Introduction
Squamous cell carcinoma of the endometrium is rare.
We report a 68-year-old woman who presented with brown discharge
and was found to have concomitant squamous cell carcinoma of the
endometrium and cervical endometrioid carcinoma. Pelvic
ultrasonography demonstrated 300 ml of purulent material, i.e.,
pyometra. Pelvic magnetic resonance imaging (MRI) also showed a
tumorous lesion occupying the cervical uteri, measuring 3 cm in
diameter, as well as confirming the pyometra. Total abdominal
hysterectomy with bilateral salpingo-oophorectomy was performed,
and the clinical diagnosis was cervical tumor with concomitant
pyometra. An existing primary cancer involving two organs in a
single patient is a rarity in the medical literature. Herein, we
report a rare case with two primary cancers, of different
histological types, one involving the cervical uteri and the other
the uterine body. Chronic and widespread inflammation of the
endometrium associated with overt ichthyosis may predispose to the
development of primary squamous cell carcinoma of the endometrium
(PSCCE). PSCCE should be considered in the differential diagnosis
when evaluating elderly postmenopausal women presenting with
pyometra.
Case report
A 68-year-old Japanese woman, gravida 1 para 1, was
admitted to our department with a chief complaint of watery brown
vaginal discharge which had persisted for 10 days. She had been
diagnosed with rheumatoid arthritis 23 years earlier. She had
experienced menopause at the age of 50. Pelvic ultrasound showed a
total of 300 ml of fluid, and the pyometra was drained from the
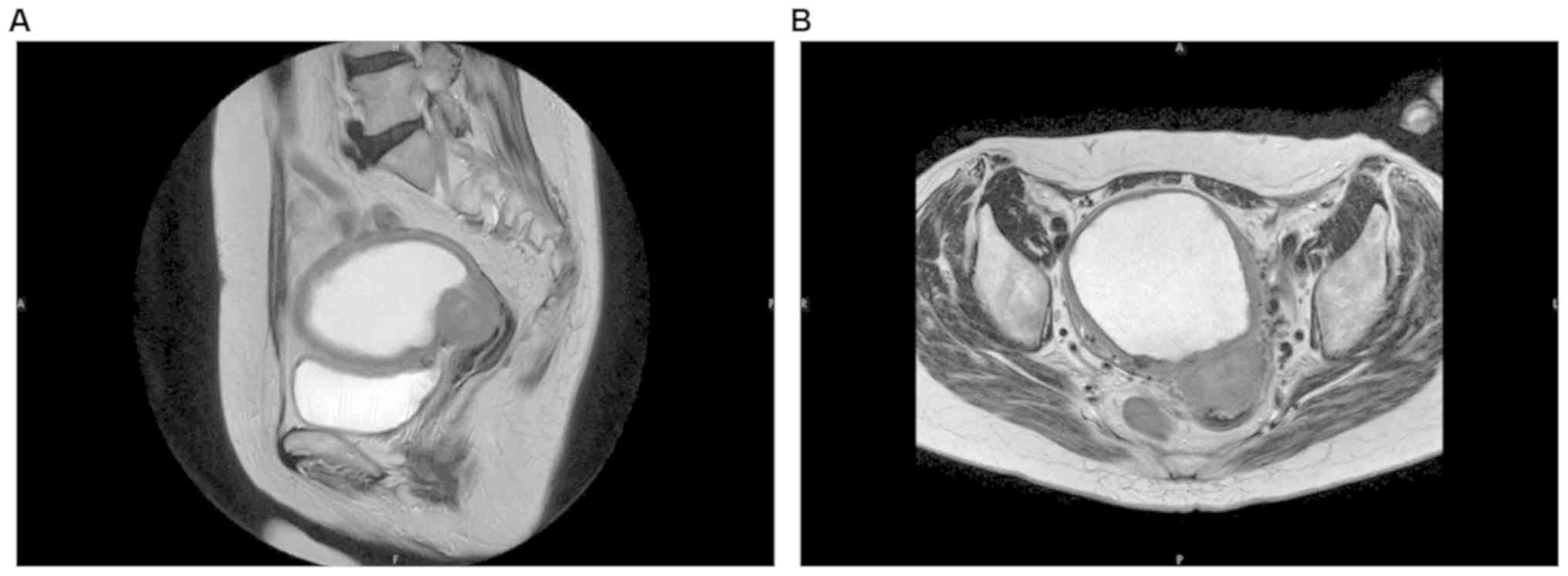
uterus. Pelvic MRI showed a tumor, measuring 3 cm in diameter, at
the bottom of the endometrium and massive fluid accumulation within
the irregular endometrium in the uterus (Fig. 1). After drainage of the fluid, an
