Introduction
Arterial hypertension is a major modifiable risk
factor for cardiovascular morbidity and mortality. The prevalence
of hypertension, particularly systolic hypertension, increases with
age. Due to arterial stiffening and frailty in older patients, the
careful management of hypertension is essential (1). Older patients with hypertension have an
increased vulnerability to developing adverse events. For this
reason, it is recommended that the Systemic Coronary Risk
Evaluation Older Persons (SCORE2-OP) system be used in clinical
practice in the follow-up period to manage older patients with
hypertension who are not already at a high or very high risk
(2). The appropriate management of
blood pressure in this population is a priority for clinicians. The
administration of anti-hypertensive drugs should always take into
consideration the benefits and risks associated with treatment,
such as the development of adverse drug events, such as acute
kidney injury (AKI), hypotension, falling, hyperkalemia, etc
(3,4). In addition to cardiovascular disease
risk stratification, a comprehensive geriatric-based evaluation is
essential to guide management decisions regarding these older
adults, since individualized decisions are often required (1).
In the American Heart Association 2025 hypertension
guideline, the authors draw attention to how, among middle-aged and
older adults, the use of intensive vs. standard blood pressure
targets has increased the risk of developing adverse events in
patients with orthostatic hypotension (OH). OH has been reported at
rates of 7-10% in hypertensive adults, particularly among those who
are older. OH is also associated with the use of anti-hypertensive
drugs. It is critical to screen for OH prior to initiating or
intensifying anti-hypertensive treatment, and to monitor for
hypotension during treatment (5).
The management of coronary artery disease in older
patients requires a complex and multidisciplinary approach. In
addition to complications related to surgery, malnutrition and poor
physical performance also affect patient prognosis (6). The present case report describes the
case of patient with AKI related to the use of anti-hypertensive
drugs who was operated on for ischemic heart disease and aortic
valve stenosis.
Case report
A 76-year-old diabetic female patient was admitted
with fatigue to the nephrology outpatient clinic of Adana Acibadem
Hospital on May 14, 2025. The patient experienced hypotension
(systolic blood pressure, 80 mmHg), dizziness, weakness and had
fallen to the ground at home. At that time, there was no history of
loss of consciousness, weakness or vomiting. Large ecchymoses
developed at the periorbital and gluteal regions, and legs. While
her systolic blood pressure was measured at 80 mmHg, in the
following days, she had continued to use anti-hypertensive drugs.
She was hospitalized due to abnormal renal function tests, a blood
urea nitrogen (BUN) level of 144 mg/dl and a creatinine level of
10.30 mg/dl on day 8 after the fall and hypotensive attack. She
denied any changes in urine volume and color. Abnormal findings
upon a physical examination were low blood pressure (80/60 mmHg in
a sitting and standing position), ecchymoses at the periorbital
regions and legs, arrhythmic heart sounds, prosthetic heart valve
sound, jugular venous distension, positive hepatojugular reflux and
pretibial edema.
The medical history of the patient included diabetes
mellitus (DM), hypertension, and coronary artery bypass graft
(CABG) and surgical aortic valve replacement (SAVR).
Surgical procedure
Simultaneous CABG which involved the autogenous vein
graft repair of five veins (internal mammary artery and saphenous
vein), as well as SAVR (biological valve; a no. 23 Edwards valve
was surgically implanted).
Post-operative course and
complications
During the early post-operative period, no
complications developed. On post-operative day 10, the patient was
discharged from the hospital. Cordarone (amiadorone) at 2x200
mg/day, cilazapril at 5 mg, hydrochlorothiazide at 12.5 mg
(Inhibace Plus 5/12.5), warfarin at 1x5 mg/day, furosemide (Lasix
tab) and insulin were prescribed. On post-operative day 34, a
hematoma and abscess that had developed at the lower end of the
sternum were drained and metoprolol (2x50 mg/day) was
commenced.
