Introduction
Indocyanine green (ICG) fluorescence imaging is used
intraoperatively to detect the disseminated recurrences of
hepatocellular carcinoma (HCC) (1). However, as the tissue penetration of
near-infrared light is limited, detecting tumors in deeper sites
using this approach is difficult. At our department, a case of
minor peritoneal dissemination of HCC was encountered, in which the
lesions were able to be accurately identified and located by
combining intraoperative fluoroscopy with ICG fluorescence imaging
during laparoscopic surgery.
Case report
A 76-year-old male was diagnosed with HCC caused by
alcoholic liver cirrhosis. The patient had received percutaneous
ethanol injection therapy for S2 and S5 HCC 13 years previously,
radiofrequency ablation for S4/5 HCC 6 years ago and S6 HCC 3 years
previously.
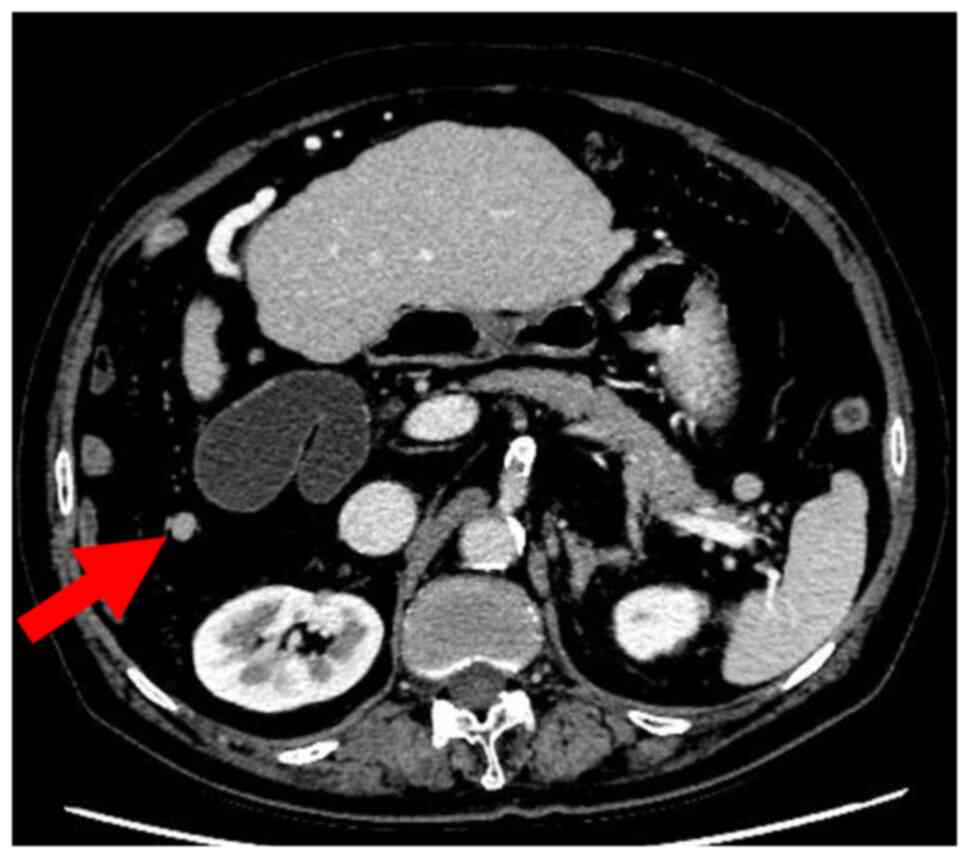
At one year prior to presentation, computed
tomography revealed tumor dissemination on the surface of S6 and
transcatheter arterial chemoembolization was performed. It also
revealed a 9-mm disseminated nodule near the gallbladder (Fig. 1). Since intrahepatic lesions were
