Introduction
Undifferentiated small-cell sarcomas are soft tissue
malignancies which are characterized by small, round to ovoid
cytomorphology with a high nuclear/cytoplasmic ratio. The most
frequent one is Ewing sarcoma, which is characterized by EWS RNA
binding protein 1 (EWSR1)-erythroblast
transformation-specific (ETS) gene fusions, and others
without theses fusions are called ‘Ewing-like sarcomas’. Based on
the discovery of novel molecular driving events, recent studies
have enabled the identification of two distinct subgroups, these
are, capicua transcriptional repressor (CIC)-rearranged
sarcoma and BCL6 corepressor (BCOR)-rearranged sarcoma,
within this previously uncharacterized group of Ewing-like sarcomas
(1,2). In CIC-rearranged sarcoma,
CIC is fused to double homeobox 4 (DUX4) with either
t(4;19)(q35;q13.1) or t(10;19)(q26.3;q13) translocation, which are
associated with oncogenesis, tumor development, and metastatic
capability (1,3,4). On
the other hand, BCOR is fused to mainly cyclin B3
(CCNB3) (5). These entities
have different clinicopathological features. Of note,
CIC-rearranged sarcomas are associated with an aggressive
clinical course and poor prognosis compared to Ewing sarcoma
(3). Median overall survival of
patients with metastatic CIC-rearranged sarcoma is only 9-10
months (6,7). The efficacy of chemotherapy has not
been prospectively evaluated, and no standard treatment has been
established (7,8). Compared to CIC-rearranged
sarcomas, BCOR-rearranged sarcomas have a much better
prognosis (5,7), although no standard treatment for
these tumors has been established either.
Here, we describe a case of metastatic
CIC-rearranged sarcoma which developed years after
chemotherapy for lymphoma that included alkylating agents and
anthracycline, and was palliated with chemotherapy used for Ewing
sarcoma.
Case report
The patient was a 24-year-old Japanese woman who had
a past medical history of anaplastic large cell lymphoma at nine
years old, treated with chemotherapy based on the ACLC99 protocol
(9) and JACLS NHL-98 protocol
(10), with subsequent autologous
hematopoietic stem cell transplantation. These protocol regimens
included cytotoxic drugs such as alkylating agents and
anthracyclines. The cumulative dose of doxorubicin (DOX) was 150
mg/m2. She had been in long-term complete remission.
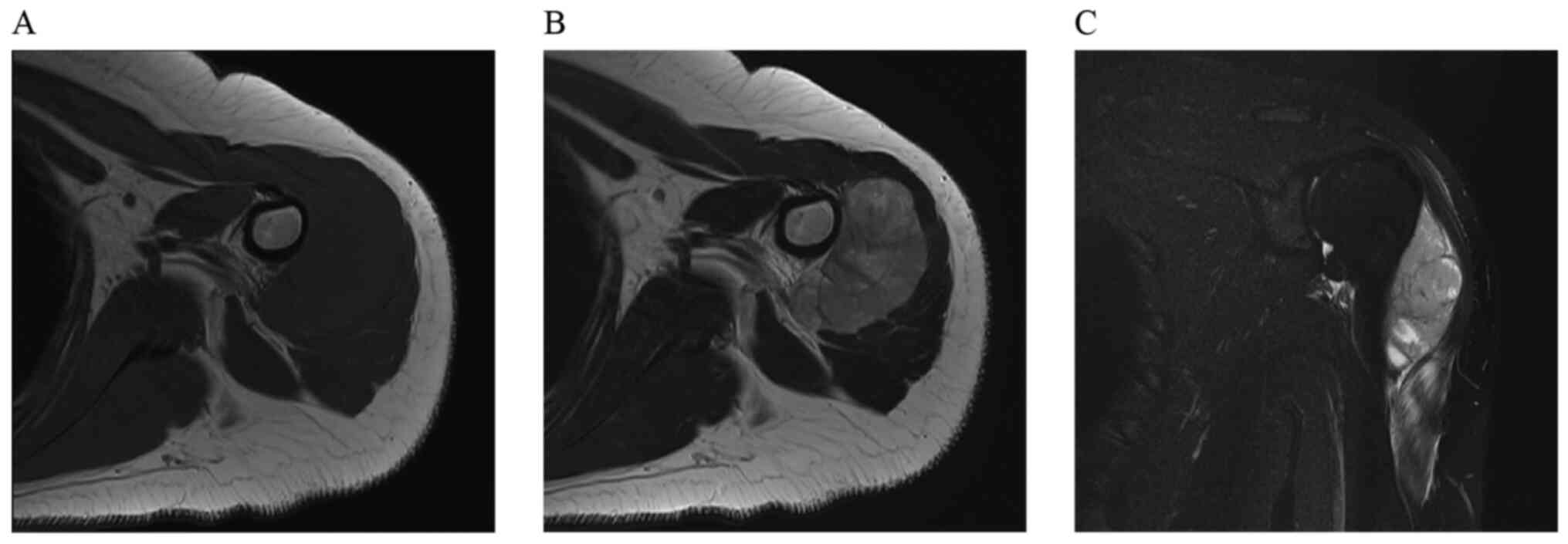
She was referred to our hospital after presenting
with pain and swelling of the left shoulder in May 2018. A magnetic
resonance imaging (MRI) scan of the left shoulder revealed a 5 cm
soft tissue mass located between the deltoid and humerus (Fig. 1A-C). Open biopsy was performed.
