Introduction
Globally, >200 million major surgical procedures
are undertaken annually (1), and
nitrous oxide is widely used in anesthesia, often administered at
an inspired concentration of ~60–70% (2–5).
Nitrous oxide has achieved marked longevity as an anesthetic,
having been used widely since 1844 (6). However, the low toxicity of modern
anesthetic agents and the accumulating evidence on the adverse
effects of nitrous oxide render the continued use of nitrous oxide
in anesthesia controversial (7–10). A
number of the adverse effects of nitrous oxide result from the
irreversible inactivation of vitamin B12, which inhibits
methionine synthase, folate metabolism and deoxyribonucleic acid
synthesis (7,8). This mechanism explains the
megaloblastic anemia and neurologic toxicity associated with
prolonged nitrous oxide administration (11,12),
and the possible risk of teratogenicity, immunodeficiency and
impaired wound healing (7,13,14).
In addition, the inhibition of methionine synthase is associated
with increased plasma homocysteine concentrations (15,16)
which may increase the risk of post-operative cardiovascular
complications (15). Furthermore,
nitrous oxide impairs cerebral blood flow-activity coupling
(10), and worsens the air space
conditions (such as pneumothorax and air embolism) and bowel
distension (8,9). Nitrous oxide is also a risk factor
for post-operative nausea and vomiting (17,18),
which are common, troublesome and costly complications of
anesthesia (19).
As a weak anesthetic, nitrous oxide is often
administered with other intravenous or volatile anesthetic agents
(such as propofol and sevoflurane, respectively) as 60–70% of the
inspired gas mixture containing 30–40% oxygen. Supplementation of
oxygen during surgery potentially reduces the risk of wound
infection (20,21), nausea and vomiting (22), which contribute to the duration of
the hospital stay and cost of care.
Despite the adverse effects that may result directly
from nitrous oxide, it is almost routinely used in patients
undergoing surgery (23). Notably,
nitrous oxide has been reported to suppress the activation of
neutrophils, an important type of inflammatory cell, in
vitro(24,25). However, the effects of nitrous
oxide on the inflammatory reaction in the respiratory tract remain
to be elucidated. Thus, in the present study, the effects of
nitrous oxide on the in vivo production of inflammatory
cytokines and chemokines by airway epithelium were evaluated by
combining nitrous oxide with other anesthetic agents (intravenous
propofol and volatile sevoflurane).
Materials and methods
Subjects
In total, 52 females [age range, 22–72; mean age ±
standard deviation (SD), 55.1±11.5 years] classified as American
Society of Anesthesiologists Physical Status category I–II and
undergoing simple or segmental mastectomy were recruited in this
study. The study protocol was approved by the Local Ethics
Committee of Juntendo University Nerima Hospital (Tokyo, Japan) and
conducted from March 2008 to June 2009 in accordance with the
principles of the amended Declaration of Helsinki and the Ethical
Guidelines for Epidemiological Research (http://aje.oxfordjournals.org/content/170/11/1451.full).
Subjects provided written informed consent prior to participating
in the study. None of subjects received premedication.
The exclusion criteria included pregnancy,
neurologic or psychiatric disease, cardiac disease classified as
New York Heart Association classes II–IV (http://www.abouthf.org/questions_stages.htm),
pre-operative severe impairment of respiratory function (such as a
vital capacity or a forced expiratory volume in one second of
<50% of that predicted), and pre-existing coagulopathy or
thrombocytopenia. Subjects that exhibited systemic or local active
infections (either clinically defined or evidenced by elevated
C-reactive protein levels, leukocytosis or body temperature
>38°C) were also excluded.
Subjects were randomly assigned to a sevoflurane
group (n=26) without (n=13) or with nitrous oxide (n=13), and a
propofol group (n=26) without (n=13) or with nitrous oxide (n=13),
using a list of random numbers generated by computer software
(Microsoft Excel; Microsoft Corporation, Redmond, WA, USA).
Study protocols
Protocol 1: Induction of anesthesia was initiated
with intravenous injection of propofol (1–2 mg/kg; AstraZeneca,
Osaka, Japan), vecuronium bromide (0.1 mg/kg; MDS, Tokyo, Japan)
and remifentanil (0.15–0.3 μg/kg/min; Janssen Pharmaceutical K.K.,
Tokyo, Japan). Subsequently, each subject was intubated with an
endotracheal tube and their end-tidal CO2 was verified.
Anesthesia was maintained with the inhalation of sevoflurane
(0.8–1.0 minimum alveolar concentration; Maruishi Pharmaceutical
Co., Ltd., Osaka, Japan) and intravenous infusion of remifentanil
(0.15–0.3 μg/kg/min).
