Introduction
Psoriasis is a chronic skin disease affecting 2–3%
of the population. Hyperproliferation of disordered epidermal
keratinocytes leads to the formation of chronic erythematous
plaques with inflammation on the thighs, joints, scalp and body
trunk. 5–20% of patients with psoriasis have arthritis, and these
patients often present with nail disorders typically featured by
pits and yellowish changes in color (1). These complex symptoms, including pain
and itchiness, considerably impair the quality of life, and the
skin lesions affect physical health and mental wellbeing (2).
Although the etiology is unknown, T cells are
thought to have a critical role in the pathogenesis of psoriasis.
At the initial step, the pathogenic T cells recruited into the
endothe-lium under the epidermis cause the dysregulation of
cytokines, including TNFα, IL-1, IL-6 and IL-17 (3–6).
They induce the expression of various adhesion molecules, including
intracellular adhesion molecule 1 and leukocyte function-associated
antigen 1, on endothelial cells and keratinocytes (1). This affects the rolling of leukocytes
and induces the extravasation of the cells into the mesenchymal
epithelium. Finally, the impaired angiogenesis is accompanied by
increased levels of vascular endothelial growth factor (7) and a five-fold increased turnover of
the basal layer results in the thickness of the skin lesions
through inflammation. A number of biological drugs have
successfully targeted these T-cell cytokine-associated or leukocyte
adhesion-mediated molecular interactions (8–10).
Apart from the protein-based molecular mechanisms,
reactive oxygen species (ROS) are thought to have an important role
in the pathogenesis of psoriasis (11,12).
Immune cells, including leukocytes that infiltrate into psoriatic
lesions, overproduce ROS and activate the redox-sensitive nuclear
factor-κB-dependent positive feedback loop (13), which, in turn, increases the
transcription of the abovementioned pro-inflammatory cytokines
(14). Based on the involvement of
ROS in the pathogenesis of psoriasis, anti-oxidant therapies have
been tested, particularly in Germany, using fumaric acid esters
that stabilize Nrf2, a transcriptional factor known to be an
activator of intrinsic protective mechanisms against oxidative
stress (15,16). However, direct evidence showing
that ROS initiate psoriasis is currently lacking; furthermore, a
therapeutic approach directly targeted to ROS has not been
developed, yet. Among ROS, peroxynitrite, which is generated from
the reaction of nitric oxide with superoxide, which are released
from the endothelium, is likely to be involved in the pathogenesis
of psoriasis, particularly in the development of plaque, with
inflammation in the microcirculation of pathological angiogenesis.
Another toxic type of ROS, the hydroxyl radical, may have a major
role in the pathogenesis of psoriasis, as the absence of the
specific scavenger of this species spontaneously causes oxidative
states in chronic inflammation (14). Inert H2 gas has the
capability to scavenge the abovementioned ROS (17,18).
H2 has been safely used for the prevention of
decompression sickness in deep divers (19). The therapeutic efficacy of
H2 in the treatment of rheumatoid arthritis (RA), an
autoimmune disease associated with psoriasis via cytokine-mediated
inflammation, was recently investigated (14); The prevalence of psoriatic
arthritis was reported to be 19.5/100,0000 individuals in Japan in
the 1990s (20). The present study
examined the effect on H2 treatment in three cases of
psoriatic skin lesions as well as psoriatic arthritis. In addition
to the administration method of drinking water containing dissolved
H2, which has been proven to reduce oxidative stress in
the body (21) and infusion of
saline containing H2, which is currently being
investigated for the efficacy in the treatment of RA (14), the inhalation of H2 gas,
which is a safe and painless method of H2
administration, was also investigated, even though its efficacy in
the treatment of arthritis has not been proven. The present study
showed a reduction in inflammation associated with psoriasis by
administration of H2.
Materials and methods
The three patients with psoriatic arthritis gave
their written informed consent to participate in the present study,
where a therapy involving molecular hydrogen as an
anti-inflammatory agent was used. The treatment protocol was
approved by the Haradoi Hospital Ethics Committee (Fukuoka, Japan).
Three methods were used to administer H2: Drop infusion
of saline containing 1-ppm H2 (H2-saline),
inhalation of 3% H2 gas, and drinking of water
containing a concentration of 5–7 ppm H2 (Hydrogen Water
7.0; Ecomo International, Co., Ltd., Iizuka-shi, Fukuoka, Japan).
All methods were previously verified regarding their safety
(21–25). H2-dissolved saline was
administered as described previously (21). Briefly, 250 ml saline in a soft bag
was placed in a circulating water bath containing 1.6 ppm
H2 generated by an electrolysis instrument (MiZ Company,
Fujisawa, Japan), and the concentration of H2 in the
saline was adjusted to 1 ppm prior to infusion. The concentration
was confirmed by using the methylene blue-platinum colloid
regent-based titration method (26). Although the present case study is
not a clinical study, H2-saline was used in a randomized
double-blinded placebo-controlled manner in order to evaluate its
effect on the patients objectively. Placebo saline, which was used
in Case 3, was prepared in the same water bath without
H2. 500 ml H2-saline or placebo-saline was
administered over 40 min by drip intravenous infusion (DIV) prior
to breakfast intake every day over five days.
The high-H2 water was prepared according
to the methods described previously (24). The high-H2 water (500 ml), which
contains 2.5–3.5 mg H2 was consumed every day during the
administration period.