Findings, management and
follow-up
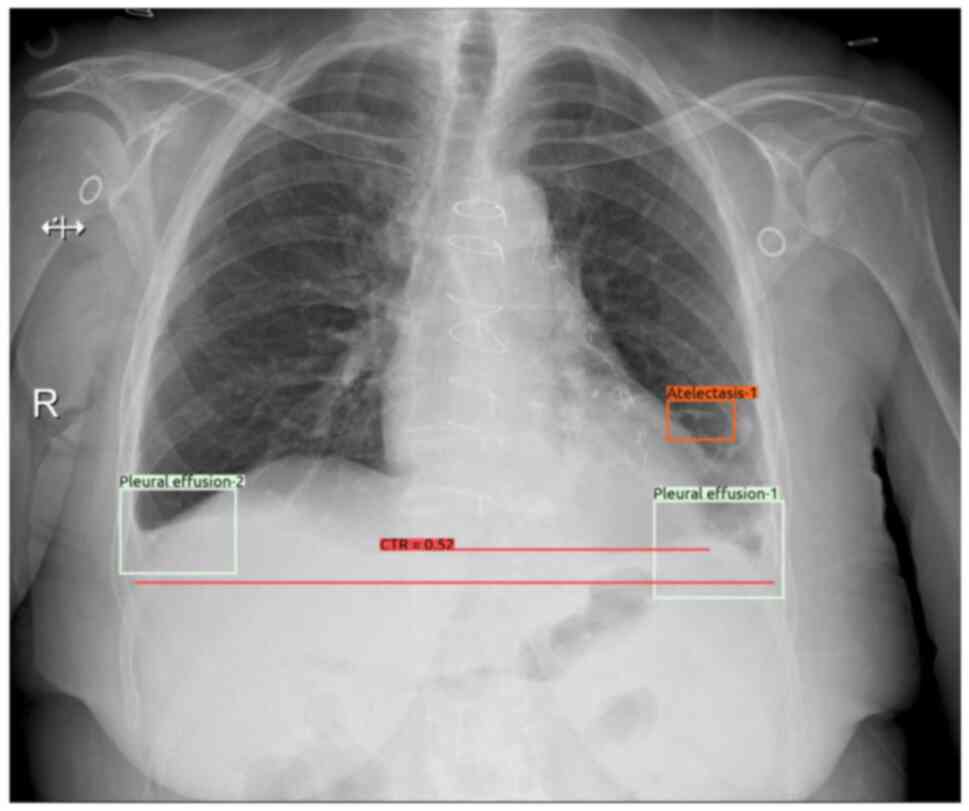
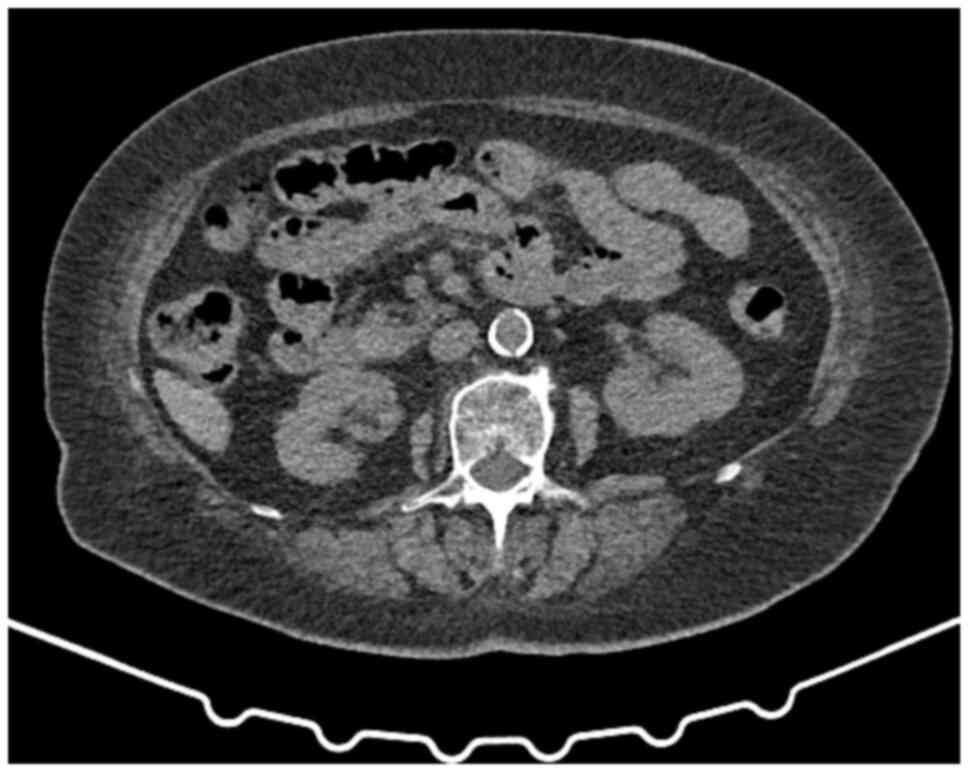
The results of laboratory tests are presented in
Table I. An abdominal
ultrasonographic examination revealed grade 1 renal parenchymal
disease without obstruction. Bilateral pleural fluid, cardiomegaly
and metallic suture and clip secondary to CABG and SAVR were
determined in the chest X-ray and the lower sections of the
thoracic computed tomography scan revealed no abnormalities in the
renal parenchyma and collecting system (Figs. 1 and 2). Echocardioraphic measurements are
presented in Table II.
