Introduction
Primary leiomyosarcoma usually occurs in the fifth
and sixth decades of life. The most common clinical symptoms are
abdominal pain and gastrointestinal bleeding (1). This type of tumor originates from
smooth muscle cells and mainly occurs in the retroperitoneum and
abdomen (2). The overall incidence
of vascular leiomyosarcoma has been reported to be <2% (3). Complete surgical resection is
considered to be the cornerstone of treatment for localized
vascular leiomyosarcomas, while the role of neoadjuvant
chemotherapy and radiation remains unknown (4). The prognosis of patients with
vascular leiomyosarcoma is reportedly poorer compared with the
prognosis of patients with leiomyosarcomas of different origins
(4). Primary leiomyosarcoma
arising from the splenic vein is an extremely rare occurrence and
its clinical features are incompletely understood. The clinical
diagnosis of this condition remains challenging, despite
advancements in imaging modalities, owing to its rarity.
Furthermore, evidence regarding treatment strategies, including
postoperative adjuvant radiation and chemotherapy, is scarce. We
herein describe the case of a patient with a history of
retinoblastoma who was diagnosed with leiomyosarcoma originating
from the splenic vein and was treated with pancreatosplenectomy and
subsequent transcatheter arterial chemoembolization due to the
development of hepatic metastases 5 months postoperatively
(5). The aim of the present report
was to help with the development of clinical guidelines for
leiomyosarcomas of the splenic vein.
Case report
A 45-year-old Japanese woman, who had a history of
infantile retinoblastoma treated by enucleation and chronic
hepatitis C diagnosed in her twenties, underwent a routine medical
check-up at Hiroo Medical Clinic (Tokyo, Japan). In May 2015, the
patient presented to the hospital with no apparent symptoms.
Abdominal ultrasonography revealed a mass ~40 mm in size located
posterior to the pancreatic tail. The pancreatic body was observed
to be distended dorsally on CT examination. The adrenal gland was
independently identified, and it was determined that the lesion did
not originate from the adrenal gland. In addition, the lesion
