Introduction
Uterine sarcomas are a group of rare neoplasms,
arising from myometrial or mesenchymal tissue, which represent 3 to
7% of uterine cancer and tend to affect more elderly women, to
exhibit aggressive behavior with fast-growing, early distant
metastasis and diagnosed in more advanced stages (1-3).
Surgery is considered the basis of the treatment and other
treatment modalities, such as chemotherapy or radiation therapy,
have shown limited results (3,4).
Sarcomas exhibit diverse histopathology and some
cases may have a Mullerian duct origin resulting in heterologous
histology. The modifications in their classifications have
contributed to a gap of knowledge with regard to risk factors,
prognosis, and management (5,6). Based
on the latest classification of gynecological malignancies by the
World Health Organization in 2014(7), the main uterine sarcoma types are the
following: Leiomyosarcoma, endometrial stromal sarcoma (ESS) and
adenosarcoma. Carcinosarcomas, on the other hand, have been
recently reclassified as a metaplastic form of endometrial
carcinoma, and considered for staging and treatment similarly as a
high-grade carcinoma. However, this type of malignancy is still
frequently analyzed as a sarcoma in association with the previous
types (7,8).
The stage of uterine sarcomas (FIGO-2009) can be
considered as the most important prognostic factor and the main
strategy for optimal results is to achieve an early diagnosis
(9). The need to expand knowledge
regarding uterine sarcomas is highlighted by the upward trend in
the incidence due to the increased life expectancy (10). The present study aimed to provide
comprehensive information regarding the characteristics of the
women affected, the tumor pattern, diagnosis and management of
various types of uterine sarcomas. The patient survival was also
assessed over time based on the histological type.
Patients and methods
Subjects
This is a cohort study including patients assisted
in the Women's Hospital of the University of Campinas (UNICAMP), in
Campinas (São Paulo), Brazil from 2001 to 2016. UNICAMP is a
teaching and research institution and a referral center for the
Brazilian public health system. All surgical procedures were
performed or supervised by surgeons with vast experience. The
pathological evaluation was conducted by pathologists specialized
in gynecological malignancies. The cases studied were identified
from 1,191 records filtered by the International Classification of
Diseases, 10th edition (ICD-10) C.54, regarding uterine
corpus malignant neoplasia (11).
There were found 123 cases of uterine sarcomas, including
carcinosarcomas. Following revision of the medical records, one
case was excluded due to the patient undergoing a hysterectomy at
another hospital and not returning after initial appointment.
Therefore the final sample size was adjusted to 122 cases.
Management definition included clinical and image
evaluation and discussion in a multidisciplinary meeting. In case
when the surgery was the first approach selected, an extrafascial
hysterectomy (Piver type 1, Querleu A) with bilateral adnexectomy
was performed and pelvic or retroperitoneal lymphadenectomy was
conducted in specific cases. Women with advanced or unresectable
disease were managed by chemotherapy and/or radiotherapy according
to their clinical performance status. The relevant information on
clinical characteristics, neoplasms, treatment, and follow-up was
collected.
Statistical analysis
The number of cases assisted overtime was analyzed
by the χ2 test. Subsequently, a descriptive analysis
using the χ2 test or Fisher exact tests was conducted in
the total group according to the histological type of sarcomas (WHO
classification) (7). The analyses
were performed by age group distribution (<50 years, 50-59
years, 60-69 years, and 70 years or more), parity (0; 1-2; 3-4, and
5 or more), menopausal status, body mass index in Kg/m2
(<25; 25-29.9; 30-34.9; and 35 or more), the presence of
comorbidities (diabetes, arterial hypertension, cardiopathy,
obstructive pulmonary disease, thyroid disease, or other
parameters), smoking (current or past, regardless of the period
since quitting), neoplasm stage according to FIGO-2009 or -2014
(9,12), modality of initial treatment
(surgery, radiotherapy, chemotherapy, or no treatment) and the
results following treatment end (optimal surgery and/or complete
clinical response following radiotherapy and/or chemotherapy).
Subsequently, ESS and adenosarcoma were considered the specific
histological types with optimal prognosis, whereas carcinosarcoma
and leiomyosarcoma were the malignancy types with poor outcomes. A
logistic regression analysis (polytomous models of proportional
risks) was performed based on these considerations. Univariate and
multivariate analysis was performed with stepwise selection
criteria, calculating odds ratios with 95% confidence intervals for
the association between specific variables and the diagnosis of the
less favorable histological type.
