Introduction
Venous thromboembolism (VTE) is a major cause of
morbidity and mortality. However, the mechanisms of the
predisposition remain unclear. Mild or moderate
hyperhomocysteinemia is a known risk factor for venous
thrombophilia as a single disorder or in combined defects (1,2).
Hyperhomocysteinemia occurs due to a combination of genetic and
environmental factors (3,4). Several mutations or combined defects
affecting the homocysteine (Hcy) pathway have been reported
(5,6). A polymorphism, C677T, in the
methylenetetrahydrofolate reductase (MTHFR) gene, is responsible
for the Ala223Val substitution (7)
in a highly conserved residue of the molecule. The substitution
renders the enzyme thermolabile and has been recognized as a cause
of intermediate hyperhomocysteinemia. Previous findings have
revealed that subjects carrying the MTHFR mutation in a homozygous
condition have significantly higher homocysteine levels than those
of heterozygotes or normal homozygotes, particularly when folate
levels are in the low-normal range (8). These subjects may be at increased
risk of cardiovascular disease. However, not all previous studies
have reported a direct association between the C677T mutation and
VTE or arterial vascular disease. Therefore, the correlation
between the C677T mutation and VTE or arterial vascular disease
remains controversial. Moreover, the frequency of the mutated
allele is high and the mutation has a significantly heterogeneous
distribution among various ethnic groups. In the present
population-based case-control study, we analyzed the frequency of
the C677T polymorphism in the MTHFR gene of patients in China with
VTE, in comparison with individuals without evidence of the
disease. In addition, we evaluated the association between this
polymorphism and plasma Hcy levels. The possible interactive
effects of tobacco smoking with risk factors for VTE were also
evaluated.
Patients and methods
Subjects
Between September 2008 and March 2010, 440 patients
(211 males and 229 females) were diagnosed with lower extremity
deep venous thrombosis (DVT) by duplex ultrasonography at Shandong
Provincial Hospital, Shandong University (Jinan, China) and were
recruited into the VTE group. The mean age was 44.7±7.5 years
(range, 28–90); 274 (62.3%) were outpatients and 166 (37.7%) were
hospitalized patients. Patients with hematological diseases, liver
or kidney dysfunction, infections, autoimmune diseases, tumors or
those receiving thrombolytic treatment or anticoagulant treatment
were excluded from this study. Venous thrombosis was localized to
the left side in 298 patients (67.7%), the right side in 125
patients (28.4%) and both sides in 17 patients (3.9%). A total of
16 patients had pulmonary embolism (PE; 3.6%). A total of 440
healthy unrelated subjects who had no previous diagnoses of VTE or
other associated diseases were recruited into the control group.
The mean age of the control subjects was 46.3±7.6 years (range,
21–82); 236 (53.6%) of the healthy subjects were male and 204
(46.4%) were female. The characteristics of the study population
are shown in Table I. Informed
consent was obtained from all study subjects and the study was
approved by the Shandong University Research Ethics Committee,
China.
 | Table ICharacteristics of participants. |
Table I
Characteristics of participants.
| Characteristic | Controls
(n=440)
n (%) |
Cases(n=440)
n (%) | χ2 | P-value |
|---|
| Age (years) |
| >45 | 193 (43.9) | 178 (40.5) | 1.049 | 0.306 |
| ≥45 | 247 (56.1) | 262 (59.5) | | |
| Gender |
| Male | 236 (53.6) | 211 (52.0) | 2.842 | 0.092 |
| Female | 204 (46.4) | 229 (50.0) | | |
Hcy determination and genotyping
Peripheral venous blood was obtained from each
subject and promptly centrifuged (1,500 rpm for 10 min) following
collection. A DNA extraction kit (Qiagen, Crawley, UK) was used to
extract genomic DNA, according to the manufacturer’s instructions.
The DNA was then stored at −70°C until use. Total Hcy was
quantified using the fluorescence polarization immunoassay (FPIA)
on the IMx analyzer from Abbott Laboratories (Abbott Park, IL,
USA). The IMx Hcy assay is based on the reduction of the plasma
samples with dithiothreitol and the subsequent conversion of free
Hcy to S-adenosyl Hcy by hydrolase in the presence of added
adenosine. The sample and the tracer compete for binding to the
monoclonal antibody. Following the reaction, the level of
S-adenosyl Hcy was evaluated by a fluorescence polarization
immunoassay. The intensity of the polarized light is inversely
correlated with the plasma concentration of Hcy.