 | Table IResults of hematological and renal
function tests during the follow-up period. |
Table I
Results of hematological and renal
function tests during the follow-up period.
| Parameters | Pre-operative | A: Day 61; B: Day
5 | A: Day 65; B: Day
8 | A: Day 69; B: Day
14 | A: Day 74; B: Day
19 | A: Day 78; B: Day
23 | A: Day 82; B: Day
29 | A: Day 97; B: Day
45 |
|---|
| Hb (g/dl) | 10.9 | 10.3 | 8.6 | 8.6 | 8.5 | | 9.5 | 10.3 |
| WBC (cells/cumm) | 9,180 | 9,330 | 7,380 | 6,730 | 6,890 | | 6,490 | 5,990 |
| BUN (6-20 mg/dl) | 18 | 114 | 126 | 103 | 98 | 69 | 42 | 18 |
| Creatinine (0.55-1.02
mg/dl) | 0.92 | 10.30 | 10.00 | 10.00 | 9.14 | 5 | 2.39 | 1.13 |
| Sodium (136-145
mEq/l) | 143 | 126 | 124 | 136 | 138 | 143 | 141 | 143 |
| Potassium (3.5-5.1
mEq/l) | 4.4 | 5.28 | 5.67 | 4.78 | 3.93 | 4.62 | 3.56 | 4.13 |
| Calcium (8.6-10
mg/dl) | 9.84 | 5.94 | 5.83 | 7.29 | 7.63 | 7.61 | 8.34 | |
| Phosphorus (2.5-4.9
mg/dl) | | 11 | 11.40 | 6.61 | 7.29 | 3.48 | 3.14 | |
| PT INR
(0,8-1.25) | 1.09 | 1.63 | 2.40 | 2.40 | 2.88 | 2.88 | 1.83 | |
| Blood pressure
mmHg | 130/70 | 117/67 | 106/68 | 115/58 | 114/70 | 125/72 | | |
| Pulse per
minute | | 60 | 70 | 102 | 60 | 70 | | |
| Urine volume day
(ml) | | 1,200 | 1,250 | 2,750 | 1,250 | 1,600 | | |
| Urine density | 1.030 | 1.005 | 1.005 | 1.015 | | | | 1.020 |
| Table IIEchocardiographic measurements of the
patient. |
Table II
Echocardiographic measurements of the
patient.
| Parameters | March 14, 2025;
pre-operative day 5 | May 12, 2025;
post-operative day 54 | June 25, 2025;
post-operative day 98 |
|---|
| Left atrium
(mm) | 43 | 46 | 16 |
| Interventricular
septum (mm) | 14 | 15 | 13 |
| Left ventricular
posterior wall thickness (mm) | 13 | 14 | 11 |
| Left ventricular
ejection fraction (%) | 68 | 70 | 71 |
| Aortic mean
gradient (mHg) | 4,6 | 7 | 5 |
| Aortic peak
gradient (mmHg) | 4-6 | 7 | 5 |
| Pulmonary arterial
pressure | | 38 | |
Clinical management
Anti-hypertensive medications were discontinued. The
systolic blood pressure was targeted to be 120-150 mmHg.
Hyponatremia was asymptomatic and secondary to hypervolemia and
dilutional. Intravenous (IV) furosemide at 300 mg/day and oral
isosorbid-5-mononitrate at 20 mg/day were initiated. Warfarin was
continued as 1x1.25 mg/day according to target level an
international normalized ratio (INR) of 2-3. The insulin dose was
adjusted to maintain blood sugar levels at 110-150 mg/dl. As
regards blood gases, the pH and HCO3 were >7.3 and
>19, respectively. The patient had nonoliguric AKI. Oral calcium
acetate was administered for hyperphosphatemia and hypocalcemia,
and IV calcium infusion was administered. On the 14th day of
hospitalization, the serum levels of BUN (107 mg/dl) and creatinine
(11 mg/dl) began to decrease. Dialysis was not performed and she
was discharged on day 15. During an outpatient clinical follow-up,
the patient was asymptomatic and her blood pressure was 120/70
mmHg. At the last visit (45 days after the onset of acute renal
failure and 97 days after CABG/SAVR), the glomerular filtration
rate was 47.3 ml/min. No proteinuria, pyuria, or cell casts were
detected.
Discussion
The present case report described the case of a
76-year-old diabetic woman with AKI and hypertension who underwent
CABG and SAVR. In addition to complications related to surgery,
malnutrition and poor physical performance also affect prognoses.
Despite adverse factors, invasive approaches should not be avoided
in the treatment of ischemic heart disease-myocardial infarction,
and complete revascularization is recommended in the presence of
multivessel disease (6).