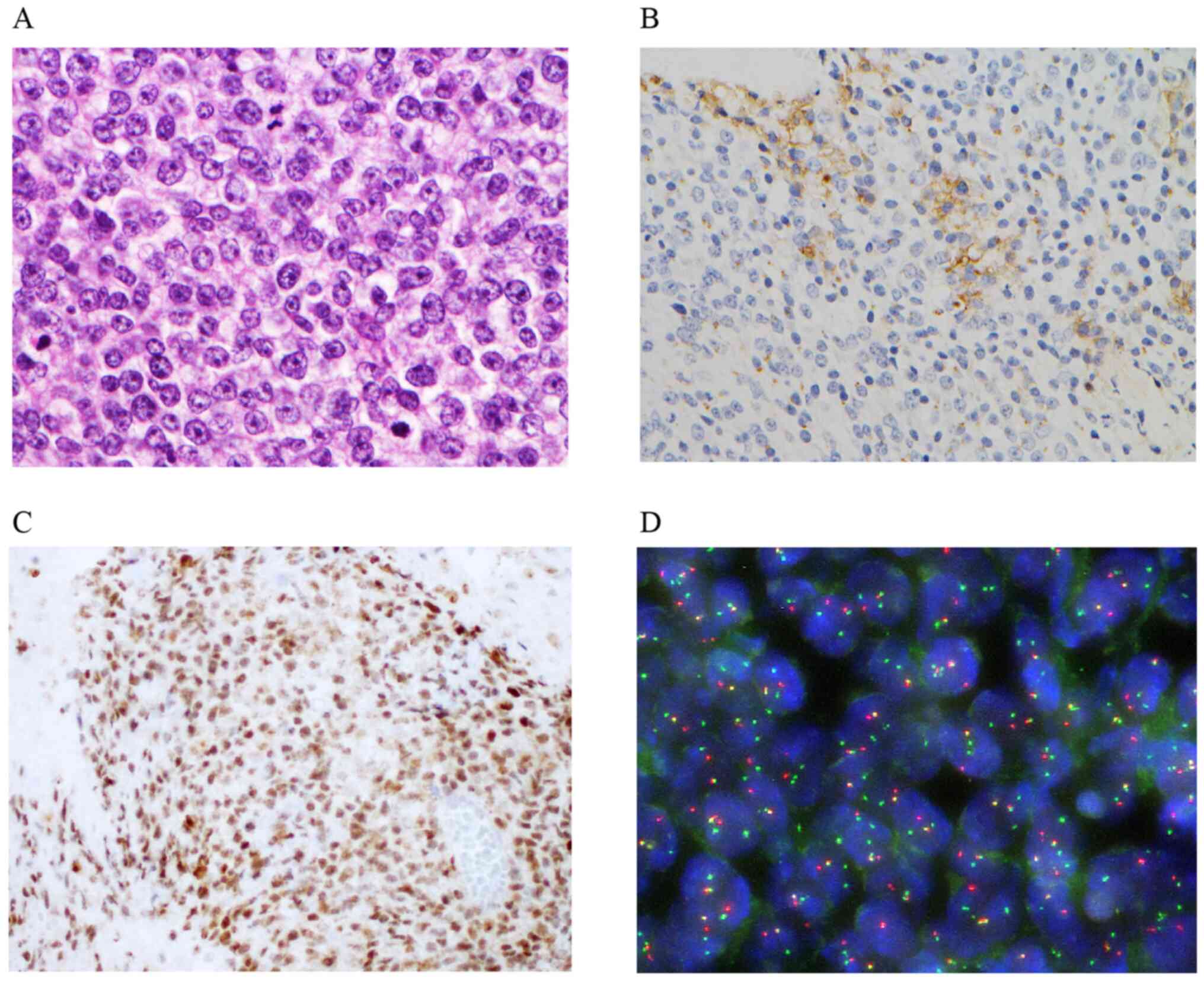
Small round atypical cells with a high nuclear/cytoplasmic ratio
grew in sheets (Fig. 2A) and formed
alveolar structures with necrosis and fibrosis.