Genomic DNA was detected by real-time polymerase
chain reaction (RT-PCR) amplification followed by digestion with
the restriction enzyme HinFI, as described by Frosst et
al (9). The primers were
designed as previously reported (10) with the following sequences for
sense, 5′-GCCCAGCCACTCACTGTTTTA-3′; and antisense,
5′-AGGACGGTGCGGTGAGAGTG-3′, used in a total volume of 25 μl
for amplification. The cycling conditions for PCR were initiation
for 5 min at 94°C, followed by 30 cycles of 40 sec denaturation at
94°C, annealing at 56°C for 4 sec and extension at 72°C for 12 sec.
A final extension step for 7 min at 72°C was also carried out. The
amplified products were stored at 4°C and were later mixed and
buffered with restriction endonuclease HinFI. The products
were then left overnight in a water bath kettle for digestion.
Finally, all products were observed following the 8% polyacrylamide
gel electrophoresis.
Statistical analysis
All statistical analyses were performed using SPSS
13.0 statistical software (SPSS Inc., Chicago, IL, USA) and data
are presented as mean ± standard deviation. Comparisons between two
groups were performed by an independent t-test; Chi-square analysis
was applied to determine the difference in the genotype and gene
frequency. Odds ratios (ORs) and 95% confidence intervals (95% CIs)
were calculated from unconditional logistic regression models. A
value of P<0.05 was considered to indicate a statistically
significant result.
Results
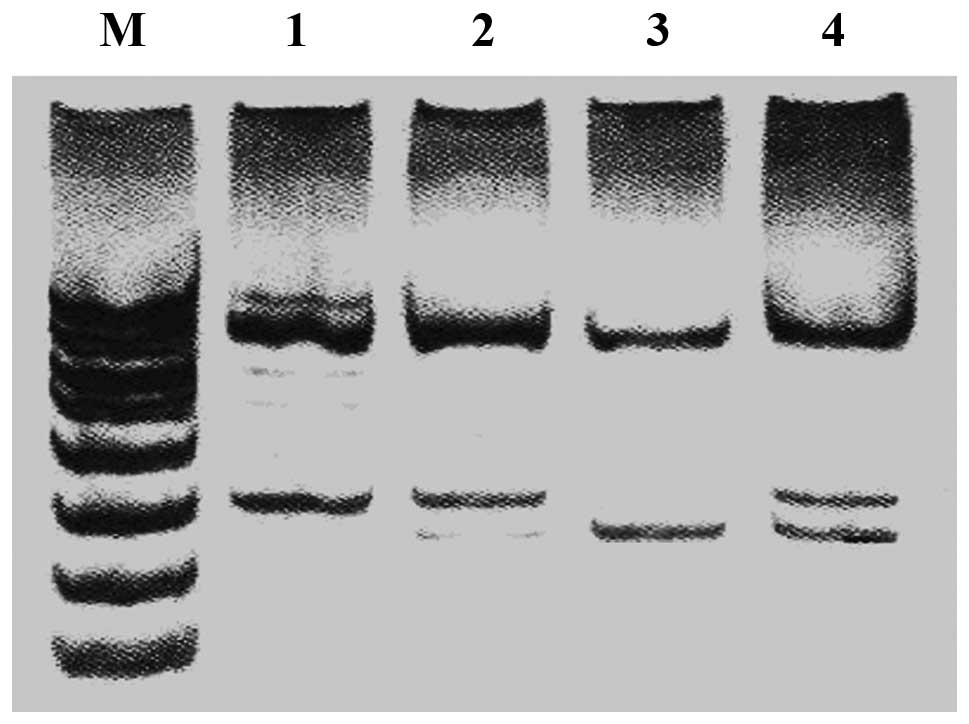
TT genotype is significantly correlated
with an increased risk of VTE
Subjects homozygous for the mutation exhibited two
DNA fragments 175 and 23 bp in length in electrophoresis, whereas
homozygous subjects without the mutation exhibited a DNA fragment
of 198-bp. Heterozygous subjects exhibited three DNA fragments of
198, 175 and 23 bp. Fig. 1 shows
the polyacrylamide gel electrophoresis with restriction
endonuclease HinFI. There were 3 genotypes, CC, CT and TT,
in the MTHFR gene at position 677 in the two groups. Table II shows that the distribution of
the MTHFR C677T gene polymorphisms in the controls were in a state
of Hardy-Weinberg equilibrium. Table
III shows the MTHFR C677T genotype frequencies and allele
frequencies between the two groups. The frequencies of the C and T
alleles were 47.4 and 52.6% in the VTE group and 63.1 and 36.9% in
the controls, respectively (χ2, 47.698; P<0.01). The
MTHFR C677T frequencies of the CC, CT and TT genotypes were 38.5,
35.7 and 25.5% in the VTE group and 41.4, 43.2 and 15.5% in the
controls, respectively (χ2, 14.237; P=0.001). Table IV shows that, compared with the CC
genotype, the TT genotype was significantly correlated with an
increased risk of VTE (OR, 1.753; 95% CI, 1.215–2.529;
P=0.003).