endometrial biopsy was performed, but the specimen obtained was not
sufficient for diagnosis. Tumor of the cervical uteri and pyometra
were the clinical diagnoses; total abdominal hysterectomy with
bilateral salpingo-oophorectomy was thus performed. The patient was
given chemotherapy with carboplatin (area under the curve, 6) and
paclitaxel (175 mg/m2). She has remained well, without
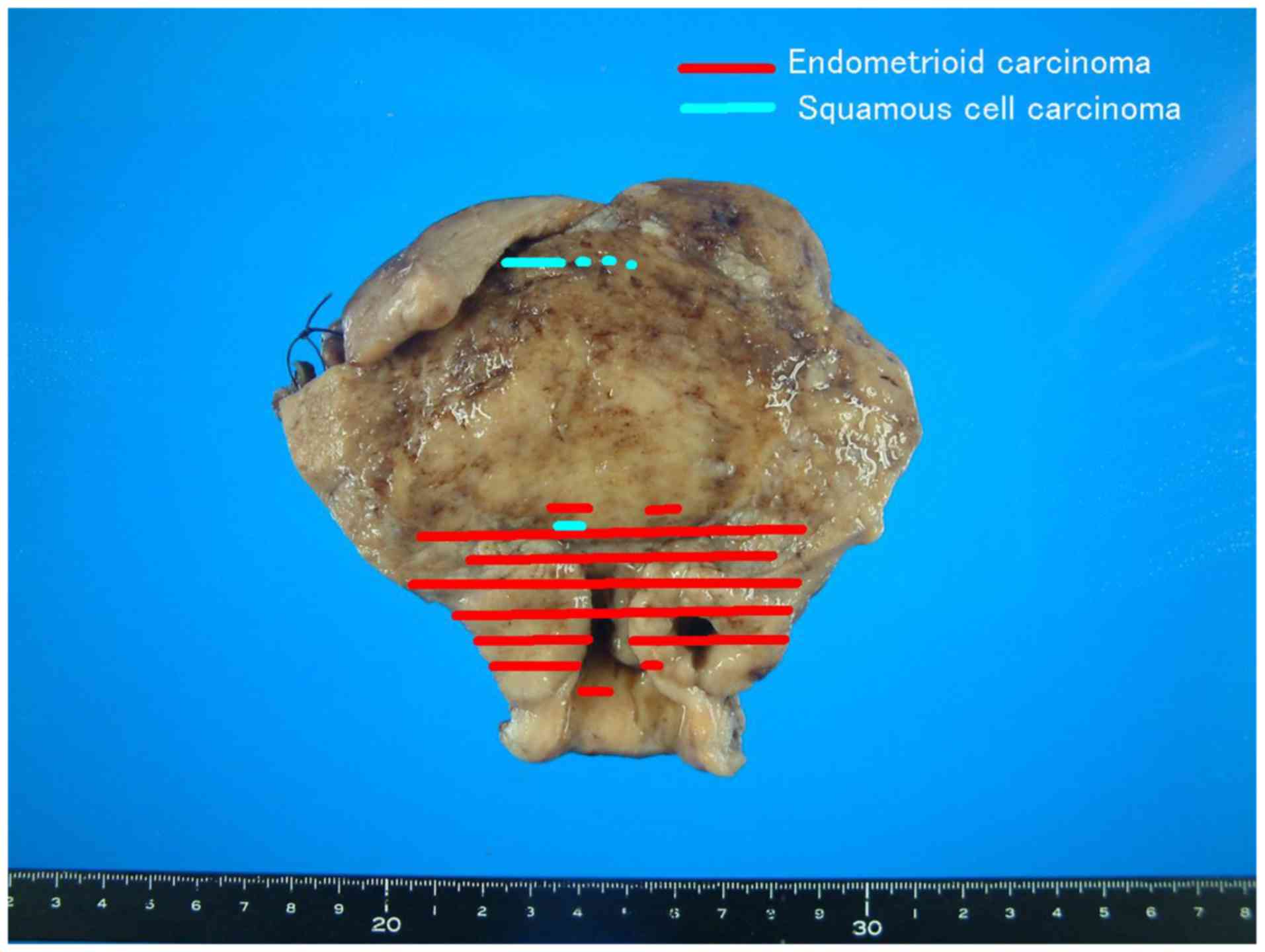
evidence of disease, for 1 year to date since the surgery. Gross
findings: The resected uterus and bilateral adnexa measured 125x125
mm in size. Macroscopically, the uterine body was markedly
enlarged. The endometrial cavity was dilated, due to being filled
with foul-smelling mossy debris and pus (Fig. 2). There was a whitish mass measuring
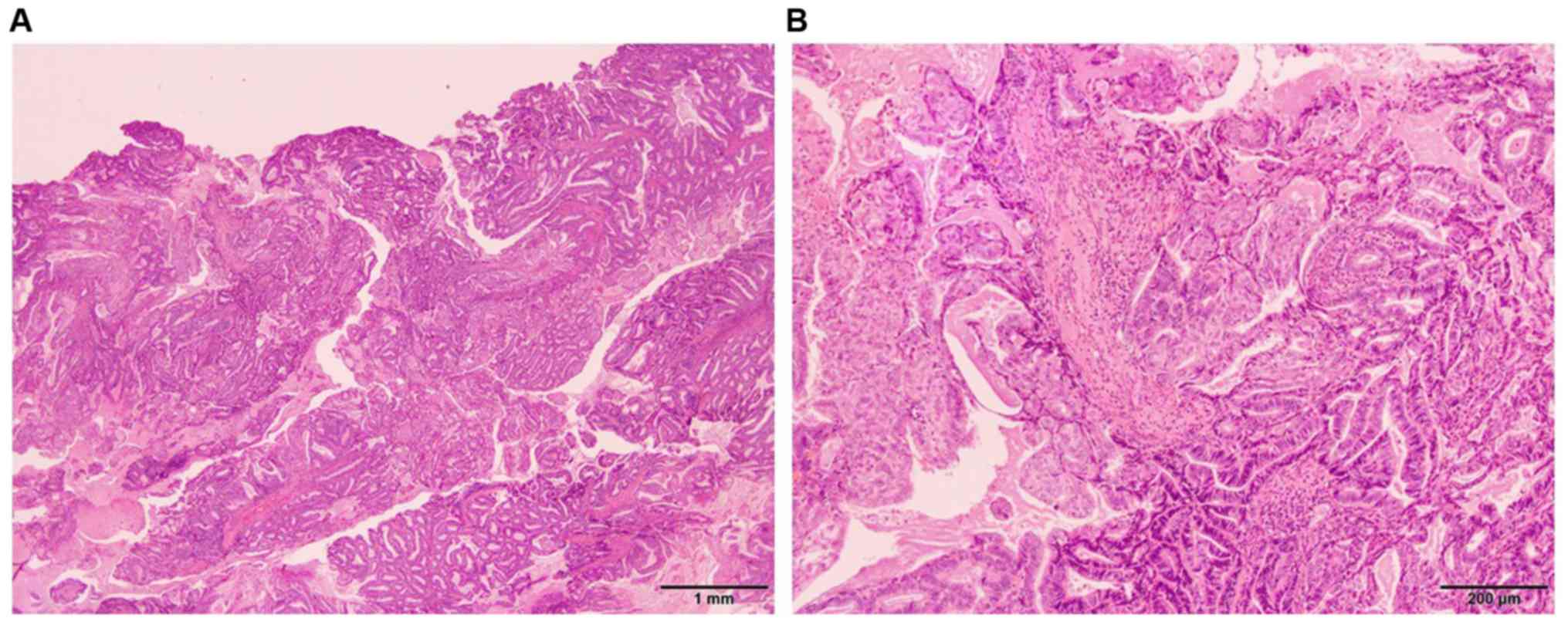
30x30x23 mm in the uterine cervix. Histologically, the cervical
tumor was endometrioid carcinoma, composed of irregular-shaped