The longitudinal analyses considered the overall
survival (OS) rate as the period between the diagnosis and the last
contact or death, whereas the disease-free survival rate was
estimated as the period between the end of treatment and the
relapse. Recurrence was confirmed by histopathology, clinical
examination or image examination and was classified as pelvic or
distant metastasis. Survival curves were constructed by the
Kaplan-Meier method and analyzed by the log-rank test. Statistical
analysis was performed using the StatsDirect statistical software
v3.0 (England, www.statsdirect.com). P<0.05 was considered to
indicate a statistically significant difference.
The present study was conducted in compliance with
the Brazilian National Health Council and was previously approved
by the Research Ethics Committee of the University of Campinas.
Results
Diagnosis trend of the uterine
sarcoma
The number of cases with malignant uterine corpus
neoplasms has increased in the period of 2001-2016. Specifically, a
trend of +10.8 additional cases was noted every two years for
carcinomas (P=0.003), whereas +1.2 additional cases were reported
every two years for sarcomas (P=0.044). During the period
2001-2002, 90 carcinomas and 10 sarcomas were recorded, while 168
carcinomas and 20 sarcomas were identified during the period
2015-2016. The proportion rate of carcinomas-sarcomas remained
relatively stable in the period with average values of
approximately 90 and 10%, respectively.
Patients and tumor
characteristics
The histological type distribution of the 122
sarcoma cases included 47% carcinosarcomas, 22% leiomyosarcomas,
16% ESSs and 14% adenosarcomas.
The signs or symptoms associated with the diagnosis
of sarcomas are presented in Table
I. The classification according to the histological type is
also shown. Abnormal uterine bleeding and abnormal image
examination were noted in 77 and 7% of the cases, respectively. The
diagnosis was confirmed through uterine curettage in 35% of the
subjects, surgery in 34%, hysteroscopy in 13% and biopsy at a
vaginal examination in 17%. A total of 16 cases of sarcoma were
diagnosed following hysterectomy due to myomatosis, and all
surgeries were performed in women aged between 29-55 years.
 | Table IDistribution of signs or symptoms
associated with the initial diagnosis of uterine sarcoma according
to the histological type. |
Table I
Distribution of signs or symptoms
associated with the initial diagnosis of uterine sarcoma according
to the histological type.
| |
Uterine
sarcomas by histological type |
|---|
| | CCS (n=57) | LMS (n=27) | ESS (n=20) | ADS (n =17) | Total
(n=122)a |
|---|
| Signs or
symptoms | n | % | n | % | n | % | n | % | n | % |
|---|
| Increased abdominal
girth | 2 | 4 | 4 | 15 | 1 | 5 | 0 | 0 | 7 | 6 |
| Pain | 1 | 2 | 4 | 15 | 0 | 0 | 0 | 0 | 5 | 4 |
| Abnormal uterine
bleeding | 49 | 85 | 15 | 55 | 18 | 90 | 12 | 70 | 94 | 77 |
| Vaginal
discharge | 2 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 2 |
| Prolapsed uterine
tumor | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 18 | 4a | 3 |
| Image exam | 3 | 5 | 3 | 11 | 1 | 5 | 2 | 12 | 9 | 7 |
| Metastasis | 0 | 0 | 1 | 4 | 0 | 0 | 0 | 0 | 1 | 1 |
The demographic characteristics of the women
according to the histological type of sarcoma are described in
Table II. The age of the patients
was 60 years or higher for 62% of the total sample size, of which
46% of carcinosarcomas were present in patients over 70 years,
while 26% of leiomyosarcomas and 45% of ESSs were detected at an
age lower than 50 years (P<0.0001). The carcinosarcoma group
exhibited 2-3 times higher nulliparous subjects (P=0.217) and 47%
of the ESS cases exhibited premenopausal status (P<0.001).
| Table IIDistribution of some variables
associated with 122 cases of uterine sarcomas managed between 2001
and 2016. |
Table II
Distribution of some variables
associated with 122 cases of uterine sarcomas managed between 2001
and 2016.