Protocol 2: Induction of anesthesia was initiated
with intravenous infusion of propofol (using a target-controlled
infusion technique with a target concentration of 3–4 μg/ml),
vecuronium (0.1 mg/kg) and remifentanil (0.15–0.3 μg/kg/min).
Subsequently, each subject was intubated with an endotracheal tube
and their end-tidal CO2 was verified. Anesthesia was
maintained with intravenous infusion of propofol (target
concentration 2–4 μg/ml) and remifentanil (0.15–0.3 μg/kg/min).
For nitrous oxide-based anesthesia, subjects were
administered with a gas mixture of 60% nitrous oxide and 40% oxygen
(O2 2 l/min + nitrous oxide 3 l/min). For nitrous
oxide-free anesthesia, subjects were administered with a gas
mixture of 40% oxygen and 60% nitrogen (O2 1 l/min + air
containing 80% nitrogen and 20% oxygen 3 l/min).
An endotracheal tube (Rüsch® endotracheal
tube; Teleflex Medical Sdn. Bhd., Kamunting, Malaysia) was inserted
in all of the subjects. The position of the endotracheal tube was
confirmed by a fiberoptic bronchoscopy (Portable Intubation
Fiberscope FI-10RBS; Pentax, Tokyo, Japan). The subjects were
ventilated by pressure-controlled ventilation with 4-cm
H2O positive end-expiratory pressure, and peak
inspiratory pressure was maintained at >20 cm H2O
with a tidal volume of 7–10 ml/kg, and the fraction of inspired
oxygen was maintained at 0.4. The oxygen saturation was adjusted to
>97% and the respiratory rate was adjusted to maintain
normocapnia (normal arterial carbon dioxide pressure).
For post-operative pain management, all the subjects
were administered with 2 μg/kg of fentanyl (Daiichi Sankyo Company,
Ltd., Tokyo, Japan) prior to the discontinuation of anesthetic
agents.
Electrocardiogram, oxygen saturation, non-invasive
blood pressure, end-tidal CO2 pressure, esophageal body
temperature and urine output were monitored during anesthesia and
recorded every 5 min. Crystalloid solution was used for infusion,
in accordance with the clinical needs of the patients. None of the
subjects required blood transfusion.
Bronchoscopic microsampling
Epithelial lining fluid (ELF) was obtained using the
bronchoscopic microsampling method prior to mastectomy (as the
pre-operative level) and following mastectomy (as the
post-operative level). A bronchofiberscope was inserted into the
trachea through an endotracheal tube and placed at the bifurcation.
A bronchoscopic microsampling probe (BC-402C; Olympus, Tokyo,
Japan) was inserted into the right main bronchus through the
channel of the bronchofiberscope; the probe consisted of a 2.6-mm
outer-diameter polyethylene sheath and an inner 1.9-mm-diameter
cotton probe (length, 20 mm) attached to a stainless steel
guidewire. The inner probe was advanced gently 2–3 cm from the
bifurcation into the right main bronchus until it made contact with
the mucosal surface. ELF was obtained from the mucosal surface
under direct observation. Subsequently, the inner probe was
withdrawn, and the probe was sectioned at 30 mm from its tip and
stored at −80°C until analysis.
Measurement of cytokines
The probe was weighed and mixed with 500 μl saline
by vortexing for 1 min, and then the solution was recovered.
Subsequently, the probe was dried and reweighed to estimate the
recovered ELF, which was calculated by subtracting the weight of
the dried probes from that of the wet probes (the difference
between the weight of the wet probe and the dried probe was ~10
mg), and the dilution factor was also calculated (26).
In the sevoflurane groups without or with nitrous
oxide, inflammatory cytokine and chemokine levels in the ELF were
measured using the cytometric bead array Human Inflammation kit and
Human Chemokine kit (Becton-Dickinson, Franklin Lakes, NJ, USA).
The Human Inflammation kit included six
fluorescently-distinguishable capture microbeads coated with
antibodies against the following six analytes: Tumor necrosis
factor (TNF)-α, and interleukin (IL)-1β, IL-6, IL-8, IL-10 and
IL-12p70. The Human Chemokine kit included five
fluorescently-distinguishable capture microbeads coated with
antibodies against the following five analytes: IL-8, regulated
upon activation normal T cell expressed and presumably secreted
(RANTES), monokine induced by interferon γ (MIG), monocyte
chemotactic protein-1 (MCP-1) and interferon γ-inducible protein 10
(IP-10). These methods detect cytokines and chemokines bound onto
the microbeads by using an enzyme-linked immunosorbent assay
(ELISA). The minimum quantifiable levels of cytokines and
chemokines detected with the Human Inflammation and Chemokine kits
were 20 and 10 pg/ml, respectively.
