Introduction
Melanoma is the cutaneous malignancy with the
highest mortality and its incidence has continued to grow over the
last 30 years (1). Although
melanoma accounts for only 4% of all dermatological cancers, it is
responsible for >80% of mortalities due to skin cancer and
<10% of patients with metastatic melanoma survive for 5-years
(2,3). The discovery and application of
biomarkers, in conjunction with conventional cancer diagnosis,
staging, and prognosis, may be useful in improving early diagnosis,
screening and the subsequent management of these patients (4). However, at present, reliable markers
are lacking and the prognosis of patients with melanoma remains
poor. Therefore, an improved understanding of the regulatory
factors contributing to melanoma initiation, progression and
metastasis is required.
The neuropilins are multifunctional proteins that
are involved in neural and vascular development, immunity and
cancer (5). Neuropilins include
two homologous proteins, NRP1 and NRP2, which are single-pass
plasma membrane receptors, that were originally identified as
binding to a tyrosine kinase receptor for semaphorin family members
and vascular endothelial growth factor (VEGF). Recent evidence also
suggests a role of neuropilins in cancer progression as a
consequence of their interaction with VEGF (6). Furthermore, neuropilins have been
observed to interact with platelet-derived growth factor (7) and other growth factors. These data
support the hypothesis that neuropilins function as a signaling
platform, regulating cancer cells and cells in the tumor
microenvironment.
NRP1 is involved in angiogenesis, axon guidance,
cell survival, invasion and migration (8). A number of types of malignant tumor
cell express NRP1, and this appears to contribute to tumor cell
aggressiveness (9,10). Furthermore, it has been
demonstrated that a soluble form of NRP1 significantly inhibits
VEGF-induced acute myeloid leukemia progression in a mouse model
(11). Blocking NRP1 function
produced a synergistic effect with that of anti VEGF, leading to
inhibition of non-small-cell lung cancer (NSCLC) growth, which
suggests that NRP1 may be a potential target for improving the
efficacy of anti-VEGF therapy (12). A study also demonstrated that
increased expression of NRP1 correlates with the growth and spread
of medulloblastoma, and with poor survival in patients with
medulloblastoma. In addition, placental growth factor acts through
NRP1, rather than VEGF receptor 1, in order to promote tumor cell
survival (13). Increased
expression of the VEGF receptors (FLT1, KDR and NRP1) and of
thrombospondin1 is associated with glomeruloid microvascular
proliferation in malignant melanoma (14). Deletion of NRP1 in healthy
epidermis prevents skin tumor initiation (15). The results of a recent study add to
the evidence suggesting that NRP1 expression promotes invasiveness
of melanoma cells through VEGFR2-dependent and -independent
mechanisms (16). However, the
significance of NRP1 in melanoma progression, diagnosis and
prognosis remains unknown.
Matrix metalloproteinase 2 (MMP2) is a
zinc-dependent proteinase that is capable of cleaving extracellular
matrix substrates. Degradation of the matrix is a crucial event in
the progression, invasion and metastasis of cancer cells. Increased
MMP2 expression was shown to predict adverse outcomes in patients
with breast cancers (17). Recent
studies have also shown that MMP2 is inversely correlated with the
survival of patients with melanoma (18,19).
It has been demonstrated that MMP2 is closely correlated with VEGF
signaling in cancer cell growth, invasion and metastasis (20,21).
NRP1 is an important receptor for VEGF. Therefore, the present
study further examined the correlation between NRP1 and MMP2
expression in melanoma biopsies, and analyzed the combined effect
of NRP1 and MMP2 expression in predicting patient outcomes.
Materials and methods
Ethics statement
The use of human skin tissues was approved by the
Clinical Research Ethics Board of the University of British
Columbia (Vancouver, BC, Canada; UBC CREB number: H09-01321)
(22). The present study was
conducted according to the principles expressed in the Declaration
of Helsinki.
Tissue microarray (TMA) construction
The collection of melanoma specimens and the
construction of the tissue microarray (TMA) have been previously
described (22,23). Briefly, formalin-fixed,
paraffin-embedded tissues from 49 common nevi, 100 dysplastic nevi,
402 primary melanomas and 162 metastatic melanomas were used for
the TMA construction. All specimens were obtained from the
1990–2009 archives of the Department of Pathology, Vancouver
General Hospital (Vancouver, BC, Canada) (22,23).