Immunohistochemically, tumor cells were positive for WT-1,
calretinin and ETS variant transcription factor 4 (ETV4), and
focally positive for CD99 (Fig. 2B
and C). Fluorescence in situ
hybridization demonstrated CIC rearrangement (Fig. 2D). Based on these findings, the
tumor was diagnosed as CIC-rearranged sarcoma. Detail of
fusion partner did not be studied. CT scan revealed multiple
nodules in the lungs, which were consistent with metastases.
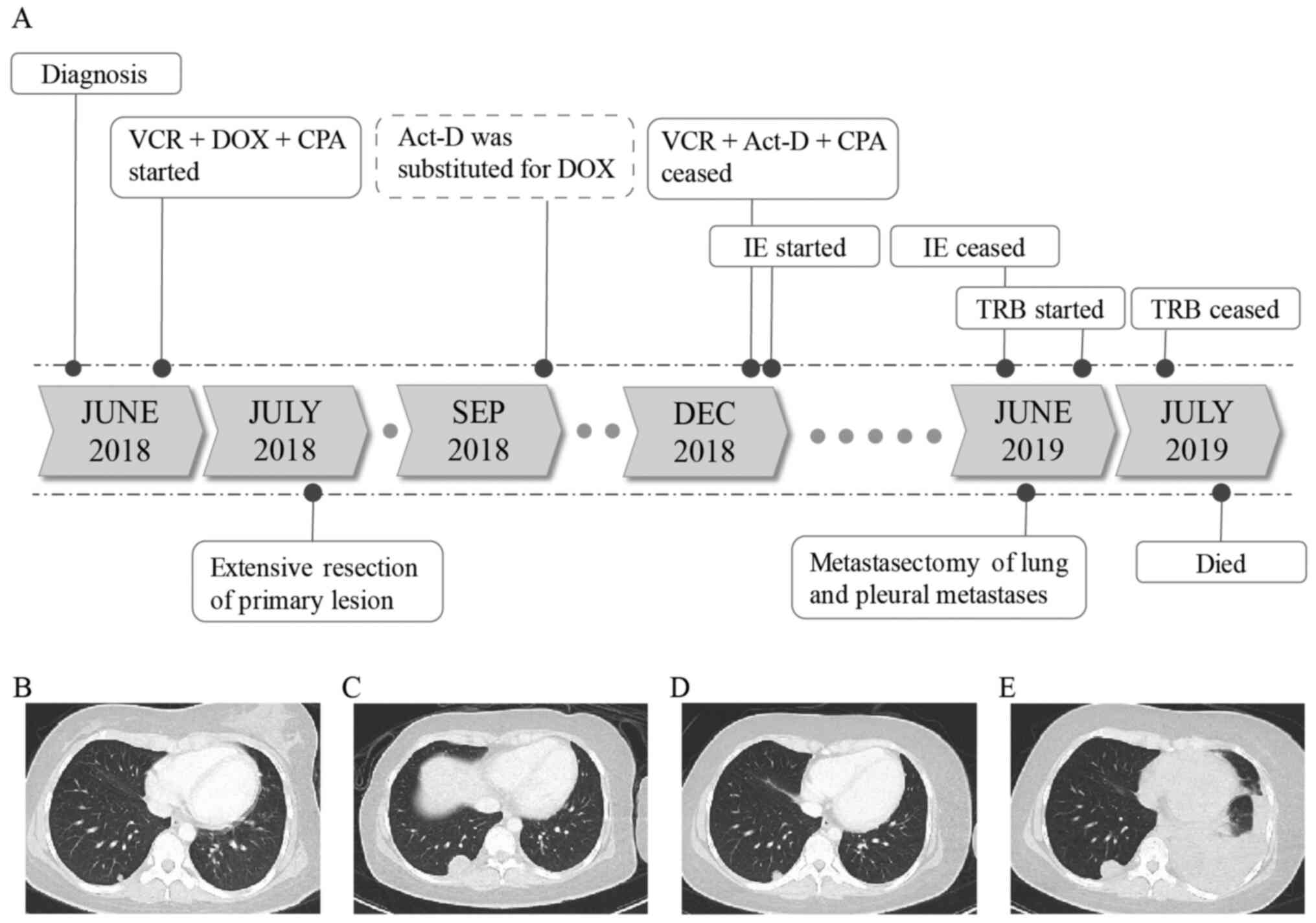
The clinical course is summarized in Fig. 3A. First-line palliative chemotherapy
with DOX, vincristine (VCR), and cyclophosphamide (CPA) was
initiated in June 2018 (Fig. 3B).