appeared to have no border with the pancreatic parenchyma and had
the same signal intensity as the pancreas. There was a tear in the
splenic vein, and the epiploic veins were highly developed as
collateral blood vessels, which is an atypical finding in
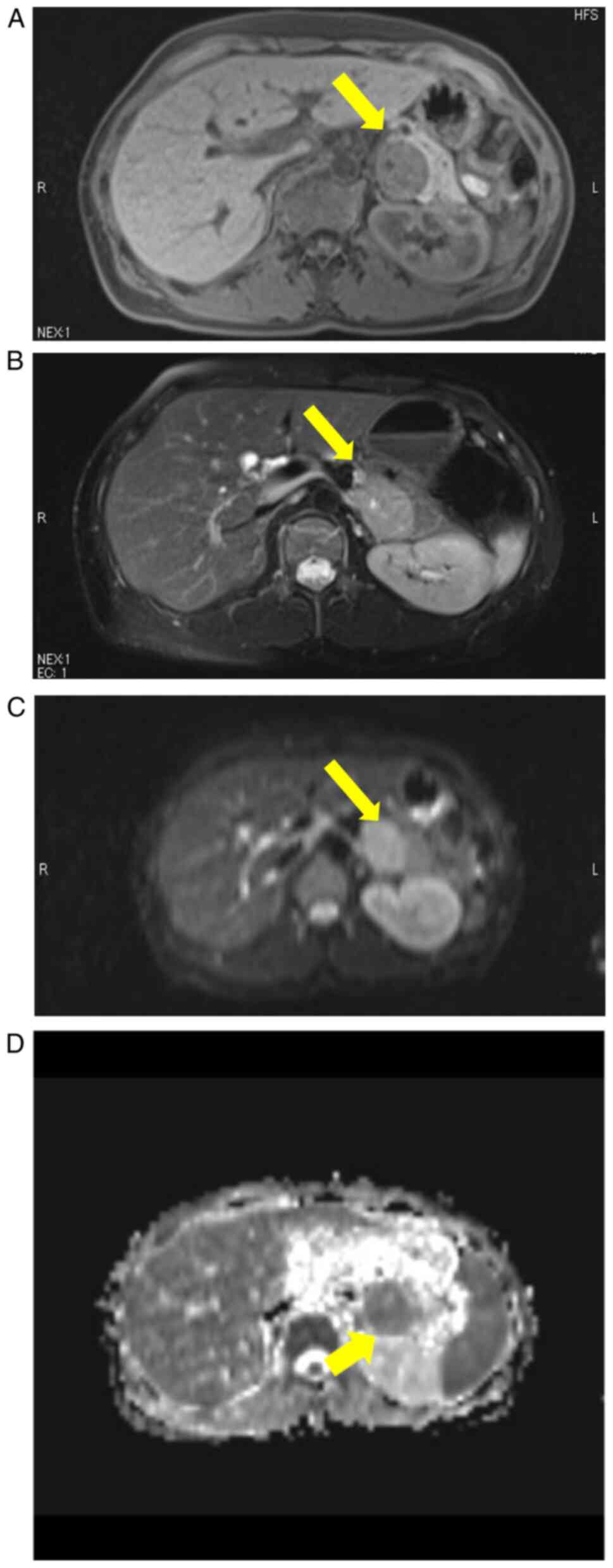
carcinoma. On MRI examination, the lesion appeared as a
well-circumscribed mass that compressed the pancreas posteriorly
with no invasion into the pancreatic parenchyma. The signal
intensity of the mass was lower on T1-weighted images and higher on
T2-weighted images as compared to that of the pancreas. The signal
intensity of the lesion on diffusion-weighted images was high and
that on an apparent diffusion coefficient map was low, suggesting
that the lesion had a high cellular density. The value of the
apparent diffusion coefficient was 0.911. Although the pattern of
these signal intensities was similar to that of the spleen, the
signal intensity of the lesion on T2-weighted images was lower than
that of the spleen (Fig. 1).
Ferucarbotran-enhanced MRI performed 1 month after the patient's
initial visit revealed that the lesion had a higher signal
intensity than the spleen, indicating that the lesion was not an
accessory spleen. Furthermore, the lesion had not increased in size
in 1 month, indicating that it was possibly not a malignant tumor.
Therefore, the lesion was suspected to be an extrapancreatic tumor,
such as a retroperitoneal tumor similar to that observed in
Castleman's disease (6). In
September 2015, the patient was subsequently referred to Toranomon
Hospital for further evaluation and management of the mass.
Considering the highly invasive nature of the surgery and the
patient's refusal to undergo surgery, we decided to perform regular
follow-ups semiannually using ultrasonography and MRI examination.
An abdominal ultrasound carried out 5 years after the first visit
to our institution revealed an increase in the size of the mass to
50 mm, which was highly suggestive of a malignancy.
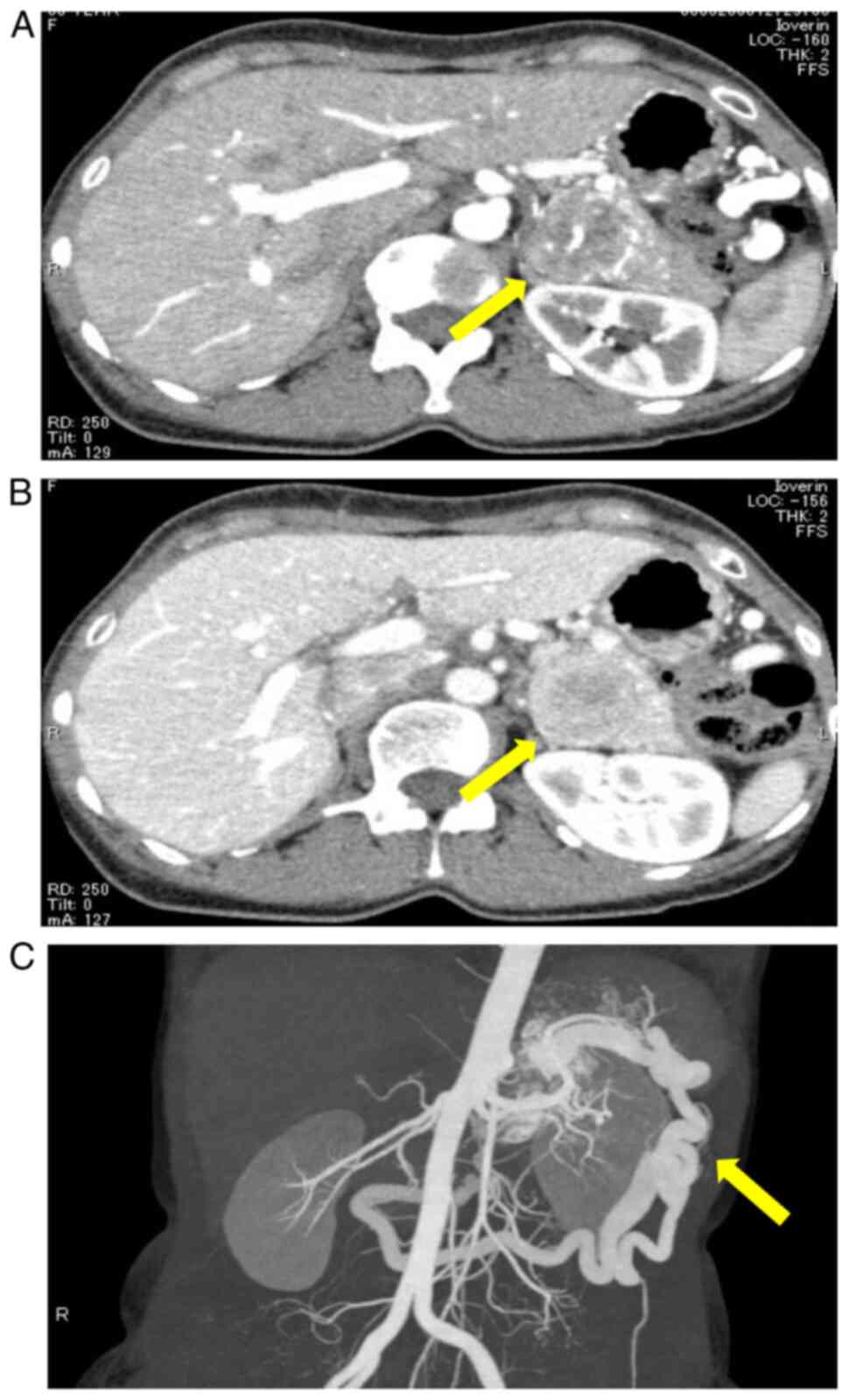
Contrast-enhanced CT revealed a well-defined mass with
heterogeneous contrast in the early phase and good enhancement in
the delayed phase. No significant enlargement of the surrounding