The most representative tumor area was selected and marked on the
hematoxylin and eosin stained slides, and the TMAs were assembled
using a tissue-array instrument (Beecher Instruments, Silver
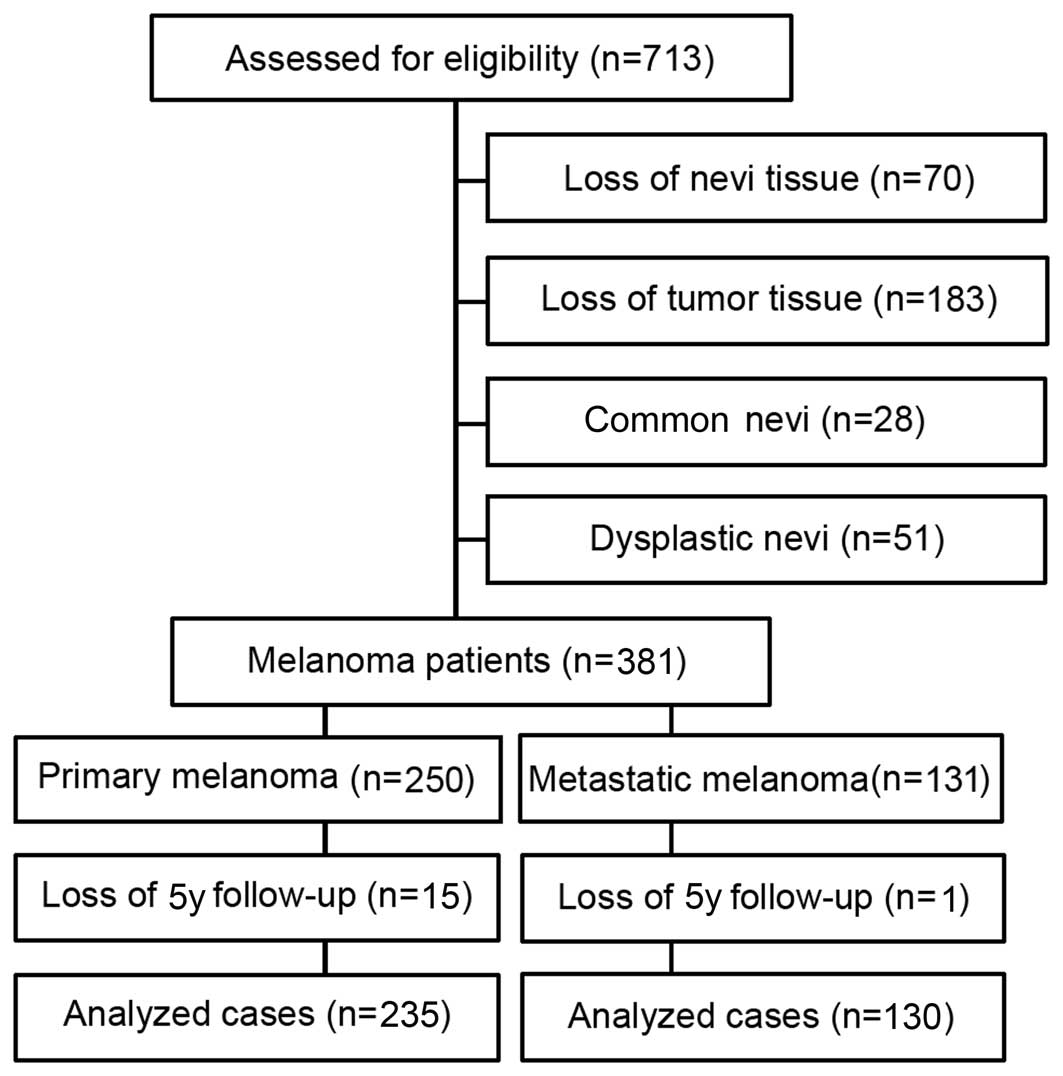
Spring, MD, USA). Due to the loss of biopsy cores or insufficient
tumor cells present in the cores, 70 nevi and 183 melanomas were
excluded from analysis. Therefore, 28 common nevi, 51 dysplastic
nevi, 250 primary melanomas and 131 metastatic melanomas were
evaluated for NRP1 staining (Fig.
1).
Immunohistochemistry of TMA
Immunohistochemistry was performed as described
previously (22,23). TMA slides were dewaxed at 55°C for
30 min and then washed with xylene (Thermo Fisher Scientific,
Waltham, MA, USA). Tissues were rehydrated by a series of washes in
100, 95 and 80% ethanol, followed by two washes in distilled water.
Antigen retrieval was performed by heating the samples at 95°C for
30 min in 10 mmol/l sodium citrate (pH 6.0; Sigma-Aldrich, St.
Louis, MO, USA). After inactivating the endogenous peroxidase by
incubating in 3% H2O2 (Sigma-Aldrich) for 30
min and blocking with universal blocking serum for 30 min, slides
were incubated with a primary mouse monoclonal anti-NRP1 antibody
(1:25; cat. no. sc-5307; Santa Cruz Biotechnology, Inc., Santa
Cruz, CA, USA) at 4°C overnight. Negative controls were produced by
omitting the NRP1 antibody during the primary antibody incubation
step. The slides were then incubated with a biotinylated
streptavidin conjugated horseradish peroxidase anti mouse and
anti-rabbit universal secondary antibody (cat. no. KO609; DAKO
Diagnostics, Glostrup, Denmark) for 30 min each, followed by
developing with a diaminobenzidine substrate kit (DAKO Diagnostics)
and counterstaining with hematoxylin.