H2 gas for inhalation was generated using
a hydrogen gas supply apparatus (patent no. 5091364; Patent Gazette
of Japan 2013; MiZ Company, Fujisawa, Japan) constituted by an
electrolysis chamber, a membrane and electrode plates.
H2 gas generated from the cathode surface was mixed with
air blown directly onto the cathode, so that the H2 gas
concentration was maintained at ~3%. The H2 gas was
inhaled via a cannula attached to the nose. The concentration of
H2 gas on the way out of the cannula was verified to be
~3% using a hydrogen gas meter (XP-3140; New Cosmos Electric Co.,
Ltd., Osaka, Japan). The H2 gas was inhaled for 1 h
prior to breakfast every day for 5 days
The improvements in the psoriatic skin lesions were
estimated using the psoriasis area and severity index (PASI) score
(27). The pruritus of the skin
lesions was measured by the visual analog scale (VAS) for itching
(28). Arthritis was estimated by
changes in the disease activity score in 28 joints (DAS28) using
C-reactive protein levels (29).
Blood samples were collected at each time point, and levels of
serum cytokines TNFα, IL-17 and IL-6 were measured using the
MILLIPLEX Human Cytokine kit (Merck Millipore, Billerica, MA,
USA).
Results
Case 1
A 55-year-old woman with multiple erythematous
plaques accompanying a scaly eruption mainly on the lower limbs
simultaneously experienced psoriatic arthritis on her wrists,
hands, knees and shoulders; her condition had significantly
affected her activities of daily life for seven years. She had been
pathologically diagnosed as having psoriasis vulgaris and had been
treated with corticosteroid and calcipotriol ointments. As her
arthritis was consistent with the 2010 American College of
Rheumatology criteria for RA (30), she had been treated with
methotrexate (14 mg per week) for six months. During that period,
her arthritis did not improve and adalimumab, approved for the
treatment of RA and psoriasis in Japan, was introduced. The therapy
was effective and was successfully continued for four months in
addition to a reduced dose of methotrexate (8 mg per week).
Following consultation of her physician, and due to financial
considerations regarding the continuation of the drug therapy, the
patient showed interest in H2 treatment, which had been
used in clinical trials for arthritis patients at Haradoi Hospital,
particularly for RA patients (24). Her treatment with adalimumab and
corticosteroid and calcipotriol ointments was suspended prior to
commencing H2 treatment. Only methotrexate was continued
throughout the study. During the four-week washout period of
adalimumab, the patient complained about recurring pain in her
wrists and shoulders. The itching sensation and psoriatic skin
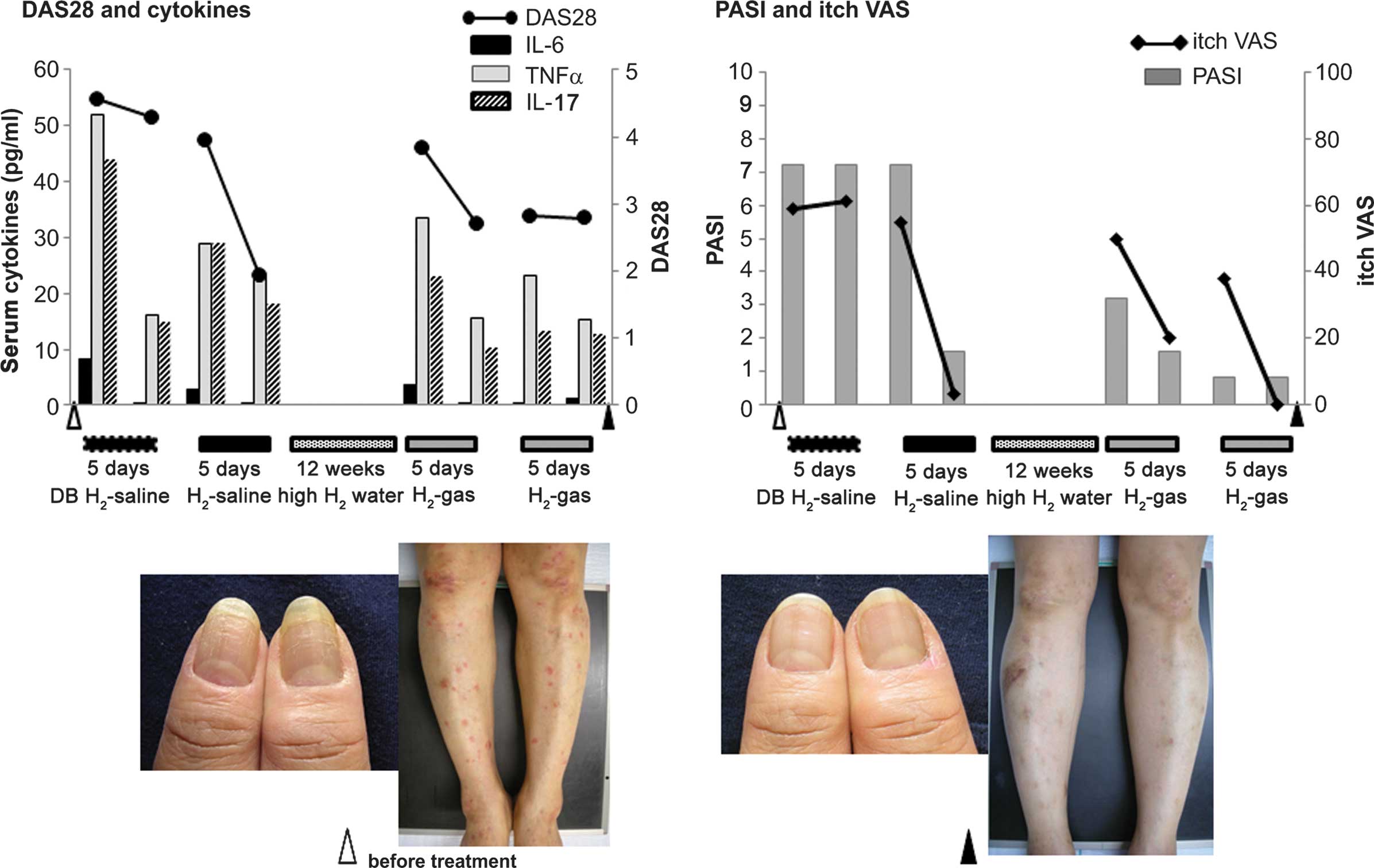
lesions also recurred (Fig. 1;
photos before treatment). She was administered an
H2-saline infusion daily for five days, first in a
randomized, double-blinded manner. As shown in Fig. 1, she underwent treatment with
double-blinded H2-saline infusion, but neither DAS28 nor
PASI score showed a remarkable decrease during this period.
