Introduction
Sudden cardiac arrest during non-cardiac surgery is
a rare, yet potentially fatal complication. In head and neck
procedures, neurally mediated reflexes including direct vagal
stimulation, trigeminocardiac reflex and oculocardiac reflex can
trigger severe cardiovascular events (1).
Throat packs are commonly used during oral and
maxillofacial surgery to prevent aspiration, although their
efficacy remains a matter of debate (2). While generally considered safe, cardiac
complications from airway manipulation have been increasingly
recognized. Direct laryngoscopy can cause severe bradycardia and
asystole through vagal stimulation (3), and even jaw thrust maneuvers, typically
used for simple airway maintenance, can trigger profound vagal
responses leading to asystole (4).
Given this context, throat pack insertion, though considered
routine practice, may pose a similar risk of severe vagally
mediated cardiac events. The trigeminovagal reflex, with an
incidence of ~~1.6% in maxillofacial surgical procedures, has been
reported during mouth opening with dental mouth gags, although such
cases resulting in asystole are extremely rare (5).
The present study describes a rare case of transient
cardiac arrest directly attributed to throat pack insertion during
oral surgery. In addition, the present study provides a discussion
of the underlying neurophysiological mechanisms and clinical
implications for routine maxillofacial procedures.
Case report
An otherwise healthy 54-year-old male patient (ASA
Physical Status 1; height, 173 cm; weight, 78.0 kg) presented to
Nagoya Tokushukai General Hospital (Kasugai, Japan) and was