| Table IIMTHFR C677T genotype distribution in
Hardy-Weinberg equilibrium.a |
Table II
MTHFR C677T genotype distribution in
Hardy-Weinberg equilibrium.a
| Gene | Genotype | Predicted value, n
(%) | Observed value, n
(%) | χ2 | P-value |
|---|
| MTHFRC677T | CC | 175 (39.8) | 182 (41.4) | 1.207 | 0.547 |
| CT | 205 (46.6) | 190 (43.2) | | |
| TT | 60 (13.6) | 68 (15.5) | | |
| Table IIIMTHFR C677T genotype frequency and
allele frequency between the two groups. |
Table III
MTHFR C677T genotype frequency and
allele frequency between the two groups.
| Genotypes and
alleles | Controls n (%) | Cases n (%) | χ2 | P-value |
|---|
| C | 557 (63.1) | 499 (47.4) | 47.698 | <0.001 |
| T | 326 (36.9) | 554 (52.6) | | |
| CC | 182 (41.4) | 171 (38.9) | 14.237 | 0.001 |
| CT | 190 (43.2) | 157 (35.7) | | |
| TT | 68 (15.5) | 112 (25.5) | | |
| Table IVMTHFR C677T polymorphism and VTE
risk. |
Table IV
MTHFR C677T polymorphism and VTE
risk.
| Genotype | Controls n (%) | Cases n (%) | OR (95% CI) | P-value |
|---|
| CC | 182 (41.4) | 171 (38.9) | 1 | - |
| CT | 190 (43.2) | 157 (35.7) | 0.879
(0.653-1.184) | 0.440 |
| TT | 68 (15.5) | 112 (25.5) | 1.753
(1.215-2.529) | 0.003 |
| CT+TT | 258 (58.6) | 269 (61.1) | 1.110
(0.847-1.453) | 0.492 |
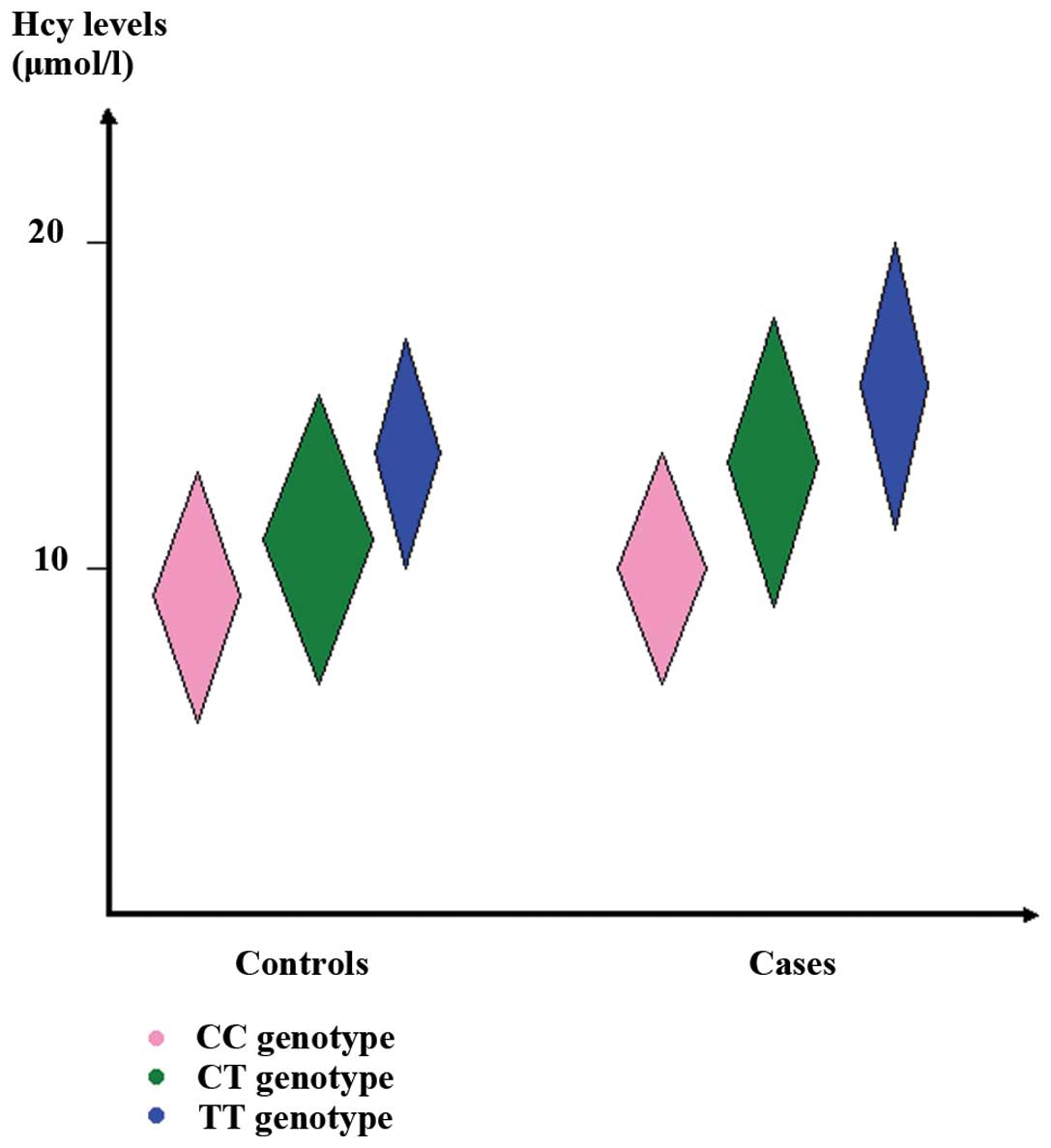
Plasma levels of Hcy are increased in
patients with VTE
The plasma level of Hcy in the VTE group (13.05±2.37
μmol/l) was significantly higher than that in the control
group (11.94±2.03 μmol/l, P<0.001). Levels of Hcy among
various genotypes are shown in Table
V. In the VTE group (F=106.051; P<0.001), the level of Hcy