In the propofol groups with or without nitrous
oxide, IL-6 and IL-8 levels in ELF were quantified by a sandwich
ELISA using a Ready-Set-Go kit (eBioscience, San Diego, CA, USA)
and a DuoSet ELISA Development kit (R&D Systems, Minneapolis,
MN, USA), respectively. The detection limits of IL-6 and IL-8
detected with the ELISAs were 2 and 31.2 pg/ml, respectively.
Statistical analysis
Data are expressed as the mean ± SD and were
statistically evaluated using the Wilcoxon signed-rank test and the
Mann-Whitney U test. Differences were considered to be indicated as
statistically significant when P<0.05. Analyses were performed
with the statistical software program JMP® 7 (SAS
Institute Inc., Cary, NC, USA).
Results
Subject characteristics
Table I shows the
characteristics and surgical operation data of the 52 subjects
divided into the four experimental groups. Subjects were evenly
distributed among the four groups (sevoflurane groups with or
without nitrous oxide, and propofol groups with or without nitrous
oxide) based on their age, weight, height, body mass index,
duration of surgery and anesthesia, and amount of blood lost. All
the subjects were extubated following the surgery in the operating
room and the post-operative course was uneventful.
 | Table IPatient characteristics and surgical
data. |
Table I
Patient characteristics and surgical
data.
| Sevoflurane group
(n=26) | Propofol group
(n=26) |
|---|
|
|
|
|---|
| Patient
characteristics | Air (n=13) | Nitrous oxide
(n=13) | Air (n=13) | Nitrous oxide
(n=13) |
|---|
| Age (years) | 56.8±3.9 | 51.9±11.7 | 55.9±11.0 | 55.5±9.8 |
| Actual weight
(kg) | 52.6±7.3 | 57.0±7.0 | 55.7±9.5 | 55.1±9.2 |
| Height (cm) | 155.3±4.4 | 155.4±4.5 | 154.3±6.3 | 158.7±3.3 |
| Body mass index
(kg/m2) | 21.8±2.6 | 21.5±4.8 | 23.3±3.0 | 21.9±3.7 |
| Duration of surgery
(min) | 135.2±44.4 | 144.8±50.3 | 142.2±40.0 | 147.5±34.5 |
| Duration of
anesthesia (min) | 183.8±43.3 | 195.2±53.4 | 194.1±44.8 | 193.9±36.8 |
| Loss of blood
(g) | 99.5±109.9 | 83.5±66.7 | 50.8±28.3 | 65.9±30.7 |
Cytokine and chemokine levels in the ELF
of the sevoflurane groups
As shown in Fig. 1,
the levels of IL-1β, IL-8 and MCP-1 were significantly increased by
the inhalation of nitrous oxide with sevoflurane (post-operative)
compared with the baseline (pre-operative) (P<0.05). By
contrast, the levels of IL-1β, IL-8 and MCP-1 were not
significantly changed by the inhalation of air with sevoflurane
(post-operative) compared with the baseline (pre-operative).