scheduled for a mandibular horizontal impacted third molar
extraction under general anesthesia.
Anesthesia was induced with propofol 130 mg (1.67
mg/kg), fentanyl 50 µg (0.64 µg/kg), and rocuronium 70 mg (0.90
mg/kg), followed by successful left nasal intubation using a
Ring-Adair-Elwyn (RAE) tube (7.0 mm, 27 cm). Anesthesia was
maintained with desflurane and remifentanil infusion (Fig. 1).
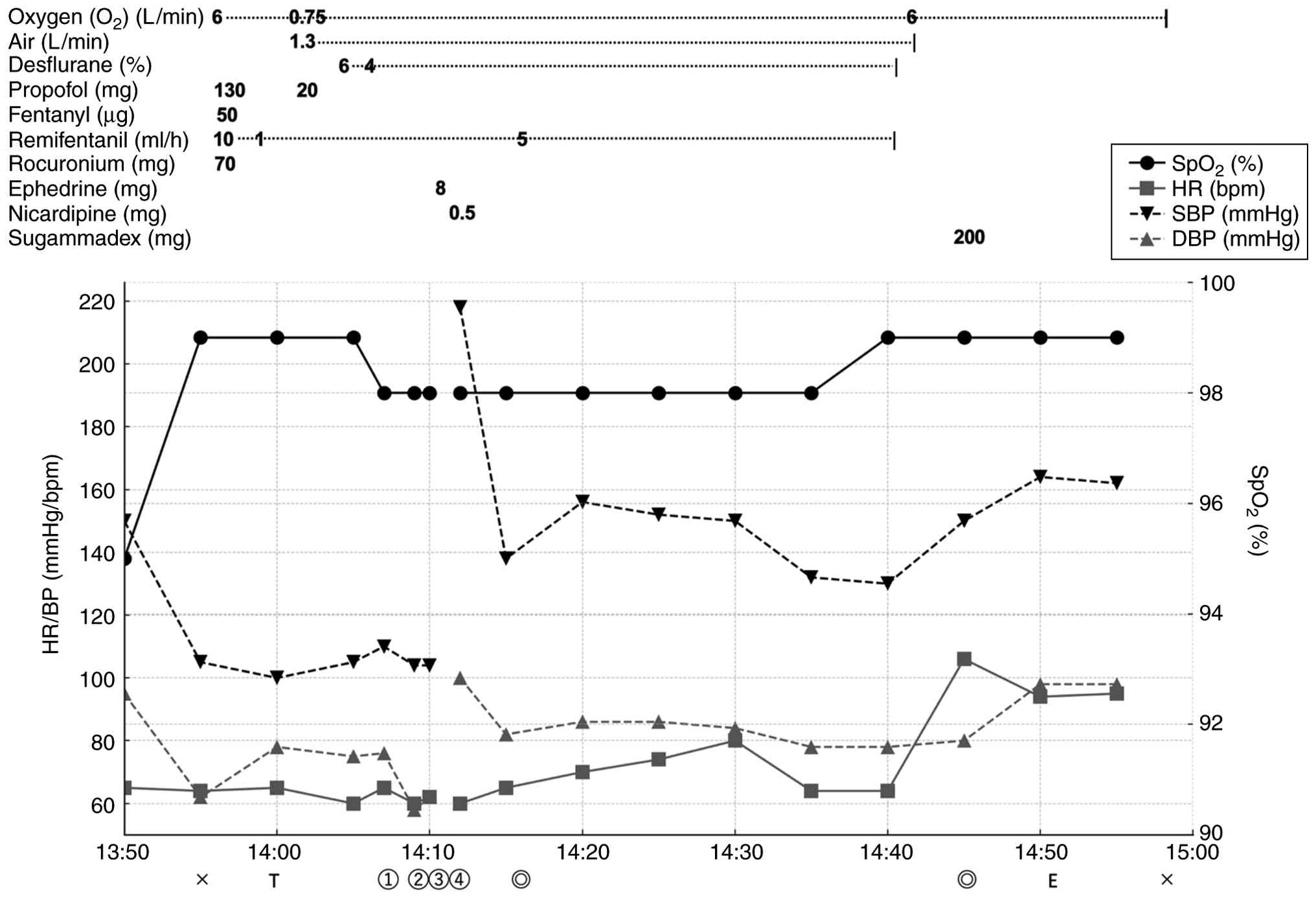 | Figure 1Intraoperative anesthetic chart
demonstrating the timeline of anesthetic management, including
medication administration and the occurrence of cardiac arrest
immediately following throat pack insertion. The chart illustrates
the progression from normal vital signs to cardiac arrest and
subsequent recovery following ephedrine administration. Crosses
mark the start and end of anesthesia; T, intubation; E, extubation;
double circles, indicate the start and end of surgery; circled
numerals ①-④ indicate: ① throat pack insertion, ② cardiac arrest, ③
ephedrine (8 mg) administration, ④ return of spontaneous
circulation. Heart rate values represent trend-averaged monitor
data; transient electrical asystole is therefore depicted as an
interruption of the HR trace rather than a numerical value of zero.
SpO2, peripheral oxygen saturation; HR, heart rate; BP,
blood pressure; DBP, diastolic blood pressure; SBP, systolic blood
pressure. |
Following intubation, throat packing was performed
according to standard institutional protocol using sterile
moistened gauze (30x30 cm). The gauze was gently placed into the
oropharynx using long forceps, positioned around the endotracheal
tube without excessive pressure.