Evaluation of immunostaining
Positive NRP1 immunostaining was defined as
cytoplasmic and membrane staining, and graded according to the
intensity and percentage of cells with positive staining. The
evaluation of NRP1 staining was done microscopic examination of the
tissue sections by two observers (including one pathologist), who
were blinded to the status of the samples, using a microscope
(Olympus BX40; Olympus, Tokyo, Japan). NRP1 staining intensity was
scored as 0, 1+, 2+ and 3+. The percentage of NRP1-positive cells
in the samples was also assigned to one of four categories: 1,
0–25%; 2, 26–50%; 3, 51–75%; and 4, 76–100%. On the basis of the
immunoreactive score, the staining pattern was defined as:
Negative, (0); weak, (1–4); moderate, (6–8); or
strong, (9–12). The optimal cut-off points for the
staining score were calculated using the MedCalc software for
Windows, version 12.5 (MedCalc Software, Ostend, Belgium). The best
area under the ROC curve (AUC) was used to determine the optimal
cut-off point of staining. Based on the AUC value, the optimal
cutoff point for the NRP1 staining was identified as 4. The
staining pattern of the biopsies was defined as: 0–4, low and 6–12,
high. The correlation between NRP1 and MMP2 expression was examined
in 365 cases (234 primary and 131 metastatic melanoma).
Statistical analysis
Differences in the demographic and clinical
characteristics, and in NRP1 expression between patient subgroups
were evaluated by the Kruskal-Wallis test and χ2 tests.
Survival time was calculated from the date of melanoma diagnosis to
the date of death or of the last follow-up. The effect of NRP1
expression on the overall and disease-specific survival was
evaluated using Kaplan-Meier analysis and a log-rank test.
Univariate and multivariate Cox proportional hazard regression
models were performed in order to estimate the hazard ratios (HRs)
or adjusted HRs, and their associated 95% confidential intervals
(CIs). P<0.05 was considered to indicate a statistically
significant difference. SPSS version 16 (SPSS Inc., Chicago, IL,
USA) software was used for all analyses.
Results
NRP1 expression is positively correlated
with melanoma progression
NRP1 staining was stronger in primary and metastatic
melanoma biopsies than that in common nevi and dysplastic nevi
cases (Fig. 2A). Kruskal-Wallis
test on the NRP1 scoring pattern in the patient samples revealed
that NRP1 expression increased significantly from common nevi (mean
3.1) and dysplastic nevi (mean 4.2), to primary melanoma (mean 6.7)
and metastatic melanoma (mean 70; P<0.0001, CN+DN vs. PM+MM;
Fig. 2B). Furthermore,