| |
Uterine
sarcomas by histological type |
|---|
| | CCS (n=57) | LMS (n=27) | ESS (n=20) | ADS (n=17) | | Total
(n=122)b |
|---|
| Variables | n | % | n | % | n | % | n | % |
P-valuea | n | % |
|---|
| Age group,
years | | | | | | | | | <0.0001 | | |
|
<50 | 0 | 0 | 7 | 26 | 9 | 45 | 3 | 18 | | 20b | 16 |
|
50-59 | 14 | 24 | 9 | 33 | 1 | 5 | 3 | 18 | | 27 | 22 |
|
60-69 | 17 | 30 | 7 | 26 | 4 | 20 | 5 | 29 | | 33 | 27 |
|
>70 | 26 | 46 | 4 | 15 | 6 | 30 | 6 | 35 | | 42 | 35 |
| Parityc | | | | | | | | | 0.217 | | |
|
0 | 13 | 23 | 2 | 7 | 2 | 10 | 2 | 12 | | 19 | 15 |
|
1-2 | 15 | 27 | 7 | 26 | 3 | 15 | 5 | 29 | | 30 | 25 |
|
3-4 | 11 | 20 | 13 | 48 | 8 | 25 | 3 | 18 | | 36b | 30 |
|
5+ | 17 | 30 | 5 | 19 | 7 | 35 | 7 | 41 | | 36 | 30 |
| Menopause | | | | | | | | | <0.001 | | |
|
Yes | 56 | 98 | 17 | 63 | 9 | 47 | 12 | 71 | | 94 | 77 |
|
No | 1 | 2 | 10 | 37 | 11 | 53 | 5 | 29 | | 28b | 23 |
| BMI,
kg/m2 | | | | | | | | | 0.640 | | |
|
<25 | 16 | 28 | 7 | 26 | 4 | 20 | 2 | 12 | | 29 | 24 |
|
25-29.9 | 19 | 33 | 10 | 37 | 10 | 50 | 6 | 35 | | 45 | 37 |
|
30-34.9 | 14 | 25 | 7 | 26 | 5 | 25 | 4 | 24 | | 30 | 25 |
|
>35 | 8 | 14 | 3 | 11 | 1 | 5 | 5 | 29 | | 18b | 14 |
| Comorbidity | | | | | | | | | 0.023 | | |
|
Yes | 47 | 83 | 17 | 63 | 10 | 50 | 10 | 59 | | 85b | 71 |
|
No | 10 | 17 | 10 | 37 | 10 | 50 | 7 | 41 | | 37 | 29 |
| Smoking | | | | | | | | | 0.365 | | |
|
Yes | 6 | 11 | 6 | 22 | 1 | 5 | 2 | 12 | | 15 | 12 |
|
No | 51 | 89 | 21 | 78 | 19 | 95 | 15 | 88 | | 107b | 88 |
Logistic regression analysis demonstrated that
leiomyosarcoma or carcinosarcoma types (poor prognosis) were
significantly associated with a mean age of 50 years or higher and
with menopause status. These types of cancer were also associated
with a comorbidity as determined by univariate analysis. Menopause
was significantly associated with the sarcoma cases as demonstrated
by the multivariate regression analysis (OR 5.45; 95% CI
2.40-12.38; P<0.001).
Staging and management of the
sarcomas
The sarcomas were diagnosed at Stage I and IV in 44
and 22% of the cases, respectively. The stage distribution by
histological type is shown in Table
III.
| Table IIIDistribution of 122 cases of uterine
sarcomas managed between 2001 and 2016 according to the FIGO
staging system. |
Table III
Distribution of 122 cases of uterine
sarcomas managed between 2001 and 2016 according to the FIGO
staging system.