However, all of the three cytokines (IL-6, 8.33 pg/ml; TNFα, 52.0
pg/ml; and IL-17, 44.1 pg/ml at baseline) decreased, particularly
IL-6, which decreased by 96% (reaching 0.3 pg/ml). Following a
two-day treatment pause, she was treated with H2-saline
openly for another five days, after which the DAS28 and PASI score
markedly decreased. Of note, the itching disappeared, and IL-6
decreased from 2.91 to 0.3 pg/ml.
After a four-week washout period, the patient was
made to drink the high-H2 water for 12 weeks. DAS28 and
PASI score as well as the VAS score for itching gradually increased
during this period. The patient then inhaled 3% H2 gas
for five days, after which PASI score as well as the pain VAS and
itch VAS were decreased. In addition, all of the cytokines were
reduced during this period. In particular, IL-6 was reduced by 92%
(from 3.64 to 0.3 pg/ml). After a three-week washout period, the
patient inhaled the H2 gas for another five days. All
symptoms, particularly those regarding the nails and skin of the
lower thigh (see images in Fig.
1), were improved at the end of the study.
Case 2
A 67-year-old man with multiple scaly erythematous
plaques on the scalp, trunk and limbs was pathologically diagnosed
as having psoriasis vulgaris >12 year prior to participation in
the present study. He complained about arthritic pain in his
wrists, knees and ankles. As radiography did not reveal any erosion
or deformity of the bones despite repetitive recurrence of
arthritis for >10 years, he was diagnosed as having psoriatic
arthritis. In addition, he had experienced severe itching on the
psoriatic lesions, which had been severely affecting his activities
of daily living for >10 years. The skin on his entire body was
frequently injured by scratching, although he had been treated with
corticosteroid and calcipotriol ointments daily, and with
narrow-band ultraviolet B (UVB) irradiation over one week at a
frequency of two or three times yearly. He was interested in
H2 treatment, since he complained of severe pain and
swelling in his wrists, left hand and right ankle, and was
experiencing itching on the psoriatic lesions. Although he had been
treated with corticosteroid and calcipotriol ointments on all the
psoriatic skin, the psoriatic lesions had not improved, except for
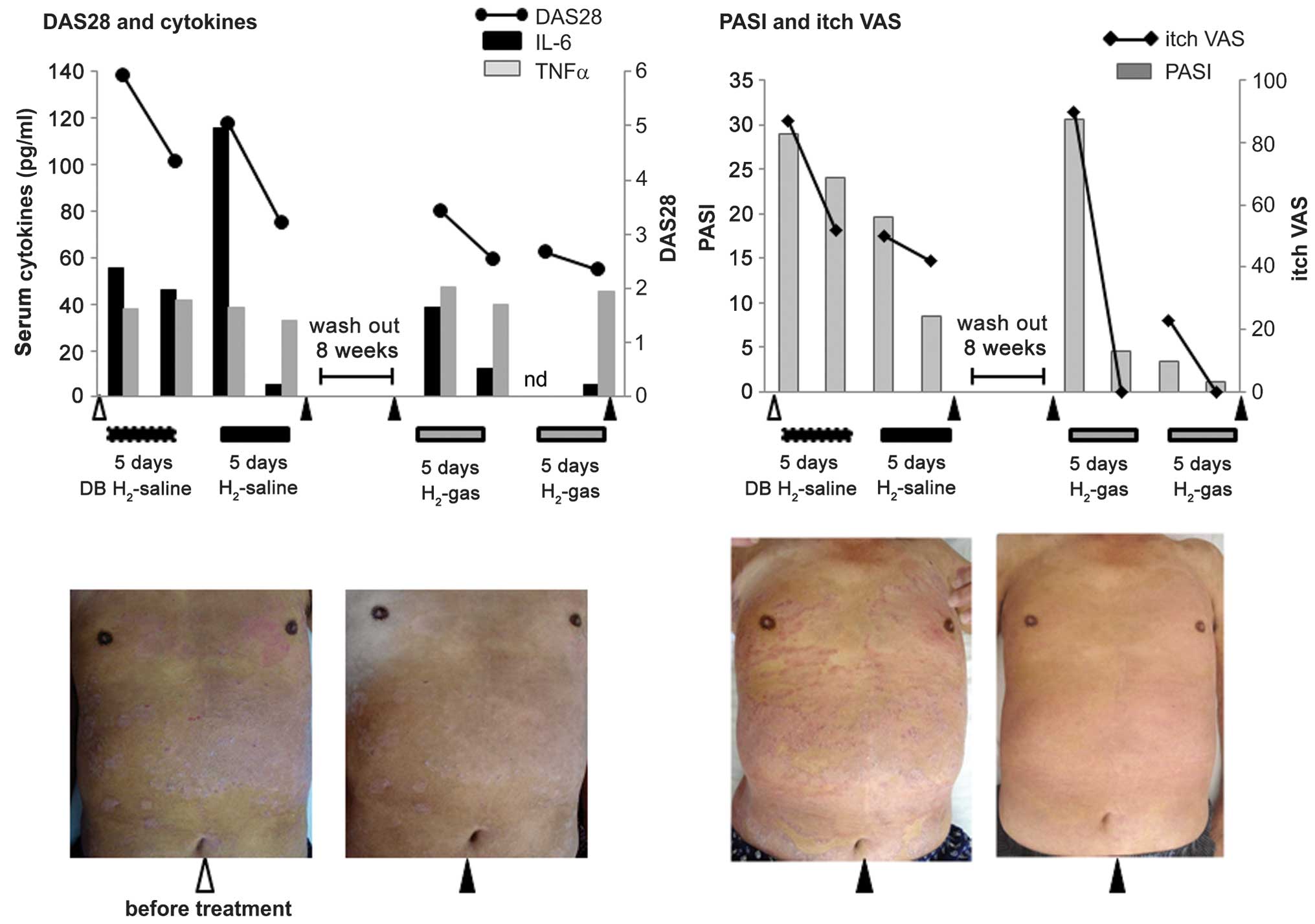
the partially reduced scale on the plaque (Fig. 2 photo, before treatment). Although
treatment with drugs was recommended to him, he declined due to
financial issues and requested H2 treatment.
After continuous treatment with corticosteroid and