χ2 test revealed that the percentage of high NRP1
staining was significantly greater in primary melanoma (56%) and
metastatic melanoma (62%), compared with that in common nevi (11%)
and dysplastic nevi (24%) (P=3.6×10−9, CN+DN vs. PM+MM;
Fig. 2C).
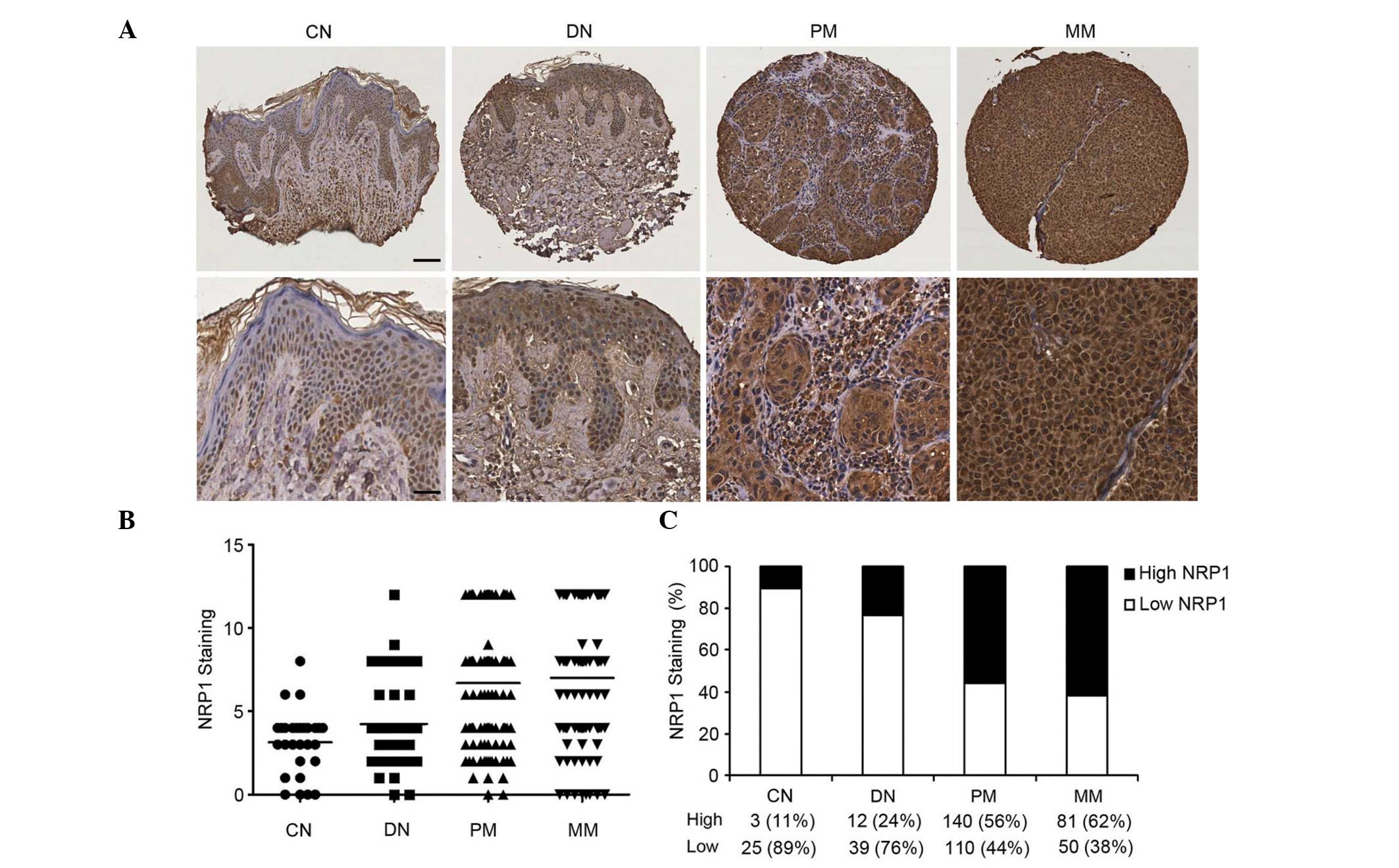 | Figure 2Increased NRP1 expression is
correlated with melanoma progression. (A) Representative images of
CN and DN, with low NRP1 expression, and PM and MM, with high NRP1
expression (upper panel, scale bar 40 µm; lower panel, scale
bar 20 µm). (B) Kruskal-Wallis test for differences in NRP1
staining among CN, DN, PM and MM. The mean is depicted as a
horizontal line in each group (n=460, P<0.0001). (C) NRP1
expression was increased from CN to DN, PM and MM (n=460,
P=3.6×10−9, χ2 test). Magnification, ×100
(upper panel), ×200 (lower panel). NRP1, neuropilin 1; CN, common
nevi; DN, dysplastic nevi; PM, primary melanoma; MM, metastatic
melanoma. |
NRP1 expression is positively correlated
with American Joint Committee on Cancer (AJCC) stage, tumor
thickness and ulceration
As NRP1 expression was correlated with melanoma
progression, the correlation between NRP1 expression and various
clinicopathological characteristics was also investigated.
Kruskal-Wallis test on the NRP1 scoring pattern in the melanoma
samples revealed that NRP1 expression increased significantly from
AJCC I (median 4) to AJCC II–IV (median 8; (P=0.007, Fig. 3A). As shown in Fig. 3B and Table I, high expression of NRP1 was
detected in 47% of melanoma specimens at AJCC stage I compared with
60–69% of melanoma specimens at AJCC II–IV (P=0.0005). However, no
significant difference was found in NRP1 expression among AJCC
stages II–IV, indicating that increased No significant difference
of NRP1 expression was found among AJCC stages II to IV, whereas a
significant increase was detected between stage I and II (P=0.0004,
stage I vs. stage II). In primary melanoma, NRP1 expression was
increased in tumors with a thickness >2.00 mm (median 8),
compared with melanomas with a thickness ≤2.00 mm (median 4;
P=0.007, Fig. 3C). Furthermore,
high NRP1 expression was observed in 67% of melanomas with a
thickness >2.00 mm, compared with 49% of tumors with a thickness
≤2.00 mm (P=0.004; Fig. 3D,
Table I). In addition, NRP1
expression was higher in melanomas with ulceration (median 8),
compared with that in melanomas with no ulceration (median 6;
P=0.004; Fig. 3E), which is in
accordance with the χ2 test results, indicating that
high NRP1 expression was observed in 76% of melanomas with
ulceration, compared with 52% of melanomas with no ulceration
(P=0.004; Fig. 3F, Table I).