| |
Uterine
sarcomas by histological type |
|---|
| | CCS (n=57) | LMS (n=27) | ESS (n=20) | ADS (n=17) | Total
(n=122)b |
|---|
| Stage | n | % | n | % | n | % | n | % | n | % |
|---|
| I | | | | | | | | | | |
|
Ia | 10 | 18 | 1 | 4 | 6 | 30 | 5 | 29 | 22 | 18 |
|
Ib | 6 | 10 | 10 | 37 | 6 | 30 | 9b | 53 | 32a | 26 |
| II | 4 | 7 | 4 | 15 | 4 | 20 | 1 | 6 | 13 | 11 |
| III | | | | | | | | | | |
|
IIIa | 4 | 7 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 3 |
|
IIIb | 13 | 23 | 1 | 4 | 1 | 5 | 0 | 0 | 15 | 12 |
|
IIIc | 6 | 10 | 2 | 7 | 1 | 5 | 1 | 6 | 10 | 8 |
| IV | | | | | | | | | | |
|
IVa | 2 | 4 | 1 | 4 | 0 | 0 | 0 | 0 | 3 | 3 |
|
IVb | 12 | 21 | 8 | 29 | 2 | 10 | 1 | 6 | 23 | 19 |
The hysterectomy surgery was the first treatment for
95 (78%) patients and was performed with retroperitoneal
lymphadenectomy in 19 patients (14 cases of carcinosarcoma) and
radiotherapy and/or chemotherapy in 75 cases (ranging from 59 to
66% per histological type). The optimal control of the disease
(complete surgical resection and/or complete clinical response) was
achieved in 58% of the cases (55/95). Following stratification
according to the type of sarcoma, this optimal control was
increased to 71% for the adenosarcoma cases, to 67% for the ESSs,
to 37% for the leiomyosarcoma patients and to 33% for the
carcinosarcoma subjects.
Sarcomas recurrence and survival over
time
Relapses occurred in 36% (20/55) of the subjects who
reached initial complete disease control. The relapses occurred in
the first 12 months in 13 cases and within 36 months in 18 cases. A
total of 11 cases were distant metastases. A late relapse was noted
after 91 months of follow up, which involved a subcutaneous tissue
metastasis (abdominal wall) in a woman with an ESS of low grade,
Stage II, and initially managed with surgery and radiotherapy.
A total of 27 women (22%) were unable to perform
surgery upfront. This was predominantly noted in the carcinosarcoma
cases (32%) compared to 12 and 15% noted for the other types of
sarcomas. However, the differences were not significant (P=0.108).
Out of these patients, 21 received initial radiotherapy and/or
chemotherapy (without surgery) and there was only one case (2%)
with complete clinical response.
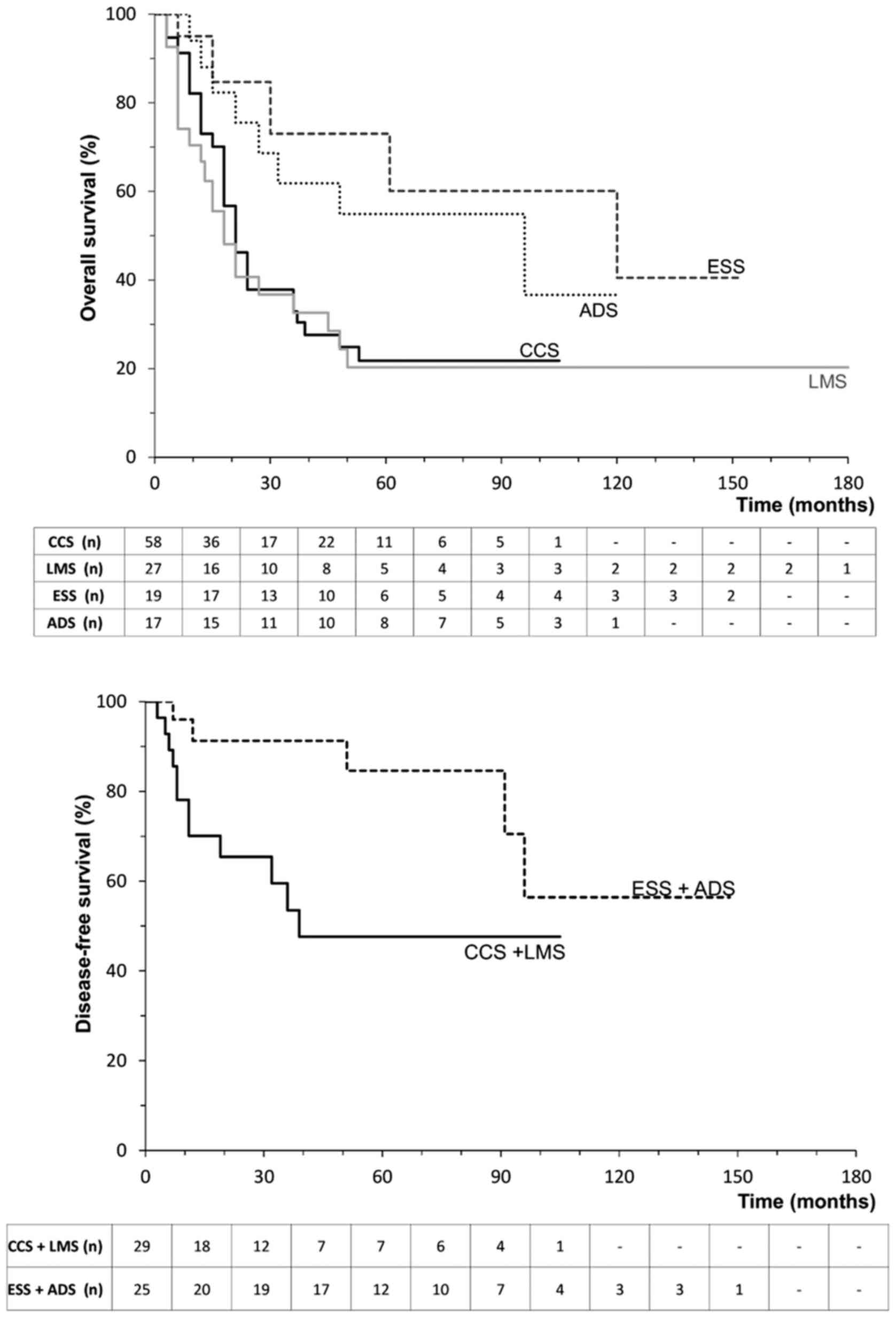
Longitudinal analysis resulted in an OS rate of 76%
in 12 months and 33% in five years. Further analysis performed
according to the histological type demonstrated that the ESSs and
adenosarcomas exhibited an OS rate of 88-90% in 12 months and of