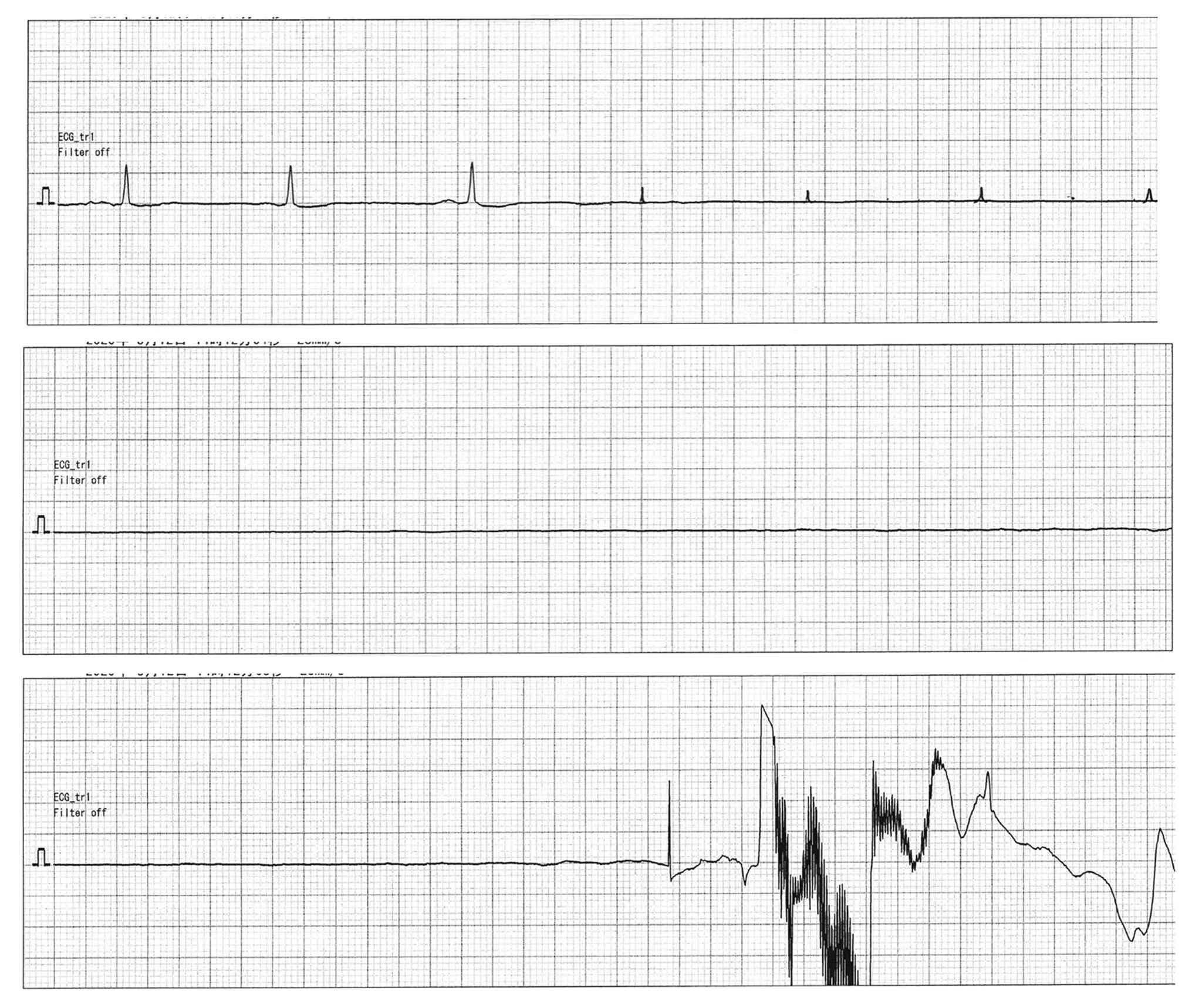
Immediately following throat pack insertion, the
patient developed sudden cardiac arrest. Electrocardiographic
monitoring revealed complete electrical asystole with absence of
all cardiac electrical activity (Fig.
2). The asystolic period lasted ~20 sec, during which the pulse
was impalpable.
Upon recognition of profound vagally mediated
bradyarrhythmia progressing to electrical asystole, the surgeon
immediately ceased all pharyngeal manipulation and removed the
throat pack. Ventilation was maintained with 100% oxygen (6 l/min)
throughout the episode, and SpO2 remained >95%. Given
the maintained oxygenation, the absence of pulseless electrical
activity confirmed by continuous arterial line monitoring, and the
brief duration of the arrhythmia, chest compressions were not
initiated. Ephedrine (8 mg) was administered intravenously as the
initial vasopressor due to its combined α- and β-adrenergic
effects. Atropine was prepared, but was not required, as
spontaneous circulation returned ~20 sec following the
administration of ephedrine and stimulus cessation. The cardiac
rhythm of the patient normalized, and the surgery was completed
successfully without further cardiovascular complications.