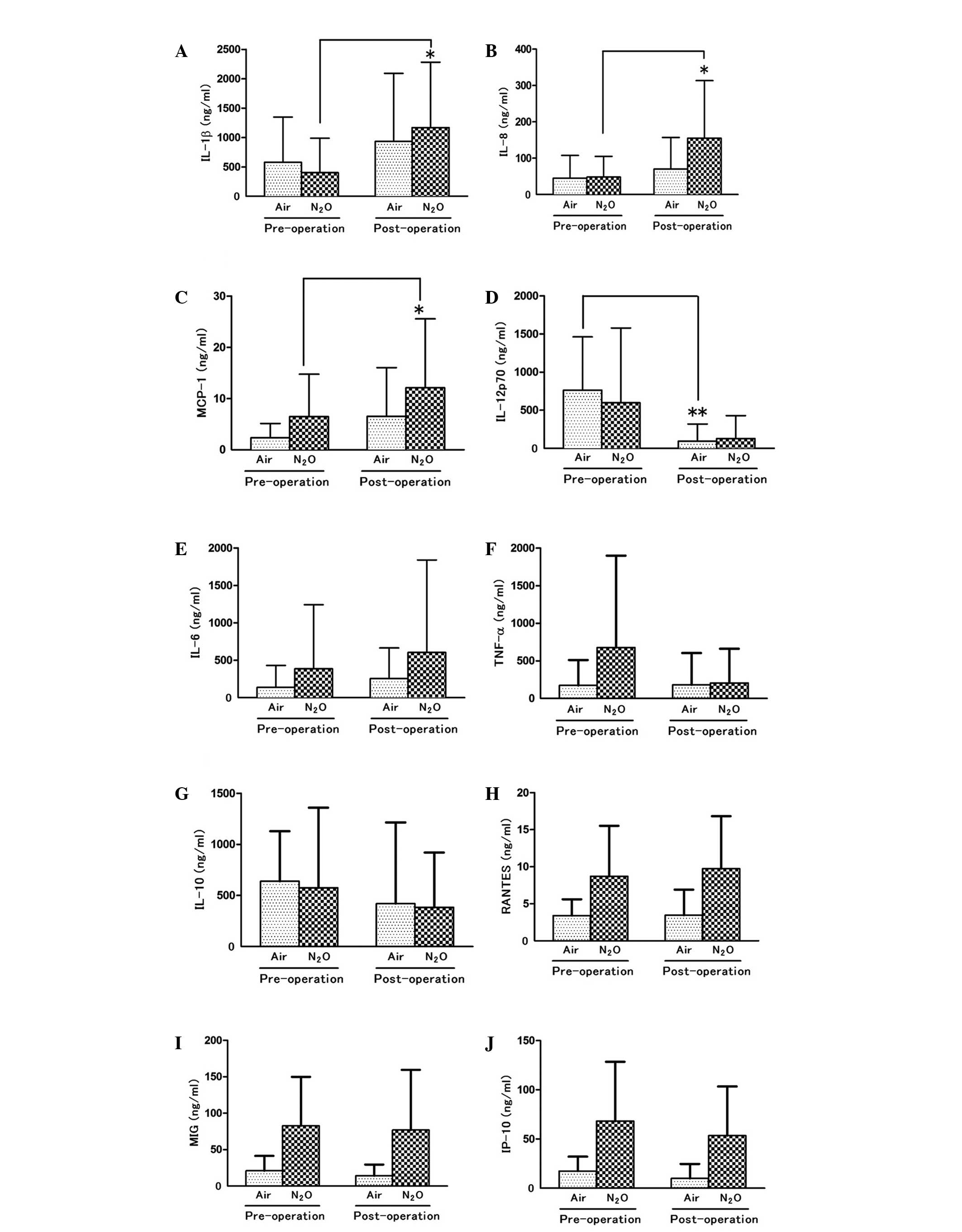 | Figure 1The levels of cytokines and chemokines
in the ELF prior to and following the inhalation of sevoflurane
with or without nitrous oxide. The levels of (A) IL-1β, (B) IL-8,
(C) MCP-1, (D) IL-12p70, (E) IL-6, (F) TNF-α, (G) IL-10, (H)
RANTES, (I) MIG and (J) IP-10 were measured with a CBA system using
ELF recovered from patients undergoing mastectomy prior to
(pre-operative) and following (post-operative) the inhalation of
sevoflurane with (N2O) or without nitrous oxide (air).
Data are expressed as the mean ± SD, and compared between the pre-
and post-operative levels. *P<0.05,
**P<0.01. IL, interleukin; MCP-1, monocyte
chemotactic protein-1; TNF, tumor necrosis factor; RANTES,
regulated upon activation normal T cell expressed and presumably
secreted; MIG, monokine induced by interferon γ; IP-10, interferon
γ-inducible protein 10; ELF, epithelial lining fluid; CBA,
cytometric bead array. |
Of note, the levels of IL-12p70 were significantly
reduced by the inhalation of sevoflurane with air (post-operative)
compared with the baseline (pre-operative) (P<0.01). However,
the levels of IL-12p70 were not significantly reduced by the
inhalation of nitrous oxide with sevoflurane (post-operative)
compared with the baseline (pre-operative).
The levels of IL-6, TNF-α, IL-10, RANTES, MIG and
IP-10 were not significantly changed by the inhalation of nitrous
oxide or air with sevoflurane (post-operative) compared with the
baseline (pre-operative).