calci-potriol ointments for one week (Fig. 2, image before treatment), he was
treated by venous infusion of H2 in a randomized,
double-blinded manner. During the double-blinded infusion,
treatment with the corticosteroid and calcipotriol ointments was
continued. As shown in Fig. 2, the
first five-day double-blinded infusion contained H2, and
the DAS28, PASI and itch VAS scores decreased during this period.
Among the three cytokines (IL-6, 55.3 pg/ml; TNFα, 38.1 pg/ml; and
IL-17, 0.97 pg/ml at baseline), the serum levels of IL-17 were
below the standard value (4 pg/ml) throughout the study. The skin
lesion improvement during this period may have been due to the
conventional ointment treatment, while the amelioration of
arthritis and decrease of IL-6 was thought to be the effect of the
H2-saline infusion. The corticosteroid and calcipotriol
ointment treatment was then discontinued; after a one-week washout
period, the patient was treated with H2-saline openly
for another five days. During this period, the left half of the
body trunk was UVB-irradiated. At the end of this period, DAS28,
PASI and itch VAS score were further improved. There was no
difference in the psoriatic lesions of his trunk between the left
side (with UVB irradiation) and right side (without the UVB
irradiation), both of which showed remarkable improvement (Fig. 2, second image from the left). TNFα
showed no remarkable change, whereas IL-6, which had recurred
during the washout period, was markedly decreased by 95%.
Improvements in arthritis and skin lesions were thought to be the
effect of H2. After the H2-saline treatment,
the patient was recommended continuous drinking of the
high-H2 water, but he refused to drink 500 ml of water
every day.
During an eight-week washout period, the skin
lesions and arthritis recurred, and the patient requested
additional H2 therapy. During the washout period,
although he had self-administered corticosteroid and calcipotriol
ointments, the psoriatic arthritis and particularly the skin
lesions exacerbated (Fig. 2, third
image from the left), with the PASI and itch VAS score increased.
The corticosteroids were discontinued, and the patient was made to
inhale 3% H2 gas. The DAS28 and PASI score decreased by
the fifth day. Of note, the itching sensation disappeared and IL-6
was reduced by 31.0%. After a one-week washout period, the patient
inhaled H2 gas for another five days, after which all
symptoms were improved (Fig. 2,
right image). Among the cytokines, IL-6 showed the highest
reduction (by 90% as compared with the baseline value).