After the first cycle, the lung metastases had shrunk, but the
primary lesion had not changed. The patient underwent a wide
resection of the primary lesion with replacement using artificial
humeral head in July 2018 to improve her quality of life.
Pathological response to initial chemotherapy was poor. DOX, VCR,
and CPA were restarted. At the end of the third cycle, her
cumulative lifetime exposure of DOX had reached 350
mg/m2. We substituted actinomycin-D (Act-D) for DOX
beginning with the fourth cycle to avoid cardiotoxicity (11). The CIC-rearranged sarcoma was
well-controlled during six cycles, although adverse events
occurred, including grade 3 febrile neutropenia and septic
arthritis requiring debridement. Six months from the beginning of
therapy, progression of the lung metastases developed (Fig. 3C).
We administered ifosfamide and etoposide as
second-line treatment. We planned 1,800 mg/m2 of
ifosfamide per day for five days and 100 mg/m2 of
etoposide per day over the same five days every three weeks. Two
cycles of IE achieved a good response in the lung metastases as
seen on CT scan; this response lasted for 4 months (Fig. 3D). However, persistent grade 2
anorexia due to chemotherapy impaired her quality of life. In
addition, some evidences have suggested that pulmonary
metastasectomy may be associated with clinical benefit (12,13).
As extrapulmonary metastases had not appeared, after careful
discussion among the multidisciplinary team and the patient, we
planned a pneumonectomy for pulmonary oligometastases for
improvement of prognosis and quality of life with subsequent
chemotherapy holiday after 5 cycles of IE. Despite rapid
progression of the lung metastases, with a left pleural effusion
appearing right before surgery (Fig.
3E), pneumonectomy and maximum debulking of the pleural
metastases were performed. However, not all residual disease could
be resected.
Following surgery, an aggressive clinical course was
maintained. As rapidly progressive malignant pleural effusion
developed, pleurodesis was performed. Although we started
trabectedin (TRB) as third-line therapy, no clinical benefit was
observed. She died one month later. Her overall survival from
diagnosis was 13 months.
Discussion
No molecular-based targeted therapy or cancer
immunotherapy for the treatment of CIC-rearranged sarcomas
has been reported, and chemotherapy with cytotoxic agents is still
generally used. The available data on treatment for metastatic
CIC-rearranged sarcoma come from small retrospective
studies. Because of the low incidence and variations in treatment,
some cases were formerly diagnosed and treated as other sarcomas
without pathognomonic molecular analysis (6,7,14).
Palmerini et al reported that in first-line settings for
metastatic CIC-rearranged sarcoma, response rates to a Ewing
regimen and another regimen (DOX and ifosfamide, unknown regimen)
were 57% (n=8/14) and 0% (n=0/4), respectively (8). In addition, neoadjuvant chemotherapy
with Ewing regimen achieved pathological response in 3 of 10
localized CIC-rearranged sarcoma (6). These findings suggest that
chemotherapy with the Ewing regimens seems to be effective for
patients newly diagnosed with metastatic CIC-rearranged
sarcoma, albeit that further studies are warranted.