in subjects with the CT+TT genotype (14.49±2.51 μmol/l) was
significantly higher than that in subjects with the CC genotype
(11.35±1.57 μmol/l, P<0.001). In the control group
(F=100.362; P<0.001), the level of Hcy in subjects with the
CT+TT genotype (12.08±3.53 μmol/l) was significantly higher
than that in subjects with the CC genotype (10.03±1.50
μmol/l, P<0.001). The plasma levels of Hcy in the two
groups are illustrated in Fig. 2.
Regression analysis was used to evaluate an environmental factor
(tobacco smoking) and its possible interaction with the MTHFR gene
C677T polymorphism in influencing venous thrombogenesis. No
interaction was revealed between the MTHFR genotype and tobacco
smoking. Table VI shows the
logistic regression analysis of the interaction of tobacco smoking
with the MTHFR C677T polymorphism in VTE.
| Table VPlasma Hcy levels among different
genotypes. |
Table V
Plasma Hcy levels among different
genotypes.
| Genotype | Cases | Controls | t | P-value |
|---|
| CC | 11.35±1.57 | 10.03±1.50 | 8.078 | <0.001 |
| CT | 11.69±1.73 | 10.58±2.05a | 5.469 | <0.001 |
| TT | 15.87±2.83a,b | 13.92±2.54a,b | 4.656 | <0.001 |
| CT+TT | 14.49±2.51a,b,c | 13.28±2.37a,b,c | 5.685 | <0.001 |
| CC+CT+TT | 13.05±2.37a,b,c,d | 11.94±2.03a,b,c,d | 7.461 | <0.001 |
| F | 106.051 | 100.362 | - | - |
| P-value | <0.001 | <0.001 | - | - |
| Table VILogistic regression analysis on
tobacco usage and MTHFR C677T for interaction in VTE. |
Table VI
Logistic regression analysis on
tobacco usage and MTHFR C677T for interaction in VTE.