well controlled and there was only one recurrent lesion, surgical
treatment was suggested to the patient. However, the patient
requested a less invasive treatment and thus, initiation of the
treatment with transcatheter arterial chemoembolization was first
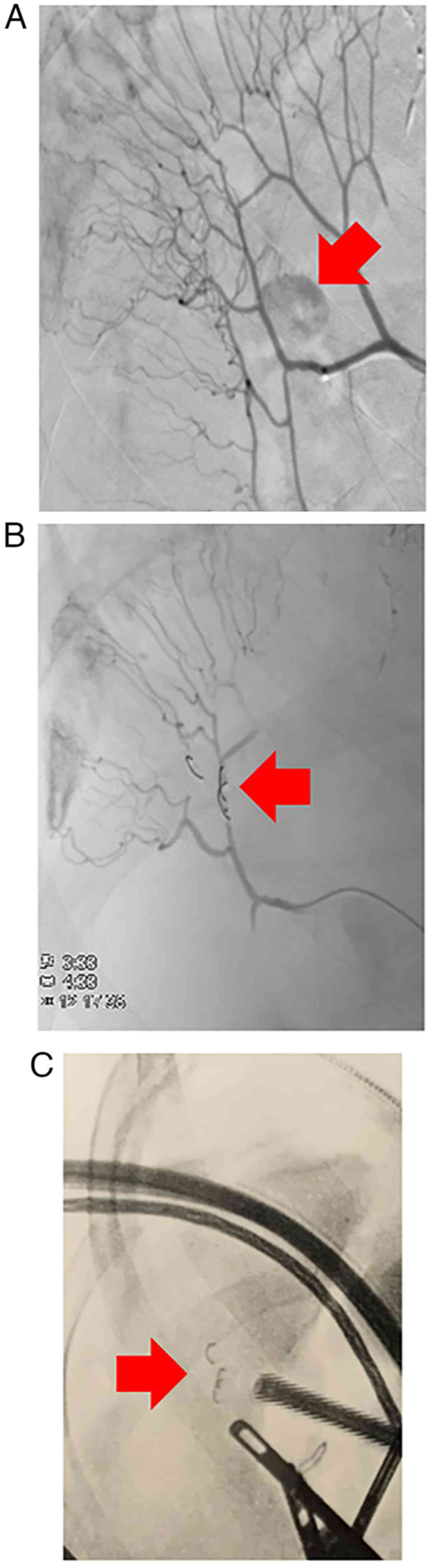
planned. A disseminated nodule was identified by selective imaging
of the ileal artery, which branches off from the superior
mesenteric artery (Fig. 2A).
Chemoembolization was attempted but impaired blood flow to the
ileum was a concern. Since it was technically difficult to treat
the lesion with chemoembolization, laparoscopic surgical resection
was opted for to remove the lesion. A coil was placed in the artery
that supplies the ileum near the disseminated nodule to serve as an
intraoperative marker (Fig.
2B).
Given the difficulty of identifying small,
disseminated lesions during laparoscopic surgery, ICG fluorescence
imaging with intraoperative fluoroscopy was used to facilitate
identification. ICG (0.5 mg/kg) was injected intravenously into the
patient 24 h prior to the operation.
