treated using RES demonstrated
significantly higher 5-year OS rates and 1- and 3-year DFS rates
compared to those treated using RFA; however, no significant
difference between the 1- and 3-year OS rates, and the 5-year DFS
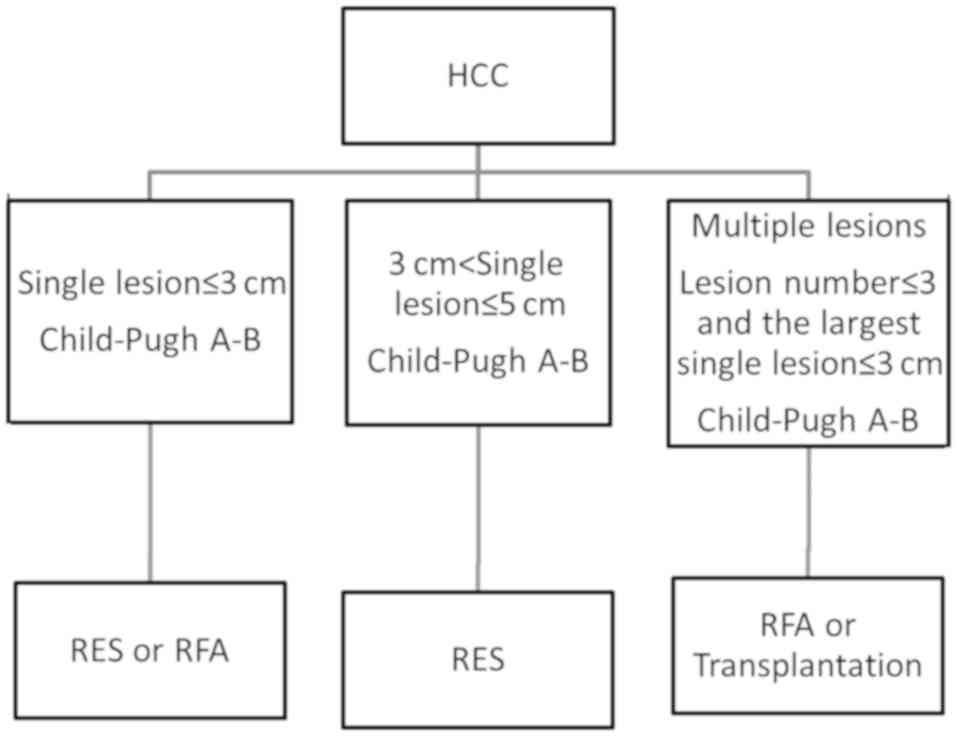
rates was observed between these groups. Based on the results of
the present study, the authors recommend a therapeutic regimen for
patients with small HCC tumors, as presented in the flow-chart
(Fig. 9).
In current studies, local intrahepatic recurrences
were found to be more frequent following RFA when compared with
RES. Local recurrences following RFA may be attributable to
insufficient ablation of the primary tumor and/or the presence of
tumor venous invasion in the adjacent liver tissue. By contrast,
RES may remove the primary tumor and venous tumor thrombi (32) which may explain the improved survival
rates following RES.
An ideal meta-analysis should include individual
patient data. However, these data are not always available or may
be impractical to collect. Therefore, the majority of
meta-analyses, including the current study, are instead performed
using summary data, which is an accepted form of analysis. However,
in the present study, it was not possible to perform a complete
analysis of the causes of death in the selected studies due to the
lack of individual patient data. Another limitation of the current
study was that numerous observational studies included in the
analysis had significant heterogeneity due to the nature of the
surgical studies. Specifically, it is difficult to perform the same
operations across different hospitals. Therefore, the outcomes of
the RES procedure across different centers may be, to some extent,
not comparable. In addition, bias caused by a number of different
factors, such as case selection, patient condition, medical
equipment and the individual dependence of surgical techniques may
affect statistical analysis of the results. In order to perform
more rigorous testing, a random-effects model was used for the
meta-analysis. The inclusion of a limited number of RCTs from
original published studies is another important limitation of the
current study, and meta-analyses have been traditionally applied
and are best confined to RCTs. However, it has also been
demonstrated that meta-analytical techniques using non-RCT and
observational studies may present a valid method in some clinical
settings, where either the number or the sample size of RCTs is
insufficient (55) (France).