lymph nodes was observed. Obstruction of the splenic vein was
observed. There was no invasion into other organs or the renal
veins (Fig. 2). Endoscopic
ultrasonography revealed a solid component in the splenic vein that
appeared as a thickening of the vascular wall, and it was
contiguous with the mass. Furthermore, multiple vessels were
observed inside the mass. The mass formed a tumor embolus within
the splenic vein, and a portion of the splenic vein had increased
in size to 49x33 mm. Although the tumor growth was relatively slow,
the presence of the tumor embolus suggested that the mass was a
malignant tumor. MRI was not performed, as the aforementioned
imaging studies were considered to be sufficient for the
development of the treatment strategy preoperatively. The levels of
serum tumor markers, such as carcinoembryonic antigen and
carbohydrate antigen 19-9, were within the normal range. The serum
amylase, lipase, elastase 1 and immunoglobulin G4 levels were
within the normal limits. The differential diagnosis included
pancreatic acinar cell carcinoma, pancreatoblastoma, neuroendocrine
tumor, gastrointestinal stromal tumor or other types of
retroperitoneal tumors. Surgical resection was decided after
discussing the options with the patient.
Open radical antegrade modular pancreatectomy was
performed in August 2020. No ascites, dissemination, or distant
metastasis were observed intraoperatively; the epiploic veins were
prominently dilated. The gastrosplenic ligament was excised. The
mass was a tense, elastically hard tumor located at the pancreatic
tail; the pancreas appeared normal. Intraoperative ultrasound
revealed a well-defined, hypervascular mass contiguous to the
splenic vein. The splenic artery was ligated at its origin. The
pancreas was sectioned at the level of the left border of the
portal vein, and the splenic vein was subsequently divided to the
terminal end. The dissection proceeded anterior to the adrenal
gland in a right-to-left antegrade manner. The splenorenal ligament
was divided and the spleen was mobilized. The entire specimen was
then resected; R0 resection was successfully performed. The
operative time was 106 min, and the total intraoperative blood loss
was 247 ml.