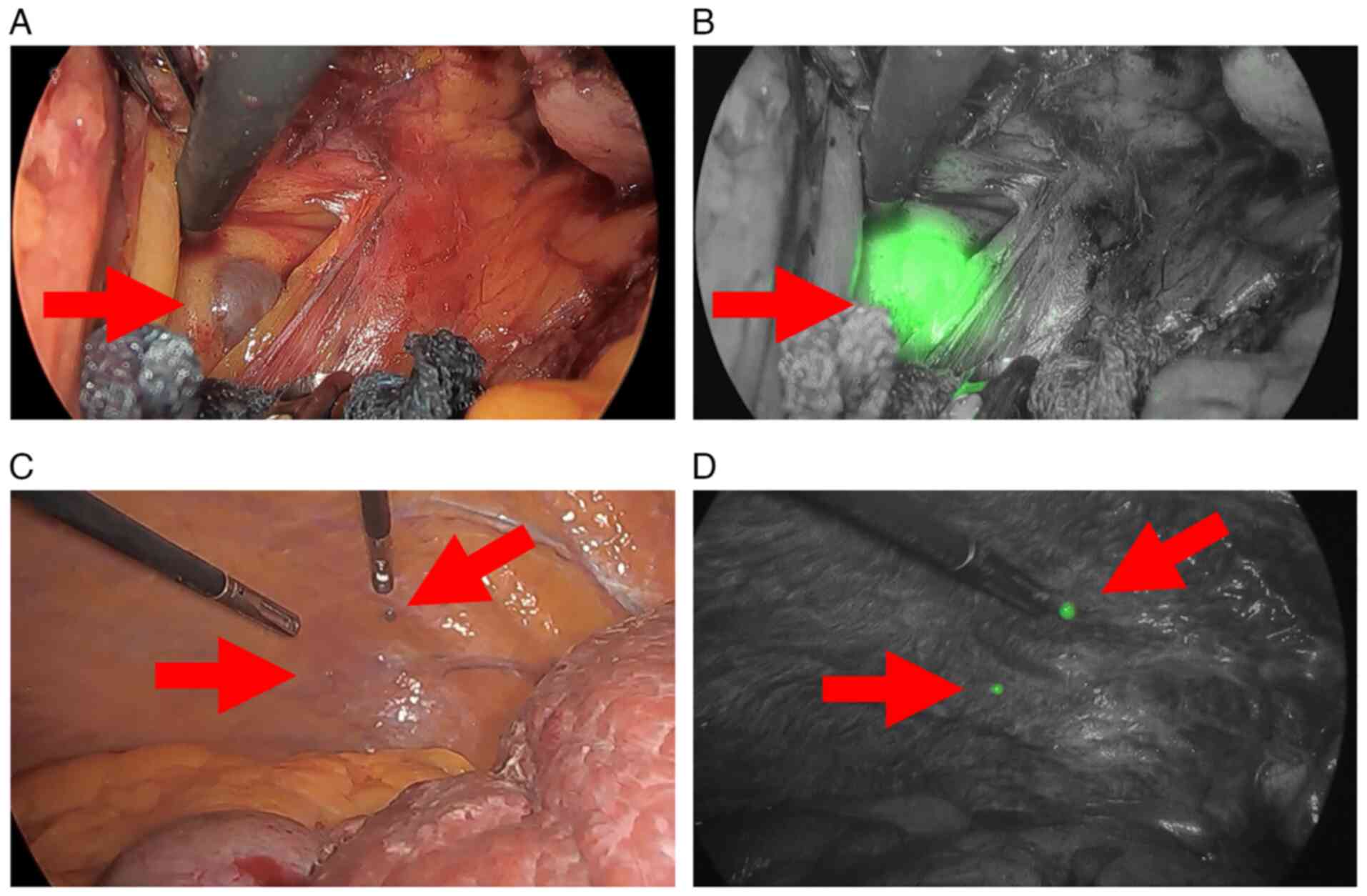
With the coil as a landmark, intraoperative
fluoroscopy was used to gauge the disseminated nodule's approximate
position (Fig. 2C), which was
beneath the adipose tissue (Fig.
3A). The Stryker 1588 AIM camera system was utilized for this.
ICG fluorescence imaging confirmed the exact position of the lesion
(Fig. 3B), which exhibited strong
fluorescence. Therefore, it was completely resected
laparoscopically. In addition, two small lesions on the right
diaphragm (Fig. 3C and D) and one small lesion on the liver
surface were also detected by fluorography and all were resected.