In conclusion, this meta-analysis of studies
compared the long-time survival rates of RFA and RES techniques for
the treatment of patients with HCC. RES was demonstrated to show
superior 1-, 3- and 5-year OS and DFS rates than RFA for patients
with small HCC that were eligible for surgical treatment. However,
RFA can be an alternative therapeutic option for patients with
small single HCC tumors that are not suitable for RES. Future RCTs
are required to clarify the value of RES and RFA for the treatment
of patients with HCC.
Acknowledgements
The authors would like to thank Professor Jinshan
Zhang, the former director of Radiology department of Chinese PLA
General Hospital, for his permission to perform the current study,
and for providing necessary consultation on radiofrequency ablation
techniques.
Funding
The present study was supported by Sanya Meical
Science and Technical Innovation Funding (grant no. 2017YW02).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JKL designed the current study and interpreted the
results. XHL retrieved the literature and wrote the manuscript. HC
interpreted and analyzed the data. XHX performed the statistical
analysis. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bosch FX, Ribes J and Borras J:
Epidemiology of primary liver cancer. Semin Liver Dis. 19:271–285.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
El-Serag HB and Rudolph KL: Hepatocellular
carcinoma: Epidemiology and molecular carcinogenesis.
Gastroenterology. 132:2557–2576. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Taylor-Robinson SD, Foster GR, Arora S,
Hargreaves S and Thomas HC: Increase in primary liver cancer in the
UK, 1979–94. Lancet. 350:1142–1143. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
El-Serag HB and Mason AC: Rising incidence
of hepatocellular carcinoma in the United States. N Engl J Med.
340:745–750. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Malago M, Rogiers X and Broelsch CE: Liver
splitting and living donor techniques. Br Med Bull. 53:860–867.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ryder SD; British Society of
Gastroenterology, : Guidelines for the diagnosis and treatment of
hepatocellular carcinoma (HCC) in adults. Gut. 52 (Suppl
3):iii1–iii8. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Johnson PJ: Hepatocellular carcinoma: Is
current therapy really altering outcome? Gut. 51:459–462. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bruix J and Llovet JM: Prognostic
prediction and treatment strategy in hepatocellular carcinoma.
Hepatology. 35:519–524. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bruix J, Sherman M, Llovet JM, Beaugrand
M, Lencioni R, Burroughs AK, Christensen E, Pagliaro L, Colombo M
and Rodés J; EASL Panel of Experts on HCC, : Clinical management of
hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL
conference. European Association for the Study of the Liver. J
Hepatol. 35:421–430. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Livraghi T: Guidelines for treatment of
liver cancer. Eur J Ultrasound. 13:167–176. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lai EC, Fan ST, Lo CM, Chu KM, Liu CL and
Wong J: Hepatic resection for hepatocellular carcinoma. An audit of
343 patients. Ann Surg. 221:291–298. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Marin-Hargreaves G, Azoulay D and Bismuth
H: Hepatocellular carcinoma: Surgical indications and results. Crit
Rev Oncol Hematol. 47:13–27. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Arii S, Yamaoka Y, Futagawa S, Inoue K,
Kobayashi K, Kojiro M, Makuuchi M, Nakamura Y, Okita K and Yamada
R: Results of surgical and nonsurgical treatment for small-sized
hepatocellular carcinomas: A retrospective and nationwide survey in
Japan. The Liver Cancer Study Group of Japan. Hepatology.