AKI and cardiovascular surgery in the
elderly
A critical issue among elderly patients undergoing
cardiovascular surgery is the development of AKI in the
post-operative period. In the early period following SAVR, AKI
lasting <48 h has been reported in 45.1% of elderly patients,
while persistent AKI has been found in 18.6% of patients (7). Independent risk factors for persistent
AKI are severe heart failure (New York Heart Association, Grade
III-IV), moderate renal dysfunction, anemia and AKI (stages 2 and
3). Complications are more common in patients with AKI. Major
adverse events in the hospital occur at a rate of 3.9% in those
without AKI, 4.7% in patients with early-recovery AKI, and 20.6% in
patients with persistent AKI (7).
The patient described herein did not develop AKI in the early
post-operative period; however, AKI stage 3 developed at 2 months
following surgery, and resolved without the loss of the glomerular
filtration rate (GFR). AKI is staged using criteria that assess
changes in the serum creatinine as follows: Stage 1, an increase in
the baseline serum creatinine levels (bSCr) by 1.5-1.9-fold; stage
2, an increase in bSCr by 2-2.9-fold; stage 3, an increase in bSCr
by 3-fold, or an increase in serum creatinine levels to >4.0
mg/dl or the initiation of renal replacement therapy (8).
In a previous study comparing to 190 patients <50
years of age and 388 patients >80 years of age who underwent
CABG, 20.9% of the older patients experienced at least one
post-operative complication compared to 10% of the younger patients
(9). Among the patients >80
years, hypertension and DM were more common. In that study, major
adverse cardiac and cerebrovascular events (MACCE) were more common
among elderly patients with advanced heart failure and
cerebrovascular accidents. Mortality occurred in 79.4% of the
elderly patients who developed MACCE. In patients with a high
ejection fraction, MACCE was lower. As regards post-operative
complications in patients <50 years of age, the risk factor was
emergency admission (9). In the
patient in the present study, MACCE did not develop following
combined CABG and SAVR.
Pre-operative neurocognitive function is a key
factor affecting complications and the length of hospitalization
following transcatheter aortic valve replacement in elderly
patients (10). The pre- and
post-operative neurological condition of the patient described
herein was good.
Oral anticoagulants and AKI in
patients undergoing valve replacement
Bleeding is a critical issue in valve replacement
patients due to the anticoagulants. In the patient described
herein, a hematoma and abscess developed at the incision site in
the lower sternum in the early post-operative period and rapidly
resolved with drainage and antibiotic therapy. The type of
anticoagulants used in patients undergoing bioprosthetic valve
replacement is critical. Compared to warfarin, new oral
anti-coagulants (NOACs) were found to be safer in the REVERSE study
(11). Rivaroxaban was used for
early post-operative anticoagulation in patients undergoing
bioprosthetic valve surgery for 6 months in the REVERSE trial.
Rivaroxaban, an NOAC, was found to be safe and effective compared
to warfarin. Warfarin was prescribed as an anticoagulant (11). Early post-operative period bleeding
developed in the patient in the present study. The dose was
adjusted to target an INR of 2-3 in the patient described herein,
and bleeding was not observed at a later period. Although bleeding
was considered as a potential cause of AKI, urine analysis and
imaging (Fig. 2) did not support
this etiology. Another etiology of AKI may have been acute
interstitial nephritis (AIN) due to incision site abscess,
infection and the drugs/antibiotic(s) used in the post-operative
period. However, proteinuria, eosinophilia and pyuria, as well as
kidney failure supporting a diagnosis of AIN, were not detected in
the patient in the present study. The history of hypotension at
home following discharge and continuing cilazapril (5 mg),
hydrochlorothiazide (12.5 mg) (ACEI) therapy during this period
suggested hemodynamic AKI/acute tubular necrosis (ATN) in the
patient described herein. An older age, hypotension due to
anti-hypertensive therapy and heart failure may be considered
predisposing factors for ATN. During the AKI (ATN), a urine test
revealed a density of 1.005 and a few erythrocytes (after urinary
catheterization) with traces of protein. At the last out-patient
clinic visit, the urine density of the patient was 1.020, and the
absence of proteinuria and hematuria support the possibility that
AKI/ATN had improved.
Changes in renal function are critical for making
prognoses in elderly patients undergoing valve replacement surgery.
In a previous study, in 4,531 patients >60 years of age, a
post-operative GFR decrease of >50% compared to pre-operative
GFR was an independent risk factor for hospital mortality and
all-cause mortality at the 1-year follow-up (12).
Patients with chronic kidney disease (CKD) requiring
cardiovascular surgery have a high comorbidity, similar to elderly
patients. In a previous study, renal function remained stable or
improved after 1 month in >80% of patients with CKD who
underwent transcatheter valve replacement (13). In addition, the 2-year mortality was
lower in patients with improved renal function. Mortality was found
to be higher in patients with deteriorating renal function.