55-61% in five years. In comparison, carcinosarcomas and
leiomyosarcomas presented the worst results with a 5-year OS of
20-22% (P=0.003; Fig. 1). The
disease-free survival rate was 66% for all cases with disease
control at the first treatment. This rate was altered from 48% in
five years for the carcinosarcoma plus leiomyosarcoma group to 85%
for the ESS plus adenosarcoma group (P=0.022; Fig. 1).
During the end of the follow-up period, only 25%
(31/122) of the women remained disease-free and survived and 57%
(69/122) were deceased due to disease progression. These statistics
were higher for leiomyosarcoma (78%) and carcinosarcoma (61%)
compared with those noted for ESS (30%) and adenosarcoma (41%)
(P=0.005).
Discussion
Uterine sarcomas have accounted for 10% of uterine
corpus malignancies from 2001-2016. An increasing trend for new
cases has been noted for these malignancies, mainly for
histological types, such as carcinosarcoma, ESS and adenosarcoma.
The increasing number of the cases and the higher proportion of
sarcomas observed in comparison to the lower incidence described
previously (range 3-7%) (3,13) may be associated with a higher rate
of severe case referrals to reference centers (10).
With regard to diagnosis, 77% of cases exhibited
abnormal uterine bleeding as an ‘early’ symptom despite the
perception that uterine sarcoma is a fast-growing tumor with a
pelvic mass. Abnormal uterine bleeding was observed for all
histological types and may reflect a delay in diagnosis, resulting
in advanced-stage disease and additional bleeding.
The main prevalent histological types were those
with a poor prognosis, such as carcinosarcomas (47%) and
leiomyosarcomas (22%) compared to ESSs (16%) and adenosarcomas
(14%). In general, uterine sarcomas predominated in patients over
60 years of age, explaining the high proportion of postmenopausal
women and of those with comorbidities. It is noteworthy that 46% of
carcinosarcomas occurred in women older than 70 years, whereas no
case under 50 years of age was noted. 26% of leiomyosarcomas and
45% of ESSs occurred before 50 years of age (P<0.0001). These
findings are in accordance with recent studies indicating that ESS
predominates in the age group of 40-50 years (14-16).
Multivariate regression analysis demonstrated 5-fold
increased risk for the incidence of carcinosarcomas and
leiomyosarcomas in subjects that were on menopause. These results
confirm the association between increased age and risk of sarcomas.