32:1224–1229. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fried MW: Treatment of hepatocellular
carcinoma: Medical options. Liver Transpl Surg. 4((5 Suppl 1)):
S92–S97. 1998.PubMed/NCBI
|
|
15
|
Ogihara M, Wong LL and Machi J:
Radiofrequency ablation versus surgical resection for single nodule
hepatocellular carcinoma: Long-term outcomes. HPB (Oxford).
7:214–221. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ogata S, Belghiti J, Varma D, Sommacale D,
Maeda A, Dondero F and Sauvanet A: Two hundred liver hanging
maneuvers for major hepatectomy: A single-center experience. Ann
Surg. 245:31–35. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li L, Zhang J, Liu X, Li X, Jiao B and
Kang T: Clinical outcomes of radiofrequency ablation and surgical
resection for small hepatocellular carcinoma: A meta-analysis. J
Gastroenterol Hepatol. 27:51–58. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ng KKC, Chok KSH, Chan ACY, Cheung TT,
Wong TCL, Fung JYY, Yuen J, Poon RTP, Fan ST and Lo CM: Randomized
clinical trial of hepatic resection versus radiofrequency ablation
for early-stage hepatocellular carcinoma. Br J Surg. 104:1755–1784.
2017. View Article : Google Scholar
|
|
19
|
Machi J, Uchida S, Sumida K, Limm WM,
Hundahl SA, Oishi AJ, Furumoto NL and Oishi RH: Ultrasound-guided
radiofrequency thermal ablation of liver tumors: Percutaneous,
laparoscopic, and open surgical approaches. J Gastrointest Surg.
5:477–489. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Poon RT, Fan ST, Tsang FH and Wong J:
Locoregional therapies for hepatocellular carcinoma: A critical
review from the surgeon's perspective. Ann Surg. 235:466–486. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen MS, Li JQ, Zheng Y, Guo RP, Liang HH,
Zhang YQ, Lin XJ and Lau WY: A prospective randomized trial
comparing percutaneous local ablative therapy and partial
hepatectomy for small hepatocellular carcinoma. Ann Surg.
243:321–328. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang J, Yan L, Cheng Z, Wu H, Du L, Wang
J, Xu Y and Zeng Y: A randomized trial comparing radiofrequency
ablation and surgical resection for HCC conforming to the Milan
criteria. Ann Surg. 252:903–912. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Feng K, Yan J, Li X, Xia F, Ma K, Wang S,
Bie P and Dong J: A randomized controlled trial of radiofrequency
ablation and surgical resection in the treatment of small
hepatocellular carcinoma. J Hepatol. 57:794–802. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hong SN, Lee SY, Choi MS, Lee JH, Koh KC,
Paik SW, Yoo BC, Rhee JC, Choi D, Lim HK, et al: Comparing the
outcomes of radiofrequency ablation and surgery in patients with a
single small hepatocellular carcinoma and well-preserved hepatic
function. J Clin Gastroenterol. 39:247–252. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Montorsi M, Santambrogio R, Bianchi P,
Donadon M, Moroni E, Spinelli A and Costa M: Survival and
recurrences after hepatic resection or radiofrequency for
hepatocellular carcinoma in cirrhotic patients: A multivariate
analysis. J Gastrointest Surg. 9:62–67; discussion 67–68. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nishikawa H, Inuzuka T, Takeda H, Nakajima
J, Matsuda F, Sakamoto A, Henmi S, Hatamaru K, Ishikawa T, Saito S,
et al: Comparison of percutaneous radiofrequency thermal ablation
and surgical resection for small hepatocellular carcinoma. BMC
Gastroenterol. 11:1432011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Vivarelli M, Guglielmi A, Ruzzenente A,
Cucchetti A, Bellusci R, Cordiano C and Cavallari A: Surgical
resection versus percutaneous radiofrequency ablation in the
treatment of hepatocellular carcinoma on cirrhotic liver. Ann Surg.