Therefore, in patients requiring transcatheter aortic valve
implantation (TAVI), cardiorenal syndrome may be a possible cause
of CKD, and cardiac and renal function may improve after the
procedure (13).
SAVR or TAVI
SAVR in elderly patients is controversial. In the
present study, the 76-year-old patient underwent a surgical
bioprosthetic heart valve replacement. In a previous study, TAVI
was more advantageous in the early post-operative period when
comparing TAVI and redo-aortic valve replacement (redo-AVR) in
terms of prognosis in patients with bioprosthetic valve
insufficiency 14). Hospital mortality was 7.2% in the redo-AVR
group and 0% in the TAVI group. The need for intra-aortic balloon
pump support, early re-operation, respiratory and neurological
complications, and multiorgan failure were higher in the surgical
group. The TAVI group had a shorter period of intensive care and
hospitalization, but moderate aortic leakage and postprocedural
gradients at discharge. In patients discharged from the hospital
after successful procedures, the prognosis at the 6-year follow-up
was similar after both TAVI and SAVR (14).
In another study, in elderly patients with aortic
stenosis (AS) who underwent SAVR with partial mini-sternotomy, the
quality of life was lower compared to patients who underwent
transfemoral TAVI (15). However,
patients who underwent SAVR with partial upper mini-sternotomy had
improved technical outcomes, with fewer pacemaker implantations and
less paravalvular leakage. SAVR required more blood transfusions,
longer ventilation and a longer period of hospitalization in the
intensive care unit (15). The
patient in the present study was hospitalized due to the
development of a hematoma and abscess at the sternotomy site
following SAVR. In patients with AS and end-stage renal disease, as
in numerous elderly patients, TAVI has been shown to be associated
with a lower hospital mortality, fewer complications, shorter
periods of hospitalization, lower treatment costs, and a higher
rate of discharge to home compared to SAVR despite the increased
comorbidities and disease burden (16). In another study, in the SAVR group
with chronic heart failure and symptomatic AS, the comorbid burden
was higher compared to the TAVI group, although hospital mortality
was similar (17). However,
cardiovascular, respiratory and renal issues were less common in
patients who underwent TAVI. Therefore, TAVI can be considered
safer in these patients (17).
A significant association was previously found
between increased serum creatinine levels and the prognosis of
patients who underwent SAVR (18).
In a long-term follow-up, all-cause mortality was similar in
patients with no or minimal increases in early serum creatinine.
The 30-day mortality was increased in patients with increased serum
creatinine levels. The risk of developing heart failure and chronic
renal failure was minimally increased (18). Quality of life was found to be
improved in elderly patients who underwent SAVR and the risk of
reoperation due to structural degeneration was lower. Mortality was
increased in non-valvular noncoronary procedures combined with SAVR
(19).
Isolated aortic valve replacement or
valve replacement combined with coronary artery surgery
In a previous study, in patients >75 years with
isolated SAVR, the duration of hospitalization and mechanical
ventilation, the need for dialysis, and the mortality were lower in
the early period compared to combined CABG and SAVR (20). Long-term mortality did not differ
between the groups (20).
Predictive score for the outcomes of
cardiovascular surgery
In a previous study, pre-operative EUROSCORE and
Thoracic Surgeon risk scores were not found to be useful in
assessing postoperative complications and prognosis in elderly
patients undergoing SAVR (21).
Mechanical or bioprosthetic valve
replacement
An SAVR bioprosthetic valve was used in the patient
in the present study. Compared to the outcome for bioprosthetic
valves, mechanical valve implantation in the 50-65 age group has
demonstrated improved results for long-term survival with fewer
major adverse events and fewer re-operations required (22).
Invasive or conservative treatment in
the elderly with coronary ischemic heart disease
In the ISCHEMIA trial, 1,236 patients with
three-vessel coronary artery disease were evaluated (23). The revascularization group [612
patients; invasive group (CABG/percutaneous intervention)] was
compared with the conservative group (624 patients; medical
treatment), and cardiovascular mortality and myocardial infarction
was found to be less common, while quality of life was improved
over a period of 4 years in the invasive group. The differences in
all-cause mortality rates between revascularization and
conservative were, however, small, with wide confidence intervals
(23).
Hypertension treatment
It should be remembered that hypotension can develop
more frequently in the treatment of hypertensive elderly patients.