However, it remains to be established whether menopause is a risk
factor for sarcomas (17,18), despite the evidence suggesting that
hormonal changes may cause modifications in mitotic activity and
uterine cell morphology (19).
Despite a lack of significant association, all
histological types exhibited a high rate of multiparity (>50%
with three or more deliveries). In contrast to this finding, 23% of
nulliparity was noted for carcinosarcomas and a history of smoking
was present in 22% of patients with leiomyosarcoma that occurred in
less than 12% of other tumor types. Currently, insufficient
evidence is present regarding the association of smoking with
sarcoma and conflicting data have been reported. A German study of
143 women demonstrated that 12% of carcinosarcomas were from
patients who were smokers, whereas this percentage was increased to
16% in leiomyosarcomas and to 28% in ESSs. A lower OS was noted in
smokers (20).
The main prognostic factors for uterine sarcomas are
stage and adequate initial approach by surgery (5,14,21). A
relatively low proportion was noted for stage I sarcomas (44%),
which was similar to the results reported by a Norwegian study of
1,042 cases (22). Furthermore,
Stage I was the predominant stage noted in ESSs (60%) and
adenosarcomas (82%), while 33% of leiomyosarcomas and 25% of
carcinosarcomas were classified as Stage IV, probably related to
histological type aggressiveness (P=0.0001). Similar findings were
noted for leiomyosarcomas in an American study with 219 patients
diagnosed with the disease from 1982 to 2005. 35% of these cases
were classified as Stage IV tumors (23).
Surgery is considered a standard therapeutic
approach for sarcomas and a hysterectomy was performed for 78% of
the patients in the present study. It is important to note that 62%
of these cases also received adjuvant therapy, which was not
associated with the histological type. However, it has been
reported that additional therapeutic interventions may yield
controversial results (20,24). In the present study, only 1 out of
21 patients treated primarily with radiotherapy and/or chemotherapy
without surgery, exhibited a satisfactory clinical response,
highlighting the poor response of these cases to the standard
radiotherapy treatment, which has been previously shown (14,21,25).
An additional factor, which was indicative of the aggressiveness of
sarcomas and possibly of the delay for diagnosis and management,
was the lack of treatment noted in the six untreated cases, which
was due to the advanced stage of the disease. A total of 5 out of
these 6 cases were carcinosarcomas.
The low OS rate observed was reduced from 76% in 12
months to 33% in five years confirming the poor prognosis of
uterine sarcomas. The formation of two different groups according
to prognosis was evident. This was defined by the different
histological types as follows: The first group included the ESS and
adenosarcoma and exhibited a high 5-year OS rate (55-61%), whereas
the second group was composed of carcinosarcoma and leiomyosarcoma
cases, which were more aggressive and led to poor outcomes and
reduced 5-year OS rate (20%, P=0.003).
Similar findings were reported by several studies
with regard to the 5-year OS rate and the histological subtype. A
percentage range of 40-46 and 30-45% has been reported for
leiomyosarcomas carcinosarcomas, respectively. In contrast to these
findings, the range and percentage was estimated to 86-97% for ESSs
and to 69% for adenosarcomas, respectively (20,26-28).
The rates reported in the present study were lower than those
previously published. These low survival rates were noted for all
histological types and may reflect the limited treatment modalities
available, the rapid progression of the disease and the delay to
the diagnosis and treatment. The latter is a common disadvantage
noted in the Brazilian public health system. The increase of the
time required for management of an aggressive sarcoma may reduce
the low OS rate of the patients.
Among 55 women that achieved remission, 20 women
exhibited recurrences (36%), of which 18 cases recurred in 36
months. Distant metastases were noted in 11 cases. The main sites
of metastasis were the lungs (n=4 cases) and the bones (n=3 cases).
These findings were in agreement with those noted in previous
reports (14,29). Disease-free survival followed the OS
pattern for two distinct histological types, with the ESS and
adenosarcoma group exhibiting a 5-year survival rate of 85%,
against 48% for the second group (carcinosarcoma and
leiomyosarcoma, P=0.022).