IE is an effective regimen for treatment of
recurrent Ewing sarcoma (15). This
regimen is not widely used in treatment for advanced soft tissue
sarcoma (16,17), although minimum activity has been
reported in small phase 2 trial (18). IE is commonly used with DOX, VCR,
and CPA (VDC-IE) for treatment of localized Ewing sarcoma based on
the results of a randomized phase 3 trial, but the same trial
revealed that VDC-IE did not improve the outcome for patients with
metastatic disease (19). Thus, we
did not use VDC-IE in our first-line palliative treatment but did
use it for second-line treatment. To our knowledge, this is the
first case with a response to an IE regimen without DOX for
refractory CIC-rearranged sarcoma. Unfortunately, the
patients showed poor prognosis regardless palliative chemotherapy.
However, Ewing regimens, especially IE regimen achieved clinically
meaningful disease control in this case, considering to highly
aggressive clinical course after IE regimen failure.
There is no established treatment for Ewing sarcoma
refractory to both DOX, VCR, and CPA and to IE. TRB, a
tetrahydroisoquinoline alkaloid, showed anti-tumor activity in
CIC-rearranged sarcoma in a xenograft model (4). Preclinical and clinical studies have
shown that TRB has an anti-tumor effect in several
translocation-related sarcomas (20-22).
Therefore, we used TRB as third-line palliative therapy based on
these findings, but saw no clinical benefit. Interestingly, TRB did
not demonstrate sufficient activity against relapsed Ewing sarcoma
in a phase 2 trial (23). Of ten
evaluable patients, there were no partial responses, one case of
stable disease, and nine cases of progressive disease. Based on the
above, the clinical response to chemotherapy in our case was
concordant with the clinical chemosensitivity of Ewing sarcoma.
Our case is the first report of secondary
CIC-rearranged sarcoma. Secondary sarcoma associated with
prior chemotherapy is well known. Various treatment-related factors
are associated with the development of secondary sarcoma, including
exposure to alkylating agents and/or anthracyclines and a history
of autologous hematopoietic stem cell transplantation (24,25).
Most secondary sarcoma belong to the category with non-recurring
genetic aberrations, including undifferentiated pleomorphic
sarcoma, osteosarcoma, and malignant peripheral nerve sheath tumor
(26). Ewing sarcoma accounts for
only 5% of secondary sarcomas (24). However, CIC-rearranged
sarcoma could have been overlooked in cases where pathognomonic
molecular analysis was not performed. It is uncertain whether the
clinical outcome differs between primary and secondary
CIC-rearranged sarcoma. In our case, the previous treatment
history restricted the use of DOX because of the patient's
cumulative exposure.
In conclusion, we describe a case of metastatic
CIC-rearranged sarcoma treated with palliative chemotherapy,
beginning with an Ewing regimen, both VDC and IE. Our case and the
best available clinical evidence suggest that treatment with Ewing
regimens is a reasonable option for patients with metastatic
CIC-rearranged sarcomas, including second malignant
case.
Acknowledgements
The authors would like to thank Dr. Akihiko Yoshida
(Department of Diagnostic Pathology, National Cancer Center
Hospital) for his important contributions to the pathological
diagnosis.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SK and YI made substantial contributions to the
conception and design of the study. SK, YI, NK, HT, SM, TKo TH, MK,
TKa, and HH substantial contributions to the acquisition of the
data. SK and YI confirmed the authenticity of the raw data and
drafted the manuscript. YFuj, YFun, MT and HM made substantial
contributions to the analysis and interpretation of the data and
were involved in revising the manuscript critically for important
intellectual content. TH and MK contributed pathological diagnosis.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of the clinical data and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kawamura-Saito M, Yamazaki Y, Kaneko K,
Kawaguchi N, Kanda H, Mukai H, Gotoh T, Motoi T, Fukayama M,
Aburatani H, et al: Fusion between CIC and DUX4 up-regulates PEA3
family genes in Ewing-like sarcomas with t(4;19)(q35;q13)
translocation. Hum Mol Genet. 15:2125–2137. 2006.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Puls F, Niblett A, Marland G, Gaston CL,
Douis H, Mangham DC, Sumathi VP and Kindblom LG: BCOR-CCNB3
(Ewing-like) sarcoma: A clinicopathologic analysis of 10 cases, in
comparison with conventional Ewing sarcoma. Am J Surg Pathol.