Hypotension may impair cerebral and renal perfusion due to arterial
stiffness, leading to AKI and other complications. OH has been
reported at a rate of 7-10% in hypertensive adults, especially in
older patients, and is also associated antihypertensive drugs
(5). In the patient described
herein, standard antihypertensive therapy caused hypotension and
AKI, falls and ecchymosis. It is thus critical to measure blood
pressure at home, and patients and their family need to be informed
what the target blood pressure level is. Patients should be
encouraged to contact their physician if they experience abnormal
blood pressure values. Preventive measures such as good control of
blood pressure can reduce complications. In a previous study, the
most common adverse events among 6,580 patients, including 1,237
patients with heart failure with reduced ejection fraction treated
with four drugs were hypotension, AKI (mean 28 days) and
hyperkalemia (24).
Renin-angiotensin system inhibitors are recommended
as the first-line treatment for hypertension in the elderly
(25). In one cohort, severe
side-effects were observed with anti-hypertensive therapy; however,
the absolute risk was low, apart from elderly patients with
moderate or severe frailty (26).
The likelihood of benefit from treatment in this group of patients
was similar to the risks of hypotension, falls, AKI, electrolyte
disturbances and syncope. Therefore, physicians may avoid
prescribing new medications and consider alternative approaches
when treating these patients (26).
In general, stringent blood pressure control
improves cardiovascular outcomes in hypertensive patients. In the
majority of subpopulations, intensive blood pressure control is
preferred over less intensive blood pressure control, although the
data for patients with diabetes or cardiovascular disease are less
clear (27). It is not recommended
to overtreat hypertension in elderly patients (28). In the patient in the present study,
AKI stage 3 developed secondary to hypotension. In critically ill
elderly patients, the added stress factor of age-related structural
deterioration and diminished renal reserve increases susceptibility
to renal function deterioration. Age is an independent risk factor
for the development of AKI. Therefore, physicians should consider
changes in renal function in elderly patients and implement
preventive measures (29).
Arrhythmia during cardiovascular
surgery
The patient in the present study developed atrial
fibrillation (AF) in the post-operative period. AF is the most
common arrhythmia that develops following cardiac surgery.
Cardiopulmonary bypass disrupts systemic homeostasis by triggering
oxidative stress and ischemia-reperfusion injury, an inflammatory
cascade. Prolonged aortic cross-clamping >60-75 min further
triggers myocardial ischemia and structural remodeling, increasing
the risk of developing post-operative AF (30). Post-operative AF following isolated
CABG surgery has been reported at a frequency of 30.94%. Risk
factors for the development of AF include an advanced age,
hypertension, smoking, coronary bypass time and a low EF (31). In the patient described herein, AF
was controlled with metoprolol.
In conclusion, mortality and morbidity are increased
in elderly patients following cardiovascular surgery, and periods
of hospitalization are longer. Invasive approaches should not be
avoided in the treatment of ischemic heart disease or myocardial
infarction, and complete revascularization is recommended in the
presence of multi-vessel disease. Although early mortality is high
in patients undergoing CABG and SAVR, the long-term prognosis is
similar to that of patients who undergo single SAVR and combined
surgery. According to the REVERSE study (11), NOACs are recommended for patients
requiring post-operative anticoagulants. Notably, the patient in
the present study developed hypotension and acute renal failure
related to standard anti-hypertensive drugs. Due to the increased
risk of renal failure in elderly patients, it is important to avoid
hypotension and implement preventive measures. The overtreatment of
hypertension in the elderly should be avoided.
In general, there is a need for greater caution
regarding hypotension and OH in the treatment of hypertension in
elderly patients, particularly those with comorbid conditions.
Clinicians should note that while high blood pressure is dangerous,
excessively low blood pressure can also cause complications, such
as falls, AKI and hospitalization. It is important that blood
pressure management be individualized in accordance with
guidelines. Patients should be encouraged to measure their blood
pressure at home, and written blood pressure target values should
be provided to both the patient and their caregivers.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SP evaluated and followed-up the patient for
nephrological issues, prepared the article and conducted the
literature review. ATS evaluated and followed-up the patient for
cardiovascular issues, and diagnosed AS and ischemic coronary heart
disease. SP and ATS confirm the authenticity of all the raw data.
Both authors have read and approved the final manuscript.
Ethical approval and consent to
participate
The present report was carried out in accordance
with the Declaration of Helsinki. The patient provided their
written consent to participate.
Patient consent for publication
The patient provided their written consent for the
publication of the present case report and any related images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bahat G, Ribeiro H, Sheppard JP, Bogaerts
JMK, Camafort M, Dallmeier D, De Backer T, Desideri G, Olszanecka
A, Persu A, et al: Twelve hot questions in the management of
hypertension in patients aged 80+ years and their answers with the
help of the 2023 European Society of Hypertension Guidelines. J
Hypertens. 42:1837–1847. 2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
SCORE2-OP working group and ESC
Cardiovascular risk collaboration. SCORE2-OP risk prediction
algorithms: estimating incident cardiovascular event risk in older
persons in four geographical risk regions. Eur Heart J.