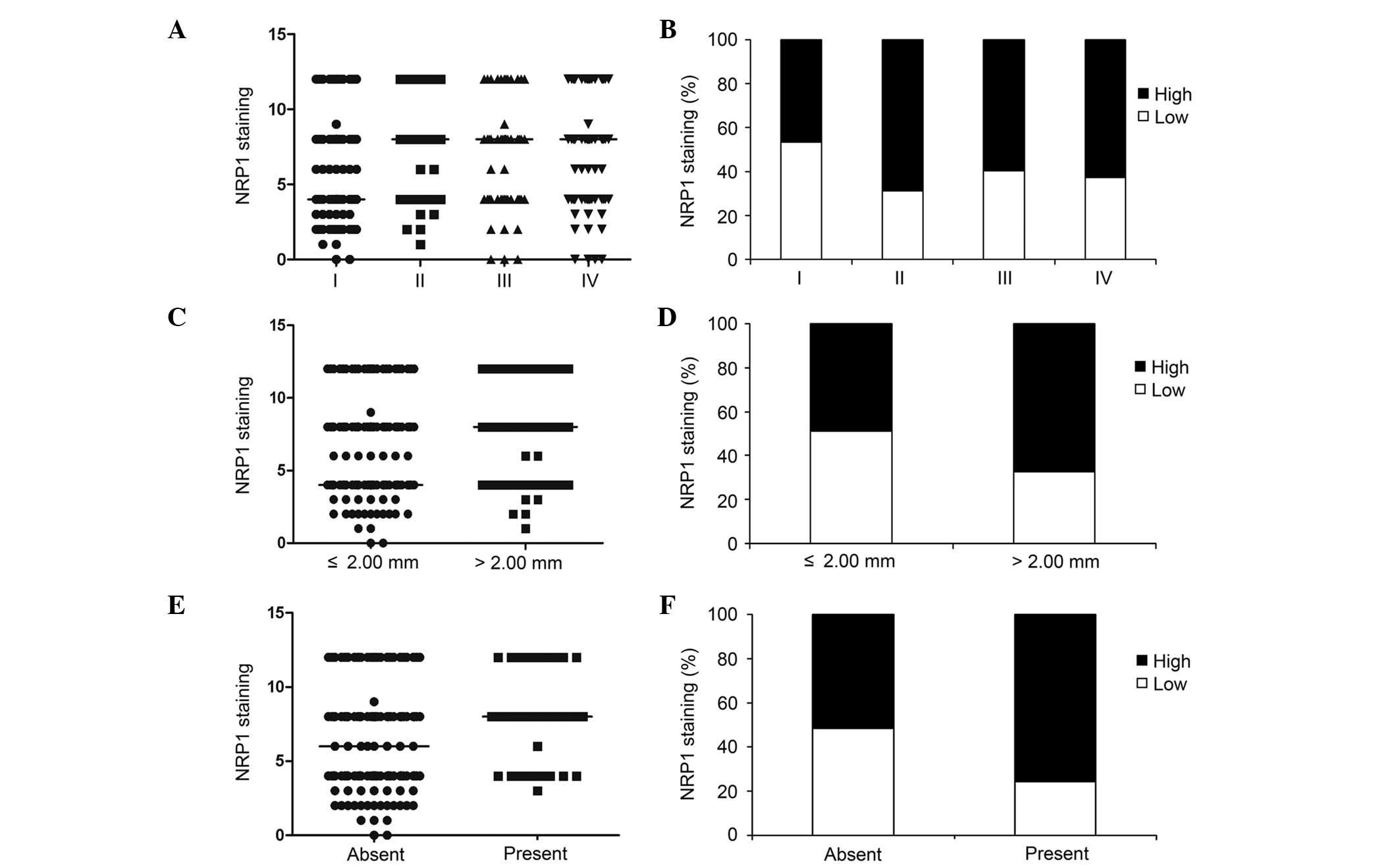 | Figure 3NRP1 expression correlates with
melanoma AJCC stage, tumor thickness and ulceration. (A)
Kruskal-Wallis test for differences in NRP1 staining among AJCC
stages I–IV. The median is depicted as a horizontal line in each
group (n=377, P=0.007). (B) Difference in NRP1 expression among
AJCC stages I–IV (n=377, P=0.003, χ2 test). Melanomas in
AJCC stages II, III and IV exhibited a higher percentage of high
NRP1 expression compared with melanomas in stage I (n=377,
P=0.0005, χ2 test). (C) Differences in NRP1 staining
between melanoma thickness ≤2.0 mm and >2.0 mm. The median is
depicted as a horizontal line in each group (n=250, P=0.007,
t-test). (D) Melanomas >2.0 mm exhibited a higher percentage of
high NRP1 expression compared with melanomas ≤2.0 mm (n=250,
P=0.004, χ2 test). (E) Differences in NRP1 staining
between melanoma patients with no ulceration and with ulceration.
The median is depicted as a horizontal line in each group (n=250,
P=0.004, t test). (F) Increased NRP1 expression was correlated with
ulceration of melanomas (n=250, P=0.004, χ2 test). NRP1,
neuropilin 1; AJCC, American Joint Committee on Cancer. |
 | Table INRP1 staining and clinicopathologic
characteristics of 381 melanomas. |
Table I
NRP1 staining and clinicopathologic
characteristics of 381 melanomas.