38:1307–1318. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Haidar A, Arekapudi S, DeMattia F, Abu-Isa
E and Kraut M: High-grade undifferentiated small round cell sarcoma
with t(4;19)(q35;q13.1) CIC-DUX4 fusion: Emerging entities of soft
tissue tumors with unique histopathologic features-a case report
and literature review. Am J Case Rep. 16:87–94. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yoshimoto T, Tanaka M, Homme M, Yamazaki
Y, Takazawa Y, Antonescu CR and Nakamura T: CIC-DUX4 induces small
round cell sarcomas distinct from ewing sarcoma. Cancer Res.
77:2927–2937. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kao YC, Owosho AA, Sung YS, Zhang L,
Fujisawa Y, Lee JC, Wexler L, Argani P, Swanson D, Dickson BC, et
al: BCOR-CCNB3 fusion positive sarcomas: A clinicopathologic and
molecular analysis of 36 cases with comparison to morphologic
spectrum and clinical behavior of other round cell sarcomas. Am J
Surg Pathol. 42:604–615. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Antonescu CR, Owosho AA, Zhang L, Chen S,
Deniz K, Huryn JM, Kao YC, Huang SC, Singer S, Tap W, et al:
Sarcomas with CIC-rearrangements are a distinct pathologic entity
with aggressive outcome: A clinicopathologic and molecular study of
115 cases. Am J Surg Pathol. 41:941–949. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Endo M, Sugawara M, Yoshida A, Kobayashi
E, Shimoi T, Kodaira M, Yunokawa M, Yonemori K, Tamura K, Toki S,
et al: 1173-CIC-rearranged sarcoma and BCOR-CCNB3 sarcoma: Clinical
characteristics and treatment results of the newly-established
‘Ewing sarcoma-like’ small round cell sarcomas. Ann Oncol. 27
(Suppl 9):ix163–ix168. 2016.
|
|
8
|
Palmerini E, Gambarotti M, Ratan R, DuBois
S, Nathenson MJ, Italiano A, de Alava E, Jones RL, Provenzano S,
Grignani G, et al: Graceful Project: A global collaboration on
CIC-DUX4, BCOR-CCNB3, high grade undifferentiated round cell
sarcoma (URCS). In: Proceedings of the CTOS Annual Meeting, Tokyo,
Japan, 2019.
|
|
9
|
Brugieres L, Le Deley MC, Rosolen A,
Williams D, Horibe K, Wrobel G, Mann G, Zsiros J, Uyttebroeck A,
Marky I, et al: Impact of the methotrexate administration dose on
the need for intrathecal treatment in children and adolescents with
anaplastic large-cell lymphoma: Results of a randomized trial of
the EICNHL group. J Clin Oncol. 27:897–903. 2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fujita N, Kobayashi R, Takimoto T,
Nakagawa A, Ueda K and Horibe K: Results of the Japan association
of childhood leukemia study (JACLS) NHL-98 protocol for the
treatment of B-cell non-Hodgkin lymphoma and mature B-cell acute
lymphoblastic leukemia in childhood. Leuk Lymphoma. 52:223–229.