The limitations of this study include the small
number of cases and its retrospective nature. A certain levels of
bias existed regarding patient selection from a cancer center and
the temporal alteration of the population access could explain the
higher prevalence of tumors with a poor prognosis. In contrast to
these findings, the advantage of the present study was the
appropriate selection of the institution in which the subjects were
treated, which included a predefined protocol for staging,
treatment, and follow-up, with accurate information recorded, and a
minimal loss of follow-up observed (one patient).
In conclusion, the present study demonstrated that
the rate of treated uterine sarcoma cases had increased from 2001
to 2016, mainly due to the incidence of different histological
types, such as carcinosarcoma, ESS and adenosarcoma, and were
predominant in women over 60 years of age and diagnosed in advanced
stages. Postmenopause was associated with histological types of
poorer prognosis, such as carcinosarcoma and leiomyosarcoma. A low
5-year OS rate was noted and estimated to 33%, which was lower than
expected. The survival rate was worse low for carcinosarcoma and
leiomyosarcoma. Recurrences occurred in one-third of cases, usually
in the first three years following diagnosis. Approximately 50% of
these recurrences were distant metastases. The improvement of the
women public health care system and a faster investigation of
symptomatic postmenopausal cases are crucial in order to achieve
early diagnosis and reduce the unfavorable outcomes observed for
uterine sarcomas.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
TBDSFP contributed to the conception and design of
this study, acquisition of data, interpretation of data, and
drafting the manuscript. ECC contributed to the conception and
design of this study, data revision, and drafting the manuscript.
LFD contributed to the acquisition of data and data revision. MCST
contributed to the conception and design of this study and
interpretation of data. DBV contributed to the methodology
development and interpretation of data. JCT contributed to the
conception and design of this study, acquisition of data, analysis
and interpretation of data, drafting the manuscript, and general
supervision. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was developed in compliance with
Resolution 466/12 of the Brazilian National Health Council and
Declaration of Helsinki and was previously approved by the Research
Ethics Committee of Unicamp (approval no. 1.760.085, October 4,
2016), which waived the requirement for informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Singh N and Gilks CB: The changing
landscape of gynaecological cancer diagnosis: Implications for
histopathological practice in the 21st century. Histopathology.
70:56–69. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tropé CG, Abeler VM and Kristensen GB:
Diagnosis and treatment of sarcoma of the uterus. A review. Acta
Oncol. 51:694–705. 2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ghirardi V, Bizzarri N, Guida F, Vascone
C, Constantini B, Scambia G and Fagotti A: Role of surgery in
gynaecological sarcomas. Oncotarget. 10:2561–2575. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Giuntoli RL 2nd, Metzinger DS, DiMarco CS,
Cha SS, Sloan JA, Keeney GL and Gostout BS: Retrospective review of
208 patients with leiomyosarcoma of the uterus: Prognostic
indicators, surgical management, and adjuvant therapy. Gynecol
Oncol. 89:460–469. 2003.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hoang L, Chiang S and Lee CH: Endometrial
stromal sarcomas and related neoplasms: New developments and
diagnostic considerations. Pathology. 50:162–177. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kurman RJ, Carcangiu ML, Herrington CS and
Young RH (eds): WHO Classification of Tumours of Female
Reproductive Organs. 4th edition. IARC Press, Lyon, pp135-147,
2014.
|
|
8
|
Oliva E: Cellular mesenchymal tumors of
the uterus: A review emphasizing recent observations. Int J Gynecol
Pathol. 33:374–384. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Prat J: FIGO staging for uterine sarcomas.
Int J Gynaecol Obstet. 104:177–178. 2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ueda SM, Kapp DS, Cheung MK, Shin JY,
Osann K, Husain A, Teng NN, Berek JS and Chan JK: Trends in
demographic and clinical characteristics in women diagnosed with
corpus cancer and their potential impact on the increasing number
of deaths. Am J Obstet Gynecol. 198(218)2008.PubMed/NCBI View Article : Google Scholar
|
|
11
|
World Health Organization: International
Statistical Classification of Diseases and Related Health Problems
10th Revision. ICD-10 version 2015. Available at: urihttps://icd.who.int/browse10/2015/ensimplehttps://icd.who.int/browse10/2015/en.
|
|
12
|
FIGO Committee on Gynecologic Oncology.
FIGO staging for carcinoma of the vulva, cervix, and corpus uteri.