Post-operatively, the patient recovered uneventfully with no
evidence of cardiac complications.
On the first post-operative day, the patient was
referred to the cardiology department at Nagoya Tokushukai General
Hospital for a comprehensive cardiac evaluation. Coronary computed
tomography angiography was performed post-operatively (data not
shown; images not available) and did not reveal clinically
significant coronary stenosis according to the cardiology report.
Transthoracic echocardiography demonstrated normal ventricular wall
motion and function, supporting the absence of overt structural
heart disease. Based on these findings and the clinical course, the
event was considered most consistent with a vagally mediated reflex
mechanism.
Discussion
Reflex arc and anatomical
background
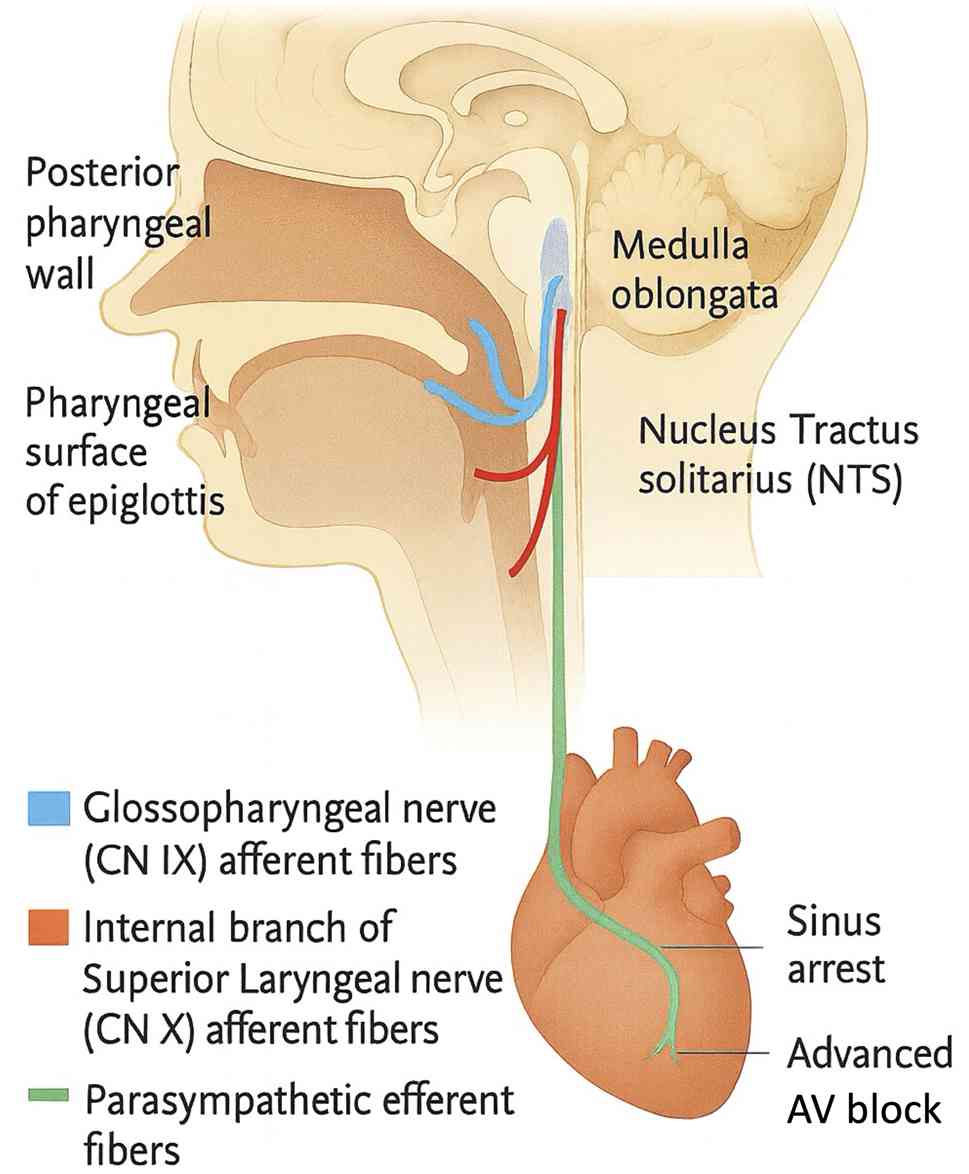
Sensory inputs from glossopharyngeal and vagal
afferents converge on the nucleus tractus solitarius (NTS) of the
medulla, where baroreceptor signals from the carotid sinus, aortic
arch, and cardiopulmonary receptors are integrated (6). Parasympathetic efferents arising from
the dorsal motor nucleus of the vagus nerve and nucleus ambiguus
then project to the sinoatrial and atrioventricular nodes, exerting
inhibitory effects on cardiac conduction. Experimental research has
further demonstrated that the disruption of NTS neuronal activity
directly induces bradycardia and hypotension (7), underscoring the central role of this
reflex arc in cardiovascular regulation.