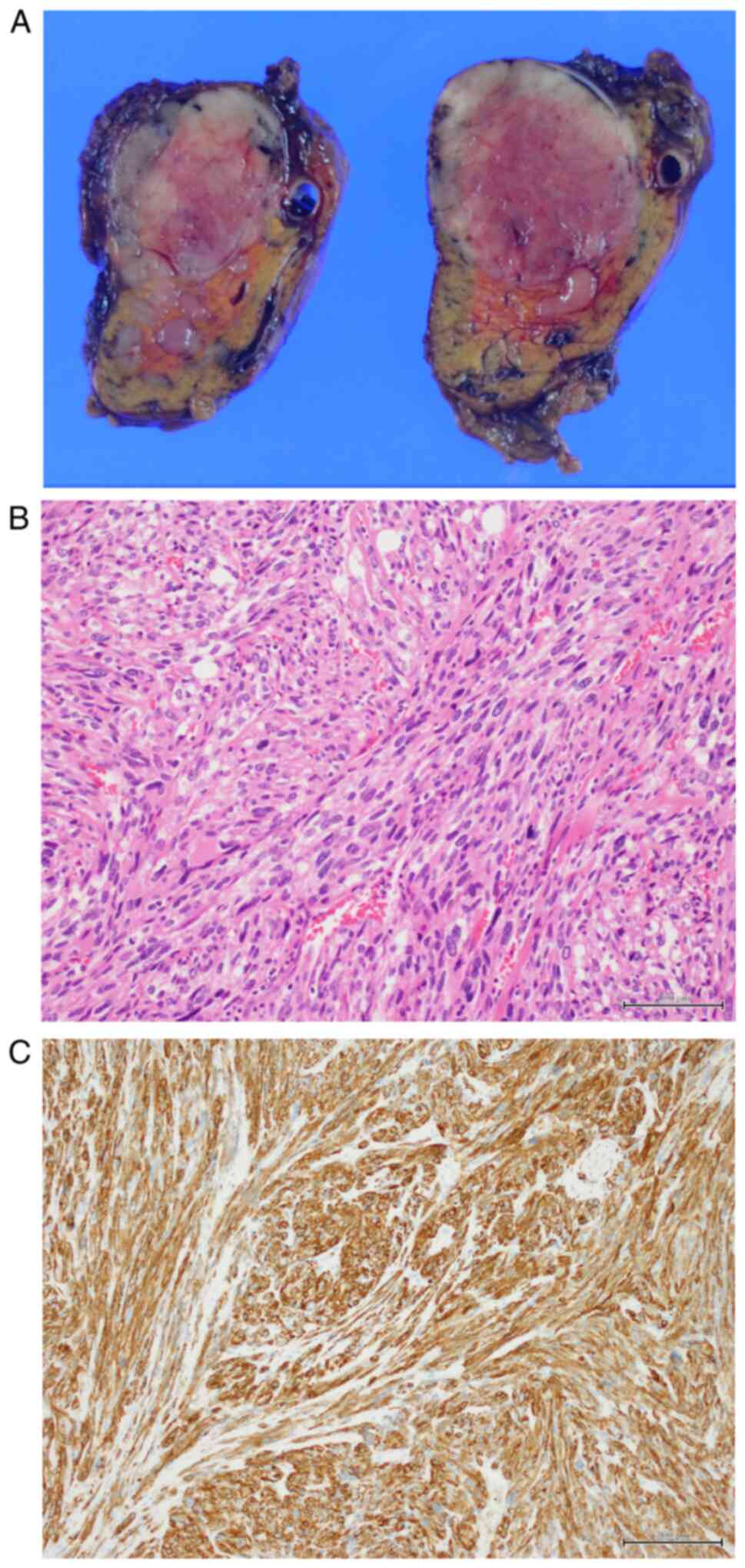
Macroscopic examination revealed that the tumor was
located in the splenic vein, forming a tumor thrombus, and small
tumor nodules were present in the pancreas. Histologically, the
tumor was composed of spindle cells arranged in interlacing
fascicles. The tumor cells were immunohistochemically positive for
desmin, h-caldesmon, muscle-specific actin and α-smooth muscle
actin. Microscopic examination showed tumor infiltration beyond the
wall of the splenic vein and into the surrounding soft tissue and
pancreatic parenchyma. The pathological diagnosis was
leiomyosarcoma arising from the splenic vein (Fig. 3).