Int J Gynecol Obstet. 125:97–98. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Koivisto-Korander R, Martinsen JI,
Weiderpass E, Lemnen A and Pukkala E: Incidence of uterine
leiomyosarcoma and endometrial stromal sarcoma in nordic countries:
Results from NORDCAN and NOCCA databases. Maturitas. 72:56–60.
2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Mbatani N, Olawaiye EA and Prat J: Uterine
sarcomas. Int J Gynecol Obstet. 143:51–58. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Felix AS, Cook LS, Gaudet MM, Rohan TE,
Schouten LJ, Setiawan VW, Wise LA, Anderson KE, Bernstein L, De
Vivo I, et al: The etiology of uterine sarcomas: A pooled analysis
of the epidemiology of endometrial cancer consortium. Br J Cancer.
108:727–734. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zhang YY, Li Y, Qin M, Cai Y, Jin Y and
Pan LY: High-grade endometrial stromal sarcoma: A retrospective
study of factors influencing prognosis. Cancer Manag Res.
11:831–837. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ishidera Y, Yoshida H, Oi Y, Katayama K,
Miyagi E, Hayashi H and Shigeta H: Analysis of uterine corporeal
mesenchymal tumors occurring after menopause. BMC Women Health.
19(13)2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Koivisto-Korander R, Butzow R, Koivisto AM
and Leminen A: Clinical outcome and prognostic factors in 100 cases
of uterine sarcoma: Experience in helsinki university central
hospital 1990-2001. Gynecol Oncol. 111:74–81. 2008.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Oliva E: Practical issues in uterine
pathology from banal to bewildering: The remarkable spectrum of
smooth muscle neoplasia. Mod Pathol. 29 (Suppl 1):S104–S120.
2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Burghaus S, Halmen S, Gass P, Mehlhorn G,
Schrauder MG, Lux MP, Renner SP, Beckmann MW, Hein A and Thiel FC:
Outcome and prognosis in uterine sarcoma and malignant mixed
mullerian tumor. Arch Gynecol Obstet. 294:343–351. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Menczer J: Review of recommended treatment
of uterine carcinoma. Curr Treat Options Oncol.
16(53)2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Nordal RR and Thoresen SO: Uterine
sarcomas in Norway 1956-1992: Incidence, survival and mortality.
Eur J Cancer. 33:907–911. 1997.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Zivanovic O, Leitao MM, Iasonos A, Jacks
LM, Zhou Q, Abu-Rustum NR, Soslow RA, Juretzka MM, Chi DS, Barakat
RR, et al: Stage-specific outcomes of patients with uterine
leiomyosarcoma: A comparison of the international federation of
gynecology and obstetrics and american joint committee on cancer
staging systems. J Clin Oncol. 27:2066–2072. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Wada H, Enomoto T, Fujita M, Yoshino K,
Nakashima R, Kurachi H, Haba T, Wakasa K, Shroyer KR, Tsujimoto M,
et al: Molecular evidence that most but not all carcinosarcomas of
the uterus are combination tumors. Cancer Res. 57:5379–5385.
1997.PubMed/NCBI
|
|
25
|
Nusrath S, Bafna S, Rajagopalan R,
Thammineedi SR, Raju KVV, Patnaik SC, Pawar S, Reddy Y, Chavali RN
and Murthy SS: Uterine sarcomas: Experience from a tertiary cancer
care center from India. Indian J Surg Oncol. 10:342–349.
2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Şükür YE, Taşkın S, Varlı B, Ateş C,
Güngör M and Ortaç F: Prognostic factors for disease-free and
overall survival of patients with uterine carcinosarcoma. Int J
Clin Oncol. 23:114–120. 2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Bernard B, Clarke BA, Malowany JI,
McAlpine J, Lee CH, Atenafu EG, Ferguson S and Mackay H: Uterine
adenosarcomas: A dual-institution update on staging, prognosis and
survival. Gynecol Oncol. 131:634–639. 2013.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Pietzner K, Buttmann-Schweiger N, Sehouli
J and Kraywinkel K: Incidence patterns and survival of
gynecological sarcoma in Germany: Analysis of population-based
cancer registry data on 1066 women. Int J Gynecol Cancer.
28:134–138. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
D'Angelo E and Prat J: Uterine sarcomas: A
review. Gynecol Oncol. 116:131–139. 2010.PubMed/NCBI View Article : Google Scholar
|