IL-8 and IL-6 levels in the ELF of the
propofol groups
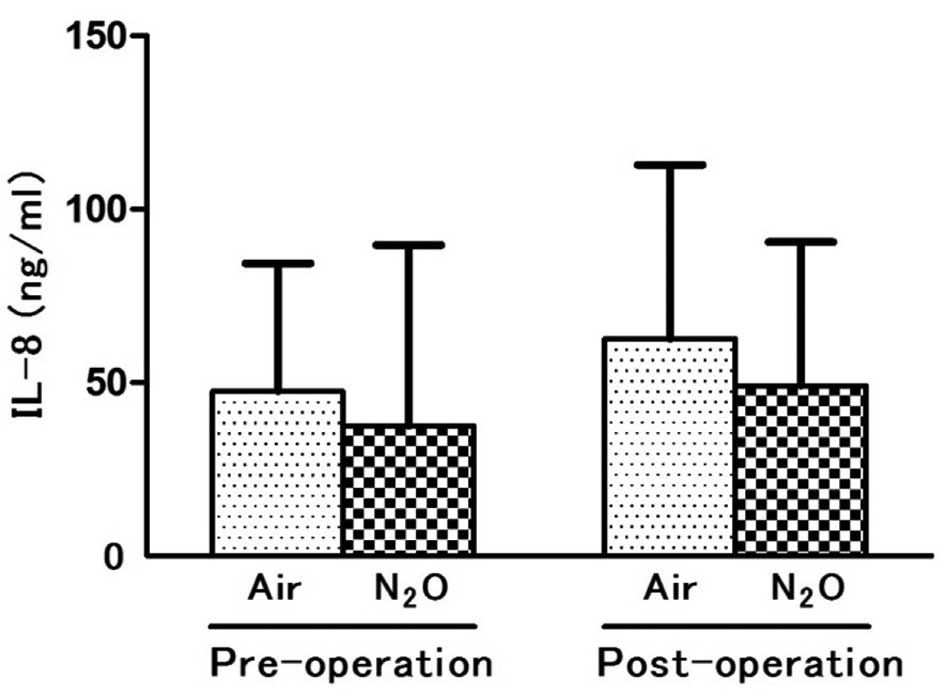
As shown in Fig. 2,
the levels of IL-8 were not significantly changed by the inhalation
of nitrous oxide with propofol anesthesia (post-operative) compared
with the baseline levels (pre-operative). Similarly, the levels of
IL-8 were not affected by the inhalation of air with propofol
anesthesia (post-operative) compared with the baseline levels
(pre-operative), as observed with sevoflurane anesthesia. In the
propofol group with or without nitrous oxide, IL-6 was not detected
in the ELF studied.
Discussion
A number of studies have shown that airway
epithelial cells express and secrete various inflammatory and
immune molecules, including cytokines (TNF-α, IL-1β and IL-6) and
chemokines (IL-8 and MCP-1) (27–29).
TNF-α, IL-1β and IL-6 function as proinflammatory molecules,
whereas IL-8 and MCP-1 act as chemoattractants that are responsible
for the recruitment of effector cells such as neutrophils and
monocytes (30,31). Moreover, IL-12 is a strong inducer
of interferon-γ and is important for the development of T-helper
type I cells (32). Through the
expression and production of these molecules, the airway epithelium
is important in the initiation and exacerbation of inflammatory
responses within the airways.
Volatile anesthetics, such as sevoflurane and
isoflurane, have been shown to attenuate the cardiac injury caused
upon ischemia-reperfusion (33)
and to exert anti-inflammatory action in a model of
endotoxin-induced lung injury in vivo(34). Furthermore, in vitro studies
have demonstrated that sevoflurane exhibited direct
anti-inflammatory and antinecrotic effects on cultured human kidney
cells following ischemia-reperfusion injury (35). In addition, sevoflurane has not
only been shown to suppress the expression of inflammatory
mediators such as MCP-1, macrophage inflammatory protein (MIP)-1β,
MIP-2 and cytokine-induced neutrophil chemoattractant-1 and the
adhesion molecule ICAM-1, but it has also been shown to reduce
neutrophil adhesion to lipopolysaccharide-injured alveolar
epithelial cells in vitro(36). In this context, one-lung
ventilation (OLV) has been demonstrated to induce an increase in
the inflammatory molecules TNF-α, IL-1β, IL-6, IL-8 and MCP-1 in
propofol- and sevoflurane-anesthesized patients; however, the
levels of inflammatory mediators following OLV, with the exception
of IL-1β, were significantly lower in the sevoflurane group
compared with those in the propofol group (29). Thus, sevoflurane likely exerts
anti-inflammatory activities on various types of cells. Notably, it
has been suggested that sevoflurane exerts an anti-inflammatory
action via the mechanisms involving the reduction of mRNA and
protein levels of the proinflammatory transcription factors NF-κB
and AP-1 (35,37).