| Variables | NRP1 staining
| Total | P value |
|---|
| Low | High |
|---|
| All melanoma
(n=381) | | | | |
| Age, years | | | | |
| ≤60 | 95 (47.0) | 107 (53.0) | 202 (53.0) | 0.03 |
| >60 | 65 (36.3) | 114 (63.7) | 179 (47.0) | |
| Gender | | | | |
| Male | 88 (38.1) | 143 (61.9) | 231 (60.6) | 0.06 |
| Female | 72 (48.0) | 78 (52.0) | 150 (39.4) | |
| AJCC stage | | | | |
| I | 77 (53.5) | 67 (46.5) | 144 (38.2) | 0.003a |
| II | 33 (31.1) | 73 (68.9) | 106 (28.1) | 0.0005b |
| III | 21 (40.4) | 31 (59.6) | 52 (13.8) | |
| IV | 28 (37.3) | 47 (62.7) | 75 (19.9) | |
| Primary melanoma
(n=250) | | | | |
| Age, years | | | | |
| ≤60 | 58 (46.8) | 66 (53.2) | 124 (49.6) | 0.38 |
| >60 | 52 (41.3) | 74 (58.7) | 126 (50.4) | |
| Gender | | | | |
| Male | 56 (40.6) | 82 (59.4) | 138 (55.2) | 0.23 |
| Female | 54 (48.2) | 58 (51.8) | 112 (44.8) | |
| Tumor thickness
(mm) | | | | |
| ≤2 | 78 (51.3) | 74 (48.7) | 152 (60.8) | 0.004 |
| >2 | 32 (32.6) | 66 (67.4) | 98 (39.2) | |
| Ulceration | | | | |
| Absent | 99 (48.3) | 106 (51.7) | 205 (82.0) | 0.004 |
| Present | 11 (24.4) | 34 (75.6) | 45 (18.0) | |
| Subtype | | | | |
| Lentigo
maligna | 24 (47.1) | 27 (52.9) | 51 (22.0) | 0.29 |
| Superficial
spreading | 46 (50.0) | 46 (50.0) | 92 (39.7) | |
| Nodular | 14 (32.6) | 29 (67.4) | 43 (18.5) | |
| Unspecified | 20 (43.5) | 26 (56.5) | 46 (19.8) | |
| Sitec | | | | |
| Sun protected | 82 (45.1) | 100 (54.9) | 182 (72.8) | 0.58 |
| Sun exposed | 28 (41.2) | 40 (58.8) | 68 (27.2) | |
| Metastatic melanoma
(n=131) | | | | |
| Age, years | | | | |
| ≤60 | 35 (41.7) | 49 (58.3) | 78 (59.5) | 0.17 |
| >60 | 18 (25.4) | 41 (74.6) | 53 (40.5) | |
| Gender | | | | |
| Male | 32 (34.4) | 61 (65.6) | 93 (71.0) | 0.17 |
| Female | 18 (47.4) | 20 (52.6) | 38 (29.0) | |
Increased NRP1 expression is associated
with poor survival in patients with melanoma
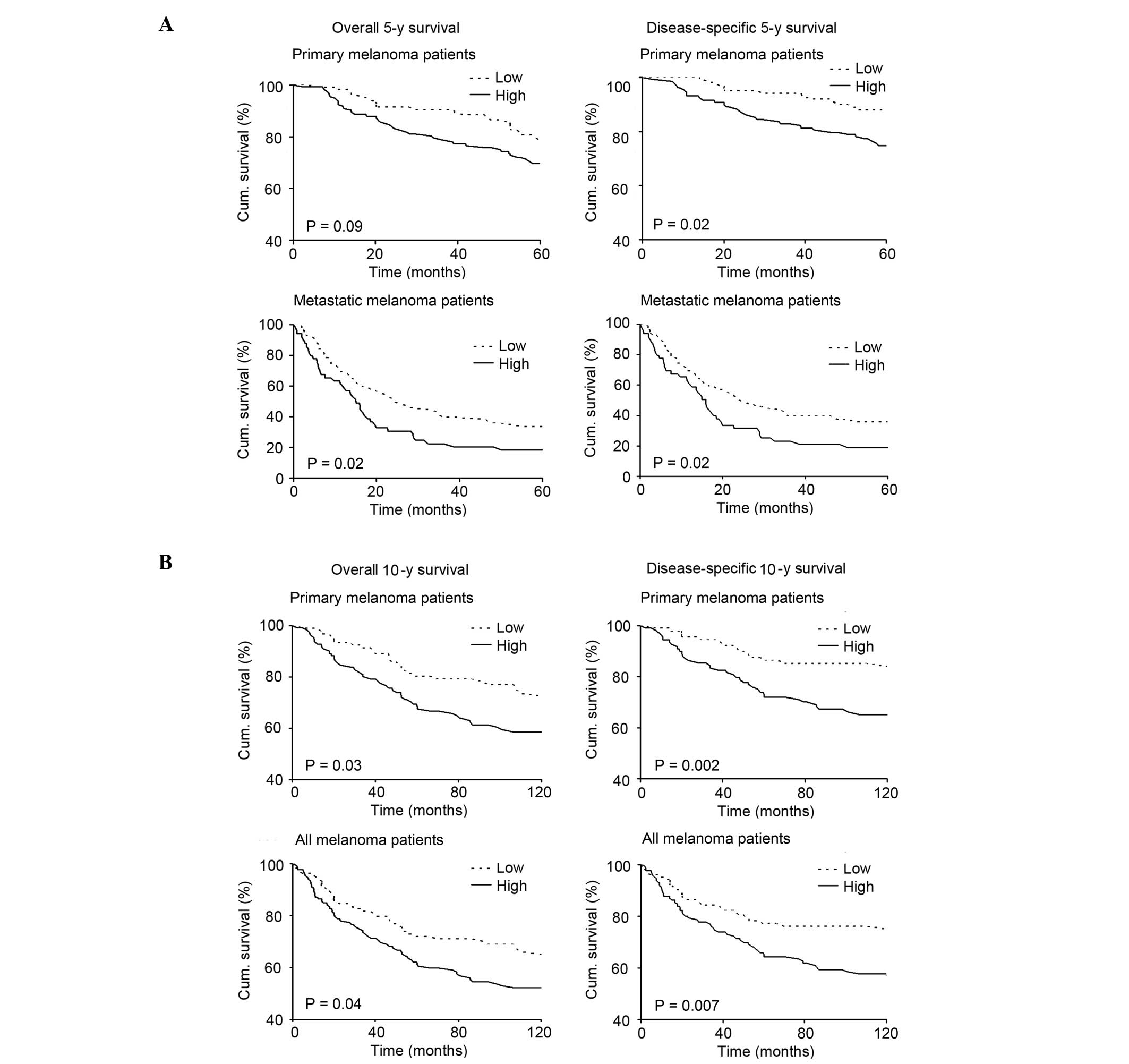
In order to investigate whether NRP1 expression is
associated with 5-year survival of patients with melanoma at