The postoperative course was uneventful, and the
patient was discharged on postoperative day 15. Following an
institutional multidisciplinary cancer board discussion, regular
follow-up visits were scheduled for the patient, as no effective
evidence-based chemotherapy was available in this case.
At a regular medical check-up 5 months
postoperatively, abdominal ultrasound revealed four space-occupying
lesions in the liver. Contrast-enhanced CT revealed four masses up
to 15 mm in size, with indistinct borders, showing high and
intermediate signal intensity in the early and in the portal and
late phases, respectively. There were no other apparent lesions.
Chemotherapy was ruled out as a treatment option, and transcatheter
arterial chemoembolization (TACE) was performed using epirubicin in
March 2021, since the lesions were limited to the liver. The tumors
were pathologically diagnosed as leiomyosarcomas by needle
biopsy.
Since the last TACE procedure, the patient has been
regularly followed up with abdominal ultrasound and CT conducted at
each visit; no recurrence was observed on the last follow-up visit
in August 2021.
Discussion
Leiomyosarcoma is a rare malignant mesenchymal tumor
originating from smooth muscle cells, which is usually located in
the retroperitoneum, mesentery, omentum, uterus or subcutaneous
tissue (7). Leiomyosarcomas of
vascular origin account for <2% of all cases (3). Venous leiomyosarcomas are mainly
observed in women between their fifth and sixth decades of life
(8). Furthermore, 75% of
large-vessel leiomyosarcomas are observed in the inferior vena cava
(9,10). However, those derived from the
splenic vein have been reported in only a few previous studies. To
the best of our knowledge, only five previous studies have reported
cases of leiomyosarcoma of the splenic vein (Table I) (7,11-14).
 | Table ISummary of the previous reports of
leiomyosarcoma of splenic vein. |
Table I
Summary of the previous reports of
leiomyosarcoma of splenic vein.
| Study (Refs.) | Age (years) | Sex | Medical history | Clinical
manifestations | Tumor marker | Treatment | Resection margin | Adjuvant therapy | Follow-up
(months) | Postoperative
metastasis | Outcome |
|---|
| Niver et al
(7) | 58 | F | Unknown | Epigastric pain | Unknown | Distal
pancreatosplenectomy, reconstruction of the portal vein | Unknown | None | Unknown | None | Alive |
| Gage et al
(13) | 58 | F | Unremarkable | Epigastric pain,
splenic vein thrombosis | Unknown | Distal
pancreatosplenectomy, reconstruction of the portal vein | Free | None | 15 | None | Alive |
| Aguilar et al
(11) | 66 | F | Unremarkable | Epigastric pain,
constipation, weight loss | Unknown | Distal
pancreatosplenectomy | Free | Doxorubicin +
ifosfamide | 12 | None | Alive |
| Patrono et al
(12) | 58 | F | Unremarkable | Epigastric pain | Normal | Local excision,
splenic vein anastomosis | Free | None | 12 | None | Alive |
| Wu et al
(14) | 52 | M | Unremarkable | Epigastric pain | Unknown | Splenic pedicle tumor
resection, splenectomy, liver tumor resection | Unknown | None | Unknown | None | Alive |
| Present case | 50 | F | Retinoblastoma | None | Normal | Distal
pancreatosplenectomy | Free | None | 10 | Liver metastasis | Alive |
Due to its rarity, the differential diagnosis of
leiomyosarcoma of the splenic vein is challenging. However,
early-stage diagnosis is crucial, as surgical resection is the only
curative option in such cases (15,16).
Ultrasound examination is frequently performed as the first
diagnostic tool. Leiomyosarcoma is characterized as a
circumscribed, soft tissue mass, commonly accompanied by necrosis,
cystic degeneration and hemorrhage on CT (17,18).