240:102–107. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Xu G, Qi FZ, Zhang JH, Cheng GF, Cai Y and
Miao Y: Meta-analysis of surgical resection and radiofrequency
ablation for early hepatocellular carcinoma. World J Surg Oncol.
10:1632012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Livraghi T, Meloni F, Di Stasi M, Rolle E,
Solbiati L, Tinelli C and Rossi S: Sustained complete response and
complications rates after radiofrequency ablation of very early
hepatocellular carcinoma in cirrhosis: Is resection still the
treatment of choice? Hepatology. 47:82–89. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Tashiro H, Aikata H, Waki K, Amano H,
Oshita A, Kobayashi T, Tanimoto Y, Kuroda S, Tazawa H, Chayama K,
et al: Treatment strategy for early hepatocellular carcinomas:
Comparison of radiofrequency ablation with or without transcatheter
arterial chemoembolization and surgical resection. J Surg Oncol.
104:3–9. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Abu-Hilal M, Primrose JN, Casaril A,
McPhail MJ, Pearce NW and Nicoli N: Surgical resection versus
radiofrequency ablation in the treatment of small unifocal
hepatocellular carcinoma. J Gastrointest Surg. 12:1521–1526. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Liu JG, Wang YJ and Du Z: Radiofrequency
ablation in the treatment of small hepatocellular carcinoma: A meta
analysis. World J Gastroenterol. 16:3450–3456. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Cho YK, Rhim H and Noh S: Radiofrequency
ablation versus surgical resection as primary treatment of
hepatocellular carcinoma meeting the Milan criteria: A systematic
review. J Gastroenterol Hepatol. 26:1354–1360. 2011.PubMed/NCBI
|
|
34
|
Zhou Y, Zhao Y, Li B and Xu D:
Meta-analysis of radiofrequency ablation versus hepatic resection
for small hepatocellular carcinoma. BMC Gastroenterol. 10:782010.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Xu XL, Liu XD, Liang M and Luo BM:
Radiofrequency ablation versus hepatic resection for small
hepatacellular carcinoma: Systematic review of randomized
controlled trials with meta-analysis and trial sequential analysis.
Radiology. 287:461–472. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jadad AR, Moore RA, Carroll D, Jenkinson
C, Reynolds DJ, Gavaghan DJ and McQuay HJ: Assessing the quality of
reports of randomized clinical trials: Is blinding necessary?
Control Clin Trials. 17:1–12. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wells G, Shea B, O'Connell D, Peterson J,
Welch V, Losos M and Tugwell P: The Newcastle-Ottawa Scale (NOS)
for assessing the quality of nonrandomised studies in
meta-analyses. http://www.evidencebasedpublichealth.de/download/Newcastle_Ottowa_Scale_Pope_Bruce.pdf
|
|
38
|
Borenstein M, Hedges L, Higgins JPT and
Rothstein H: Fixed effect vs. random effectsIntroduction to
Meta-Analysis. John Wiley and Sons Ltd.; Chichester, UK: 2009,
View Article : Google Scholar
|
|
39
|
Yakoub D, Athanasiou T, Tekkis P and Hanna
GB: Laparoscopic assisted distal gastrectomy for early gastric
cancer: Is it an alternative to the open approach? Surg Oncol.
18:322–333. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Huang J, Hernandez-Alejandro R, Croome KP,
Yan L, Wu H, Chen Z, Prasoon P and Zeng Y: Radiofrequency ablation
versus surgical resection for hepatocellular carcinoma in Childs A
cirrhotics-a retrospective study of 1,061 cases. J Gastrointest
Surg. 15:311–320. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Peng ZW, Lin XJ, Zhang YJ, Liang HH, Guo
RP, Shi M and Chen MS: Radiofrequency ablation versus hepatic
resection for the treatment of hepatocellular carcinomas 2 cm or
smaller: A retrospective comparative study. Radiology.