42:2455–2467. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hohl CM, Dankoff J, Colacone A and Afilalo
M: Polypharmacy, adverse drugrelated events, and potential adverse
drug interactions in elderly patients presenting to an emergency
department. Ann Emerg Med. 38:666–671. 2001.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bourgeois FT, Shannon MW, Valim C and
Mandl KD: Adverse drug events in the outpatient setting: An 11-year
national analysis. Pharmacoepidemiol Drug Saf. 19:901–910.
2010.PubMed/NCBI View
Article : Google Scholar
|
|
5
|
Writing Committee Members*. Jones DW,
Ferdinand KC, Taler SJ, Johnson HM, Shimbo D, Abdalla M, Altieri
MM, Bansa N, Bello NA, Bress AP, et al: 2025
AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM
Guideline for the Prevention, Detection, Evaluation and Management
of High Blood Pressure in Adults: A Report of the American College
of Cardiology/American Heart Association Joint Committee on
Clinical Practice Guidelines. Hypertension. 82:e212–e316.
2025.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pavasini R, Biscaglia S, Kunadian V,
Hakeem A and Campo G: Coronary artery disease management in older
adults: Revascularization and exercise training. Eur Heart J.
45:2811–2823. 2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lin YW, Wang Q, Lu PS, Jiang M, Li XH,
Wang SH, Liao X, Zeng QC, Yu DQ and Wei XB: Early acute kidney
injury recovery in elderly patients undergoing valve replacement
surgery. J Cardiothorac Vasc Anesth. 38:2261–2268. 2024.PubMed/NCBI View Article : Google Scholar
|
|
8
|
KDIGO: KDIGO Clinical Practice Guideline
for Acute Kidney Injury (AKI) and Acute Kidney Disease (AKD)/
Update 2023. https://kdigo.org › wp-content › uploads
› 2023/10.
|
|
9
|
Piątek J, Kędziora A, Kiełbasa G,
Olszewska M, Sobczyk D, Song BH, Konstanty-Kalandyk J, Darocha T,
Wierzbicki K, Milaniak I, et al: How to predict the risk of
postoperative complications after coronary artery bypass grafting
in patients under 50 and over 80 years old. A retrospective
cross-sectional study. Kardiol Pol. 75:975–982. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bobet AS, Brouessard C, Le Tourneau T,
Manigold T, de Decker L and Boureau AS: Length of stay in older
patients undergoing transcatheter aortic valve replacement: Value
of a geriatric approach. Gerontology. 68:746–754. 2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Wang X, Zhang C, Pan MM, Lin HW, Xue S,
Xie B and Gu ZC: Design and rationale of the multicenter randomized
clinical trial (REVERSE): Efficacy and safety of rivaroxaban in the
early postoperative period for patients with bioprosthetic valve
replacement or valve repair. Int J Cardiol.
425(133023)2025.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yang L, Wu ZJ, Weng H, Wu D, Lu JQ and
Chen SL: The prognostic value of estimated glomerular filtration
rate change in elderly patients undergoing valvular replacement
surgery. Arch Gerontol Geriatr. 130(105719)2025.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Witberg G, Steinmetz T, Landes U, Pistiner
Hanit R, Green H, Goldman S, Vaknin-Assa H, Codner P, Perl L,
Rozen-Zvi B and Kornowski R: Change in kidney function and 2-year
mortality after transcatheter aortic valve replacement. JAMA Netw
Open. 4(e213296)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gatta F, Haqzad Y, Gradinariu G, Malvindi
PG, Khalid Z, Suelo-Calanao RL, Moawad N, Bashir A, Rogers LJ,
Lloyd C, et al: Redo aortic valve replacement versus valve-in-valve
trans-catheter aortic valve implantation: A UK propensity-matched
analysis. Monaldi Arch Chest Dis. 94(1):2023.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Andrási TB, Schellenberg C, Vasiloi A and
Glück AC: Health-related quality of life after minimal-invasive
treatment of aortic valve stenosis in the elderly. J Thorac Dis.
16:2274–2284. 2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Khan MZ, Khan MU, Kalra A, Krupica T,
Kaluski E and Khan SU: Transcatheter versus surgical aortic valve
replacement in patients with end stage renal disease. Catheter
Cardiovasc Interv. 96:1102–1109. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Mubashir T, Balogh J, Chaudhry R, Quiroz
C, Kar B, De Armas IAS, Liang Y, Markham T, Kumar R, Choi W, et al:
Transcatheter and surgical aortic valve replacement outcomes for
patients with chronic heart failure. J Cardiothorac Vasc Anesth.