2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Bristow MR, Mason JW, Billingham ME and
Daniels JR: Doxorubicin cardiomyopathy: Evaluation by
phonocardiography, endomyocardial biopsy, and cardiac
catheterization. Ann Intern Med. 88:168–175. 1978.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Predina JD, Puc MM, Bergey MR, Sonnad SS,
Kucharczuk JC, Staddon A, Kaiser LR and Shrager JB: Improved
survival after pulmonary metastasectomy for soft tissue sarcoma. J
Thorac Oncol. 6:913–919. 2011.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Schur S, Hoetzenecker K, Lamm W, Koestler
WJ, Lang G, Amann G, Funovics P, Nemecek E, Noebauer I, Windhager
R, et al: Pulmonary metastasectomy for soft tissue sarcoma-report
from a dual institution experience at the Medical University of
Vienna. Eur J Cancer. 50:2289–2297. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yoshida A, Goto K, Kodaira M, Kobayashi E,
Kawamoto H, Mori T, Yoshimoto S, Endo O, Kodama N, Kushima R, et
al: CIC-rearranged sarcomas: A study of 20 cases and comparisons
with Ewing sarcomas. Am J Surg Pathol. 40:313–323. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Miser JS, Kinsella TJ, Triche TJ, Tsokos
M, Jarosinski P, Forquer R, Wesley R and Magrath I: Ifosfamide with
mesna uroprotection and etoposide: An effective regimen in the
treatment of recurrent sarcomas and other tumors of children and
young adults. J Clin Oncol. 5:1191–1198. 1987.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Minchom A, Jones RL, Fisher C, Al-Muderis
O, Ashley S, Scurr M, Karavasilis V and Judson IR: Clinical benefit
of second-line palliative chemotherapy in advanced soft-tissue
sarcoma. Sarcoma. 2010(264360)2010.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Leahy M, Garcia Del Muro X, Reichardt P,
Judson I, Staddon A, Verweij J, Baffoe-Bonnie A, Jönsson L, Musayev
A, Justo N, et al: Chemotherapy treatment patterns and clinical
outcomes in patients with metastatic soft tissue sarcoma. The
sarcoma treatment and Burden of Illness in North America and Europe
(SABINE) study. Ann Oncol. 23:2763–2770. 2012.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kawai A, Chuman H, Makimoto A, Ito Y,
Yamaguchi U, Morimoto Y and Beppu Y: Ifosfamide-etoposide
chemotherapy in patients with advanced adult soft tissue sarcomas.
J Clin Oncol. 22 (Suppl 14)(S9062)2004.
|
|
19
|
Grier HE, Krailo MD, Tarbell NJ, Link MP,
Fryer CJ, Pritchard DJ, Gebhardt MC, Dickman PS, Perlman EJ, Meyers
PA, et al: Addition of ifosfamide and etoposide to standard
chemotherapy for Ewing's sarcoma and primitive neuroectodermal
tumor of bone. N Engl J Med. 348:694–701. 2003.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Grohar PJ, Griffin LB, Yeung C, Chen QR,
Pommier Y, Khanna C, Khan J and Helman LJ: Ecteinascidin 743
interferes with the activity of EWS-FLI1 in Ewing sarcoma cells.
Neoplasia. 13:145–153. 2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Forni C, Minuzzo M, Virdis E, Tamborini E,
Simone M, Tavecchio M, Erba E, Grosso F, Gronchi A, Aman P, et al:
Trabectedin (ET-743) promotes differentiation in myxoid liposarcoma
tumors. Mol Cancer Ther. 8:449–457. 2009.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kawai A, Araki N, Sugiura H, Ueda T,
Yonemoto T, Takahashi M, Morioka H, Hiraga H, Hiruma T, Kunisada T,
et al: Trabectedin monotherapy after standard chemotherapy versus
best supportive care in patients with advanced,
translocation-related sarcoma: A randomised, open-label, phase 2
study. Lancet Oncol. 16:406–416. 2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Baruchel S, Pappo A, Krailo M, Baker KS,
Wu B, Villaluna D, Lee-Scott M, Adamson PC and Blaney SM: A phase 2
trial of trabectedin in children with recurrent rhabdomyosarcoma,
Ewing sarcoma and non-rhabdomyosarcoma soft tissue sarcomas: A
report from the children's oncology group. Eur J Cancer.
48:579–585. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Henderson TO, Whitton J, Stovall M,
Mertens AC, Mitby P, Friedman D, Strong LC, Hammond S, Neglia JP,
Meadows AT, et al: Secondary sarcomas in childhood cancer
survivors: A report from the childhood cancer survivor study. J
Natl Cancer Inst. 99:300–308. 2007.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ishida Y, Maeda M, Adachi S, Rikiishi T,
Sato M, Kawaguchi H, Manabe A, Tokuyama M, Hori H, Okamura J, et
al: Secondary bone/soft tissue sarcoma in childhood cancer
survivors: A nationwide hospital-based case-series study in Japan.
Jpn J Clin Oncol. 48:806–814. 2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Wolpert F, Grotzer MA, Niggli F,
Zimmermann D, Rushing E and Bode-Lesniewska B: Ewing's sarcoma as a
second malignancy in long-term survivors of childhood hematologic
malignancies. Sarcoma. 2016(5043640)2016.PubMed/NCBI View Article : Google Scholar
|