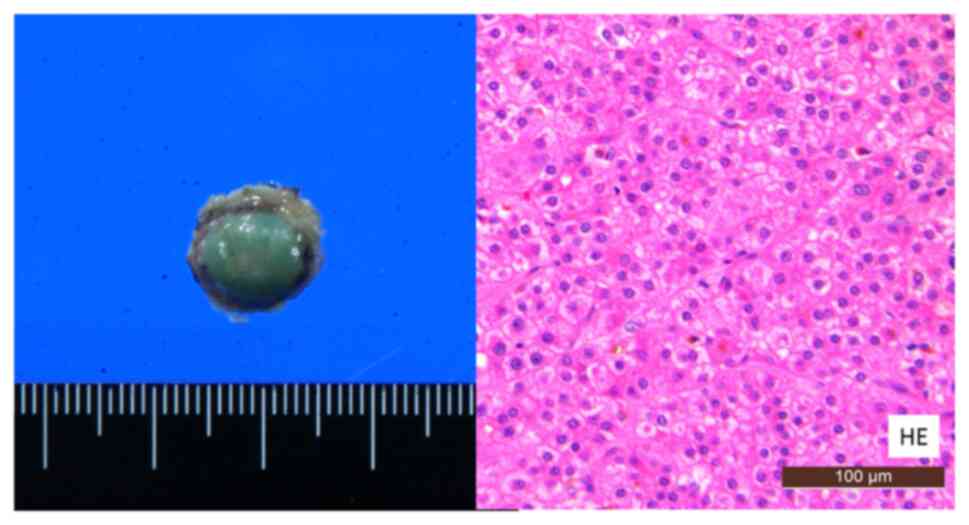
The patient's postoperative course was uneventful and he was
discharged on postoperative day 4. Pathologically, all four lesions
were diagnosed as HCC disseminations (Fig. 4). At the time of writing this case
study, 10 months had passed since the operation and the patient has
been alive without any recurrence.
Discussion
Molecular targeted drug therapy is the standard
treatment for advanced HCC with extrahepatic lesions (2,3).
However, if intrahepatic lesions are absent or well-controlled,
resection of the disseminations may be beneficial. A previous study
reported that the cumulative 1-, 3- and 5-year overall survival
rates after resection of thoracoabdominal implants were 71, 44 and
39%, respectively, with a median survival time of 34.5 months
(4).
ICG fluorescence imaging has been used in various
fields of surgery. In breast cancer surgery, the identification of
sentinel lymph nodes using ICG fluorescence imaging has been
standardized (5). ICG fluorescence
imaging is also used to determine the excision range of
non-occlusive mesenteric ischemia (6-8)
and evaluate the blood flow at the anastomotic site in colorectal
cancer surgery (9). In the field
of lung surgery, thoracoscopic lung segment resection using ICG
fluorescence imaging has also been performed (10). Nishino et al (11) reported that ICG fluorescence
imaging is useful for evaluating arterial blood flow to the stomach
in distal pancreatectomy with celiac axis resection. In HCC
surgery, ICG fluorescence imaging provides anatomical information
during laparotomy and laparoscopic surgery (12,13).
Previous studies have reported that ICG fluorescence imaging is a
convenient method for intraoperatively detecting extrahepatic HCC
metastases (14,15) The uptake of ICG by HCC cells in
extrahepatic metastases is similar to that observed in hepatocytes
and intrahepatic HCC cells (16).
According to Satou et al (1), of the 33 lesions (lung, adrenal
gland, lymph node and peritoneum) suspected to be extrahepatic
metastases of HCC, 26 exhibited fluorescence on ICG and all were
metastases of HCC. Of the seven lesions that did not exhibit any
fluorescence, one was a metastasis of HCC and six were benign
(1).
Ishizawa and Saiura (17) proposed that in patients with
intrahepatic HCC, ICG at a dose of 0.5 mg/kg body weight should be
administered within 2 weeks prior to surgery. In addition, they
advised against the administration of ICG 1 day prior to surgery to
decrease the possibility of false-positive nodules. In patients
with extrahepatic HCC, the currently recommended interval ranges
from 1 to 5 days (1). However, the
duration of ICG retention in extrahepatic HCC may be longer than
expected and ICG administration immediately prior to surgery may be
permissible due to the lack of uptake by the background tissue
(18). In the present case, ICG
0.5 mg/kg was administered intravenously 24 h prior to surgery.