Nitrous oxide is widely used as an anesthetic in
humans. Its short-acting analgesic properties reduce the
requirement for the more potent anesthetics combined. Thus, nitrous
oxide is generally considered to be a relatively safe anesthetic.
Nevertheless, a number of adverse effects are known, including
megaloblastic anemia, homocysteinemia and possible risks for
atherosclerosis, thrombosis, cognitive dysfunction, neurotoxicity,
teratogenicity, increased intracranial pressure, hypoxia,
post-operative nausea and vomiting, and immunosuppression.
Although controversial, in vitro and in
vivo studies have demonstrated that nitrous oxide reduces
neutrophil motility and chemotaxis as well as the oxidative
response (25,38–40,41–43).
Furthermore, nitrous oxide depresses the expression of endogenous
sugar receptors on polymorphonuclear leukocytes and impairs
intracellular signaling in leukocytes, resulting in the
interference of the leukocyte adhesion-activation cascade (44,45).
These observations clearly indicate that nitrous oxide acts as an
anti-inflammatory molecule.
Notably, in the present study, it was identified
that the levels of IL-1β, IL-8 and MCP-1 in ELF were significantly
increased by the inhalation of sevoflurane with nitrous oxide,
although the levels of IL-1β, IL-8 and MCP-1 were not significantly
changed by the inhalation of sevoflurane with air. Furthermore, the
levels of IL-12p70 were not significantly reduced by the inhalation
of nitrous oxide with sevoflurane, although the levels of IL-12p70
were significantly reduced by the inhalation of sevoflurane with
air. These observations suggest that the aforementioned
anti-inflammatory actions of sevoflurane and nitrous oxide are
abrogated by the combination of these compounds, and the inhalation
of nitrous oxide likely induces the inflammatory response
(increased production of IL-1β, IL-8 and MCP-1) or suppresses the
anti-inflammatory response (reduced production of IL-12p70) under
the sevoflurane anesthesia. Of note, this possibility is supported
by the finding that the IL-8 levels were not increased by the
inhalation of nitrous oxide with propofol. Moreover, our hypothesis
is reinforced by the following findings from a previous study: The
number of leukocytes rolling along and firmly adherent to the
endothelial wall of cerebral venules were significantly increased
in animals anesthetized with nitrous oxide in combination with
isoflurane or halothane (a halogenated fluorine-containing
anesthetic similar to sevoflurane), compared with isoflurane or
halothane alone; and the combination of isoflurane or halothane and
nitrous oxide significantly increased the number of neutrophils
invading the brain parenchyma in animals compared with that of
isoflurane or halothane alone (46).
In the present study, it was demonstrated that
several cytokine and chemokine levels were increased in ELF by the
inhalation of nitrous oxide with sevoflurane (following the surgery
of mastectomy). Notably, it has already been reported that the
levels of cytokines and chemokines (TNF-α, IL-8, IL-1β, IL-10 and
IL-12p70) are increased in the ELF, however, these
cytokine/chemokine levels remained undetectable in the plasma even
following OLV and thoracic surgery (lobectomy and partial lung
resection) (47). Thus, we
hypothesize that the inflammatory response observed in the present
study is restricted to the local airway surface. In conclusion,
findings of the present study suggest that nitrous oxide and
sevoflurane should be carefully administered for anesthesia, as the
combination of these compounds induces an inflammatory response in
the local milieu of the airway (as evidenced by enhanced
cytokine/chemokine expression).
References
|
1
|
Weiser TG, Regenbogen SE, Thompson KD, et
al: An estimation of the global volume of surgery: a modelling
strategy based on available data. Lancet. 372:139–144.
2008.PubMed/NCBI
|
|
2
|
Fisher DM and Zwass MS: MAC of desflurane
in 60% nitrous oxide in infants and children. Anesthesiology.
76:354–356. 1992.
|
|
3
|
Gupta K, Vohra V and Sood J: The role of
magnesium as an adjuvant during general anaesthesia. Anaesthesia.
61:1058–1063. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Myles PS, Leslie K, Chan MT, et al; ENIGMA
Trial Group. Avoidance of nitrous oxide for patients undergoing
major surgery: a randomized controlled trial. Anesthesiology.
107:221–231. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Myles PS, Leslie K, Peyton P, et al; ANZCA
Trials Group. Nitrous oxide and perioperative cardiac morbidity
(ENIGMA-II) Trial: rationale and design. Am Heart J. 157:488–494.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Urman RD and Desai SP: History of
anesthesia for ambulatory surgery. Curr Opin Anaesthesiol.