Case 3
An 81-year-old woman had experienced psoriasis
vulgaris with multiple erythematous scaly plaques mainly on the
lower limbs with simultaneous psoriatic arthritis on her wrists,
hands and knees for >20 years. She had been treated with topical
corticosteroid and calcipotriol ointment. Despite continuous
treatment with corticosteroids, her psoriatic lesion on her lateral
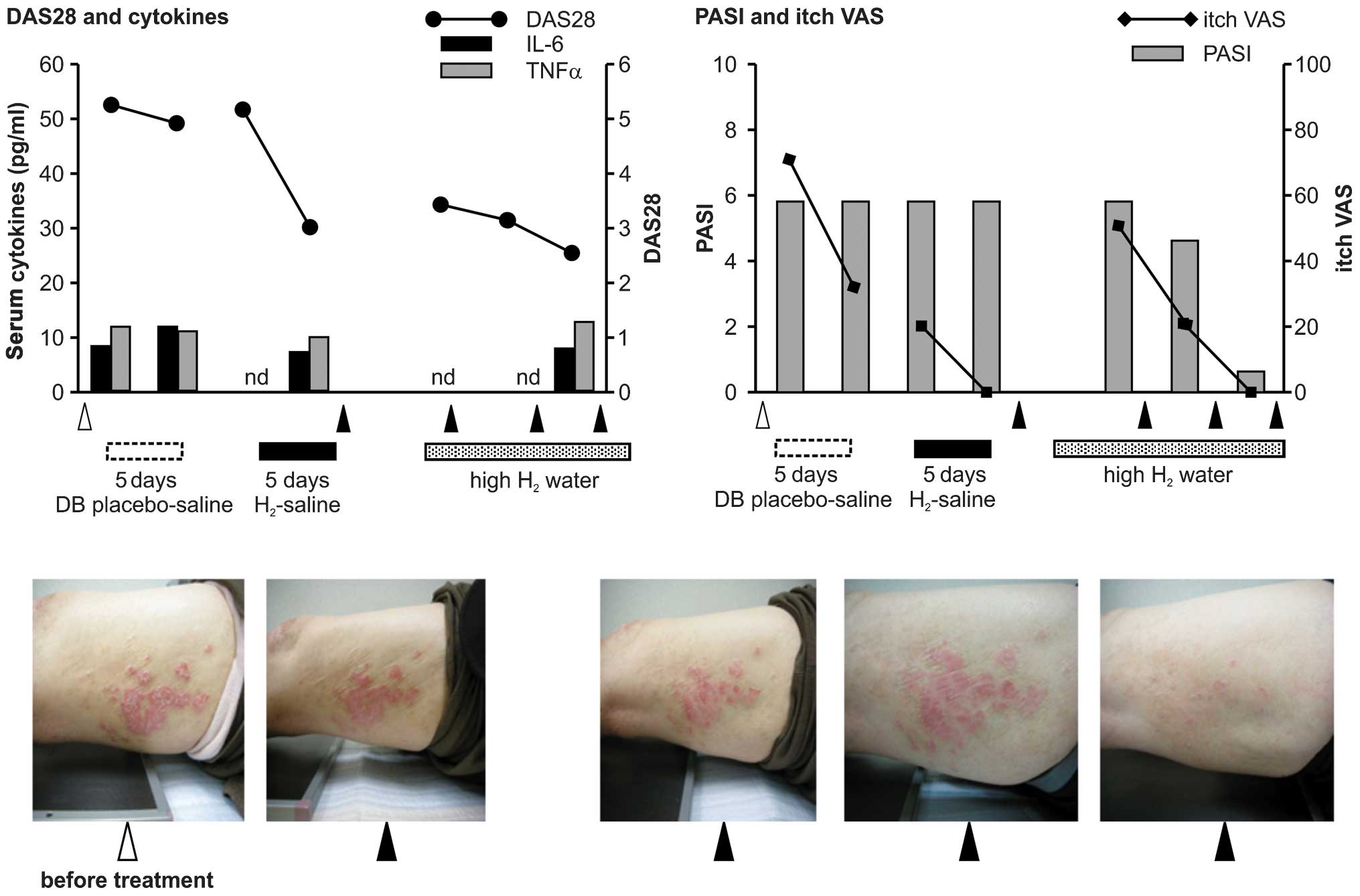
femoris had been intractable throughout (Fig. 3, image before treatment). Although
the psoriatic lesion was restricted to her limbs by continuous
treatment with corticosteroid and calcipotriol ointments, her PASI
score, which had been relatively low, remained unchanged, and the
itching on the psoriatic lesions and the pain on her wrists, hands,
shoulders and knees had severely affected her quality of life. When
she expressed her interest in H2 therapy, she complained
of pain and swelling on her wrists and hands. Since radiography did
not reveal any erosion or deformity of the bones despite persistent
arthritis for >20 years, her arthritis was not classified as RA.
The corticosteroid and calcipotriol ointments were used until the
itching was reduced during the period she drank the
high-H2 water after the infusion study. As shown in
Fig. 3, the first infusion was
double-blinded placebo saline. There was no remarkable change in
the DAS28 and PASI score. Only the itching sensation was reduced by
the placebo effect. Among the three cytokines (IL-6, 8.36 pg/ml;
TNFα, 11.9 pg/ml; and IL-17, 1.16 pg/ml at baseline), IL-6
increased and showed no remarkable change during this period. IL-17
decreased, but the serum levels were below the standard value (4
pg/ml) throughout the study (data not shown). After a two-day
treatment pause, H2 was infused openly for an additional
five days. Although the range of the femoral psoriatic lesions
appeared nearly unchanged during this period, the scaling was
improved (Fig. 3, second image
from the left) and the itching disappeared at the end of the
infusion therapy. The DAS28 also decreased during this period.
The patient was not willing to inhale H2
gas; however, she continuously drank the high-H2 water
for 16 weeks. During the first four weeks, there was no reduction
in the PASI score (Fig. 3, third
image from the left). The itch VAS score gradually increased during
this period. At eight weeks, the PASI score was slightly reduced
(Fig. 3, right image). The itching
and DAS28 scores also decreased, and the patient discontinued the
treatment with corticosteroid and calcipotriol ointments. After 16
weeks of drinking high-H2 water, the PASI score was
markedly reduced with the disappearance of the psoriatic lesions on
her lateral femoris (Fig. 3, right
image). The itching also disappeared. At the end of the study,
cytokine levels showed no significant change from those at the
beginning of the study.