Small metastatic nodules are difficult to recognize
with the naked eye or on standard laparoscopic view. For
extrahepatic HCC metastases, ICG fluorescence imaging has a
positive predictive value of 100% and a sensitivity of 92%
(1). However, as the tissue
penetration of near-infrared light is limited to 5-10 mm (19), detecting tumors in deeper sites,
such as the dorsal site of adipose tissue, using this approach is
difficult. To identify deep-seated lesions, a coil may be placed in
the artery near the lesion and intraoperative fluoroscopy with ICG
fluorescence may be used to facilitate detection. In the present
case, the disseminated lesion was able to be identified
laparoscopically using this method. Placing a marker, such as a
coil, around a tumor may be considered if the tumor is difficult to
detect with ICG fluorescence imaging alone. Furthermore,
disseminated lesions that cannot be identified preoperatively may
be identified using ICG fluorescence imaging.
ICG contains iodine, and there are reports of
occasional anaphylactic shock due to administration (20,21).
Therefore, it is necessary to be aware of the patient's history of
allergies.
In conclusion, the combination of intraoperative ICG
fluorescence imaging and fluoroscopy is useful for identifying
small, disseminated HCC lesions laparoscopically.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
SS drafted the manuscript. MT revised the
manuscript. YM and SN contributed to preoperative checks and
diagnoses. SS, MT and TH performed the surgery. YM and SN followed
up the patient. SI diagnosed the disease as a pathologist. MT and
SS checked and confirmed the authenticity of the raw data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Satou S, Ishizawa T, Masuda K, Kaneko J,
Aoki T, Sakamoto Y, Hasegawa K, Sugawara Y and Kokudo N:
Indocyanine green fluorescent imaging for detecting extrahepatic
metastasis of hepatocellular carcinoma. J Gastroenterol.
48:1136–1143. 2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S,
Kim JS, Luo R, Feng J, Ye S, Yang TS, et al: Efficacy and safety of
sorafenib in patients in the Asia-Pacific region with advanced
hepatocellular carcinoma: A phase III randomised, double-blind,
placebo-controlled trial. Lancet Oncol. 10:25–34. 2009.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Takemura N, Hasegawa K, Aoki T, Sakamoto
Y, Sugawara Y, Makuuchi M and Kokudo N: Surgical resection of
peritoneal or thoracoabdominal wall implants from hepatocellular
carcinoma. Br J Surg. 101:1017–1022. 2014.PubMed/NCBI View
Article : Google Scholar
|
|
5
|
Sugie T, Kinoshita T, Masuda N, Sawada T,
Yamauchi A, Kuroi K, Taguchi T, Bando H, Yamashiro H, Lee T, et al:
Evaluation of the clinical utility of the ICG fluorescence method
compared with the radioisotope method for sentinel lymph node
biopsy in breast cancer. Ann Surg Oncol. 23:44–50. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nakagawa Y, Kobayashi K, Kuwabara S,
Shibuya H and Nishimaki T: Use of indocyanine green fluorescence
imaging to determine the area of bowel resection in non-occlusive
mesenteric ischemia: A case report. Int J Surg Case Rep.
51:352–357. 2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Irie T, Matsutani T, Hagiwara N, Nomura T,
Fujita I, Kanazawa Y, Kakinuma D and Uchida E: Successful treatment
of non-occlusive mesenteric ischemia with indocyanine green
fluorescence and open-abdomen management. Clin J Gastroenterol.