25:641–647. 2012.PubMed/NCBI
|
|
7
|
Nunn JF: Clinical aspects of the
interaction between nitrous oxide and vitamin B12. Br J Anaesth.
59:3–13. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Myles PS, Leslie K, Silbert B, Paech M and
Peyton P: A review of the risks and benefits of nitrous oxide in
current anaesthetic practice. Anaesth Intensive Care. 32:165–172.
2004.PubMed/NCBI
|
|
9
|
Akca O, Lenhardt R, Fleischmann E, et al:
Nitrous oxide increases the incidence of bowel distension in
patients undergoing elective colon resection. Acta Anaesthesiol
Scand. 48:894–898. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kaisti KK, Langsjo JW, Aalto S, et al:
Effects of sevoflurane, propofol, and adjunct nitrous oxide on
regional cerebral blood flow, oxygen consumption, and blood volume
in humans. Anesthesiology. 99:603–613. 2003.PubMed/NCBI
|
|
11
|
Marie RM, Le Biez E, Busson P, et al:
Nitrous oxide anesthesia-associated myelopathy. Arch Neurol.
57:380–382. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schilling RF: Is nitrous oxide a dangerous
anesthetic for vitamin B12-deficient subjects. JAMA. 255:1605–1606.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Parbrook GD: Leucopenic effects of
prolonged nitrous oxide treatment. Br J Anaesth. 39:119–127. 1967.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mazze RI, Wilson AI, Rice SA and Baden JM:
Reproduction and fetal development in rats exposed to nitrous
oxide. Teratology. 30:259–265. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Badner NH, Beattie WS, Freeman D and
Spence JD: Nitrous oxide-induced increased homocysteine
concentrations are associated with increased postoperative
myocardial ischemia in patients undergoing carotid endarterectomy.
Anesth Analg. 91:1073–1079. 2000.
|
|
16
|
Badner NH, Drader K, Freeman D and Spence
JD: The use of intraoperative nitrous oxide leads to postoperative
increases in plasma homocysteine. Anesth Analg. 87:711–713.
1998.PubMed/NCBI
|
|
17
|
Tramer M, Moore A and McQuay H:
Meta-analytic comparison of prophylactic antiemetic efficacy for
postoperative nausea and vomiting: Propofol anaesthesia versus
omitting nitrous oxide versus total i.v. anaesthesia with propofol.
Br J Anaesth. 78:256–259. 1997. View Article : Google Scholar
|
|
18
|
Apfel CC, Korttila K, Abdalla M, et al: A
factorial trial of six interventions for the prevention of
postoperative nausea and vomiting. N Engl J Med. 350:2441–2451.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Macario A, Weinger M, Carney S and Kim A:
Which clinical anesthesia outcomes are important to avoid? The
perspective of patients. Anesth Analg. 89:652–658. 1999.PubMed/NCBI
|
|
20
|
Greif R, Akca O, Horn EP, Kurz A and
Sessler DI: Supplemental perioperative oxygen to reduce the
incidence of surgical wound infection. N Engl J Med. 342:161–167.
2000. View Article : Google Scholar
|
|
21
|
Belda FJ, Aguilera L, Garcia de la
Asunción J, et al: Supplemental perioperative oxygen and the risk
of surgical wound infection. JAMA. 294:2035–2042. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Grief R, Laciny S, Rapf B, Hickle RS and
Sessler DI: Supplemental oxygen reduces the incidence of
postoperative nausea and vomiting. Anesthesiology. 91:1246–1252.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Henderson KA, Raj N and Hall JE: The use
of nitrous oxide in anaesthetic practice: a questionnaire survey.
Anaesthesia. 57:1155–1158. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schneemilch CE, Hachenberg T, Ansorge S,
Ittenson A and Bank U: Effects of different anaesthetic agents on
immune cell function in vitro. Eur J Anaesthesiol. 22:616–623.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Moudgil GC, Gordon J and Forrest JB:
Comparative effects of volatile anaesthetic agents and nitrous
oxide on human leucocyte chemotaxis in vitro. Can Anaesth Soc J.
31:631–637. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ishizaka A, Watanabe M, Yamashita T, et
al: New bronchoscopic microsample probe to measure the biochemical
constituents in epithelial lining fluid of patients with acute
respiratory distress syndrome. Crit Care Med. 29:896–898. 2001.