| Smoking status | Genotype | Cases n (%) | Controls n (%) | OR (95% CI) | P-value |
|---|
| Smoking | CC | 66 (32.5) | 83 (46.9) | 1 | - |
| CT | 85 (41.9) | 56 (31.6) | 1.909
(1.196-3.046) | 0.009 |
| TT | 52 (25.6) | 38 (21.5) | 1.721
(1.014-2.920) | 0.043 |
| Non-smoking | CC | 105 (44.3) | 109 (41.4) | 1 | - |
| CT | 72 (30.4) | 124 (47.1) | 0.603
(0.406-0.895) | 0.016 |
| TT | 60 (25.3) | 30 (11.4) | 2.076
(1.242-3.470) | 0.007 |
Discussion
Thrombophilia is defined as a disorder of
coagulation that contributes to a predisposition towards thrombosis
(11). Although the term
thrombophilia has been used to describe arterial thrombosis, its
most common usage has been in reference to VTE (12). Thrombophilia is a consequence of
acquired and inherited or genetic causes. Acquired causes include
conditions such as surgery, cancer and prolonged immobilization,
while genetic causes have been linked to the inherited deficiencies
of antithrombin (13), protein C
(14,15) and protein S (14,16).
The identification of the genetic basis of these inherited causes
of thrombophilia has changed the way thrombosis and the importance
of its genetic component are viewed. Interest in the genetic basis
of VTE was accelerated with the subsequent discovery of factor V
Leiden (17), prothrombin G20210A
(18) and MTHFR C677T (19). The identification of new genetic
variants that may either directly or indirectly affect coagulation
or the anticoagulant pathway may greatly advance the understanding
and clinical management of thrombophilia.
Hyperhomocysteinemia is associated with the
occurrence of vascular complications. The significance of
hyperhomocysteinemia in predicting vascular complications in
various locations has been highlighted by several studies (20,21).
The underlying mechanism by which Hcy affects thrombosis is
unclear. Hcy, which is formed from methionine, is either
remethylated into methionine or catabolized via the vitamin
B6-dependent transsulfuration pathway (22). Methionine synthase catalyzes the
remethylation of Hcy and requires 5-methyltetrahydrofolate, as a
substrate, and vitamin B12, as a co-factor, to function.
5-Methyltetrahydrofolate is produced from the reduction of
5,10-methylenetetrahydrofolate by MTHFR, which is thereby a Hcy
metabolism-regulator. However, in the absence of low serum folate,
the presence of a mutation of the MTHFR gene which is responsible
for hyperhomocysteinemia has not been identified as a vascular risk
factor (23). The MTHFR 677T
allele codes for the thermolabile form of MTHFR, a key enzyme in
the conversion pathway of Hcy to methionine. The C677T MTHFR
mutation involves the substitution of an alanine residue for a
valine, which results in a substantial reduction in its
thermolabile enzymatic activity. The C677T MTHFR mutation is a
possible genetic contributor to hyperhomocysteinemia.
Gemmati et al (24) reported that there was a high
prevalence of homozygotes for the mutated MTHFR allele among cases
with VTE disease, suggesting that in selected patients homozygosity
for the MTHFR mutation increases the risk of arterial and venous
thromboses and that differences in selection criteria for the
patient group may be partly responsible for the controversial
association of the MTHFR mutation and vascular disease. Couturaud
et al (25) reported that
the frequency of the C677T mutation MTHFR was 21.8% in its
homozygous state and 34.5% in its heterozygous state. The OR for
having VTE in the presence of the mutation in its homozygous state
was 2.9 (95% CI, 1.0–8.6). Salomon et al (26) suggested that homozygous MTHFR C677T
was an independent risk factor for VTE, with an OR of 2.1. Oger
et al (27) reported that
mild hyperhomocysteinemia, low serum folates and vitamin B12 were
associated with VTE independently of each other. In multivariate
analysis, VTE was associated with mild hyperhomocysteinemia, low
serum folates and vitamin B12. An MTHFR 677TT genotype was not
significantly associated with VTE (OR, 1.13; 95% CI, 0.70–1.81).