262:1022–1033. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sironi S, Livraghi T, Meloni F, De Cobelli
F, Ferrero C and Del Maschio A: Small hepatocellular carcinoma
treated with percutaneous RF ablation: MR imaging follow-up. AJR Am
J Roentgenol. 173:1225–1229. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Livraghi T, Goldberg SN, Lazzaroni S,
Meloni F, Ierace T, Solbiati L and Gazelle GS: Hepatocellular
carcinoma: Radio-frequency ablation of medium and large lesions.
Radiology. 214:761–768. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Livraghi T, Solbiati L, Meloni MF, Gazelle
GS, Halpern EF and Goldberg SN: Treatment of focal liver tumors
with percutaneous radio-frequency ablation: Complications
encountered in a multicenter study. Radiology. 226:441–451. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Goldberg SN and Gazelle GS: Radiofrequency
tissue ablation: Physical principles and techniques for increasing
coagulation necrosis. Hepatogastroenterology. 48:359–367.
2001.PubMed/NCBI
|
|
46
|
Miao Y, Ni Y, Yu J and Marchal G: A
comparative study on validation of a novel cooled-wet electrode for
radiofrequency liver ablation. Invest Radiol. 35:438–444. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Goldberg SN, Gazelle GS, Solbiati L,
Rittman WJ and Mueller PR: Radiofrequency tissue ablation:
Increased lesion diameter with a perfusion electrode. Acad Radiol.
3:636–644. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Sasaki A, Kai S, Iwashita Y, Hirano S,
Ohta M and Kitano S: Microsatellite distribution and indication for
locoregional therapy in small hepatocellular carcinoma. Cancer.
103:299–306. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Shiina S, Tagawa K, Unuma T, Takanashi R,
Yoshiura K, Komatsu Y, Hata Y, Niwa Y, Shiratori Y and Terano A:
Percutaneous ethanol injection therapy for hepatocellular
carcinoma. A histopathologic study. Cancer. 68:1524–1530. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Mulier S, Ni Y, Jamart J, Ruers T, Marchal
G and Michel L: Local recurrence after hepatic radiofrequency
coagulation: Multivariate meta-analysis and review of contributing
factors. Ann Surg. 242:158–171. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Park EK, Kim HJ, Kim CY, Hur YH, Koh YS,
Kim JC, Kim HJ, Kim JW and Cho CK: A comparison surgical resection
and radiofrequency ablation in the treatment of hepatocellular
carcinoma. Ann Surg Treat Res. 87:72–80. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Kutlu OC, Chan JA, Aloia TA, Chun YS,
Kaseb AO, Passot G, Yamashita S, Vauthey JN and Conrad C:
Comparative effectiveness of first-line radiofrequency ablation
versus surgical resection and transplantation for patents with
early hepatocellular carcinoma. Cancer. 123:1817–1827. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Gravante G, Overton J, Sorge R, Bhardwaj
N, Metcalfe MS, Lloyd DM and Dennison AR: Radiofrequency ablation
versus resection for liver tumors: An evidence-based approach to
retrospective compartive studies. J Gastrointest Surg. 15:378–387.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Guo W, He X, Li Z and Li Y: Combination of
transarterial chemoembolization (TACE) and radiofrequency ablation
(RFA) vs. Surgical resection (SR) on survival outcome of early
hepatocellular carcinoma: A meta-analysis. Hepatogastroenterology.
62:710–714. 2015.PubMed/NCBI
|
|
55
|
Mathurin P, Raynard B, Dharancy S, Kirzin
S, Fallik D, Pruvot FR, Roumilhac D, Canva V, Paris JC, Chaput JC
and Naveau S: Meta-analysis: Evaluation of adjuvant therapy after
curative liver resection for hepatocellular carcinoma. Aliment
Pharmacol Ther. 17:1247–1261. 2003. View Article : Google Scholar : PubMed/NCBI
|