neoplastic glands. The tumor tissue invaded the myometrium
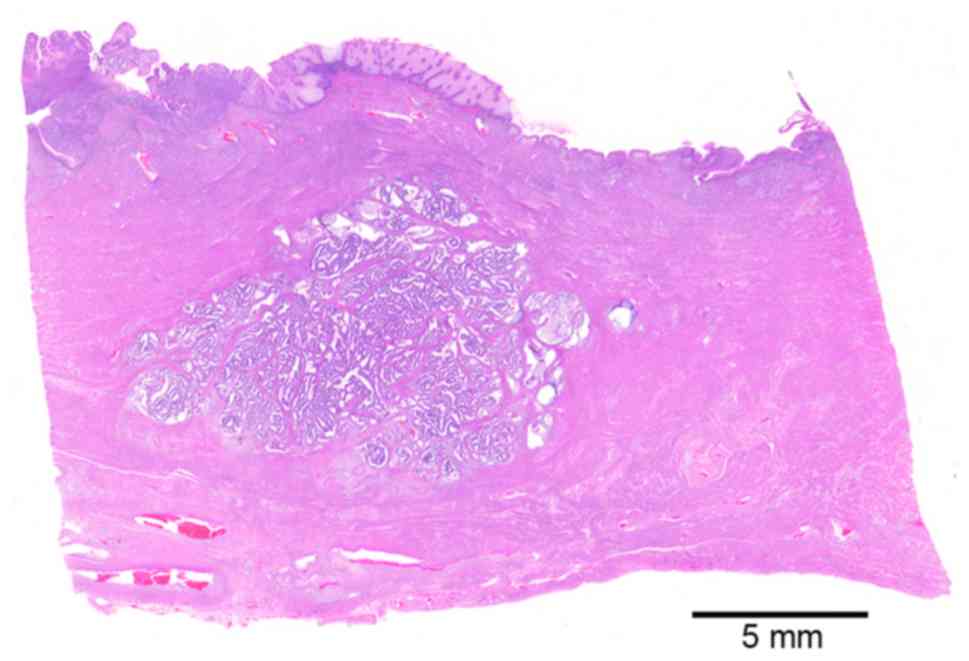
(Fig. 3). We added immunostaining
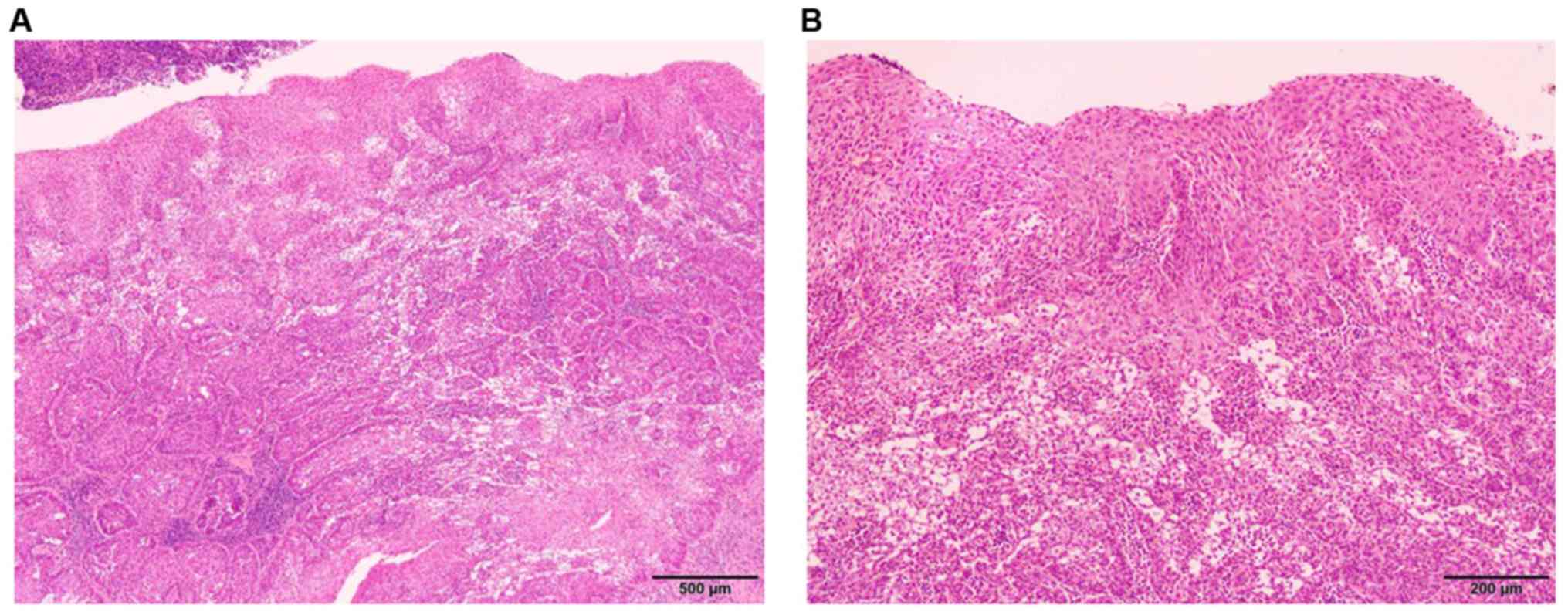
investigation, but detected no lymphovascular involvement. Most of
the endometrium had shed the epithelial lining and was covered with
granulation tissue. The residual epithelia had been replaced by
ichthyosis uteri which was accompanied by squamous epithelium.
There were two foci of squamous cell carcinoma, one of which was
close to the endometrioid carcinoma, but the upper endometrium
showed no connection with the squamous epithelium of the cervix
(Figs. 4 and 5). All of the tumors were negative for
p16INK4a, indicating that a contribution of the human
papilloma virus to carcinogenesis was unlikely.
Discussion
Our present patient was an elderly postmenopausal
woman, who had initially developed cervical endometrioid carcinoma.
In this case, the cervical cancer had resulted in stenosis of the
uterine orifice. Subsequently, persistent endometrial inflammatory
changes with pyometra produced extensive ichthyosis uteri. Notably,
this patient developed squamous cell carcinoma in the endometrium
with two foci. Ichthyosis uteri is characterized by replacement of
the entire endometrial surface by stratified squamous epithelium
(1,2). PSCCE can arise from squamous
metaplasia of the endometrium (3).
Many factors predisposing to the development of PSCCE have been
suggested, including pyometra, radiation, and abnormal estrogen
levels (1,2,4,5). The
pyometra in this patient had been caused by neoplastic obstruction
of the uterine orifice and persistent infection. However, the
mechanisms of squamous metaplasia and malignant transformation
remain unknown. No more than 50% of PSCCE cases can be definitively
diagnosed prior to the surgery (5).