specific stages of the disease, the patient cohort was divided into
those with primary melanoma and those with metastatic melanoma, and
patient survival in each group was analyzed. The Kaplan-Meier
survival curve revealed that patients with primary or metastatic
melanoma who exhibited low NRP1 expression had a better overall
5-year survival than patients with high NRP1 expression (P=0.09 and
0.02, respectively; Fig. 4A, left
column). Furthermore, patients with low NRP1 expression who had a
diagnosis of primary or metastatic melanoma had a significantly
better disease-specific 5-year survival compared with patients with
high NRP1 expression (P=0.02 for primary and metastatic groups;
Fig. 4A, right column). In
addition, the present study investigated whether NRP1 expression
was associated with 10-year survival in patients with melanoma. As
the number of patients with metastatic melanoma is relatively small
for 10-year survival analysis, the 202 patients with primary
melanoma and 235 patients with all stages of melanoma were
analyzed. The results showed that patients with primary or all
melanoma who had low NRP1 expression had a better overall 10-year
survival than patients with high NRP1 expression (P=0.03 and 0.04,
respectively; Fig. 4B, left
column). Patients with low NRP1 expression, with primary or all
melanoma also had significantly better disease-specific 10-year
survival compared with patients with high NRP1 expression (P=0.002
and 0.007, respectively; Fig. 4B,
right column). The results of Kaplan-Meier analysis were further
confirmed by a Univariate Cox proportional hazards regression model
for 10-year survival of patients with primary melanoma (HR, 1.7;
95% CI, 1.06–2.80; P=0.03, for overall survival; HR, 2.51; 95% CI,
1.36–4.64; P=0.003, for disease-specific survival; Table II).
| Table IIUnivariate and multivariate Cox
regression analysis of 10-year survival of 202 patients with
primary melanoma. |
Table II
Univariate and multivariate Cox
regression analysis of 10-year survival of 202 patients with
primary melanoma.