Ray et al (28) reported
that the classic MTHFR C677T gene polymorphism is weakly associated
with an increased risk of VTE. It is unlikely that the purported
correlation between hyperhomocysteinemia and VTE is mediated by
this gene defect to a substantial degree, although other
unidentified gene polymorphisms may explain this association. The
main finding of the present study was that high plasma levels of
Hcy and the MTHFR C677T gene polymorphism are significantly
associated with VTE pathogenesis. By contrast, there were no
significant differences in the frequency of the thermolabile form
of MTHFR between diabetic patients and control subjects. Our data
suggest an association between the TT genotype and an increased
risk for VTE. In the present study, the VTE patients with the TT
genotype had higher plasma Hcy levels compared with those with the
CC or CT genotype. This result is consistent with those of previous
studies and revealed the effect of the MTHFR gene C677T mutation on
Hcy levels. The logistic regression analysis in this study
demonstrated that the TT genotype was a significant risk factor for
VTE. The difference in Hcy levels among the MTHFR genotype implies
that the Hcy levels account for the genotypic effect on venous
thrombogenesis.
Notably, the majority of the aforemention studies
are based are case-control studies. The finding of an association
between MTHFR homozygosity and any of these endpoints was not
reproduced in the current population-based case-control study.
There are several possible explanations for these differences in
demographics and risk factor prevalence between previous studies
and the present. Alternatively, differences in study design may
account for the apparent discrepancy. Clustering of additional risk
factors among cases in case-control studies may introduce bias
toward a higher risk estimate than in population-based studies.
In conclusion, our data suggest an association
between the TT genotype and an increased risk of VTE. The present
observations suggest that the C677T mutation of the MTHFR gene,
which is known to cause mild hyperhomocysteinemia, is one of the
candidate genetic risk factors predisposing to the development of
VTE. Whether genetic or environmental risk factors interact with
hereditary conditions requires further investigation.
References
|
1
|
Cattaneo M: Hyperhomocysteinemia and
venous thromboembolism. Semin Thromb Hemost. 32:716–723. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Božič-Mijovski M: Hyperhomocysteinemia and
thrombophilia. Clin Chem Lab Med. 48(Suppl 1): S89–S95. 2010.
|
|
3
|
Aguilar B, Rojas JC and Collados MT:
Metabolism of homocysteine and its relationship with cardiovascular
disease. J Thromb Thrombolysis. 18:75–87. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Franchini M, Veneri D, Salvagno GL,
Manzato F and Lippi G: Inherited thrombophilia. Crit Rev Clin Lab
Sci. 43:249–290. 2006. View Article : Google Scholar
|
|
5
|
Melo SS, Persuhn DC, Meirelles MS, Jordao
AA and Vannucchi H: G1793A polymorphisms in the
methylenetetrahydrofolate gene: effect of folic acid on
homocysteine levels. Mol Nutr Food Res. 50:769–774. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kumar J, Garg G, Kumar A, et al: Single
nucleotide polymorphisms in homocysteine metabolism pathway genes:
association of CHDH A119C and MTHFR C677T with
hyperhomocysteinemia. Circ Cardiovasc Genet. 2:599–606. 2009.
View Article : Google Scholar
|
|
7
|
Legnani C, Palareti G, Grauso F, et al:
Hyperhomocyst(e)inemia and a common methylenetetrahydrofolate
reductase mutation (Ala223Val MTHFR) in patients with inherited
thrombophilic coagulation defects. Arterioscler Thromb Vasc Biol.
17:2924–2929. 1997. View Article : Google Scholar
|
|
8
|
D’Angelo A, Mazzola G and Fermo I:
Gene-gene and gene-environment interactions in mild
hyperhomocysteinemia. Pathophysiol Haemost Thromb. 33:337–341.
2003.PubMed/NCBI
|
|
9
|
Frosst P, Blom HJ, Milos R, et al: A
candidate genetic risk factor for vascular disease: a common
mutation in methylenetetrahydrofolate reductase. Nat Genet.