In our present case, it was not possible to establish the diagnosis
of PSCCE prior to the hysterectomy being performed. Although an
endometrial biopsy should have been performed to obtain a
definitive diagnosis of endometrioid cancer, this was difficult due
to the cervical stenosis and pyometra. When pyometra and PSCCE are
found in elderly postmenopausal women, potentially causative
factors such as chronic and persistent inflammation of the
endometrium leading to extensive ichthyosis uteri should be
considered (1,2). Hysterectomy is required, given the
possibility of malignancy. PSCCE is a rare disease. Squamous cell
carcinomas found in the endometrium are mostly of cervical uteri
origin. Though endometrioid squamous cell carcinoma is not included
in the WHO classification of tumors of Female Reproductive Organs
(6), there are several reports
describing endometrioid squamous differentiation and PSCCE
(1,2,7,8). PSCCE
can be differentiated from endometrial squamous cell carcinoma
involvement based on the pathological criteria proposed by
Fluhmann: i) no evidence of a coexisting endometrial adenocarcinoma
or primary cervical squamous cell carcinoma; ii) no connection
between the endometrial tumor and squamous epithelium of the
cervix; iii) no connection between any in situ carcinoma of
cervix and endometrial neoplasm (9). Our present case fulfilled the criteria
proposed by Fluhmann. Thus, we diagnosed the patient as having two
primary cancers, i.e., endometrioid carcinoma of the cervix and
PSCCE. Moreover, this patient had been taking methotrexate for
several years as treatment for rheumatoid arthritis. The resulting
immunocompromised state might have exacerbated the persistent
inflammation, possibly contributing to the development of PSCCE
(10).
In conclusion, the possibility of PSCCE should be
considered in elderly postmenopausal women presenting with
long-standing pyometra. Chronic and extensive inflammation of the
endometrium associated with overt ichthyosis uteri may predispose
affected individuals to the development of PSCCE.
Acknowledgements
Not applicable.
Funding
This study was supported in part by JSPS KAKENHI
(grant no. 17K11162 to YN).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YAk, TY, YN and TT collaborated in the conception
and design of the study. YAk and YN wrote the manuscript. TY, TK,
YH, KO, YAb and YN analyzed the data and reviewed the manuscript.
All authors were involved in writing the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent for publication of clinical
details was obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jain M, Kashyap A and Biswas R: Primary
endometrial squamous cell carcinoma in-situ with extensive
ichthyosis uteri: A rare case report. J Clin Diagn Res.
11:ED13–ED14. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Takeuchi K, Tsujino T, Yabuta M and
Kitazawa S: A case of primary squamous cell carcinoma of the
endometrium associated with extensive ‘ichthyosis uteri’. Eur J
Gynaecol Oncol. 33:552–554. 2012.PubMed/NCBI
|
|
3
|
Lee SJ and Choi HJ: Primary endometrial
squamous cell carcinoma: A case report and review of relevant
literature on Korean women. Korean J Pathol. 46:395–398.
2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Baggish MS and Woodruff JD: The occurrence
of squamous epithelium in the endometrium. Obstet Gynecol Surv.
22:69–115. 1967.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Goodman A, Zukerberg LR, Rice LW, Fuller
AF, Young RH and Scully RE: Squamous cell carcinoma of the
endometrium: A report of eight cases and a review of the
literature. Gynecol Oncol. 61:54–60. 1996.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kurman RJ, Carcangiu ML, Herrington CS and
Young RH: IARC. WHO Classification of Tumours of Female
Reproductive Organs. 4rth edition. In: WHO Classification of
Tumours, vol. 6. IARC, Lyon, France, 2014.
|
|
7
|
Farhane FZ, Alami Z, Bouhafa T, Elmazghi A
and Hassouni K: Primary squamous cell carcinoma of endometrium:
Case report and literature review. Pan Afr Med J.
30(208)2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Terada T and Tateoka K: Primary pure
squamous cell carcinoma of the endometrium: A case report. Int J
Clin Exp Pathol. 6:990–993. 2013.PubMed/NCBI
|
|
9
|
Fluhmann CF: The histogenesis of squamous
cell metaplasia of the cervix and endometrium. Surg Gynecol Obstet.
97:45–58. 1953.PubMed/NCBI
|
|
10
|
Lim XR, Xiang W, Tan JWL, Koh LW, Lian TY,
Leong KP and Koh ET: TTSH Rheumatoid Arthritis Study Group.
Incidence and patterns of malignancies in a multi-ethnic cohort of
rheumatoid arthritis patients. Int J Rheum Dis. 22:1679–1685.
2019.PubMed/NCBI View Article : Google Scholar
|