View Article : Google Scholar
|
|
27
|
Simon RH and Paine R III: Participation of
pulmonary alveolar epithelial cells in lung inflammation. J Lab
Clin Med. 126:108–118. 1995.PubMed/NCBI
|
|
28
|
Takizawa H: Airway epithelial cells as
regulators of airway inflammation. Int J Mol Med. 1:367–378.
1998.PubMed/NCBI
|
|
29
|
De Conno E, Steurer MP, Wittlinger M, et
al: Anesthetic-induced improvement of the inflammatory response to
one-lung ventilation. Anesthesiology. 110:1316–1326.
2009.PubMed/NCBI
|
|
30
|
Vozzelli MA, Mason SN, Whorton MH and
Auten RL Jr: Antimacrophage chemokine treatment prevents neutrophil
and macrophage influx in hyperoxia-exposed newborn rat lung. Am J
Physiol Lung Cell Mol Physiol. 286:L488–L493. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Beck-Schimmer B, Schwendener R, Pasch T,
Reyes L, Booy C and Schimmer RC: Alveolar macrophages regulate
neutrophil recruitment in endotoxin-induced lung injury. Respir
Res. 6:61–66. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Brunda MJ: Interleukin-12. J Leukoc Biol.
55:280–288. 1994.
|
|
33
|
Tanaka K, Ludwig LM, Kersten JR, Pagel PS
and Warltier DC: Mechanisms of cardioprotection by volatile
anesthetics. Anesthesiology. 100:707–721. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Reutershan J, Chang D, Hayes JK and Ley K:
Protective effects of isoflurane pretreatment in endotoxin-induced
lung injury. Anesthesiology. 104:511–517. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee HT, Kim M, Jan M and Emala CW:
Anti-inflammatory and antinecrotic effects of the volatile
anesthetic sevoflurane in kidney proximal tubule cells. Am J
Physiol Renal Physiol. 291:67–78. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Suter D, Spahn DR, Blumenthal S, Reyes L,
Booy C, Z’Graggen BR and Beck-Schimmer B: The immunomodulatory
effect of sevoflurane in endotoxin-injured alveolar epithelial
cells. Anesth Analg. 104:638–645. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Loop T, Scheiermann P, Doviakue D, et al:
Sevoflurane inhibits phorbol-myristate-acetate-induced activator
protein-1 activation in human T lymphocytes in vitro: potential
role of the p38-stress kinase pathway. Anesthesiology. 101:710–721.
2004. View Article : Google Scholar
|
|
38
|
Frohlich D, Rothe G, Wittmann S, Schmitz
G, Schmid P, Taeger K and Hobbhahn J: Nitrous oxide impairs the
neutrophil oxidative response. Anesthesiology. 88:1281–1290. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hill GE, English JB, Stanley TH, Kawamura
R, Loeser EA and Hill HR: Nitrous oxide and neutrophil chemotaxis
in man. Br J Anaesth. 50:555–558. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kripke BJ, Kupferman A and Luu KC:
Suppression of chemotaxis to corneal inflammation by nitrous oxide.
Zhonghua Min Guo Wei Sheng Wu Ji Mian Yi Xue Za Zhi. 20:302–310.
1987.PubMed/NCBI
|
|
41
|
Nunn JF and O’Morain C: Nitrous oxide
decreases motility of human neutrophils in vitro. Anesthesiology.
56:45–48. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Welch WD: Effect of enflurane, isoflurane,
and nitrous oxide on the microbicidal activity of human
polymorphonuclear leukocytes. Anesthesiology. 61:188–192. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Welch WD and Zaccari J: Effect of
halothane and N2O on the oxidative activity of human
neutrophils. Anesthesiology. 57:172–176. 1982.
|
|
44
|
Bardosi L, Bardosi A and Gabius HJ:
Changes of expression of endogenous sugar receptors by
polymorphonuclear leukocytes after prolonged anaesthesia and
surgery. Can J Anaesth. 39:143–150. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Frohlich D, Rothe G, Schmitz G and Taeger
K: Nitrous oxide impairs the signaling of neutrophils downstream of
receptors. Toxicol Lett. 100–101:121–127. 1998.PubMed/NCBI
|
|
46
|
Lehmberg J, Waldner M, Baethmann A and Uhl
E: Inflammatory response to nitrous oxide in the central nervous
system. Brain Res. 30:1246:88–95. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Sugasawa Y, Yamaguchi K, Kumakura S,
Murakami T, Suzuki K, Nagaoka I and Inada E: Effects of sevoflurane
and propofol on pulmonary inflammatory responses during lung
resection. J Anesth. 26:62–69. 2012. View Article : Google Scholar : PubMed/NCBI
|