In the present case, there were two possible diagnoses: A primary
retroperitoneal leiomyosarcoma with secondary venous invasion or a
primary venous leiomyosarcoma with secondary extravascular
extension, as in the study by Niver et al (7). It was difficult to determine whether
the tumor originated from the retroperitoneum or the vasculature
preoperatively.
As regards the treatment strategy, en bloc resection
is the only curative treatment option for this condition in the
absence of disseminated disease (13), although the prognostic value of
microscopic involvement of the resection margin remains disputable
(16). Furthermore, in all the
previous reports of leiomyosarcoma of the splenic vein, the correct
diagnosis was established only after surgical resection (7,11-14).
Radiation treatment is commonly performed for high-grade soft
tissue sarcomas of the extremities, intermediate-grade tumors of
the limbs with close margins, and recurring low-grade sarcomas
(14). Among retroperitoneal
sarcomas, primary leiomyosarcomas of vascular origin have the
highest incidence of local recurrence and the worst long-term
survival outcomes (16). The
incidence of post-resection metastases is ~40% in such cases
(9,19). The high risk of local recurrence of
leiomyosarcoma may justify adjuvant radiotherapy in some cases.
While chemotherapy can be performed for systemic control, the
sensitivity of sarcomas to chemotherapy is considered to be low
(20). Therefore, the role of
chemotherapy as an adjuvant treatment for leiomyosarcoma for
prolonging life expectancy has not yet been established (20). Evidence of prolonged survival due
to adjuvant radiotherapy or chemotherapy is scarce. Among previous
reports of leiomyosarcomas of the splenic vein, only one study
reported that the patient underwent postoperative adjuvant therapy
(Table I) (11). In a meta-analysis of soft tissue
sarcomas treated with adjuvant chemotherapy, no improvement in
prognosis was observed (21).
A history of hereditary retinoblastoma is associated
with an increased incidence of a second, non-ocular, primary tumor
(22). Retinoblastoma is an
uncommon childhood tumor with an incidence of 1 per 20,000 live
births (22). It can exhibit an
autosomal dominant form of inheritance, although the majority of
retinoblastomas are sporadic. The incidence of second non-ocular
primary tumors is known to increase with time, and tumor
development is associated with the loss of tumor suppressor
activity caused by alterations in the Rb1 gene due to radiation,
genetic mutations, or other causes (23). Although various types of secondary
malignant tumors have been reported in patients with hereditary
retinoblastoma, no cases of secondary tumors with splenic vein
origin have previously been reported in such patients, to the best
of the authors' knowledge.
In the present case, despite complete resection with
a negative margin, hepatic recurrence was identified within 1 year
after resection. Taking into consideration the poor outcomes of
leiomyosarcomas of venous origin, successful resection may have
contributed to an improved prognosis in the present case, although
continuous follow-up is required.
In conclusion, the present report of a
leiomyosarcoma originating in the splenic vein is, to the best of
our knowledge, the sixth case of a splenic vein leiomyosarcoma
reported in the English literature to date. There are currently
insufficient case reports to develop clinical guidelines regarding
treatment strategies for leiomyosarcoma of the splenic vein. The
importance of this case lies with the rarity of leiomyosarcoma of
the splenic vein and the rarity of leiomyosarcoma as a second
non-ocular tumor in patients with a history of retinoblastoma.
Recognition of this clinical condition at the preoperative
examination stage may prove helpful for preoperative diagnosis.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MA wrote the manuscript and contributed to its
design. MH contributed to the operation and helped draft the
manuscript. DH, RK and TI performed patient follow-up and provided
advice on patient treatment. YT contributed to the pathological
diagnosis. MH and TI have seen and confirmed the authenticity of
the raw data. All the authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient regarding the publication of the case details and any
associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yang J: Primary leiomyosarcoma in the
colon: A case report. Medicine (Baltimore).
97(e9923)2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wile AG, Evans HL and Romsdahl MM:
Leiomyosarcoma of soft tissue: A clinicopathologic study. Cancer.