During throat pack placement, the stimulation of the
laryngopharyngeal mucosa, particularly the epiglottic surface
innervated by the internal branch of the superior laryngeal nerve,
has been reported to trigger vagal reflexes that may culminate in
profound bradyarrhythmia or asystole (3). In addition, the activation of the
Bezold-Jarisch reflex, mediated by cardiac receptors with
non-myelinated vagal C-fiber afferents, produces a characteristic
triad of bradycardia, hypotension and peripheral vasodilation
(8). These reflex mechanisms
collectively provide a plausible physiologic explanation for the
abrupt vagally mediated cardiac arrest observed in the case
presented herein (Fig. 3).
Clinical significance of throat
pack-induced cardiac arrest
Reflex-mediated cardiovascular responses may
progress stepwise. Campagna and Carter (8) described how vagal reflexes can evolve
from initial bradycardia and hypotension to sinus arrest and
high-grade atrioventricular block, and ultimately to asystole and
pulseless electrical activity. Clinically, such events have been
observed during airway manipulation: Redmann et al (3) reported asystole during suspension
microlaryngoscopy, attributed to direct vagal stimulation, while
Chung et al (9) documented
transient asystole immediately after balloon dilation of the
Eustachian tube.
In contrast to these reports of vigorous stimuli,
cardiac arrest from throat pack insertion alone remains uncommon.
Its occurrence in the case described herein, despite the minimally
invasive nature of the intervention, may reflect high baseline
vagal tone or a lowered reflex threshold under light
anesthesia.
Risk factors and prevention
Under light anesthesia, the suppression of
sympathetic activity predisposes patients to parasympathetic
dominance. Propofol and suxamethonium can produce profound
bradycardia without anticholinergic premedication (10), while hypercapnia enhances cardiac
vagal responsiveness (11).
Fluctuations in autonomic balance have also been implicated in
vagally mediated bradycardia and circulatory collapse in patients
with syncope (12). Adequate
anesthetic depth and ventilation before pharyngeal manipulation are
therefore essential, and prophylactic atropine may be warranted
when vagal predominance is anticipated.
Clinical management
In the patient described in the present case report,
spontaneous cardiac rhythm resumed within ~20 sec without chest
compressions after cessation of the stimulus and the administration
of 8 mg ephedrine. This rapid recovery is consistent with vasovagal
cardiac arrest, in which vagal dominance and sympathetic inhibition
predominate (8,12). The prompt return of spontaneous
circulation suggests that pharmacologic intervention effectively
interrupted the reflex arc. Clinically, the key measures are to
discontinue the provoking stimulus immediately and administer
anticholinergic or vasopressor agents without delay.
While the temporal association and clinical course
strongly suggest a vagally mediated mechanism, definitive
confirmation would require comprehensive exclusion of alternative
factors including anesthetic depth, ventilation status and baseline
autonomic tone, data not completely documented in real-time during
this event.