10:514–518. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Nitori N, Deguchi T, Kubota K, Yoshida M,
Kato A, Kojima M, Kadomura T, Okada A, Okamura J, Kobayashi M, et
al: Successful treatment of non-occlusive mesenteric ischemia
(NOMI) using the HyperEye Medical System™ for
intraoperative visualization of the mesenteric and bowel
circulation: Report of a case. Surg Today. 44:359–362.
2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Arezzo A, Bonino MA, Ris F, Boni L,
Cassinotti E, Foo DC, Shum NF, Brolese A, Ciarleglio F, Keller DS,
et al: Intraoperative use of fluorescence with indocyanine green
reduces anastomotic leak rates in rectal cancer surgery: An
individual participant data analysis. Surg Endosc. 34:4281–4290.
2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Mun M, Okumura S, Nakao M, Matsuura Y and
Nakagawa K: Indocyanine green fluorescence-navigated thoracoscopic
anatomical segmentectomy. J Vis Surg. 3(80)2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Nishino H, Takano S, Yoshitomi H, Furukawa
K, Takayashiki T, Kuboki S, Suzuki D, Sakai N, Kagawa S, Nojima H,
et al: Ischemic gastropathy after distal pancreatectomy with en
bloc celiac axis resection versus distal pancreatectomy for
pancreatic body/tail cancer. Surg Open Sci. 1:14–19.
2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ishizawa T, Fukushima N, Shibahara J,
Masuda K, Tamura S, Aoki T, Hasegawa K, Beck Y, Fukayama M and
Kokudo N: Real-time identification of liver cancers by using
indocyanine green fluorescent imaging. Cancer. 115:2491–2504.
2009.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Felli E, Ishizawa T, Cherkaoui Z, Diana M,
Tripon S, Baumert TF, Schuster C and Pessaux P: Laparoscopic
anatomical liver resection for malignancies using positive or
negative staining technique with intraoperative indocyanine
green-fluorescence imaging. HPB (Oxford): Jun 7, 2021 (Epub ahead
of print).
|
|
14
|
Nanashima A, Tominaga T, Sumida Y,
Tobinaga S and Nagayasu T: Indocyanine green identification for
tumor infiltration or metastasis originating from hepatocellular
carcinoma. Int J Surg Case Rep. 46:56–61. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
He P, Huang T, Fang C, Su S, Tian J, Xia X
and Li B: Identification of extrahepatic metastasis of
hepatocellular carcinoma using indocyanine green fluorescence
imaging. Photodiagn Photodyn Ther. 25:417–420. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ishizawa T, Masuda K, Urano Y, Kawaguchi
Y, Satou S, Kaneko J, Hasegawa K, Shibahara J, Fukayama M, Tsuji S,
et al: Mechanistic background and clinical applications of
indocyanine green fluorescence imaging of hepatocellular carcinoma.
Ann Surg Oncol. 21:440–448. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ishizawa T and Saiura A: Fluorescence
imaging for minimally invasive cancer surgery. Surg Oncol Clin N
Am. 28:45–60. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Yamamura K, Beppu T, Sato N, Kinoshita K,
Oda E, Yuki H, Motohara T, Miyamoto H, Komohara Y and Akahoshi S:
Complete removal of adrenal metastasis in hepatocellular carcinoma
using indocyanine green fluorescent imaging. Anticancer Res.
40:5823–5828. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Ishizawa T, Bandai Y and Kokudo N:
Fluorescent cholangiography using indocyanine green for
laparoscopic cholecystectomy: An initial experience. Arch Surg.
144:381–382. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kim M, Lee S, Park JC, Jang DM, Ha SI, Kim
JU, Ahn JS and Park W: Anaphylactic shock after indocyanine green
video angiography during cerebrovascular surgery. World Neurosurg.
133:74–79. 2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Chu W, Chennamsetty A, Toroussian R and
Lau C: Anaphylactic shock after intravenous administration of
indocyanine green during robotic partial nephrectomy. Urol Case
Rep. 12:37–38. 2017.PubMed/NCBI View Article : Google Scholar
|