35:888–895. 2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lu R, Dismorr M, Hertzberg D, Glaser N and
Sartipy U: Early creatinine changes after aortic valve replacement
and late survival, heart failure, and chronic kidney disease in a
national registry. Ann Thorac Surg. 119:577–584. 2025.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mourad F, Haddad A, Nowak J, Elbarraki M,
Elhmidi Y, Jasarevic M, Marx P, Demircioglu E, Wendt D, Thielmann
M, et al: Impact of non-valvular non-coronary concomitant
procedures on outcomes of surgical aortic valve replacement in
intermediate risk patients. J Clin Med. 10(5592)2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
D'Alessandro S, Tuttolomondo D, Singh G,
Hernandez-Vaquero D, Pattuzzi C, Gallingani A, Maestri F, Nicolini
F and Formica F: The early and long-term outcomes of coronary
artery bypass grafting added to aortic valve replacement compared
to isolated aortic valve replacement in elderly patients: A
systematic review and meta-analysis. Heart Vessels. 37:1647–1661.
2022.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Taleb Bendiab T, Brusset A, Estagnasié P,
Squara P and Nguyen LS: Performance of EuroSCORE II and Society of
Thoracic Surgeons risk scores in elderly patients undergoing aortic
valve replacement surgery. Arch Cardiovasc Dis. 114:474–481.
2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Florian A, Auer J, Reichardt B, Krotka P,
Wagenlechner C, Wendt R, Mildner M, Mascherbauer J, Ankersmit HJ,
Zimpfer D and Graf A: The choice of surgical aortic valve
replacement type and mid-term outcomes in 50 to 65-year-olds:
results of the AUTHEARTVISIT study. Eur J Cardiothorac Surg.
67(ezaf200)2025.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Bangalore S, Rhodes G, Maron DJ,
Anthopolos R, O'Brien SM, Jones PG, Mark DB, Reynolds HR, Spertus
JA, Stone GW, et al: Outcomes with revascularisation versus
conservative management of participants with 3-vessel coronary
artery disease in the ISCHEMIA trial. EuroIntervention.
20:e1276–e1287. 2024.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Lin S, Zhao R, Zhang H, Liang Y, Lin J, Yu
M, Li D, Zhang B, Ma L and Peng L: Assessing the risk of acute
kidney injury associated with a four-drug regimen for heart
failure: A ten-year real-world pharmacovigilance analysis based on
FAERS events. Expert Opin Drug Saf. 24:547–556. 2025.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Villain C, Metzger M, Liabeuf S, Hamroun
A, Laville S, Mansencal N, Combe C, Fouque D, Frimat L, Jacquelinet
C, et al: Effectiveness and tolerance of renin-angiotensin system
inhibitors with aging in chronic kidney disease. J Am Med Dir
Assoc. 23:998–1004. e7. 2022.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Sheppard JP, Koshiaris C, Stevens R,
Lay-Flurrie S, Banerjee A, Bellows BK, Clegg A, Hobbs FDR, Payne
RA, Swain S, et al: The association between antihypertensive
treatment and serious adverse events by age and frailty: A cohort
study. PLoS Med. 20(e1004223)2023.PubMed/NCBI View Article : Google Scholar
|
|
27
|
D'Anci KE, Tipton K, Hedden-Gross A, Rouse
B, Hermanson L and Fontanarosa J: Effect of intensive blood
pressure lowering on cardiovascular outcomes: A systematic review
prepared for the 2020. U.S. Department of veterans affairs/U.S.
department of defense guidelines. Ann Intern Med. 173:895–903.
2020.PubMed/NCBI View
Article : Google Scholar
|
|
28
|
Angeli F, Reboldi G and Verdecchia P:
Blood pressure goal for hypertension in the elderly. G Ital Cardiol
(Rome). 24:305–309. 2023.PubMed/NCBI View Article : Google Scholar : (In Italian).
|
|
29
|
Perschinka F, Boyer N, Forni LG and
Joannidis M: Renal function in very old critically ill patients.
Curr Opin Crit Care. 29:534–541. 2023.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ballas C, Katsouras CS, Tourmousoglou C,
Siaravas KC, Tzourtzos I and Alexiou C: A review on the etiologies
of the development of atrial fibrillation after cardiac surgery.
Biomolecules. 15(374)2025.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Zhou JY, Zhang JL, Xi L, Guo ZP, Liu XC,
Liu ZG, Yang Q and He GW: Risk factors of postoperative atrial
fibrillation after isolated coronary artery bypass grafting surgery
in the recent 10 years: Clinical analysis of 6229 patients. Clin
Cardiol. 47(e24335)2024.PubMed/NCBI View Article : Google Scholar
|