Limitations
The present case report has several limitations
which should be mentioned. First, as a single case report, the
findings cannot be generalized to all patients undergoing throat
pack insertion. Second, although coronary computed tomography
angiography was performed, the original axial and multiplanar
reconstructed imaging data were unavailable for publication, which
limits independent visual assessment of coronary anatomy.
Nevertheless, the cardiology report, normal transthoracic
echocardiographic findings and the uneventful postoperative course
support the absence of clinically significant structural heart
disease. Third, other potential contributing factors that may have
predisposed this patient to vagal reflex, such as individual
variations in autonomic tone or unrecognized cardiovascular
sensitivity, cannot be definitively excluded.
In conclusion, the exact mechanism of reflex
activation remains speculative, as direct neurophysiological
monitoring was not performed during the procedure, and long-term
follow-up data are limited, although no immediate complications
were observed.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
KY was responsible for anesthetic management and
initial case documentation. MA conceptualized the case report,
conducted the literature review and drafted the manuscript. Both
authors revised the manuscript critically for important
intellectual content. Both authors have read and approved the final
manuscript. KY and MA confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
The present case report was exempted from
institutional review board approval as it involved a single
clinical case with no experimental intervention. Written informed
consent for participation in the present case report was obtained
from the patient.
Patient consent for publication
Written informed consent for the publication of the
present case report and any accompanying images was obtained from
the patient.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, Fig. 3 was created using ChatGPT-4 (OpenAI)
based on anatomical and neurophysiological descriptions provided by
the authors. All other content in this manuscript was written by
the authors without AI assistance.
References
|
1
|
Taufique Z, Dion GR and Amin MR: Asystole
during direct laryngoscopy for vocal fold injection in a healthy
patient. J Voice. 31:517.e19–517.e21. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Saha M, Singh A, Pentapati KC, Gadicherla
S, Aramanadka C and Kudva A: The role of throat packs in
orthognathic Surgery-A systematic review and Meta-analysis.
ScientificWorldJournal. 2025(9229475)2025.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Redmann AJ, White GD, Makkad B and Howell
R: Asystole from direct laryngoscopy: A case report and literature
review. Anesth Prog. 63:197–200. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Meng J, Wang Y, Kehar M and Popilevsky L:
Asystole following jaw thrust maneuver: A case report. Cureus.
16(e71077)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Hoshijima H, Takeuchi R, Kikuchi K and
Mizuta K: Asystole triggered by the mouth opening with a dental
mouth gag under general anesthesia during pediatric oral surgery:
Report of a rare case. J Oral Maxillofac Surg. 79:1862–1865.
2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Norcliffe-Kaufmann L: The Vagus and
glossopharyngeal nerves in two autonomic disorders. J Clin
Neurophysiol. 36:443–451. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Higuchi S, Takeshita A, Higashi H, Ito N,
Imaizumi T, Matsuguchi H and Nakamura M: Lowering calcium in the
nucleus tractus solitarius causes hypotension and bradycardia. Am J
Physiol. 250:H226–H230. 1986.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Campagna JA and Carter C: Clinical
relevance of the Bezold-jarisch reflex. anesthesiology.
98:1250–1260. 2003.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chung MY, Shin MJ, Cha SH and Lee JY:
Transient asystole during balloon dilation of the Eustachian tube:
A case report. Medicine (Baltimore). 101(e31720)2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Baraka A: Severe bradycardia following
propofol-suxamethonium sequence. Br J Anaesth. 61:482–483.
1988.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Yasuma F and Hayano J: Respiratory sinus
arrhythmia: Why does the heartbeat synchronize with respiratory
rhythm? Chest. 125:683–690. 2004.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Wieling W, Thijs RD, van Dijk N, Wilde
AAM, Benditt DG and van Dijk JG: Symptoms and signs of syncope: A
review of the link between physiology and clinical clues. Brain.
132:2630–2642. 2009.PubMed/NCBI View Article : Google Scholar
|