10:111–113. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Frederiksen J, Juul K, Grande P, Jensen
GB, Schroeder TV, Tybjaerg-Hansen A and Nordestgaard BG:
Methylenete-trahydrofolate reductase polymorphism (C677T),
hyperhomocysteinemia, and risk of ischemic cardiovascular disease
and venous thromboembolism: prospective and case-control studies
from the Copenhagen City Heart Study. Blood. 104:3046–3051. 2004.
View Article : Google Scholar
|
|
11
|
Khare A, Ghosh K, Kulkarni B and Mohanty
D: Thrombophilia: hereditary and acquired in cardiovascular
disease. Haematologia (Budap). 32:293–311. 2002.PubMed/NCBI
|
|
12
|
Greer IA: Inherited thrombophilia and
venous thromboembolism. Best Pract Res Clin Obstet Gynaecol.
17:413–425. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Martinelli I: Risk factors in venous
thromboembolism. Thromb Haemost. 86:395–403. 2001.PubMed/NCBI
|
|
14
|
Bereczky Z, Kovács KB and Muszbek L:
Protein C and protein S deficiencies: similarities and differences
between two brothers playing in the same game. Clin Chem Lab Med.
48(Suppl 1): S53–S66. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Castoldi E and Rosing J: APC resistance:
biological basis and acquired influences. J Thromb Haemost.
8:445–453. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Slavik L, Krcova V, Hlusi A, et al:
Molecular pathophysiology of thrombotic states and their impact to
laboratory diagnostics. Biomed Pap Med Fac Univ Palacky Olomouc
Czech Repub. 153:19–25. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Simioni P, Scudeller A and Girolami A:
Factor V Leiden and thrombophilia. N Engl J Med. 332:13821995.
|
|
18
|
Nguyen A: Prothrombin G20210A polymorphism
and thrombophilia. Mayo Clin Proc. 75:595–604. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hoţoleanu C, Porojan-Iuga M, Rusu ML and
Andercou A: Hyperhomocysteinemia: clinical and therapeutical
involvement in venous thrombosis. Rom J Intern Med. 45:159–164.
2007.PubMed/NCBI
|
|
20
|
Van Oijen MG, Vlemmix F, Laheij RJ,
Paloheimo L, Jansen JB and Verheugt FW: Hyperhomocysteinaemia and
vitamin B12 deficiency: the long-term effects in cardiovascular
disease. Cardiology. 107:57–62. 2007.PubMed/NCBI
|
|
21
|
Aksoy M, Basar Y, Salmayenli N, et al:
Hyperhomocysteinemia in patients with arterial occlusive disease.
Surg Today. 36:327–331. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ramakrishnan S, Sulochana KN, Lakshmi S,
Selvi R and Angayarkanni N: Biochemistry of homocysteine in health
and diseases. Indian J Biochem Biophys. 43:275–283. 2006.PubMed/NCBI
|
|
23
|
Cortese C and Motti C: MTHFR gene
polymorphism, homocysteine and cardiovascular disease. Public
Health Nutr. 4:493–497. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gemmati D, Serino ML, Trivellato C,
Fiorini S and Scapoli GL: C677T substitution in the
methylenetetrahydrofolate reductase gene as a risk factor for
venous thrombosis and arterial disease in selected patients.
Haematologica. 84:824–828. 1999.PubMed/NCBI
|
|
25
|
Couturaud F, Oger E, Abalain JH, et al:
Methylenetetrahydrofolate reductase C677T genotype and venous
thromboembolic disease. Respiration. 67:657–661. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Salomon O, Steinberg DM, Zivelin A, et al:
Single and combined prothrombotic factors in patients with
idiopathic venous thromboembolism: prevalence and risk assessment.
Arterioscler Thromb Vasc Biol. 19:511–518. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Oger E, Lacut K, Le Gal G, et al; EDITH
COLLABORATIVE STUDY GROUP. Hyperhomocysteinemia and low B vitamin
levels are independently associated with venous thromboembolism:
results from the EDITH study: a hospital-based case-control study.
J Thromb Haemost. 4:793–799. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ray JG, Shmorgun D and Chan WS: Common
C677T polymorphism of the methylenetetrahydrofolate reductase gene
and the risk of venous thromboembolism: meta-analysis of 31
studies. Pathophysiol Haemost Thromb. 32:51–58. 2002. View Article : Google Scholar : PubMed/NCBI
|