48:1022–1032. 1981.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kevorkian J and Cento DP: Leiomyosarcoma
of large arteries and veins. Surgery. 73:390–400. 1973.PubMed/NCBI
|
|
4
|
Italiano A, Toulmonde M, Stoeckle E, Kind
M, Kantor G, Coindre JM and Bui B: Clinical outcome of
leiomyosarcomas of vascular origin: Comparison with leiomyosarcomas
of other origin. Ann Oncol. 21:1915–1921. 2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Riley DS, Barber MS, Kienle GS, Aronson
JK, von Schoen-Angerer T, Tugwell P, Kiene H, Helfand M, Altman DG,
Sox H, et al: CARE guidelines for case reports: Explanation and
elaboration document. J Clin Epidemiol. 89:218–235. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Shimokihara K, Kawahara T, Kasahara R,
Kasuga J, Sugiura S, Tajiri R, Uemura H and Chiba K:
Retroperitoneal castleman's disease. Case Rep Oncol. 12:885–889.
2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Niver BE, Megibow AJ, Faust MJ and
Rosenkrantz AB: Multidetector CT appearance of leiomyosarcoma of
the splenic vein. Clin Radiol. 66:688–690. 2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tilkorn DJ, Hauser J, Ring A, Goertz O,
Stricker I, Steinau HU and Kuhnen C: Leiomyosarcoma of
intravascular origin-a rare tumor entity: Clinical pathological
study of twelve cases. World J Surg Oncol. 8(103)2010.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Székely E, Kulka J, Miklós I and Kaliszky
P: Leiomyosarcomas of great vessels. Pathol Oncol Res. 6:233–236.
2000.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Burke AP and Virmani R: Sarcomas of the
great vessels. A clinicopathologic study. Cancer. 71:1761–1773.
1993.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Aguilar C, Socola F, Donet JA, Gallastegui
N and Hernandez GA: Leiomyosarcoma of the splenic vein. Clin Med
Insights Oncol. 7:263–268. 2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Patrono D, Molinaro L, Mazza E, Romagnoli
R and Salizzoni M: Splenic vein leiomyosarcoma: Case report and
review of the literature. JOP. 15:512–514. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gage MJ, Newman E, Maldonado TS and Hajdu
CH: Leiomyosarcoma of the splenic vein. J Vasc Surg. 55:1485–1487.
2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Wu W, Zhao X, Wang Y, Di C, Cai R, Zhang
Y, Chen S, Zhang W and Yue X: Leiomyosarcoma of the splenic vein: A
case report. Oncol Lett. 14:977–980. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Barbetakis N, Asteriou C, Papadopoulou FI
and Stergiou E: Sarcomas of the great vessels. Is there a role for
chemotherapy? Interact Cardiovasc Thorac Surg. 10:463–464.
2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hollenbeck ST, Grobmyer SR, Kent KC and
Brennan MF: Surgical treatment and outcomes of patients with
primary inferior vena cava leiomyosarcoma. J Am Coll Surg.
197:575–579. 2003.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Hartman DS, Hayes WS, Choyke PL and
Tibbetts GP: From the archives of the AFIP. Leiomyosarcoma of the
retroperitoneum and inferior vena cava: Radiologic-pathologic
correlation. Radiographics. 12:1203–1220. 1992.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Narata M, Okuhata Y, Abe K, Takemoto A,
Maebayashi T, Furuhashi S and Takahashi M: Primary leiomyosarcoma
of the inferior vena cava: Case report. Abdom Imaging. 35:481–484.
2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hilliard NJ, Heslin MJ and Castro CY:
Leiomyosarcoma of the inferior vena cava: Three case reports and
review of the literature. Ann Diagn Pathol. 9:259–266.
2005.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Clark MA, Fisher C, Judson I and Thomas
JM: Soft-tissue sarcomas in adults. N Engl J Med. 353:701–711.
2005.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Adjuvant chemotherapy for localised
resectable soft-tissue sarcoma of adults: Meta-analysis of
individual data. Sarcoma meta-analysis collaboration. Lancet.
350:1647–1654. 1997.PubMed/NCBI
|
|
22
|
Lueder GT and Smith ME: Retinoblastoma.
Semin Diagn Pathol. 11:104–106. 1994.PubMed/NCBI
|
|
23
|
Friend SH, Bernards R, Rogelj S, Weinberg
RA, Rapaport JM, Albert DM and Dryja TP: A human DNA segment with
properties of the gene that predisposes to retinoblastoma and
osteosarcoma. Nature. 323:643–646. 1986.PubMed/NCBI View
Article : Google Scholar
|