The results are summarized in Table I. No adverse effects have been
observed in any of the cases presented in the present study.
 | Table ISummary of three cases. |
Table I
Summary of three cases.
| Parameters | Case 1 | Case 2 | Case 3 |
|---|
| Age
(years)/Gender | 55/F | 67/M | 81/F |
| Disease duration
(years) | 7 | 12 | 20 |
| Family history | Positive | Negative | Negative |
| Treatment for
arthritis prior to H2 | Methotrexate, 8
mg/week
Adalimumab, 40 mg/2 weeks | NSAIDs | NSAIDs |
| Treatment for skin
lesions prior to H2 | Corticosteroid and
calcipotriol ointment | Corticosteroid and
calcipotriol ointment
UVB irradiation, 2–3 times/year | Corticosteroid and
calcipotriol ointment |
| Concomitant drug
with H2 | Methotrexate | Corticosteroids
partiallya and calcipotriol
ointment
UVBb irradiation on the left
side of the trunk | Corticosteroid
ointment |
| Therapeutic
efficacy |
|
H2-infusion | Effective | Effective | Effective |
|
H2-inhalation | Effective | Effective | nd |
|
H2-drink | Partially
effective | nd | Effective |
Discussion
Psoriasis is known as a representative disease that
shows the orchestrated mechanisms of chronic inflammation (2). In the present report, the treatment
effects of three psoriasis cases with H2 appeared to
demonstrate the participation of ROS in chronic inflammation and
also the therapeutic possibilities and preventive potential of
H2, free from adverse effects.
In the present study, each of the three methods used
for H2 administration had their respective advantages.
The effect of H2-saline infusion on the autoimmune-based
and ROS-associated arthritis, such as RA, was investigated in the
present study. The high-H2 water method does not require
hospitalization and is suitable for the daily intake of
H2; however, evidence of cytokine-based improvement was
not obtained in the present study. The third method, H2
inhalation, is expected to produce a higher concentration of
H2 in the arterial blood (21); however, there is no evidence
concerning its efficacy in the treatment of arthritis or psoriatic
skin lesions. Among these methods, the infusion method, which is
currently being investigated for its therapeutic efficacy against
RA, was applied first, as the psoriatic arthritis in Cases 1 and 2
also fulfilled the diagnostic criteria of RA; however, continuous
treatment using the infusion method is difficult due to the pain
caused by the injection and the inconvenience of hospitalization;
therefore, following establishment of the proof of principle
regarding the efficacy of H2 in the treatment of
arthritis and psoriasis, other forms of administration were
employed subsequently. After the period of H2-saline
infusion, H2 was observed to continue to be efficacious.
When the symptoms recurred, it was estimated that the washout
period of H2 administered by infusion of
H2-saline was completed. The intake of H2 was
then continued by drinking high-H2 water daily. The
patient in Case 1 reported a higher efficacy of the
H2-saline than that of high-H2 water, while
the patient in Case 2, who refused drinking water as prescribed,
requested periodic treatment with H2-saline. Although
there was no clear evidence for the efficacy of the inhalation of
H2 gas, patients in Case 1 and 2 requested to try the
H2 gas inhalation method.
H2-saline infusion in a double-blinded
manner effectively reduced DAS28 and PASI score in Case 2. In
addition, the open-labeled infusion suggested beneficial effects of
H2 infusion in the treatment of psoriatic skin lesions
as well as psoriatic arthritis in all three cases. In particular,
the marked reduction of IL-6 observed in Case 1 and 2 demonstrates
the anti-inflammatory effects of H2. IL-17, which is
involved in the pathogenesis of psoriasis as well as RA, was
reduced following infusion of H2-saline in Case 1, which
was the only case in which IL-17 was above the standard value. In
Case 1, TNFα was also reduced following administration of
H2-saline. The results of all of the three cases
suggested a potential therapeutic effect of H2-saline on
psoriasis.
The inhalation of 3% H2 gas also showed
potential therapeutic efficacy in Case 1 and 2. Five days of
treatment effectively improved arthritis and skin lesions of
psoriasis. The marked decrease of IL-6 (Case 1 and 2), TNFα (Case
1), and IL-17 (Case 1) supports the therapeutic potential of
H2 gas. It should be noted that the influence of
H2 on the itching sensation of psoriasis was
significant, whether it was by venous infusion or by
inhalation.
The effects of continuous consumption of water
containing 5–7 ppm H2 on psoriasis was also marked.
Although the effect was limited in Case 1, all of the parameters,
including DAS28, PASI, itch VAS and cytokine levels, remained below
the baseline during the treatment period. In Case 3, the
therapeutic potential of the continuous consumption of
high-H2 water was obviously demonstrated, as at 16
weeks, the patient became almost free of the inveterate psoriatic
skin lesions that had not been improved by the long-term treatment
with glucocorticoid.
Although concomitant treatment was used for the skin
lesions as shown in Table I, the
treatment of arthritis was monotherapy with H2, and the
severity of arthritis was reduced in Case 2 and 3. As the psoriatic
arthritis was improved by monotherapy with H2, which was
not due to the external use of corticosteroids, it appears that the
improvement of the skin lesions was caused, to a certain extent, by
H2 treatment. Furthermore, regarding Case 1, it should
be noted that the dosage of methotrexate concomitantly used for
treating arthritis was not effective in combination with adalimumab
prior to participation in the present study, whereas the arthritis
was improved by the treatment with H2, while adalimumab
treatment was discontinued. Although the possibility that the skin
lesion improvements were caused by methotrexate treatment cannot be
excluded, it is indicated that they were in part owing to the
intake of H2 alongside the H2-mediated
improvements of psoriatic arthritis.
The involvement of ROS in the pathogenesis of
psoriasis is partially explained by the function of the skin as a
barrier against UV irradiation from sunlight or other environmental
oxidative stressors. On the contrary, UVB irradiation is used for
the treatment of psoriasis, and environmental factors may not be
sufficient to induce arthritic psoriasis. It is likely that in the
generation of psoriasis, the intrinsically produced ROS were able
to overcome the initiating hurdle formed by the activated immune
system in individuals with inherent or genetic susceptibility for
the disease. The downregulation of the cytokines that have crucial
roles in the pathogenesis of psoriasis observed in the present case
report indicates the involvement of intrinsically generated free
radicals in the development of psoriatic lesions as well as the
therapeutic efficacy of H2.
Regarding the present study, it should be noted that
the itching sensation was markedly reduced in all cases. Although
it is known that cutaneous nerves are rich in psoriatic lesions and
>50% of the patients with psoriasis experience chronic itchiness
(31,32), a more substantial contribution of
the nervous system to the pathogenesis of psoriasis, including
nerve growth factor and its receptor, has been suggested (33,34).
The influence of H2 on the itching sensation suggests
the presence of neurogenic inflammation associated with ROS in the
psoriatic lesion and the possibility of a therapeutic approach
similar to that for neurological inflammatory disorders. Among the
three methods of H2 intake, H2 gas inhalation
appeared to be particularly efficient for psoriatic skin lesions.
This may be due to the uptake of H2 into the arterial
blood in the lungs, since it is able to circulate through the body
and is released through the skin.
Recently, a compulsory anti-inflammatory approach
using biological drugs, including antibodies and chimeric proteins,
has been emerging in the treatment of psoriasis, and it is expected
to become one of the major therapeutic strategies due to the unmet
requirements of conventional therapies. These effective drugs are,
however, accompanied by side effects, recurrence after
discontinuation of the drugs, and high cost. More convenient, safe
and widely effective treatments are required to emerge.
The findings presented in this study have
limitations, as only three individual cases are reported, where
improvement of symptoms of psoriasis was observed following
H2 therapy. However, the present study provided
preliminary findings strongly indicating that H2
possesses therapeutic properties against psoriasis. Large-scale
clinical trials should be performed to evaluate the therapeutic
effect of H2. Since the safety of H2 is
established by its intrinsic production in the human body and as
H2 is inert against biogenic components, it may be
considered for the treatment of psoriasis. The daily consumption of
water containing 5–7 ppm H2, which is commercially
available, may show efficacy in the treatment of psoriasis.
Acknowledgments
The authors would like to thank Kimiko Nagao
(Haradoi-Hospital) for the technical support. We are grateful to
Ryosuke Kurokawa, Shinichi Hirano, Tomoki Seo (MiZ company), Mami
Nagao, Kazuhiro Kiyota, and Kazuhisa Fukuoka (Ecomo International)
for their excellent advice on the preparation of the devices for
using H2.
References
|
1
|
Schon MP and Boehncke WH: Psoriasis. N
Engl J Med. 352:1899–1912. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nestle FO, Kaplan DH and Barker J:
Psoriasis. N Engl J Med. 361:496–509. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goodman WA, Levine AD, Massari JV, et al:
IL-6 signaling in psoriasis prevents immune suppression by
regulatory T cells. J Immunol. 183:3170–3176. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Arican O, Aral M, Sasmaz S and Ciragil P:
Serum levels of TNF-alpha, IFN-gamma, IL-6, IL-8, IL-12, IL-17 and
IL-18 in patients with active psoriasis and correlation with
disease severity. Mediators Inflamm. 2005:273–279. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mizutani H, Ohmoto Y, Mizutani T, Murata M
and Shimizu M: Role of increased production of monocytes TNF-alpha,
IL-1beta and IL-6 in psoriasis: relation to focal infection,
disease activity and responses to treatments. J Dermatol Sci.
14:145–153. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Martin DA, Towne JE, Kricorian G, et al:
The emerging role of IL-17 in the pathogenesis of psoriasis:
preclinical and clinical findings. J Invest Dermatol. 133:17–26.
2013. View Article : Google Scholar :
|
|
7
|
Canavese M, Altruda F, Ruzicka T and
Schauber J: Vascular endothelial growth factor (VEGF) in the
pathogenesis of psoriasis-a possible target for novel therapies? J
Dermatol Sci. 58:171–176. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zaba LC, Suárez-Fariñas M, Fuentes-Duculan
J, et al: Effective treatment of psoriasis with etanercept is
linked to suppression of IL-17 signaling, not immediate response
TNF genes. J Allergy Clin Immunol. 124:1022–1010. PubMed/NCBI
|
|
9
|
Chaudhari U, Romano P, Mulcahy LD, et al:
Efficacy and safety of infliximab monotherapy for plaque-type
psoriasis: a randomised trial. Lancet. 357:1842–1847. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ulmer A, Wölbing F, Metzler G, et al:
Severe exacerbation of chronic plaque psoriasis following initially
effective therapy with efalizumab: clinical characterization and
therapeutic management. Br J Dermatol. 158:867–869. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhou Q, Mrowietz U and Rostami-Yazdi M:
Oxidative stress in the pathogenesis of psoriasis. Free Radic Biol
Med. 47:891–905. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gabr SA and Al-Ghadir AH: Role of cellular
oxidative stress and cytochrome c in the pathogenesis of psoriasis.
Arch Dermatol Res. 304:451–457. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lowes MA, Bowcock AM and Krueger JG:
Pathogenesis and therapy of psoriasis. Nature. 445:866–873. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ishibashi T: Molecular hydrogen: new
antioxidant and anti-inflammatory therapy for rheumatoid arthritis
and related diseases. Curr Pharm Des. 19:6375–6381. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Arbiser JL: Fumarate esters as
angiogenesis inhibitors: key to action in psoriasis? J Invest
Dermatol. 131:1189–1191. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lee DH, Gold R and Linker RA: Mechanisms
of oxidative damage in multiple sclerosis and neurodegenerative
diseases: therapeutic modulation via fumaric acid esters. Int J Mol
Sci. 13:11783–11803. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ohsawa I, Ishikawa M, Takahashi K, et al:
Hydrogen acts as a therapeutic antioxidant by selectively reducing
cytotoxic oxygen radicals. Nat Med. 13:688–694. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gharib B, Hanna S, Abdallahi OM, et al:
Anti-inflammatory properties of molecular hydrogen: investigation
on parasite-induced liver inflammation. C R Acad Sci III.
324:719–724. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ohno K, Ito M and Ichihara M: Molecular
hydrogen as an emerging therapeutic medical gas for
neurodegenerative and other diseases. Oxid Med Cell Longev.
2012:3531522012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hukuda S, Minami M, Saito T, et al:
Spondyloarthropathies in Japan: nationwide questionnaire survey
performed by the Japan Ankylosing Spondylitis Society. J Rheumatol.
28:554–559. 2001.PubMed/NCBI
|
|
21
|
Ishibashi T, Sato B, Rikitake M, et al:
Consumption of water containing a high concentration of molecular
hydrogen reduces oxidative stress and disease activity in patients
with rheumatoid arthritis: an open-label pilot study. Med Gas Res.
2:272012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ono H, Nishijima Y, Adachi N, et al: A
basic study on molecular hydrogen (H2) inhalation in acute cerebral
ischemia patients for safety check with physiological parameters
and measurement of blood H2 level. Med Gas Res. 2:212012.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ono H, Nishijima Y, Adachi N, et al:
Improved brain MRI indices in the acute brain stem infarct sites
treated with hydroxyl radical scavengers, Edaravone and hydrogen,
as compared to Edaravone alone. A non-controlled study. Med Gas
Res. 1:122011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ono H, Nishijima Y, Adachi N, Sakamoto M,
et al: Hydrogen (H2) treatment for acute erythematous
skin diseases. A report of 4 patients with safety data and a
non-controlled feasibility study with H2 concentration
measurement on two volunteers. Med Gas Res. 2:142012. View Article : Google Scholar
|
|
25
|
Abraini JH, Gardette-Chauffour MC,
Martinez E, Rostain JC and Lemaire C: Psychophysiological reactions
in humans during an open sea dive to 500 m with a
hydrogen-helium-oxygen mixture. J Appl Physiol (1985).
76:1113–1118. 1994.
|
|
26
|
Seo T, Kurokawa R and Sato B: A convenient
method for determining the concentration of hydrogen in water: use
of methylene blue with colloidal platinum. Med Gas Res. 2:12012.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
van de Kerkhof PC: The psoriasis area and
severity index and alternative approaches for the assessment of
severity: persisting areas of confusion. Br J Dermatol.
137:661–662. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mabuchi T, Yamaoka H, Kojima T, Ikoma M,
et al: Psoriasis affects patient’s quality of life more seriously
in female than in male in Japan. Tokai J Exp Clin Med. 37:84–88.
2012.PubMed/NCBI
|
|
29
|
Prevoo ML, van’t Hof MA and Kuper HH:
Modified disease activity scores that include twenty-eight-joint
counts. Development and validation in a prospective longitudinal
study of patients with rheumatoid arthritis. Arthritis Rheum.
38:44–48. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Levin RW, Park J, Ostrov B, Reginato A, et
al: Clinical assessment of the 1987 American College of
Rheumatology criteria for rheumatoid arthritis. Scand J Rheumatol.
25:277–281. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Reich A, Hrehorów E and Szepietowski JC:
Pruritus is an important factor negatively influencing the
well-being of psoriatic patients. Acta Derm Venereol. 90:257–263.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Verhoeven EW, Kraaimaat FW, van de Kerkhof
PC, et al: Prevalence of physical symptoms of itch, pain and
fatigue in patients with skin diseases in general practice. Br J
Dermatol. 156:1346–1349. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Raychaudhuri SK and Raychaudhuri SP: NGF
and its receptor system: a new dimension in the pathogenesis of
psoriasis and psoriatic arthritis. Ann NY Acad Sci. 1173:470–477.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zegarska B, Lelińska A and Tyrakowski T:
Clinical and experimental aspects of cutaneous neurogenic
inflammation. Pharmacol Rep. 58:13–21. 2006.PubMed/NCBI
|