A, Overall survival
|
|---|
| Variable | Univariate Cox
regression
| P | Multivariate Cox
regression
| P |
|---|
| βa | SE | HR | 95% CI | βa | SE | HR | 95% CI |
|---|
| Age | −1.22 | 0.26 | 0.29 | 0.18–0.49 |
4×10−6 | −0.79 | 0.28 | 0.45 | 0.26–0.79 | 0.005 |
| Thickness | 1.64 | 0.27 | 5.14 | 3.03–8.71 |
1×10−9 | −1.31 | 0.32 | 0.27 | 0.14–0.50 |
4×10−5 |
| Ulceration | 1.41 | 0.25 | 4.10 | 2.50–6.73 |
2×10−8 | −0.67 | 0.27 | 0.51 | 0.30–0.87 | 0.01 |
| NRP1 | 0.54 | 0.25 | 1.72 | 1.06–2.80 | 0.03 | −0.54 | 0.27 | 0.58 | 0.35–0.99 | 0.04 |
B, Disease-specific
survival
|
|---|
| Variable | Univariate Cox
regression
| P | Multivariate Cox
regression
| P |
|---|
| βa | SE | HR | 95% CI | βa | SE | HR | 95% CI |
|---|
| Age | −0.83 | 0.29 | 0.44 | 0.25–0.77 | 0.004 | −0.41 | 0.31 | 0.67 | 0.36–1.22 | 0.19 |
| Thickness | 1.82 | 0.33 | 6.15 | 3.22–11.75 |
4×10−8 | −1.42 | 0.37 | 0.24 | 0.12–0.50 |
1×10−4 |
| Ulceration | 1.51 | 0.29 | 4.52 | 2.56–7.99 |
2×10−7 | −0.77 | 0.31 | 0.46 | 0.25–0.85 | 0.01 |
| NRP1 | 0.92 | 0.31 | 2.51 | 1.36–4.64 | 0.003 | −0.76 | 0.33 | 0.47 | 0.25–0.89 | 0.02 |
NRP1 expression is an independent
prognostic marker for melanoma
The current study also examined whether NRP1
expression is an independent prognostic marker for survival of
patients with melanoma patients, using multivariate Cox
proportional hazard analysis. For 10-year survival, as the number
of metastatic melanoma cases is relatively small, initial analysis
was conducted in primary melanoma patients, adjusted for important
clinical variables, such as age, thickness and ulceration. The
results clearly indicate that, as with tumor thickness and the
presence of ulceration, which have been widely accepted as
independent prognostic factors for survival in patients with
melanoma (24), NRP1 expression is
an independent prognostic factor for overall (HR, 0.58; 95% CI,
0.35–0.99; P=0.04), and disease-specific 10-year survival (HR,
0.4.7; 95% CI, 0.25–0.89; P=0.02; Table II). Furthermore, multivariate Cox
regression analysis of 5-year survival of 130 patients with
metastatic melanoma was analyzed. The results showed that NRP1
expression was also correlated with overall (HR, 1.65; 95% CI,
1.07–2.54; P=0.02), and disease specific 5-year survival (HR, 1.64;
95% CI, 1.06–2.53; P=0.03) in patients with metastatic melanoma
(Table III).
| Table IIIMultivariate Cox regression analysis
of 5-year survival of 130 patients with metastatic melanoma. |
Table III
Multivariate Cox regression analysis
of 5-year survival of 130 patients with metastatic melanoma.
| Variable | Overall survival
| P | Disease-specific
survival
| P |
|---|
| βa | SE | HR | 95% CI | βa | SE | HR | 95% CI |
|---|
| Age | −0.12 | 0.22 | 0.88 | 0.58–1.36 | 0.57 | −0.09 | 0.22 | 0.91 | 0.59–1.41 | 0.68 |
| Sex | −0.08 | 0.23 | 0.93 | 0.59–1.45 | 0.74 | −0.12 | 0.23 | 0.89 | 0.56–1.39 | 0.60 |
| NRP1 | 0.50 | 0.22 | 1.65 | 1.07–2.54 | 0.02 | 0.49 | 0.22 | 1.64 | 1.06–2.53 | 0.03 |
NRP1 expression is positively correlated
with MMP2 expression, and their concomitant expression is
associated with reduced survival in patients with melanoma
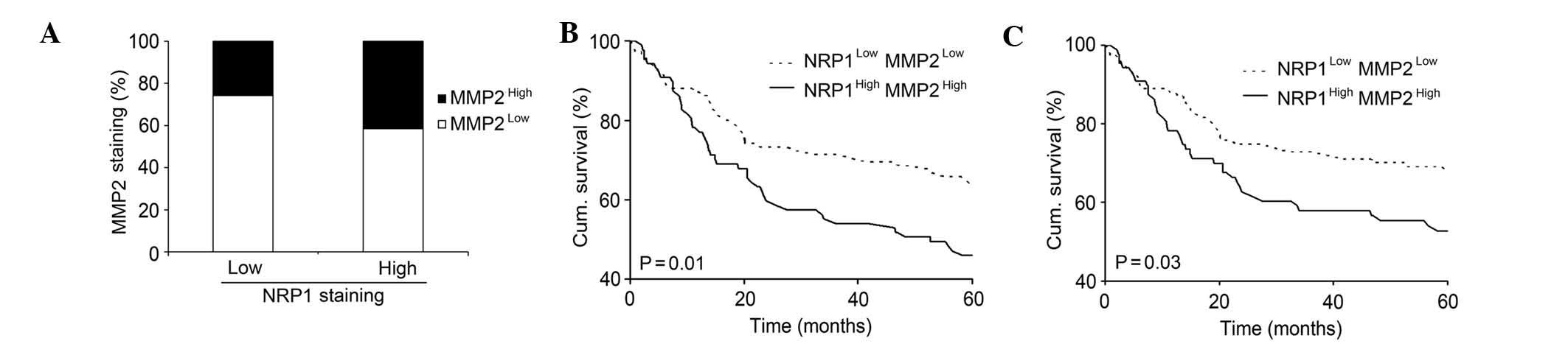
MMP2 has been shown to be associated with increased
invasion and poorer patient survival (18,19).
As the TMA used for NRP1 staining in the present study was the same
as as that previously used by this group to detect MMP2 (18), it was possible to analyze the
correlation between NRP1 and MMP2 expression. The results
demonstrated that high NRP1 was positively correlated with high
MMP2 expression (P=0.02; Fig. 5A).
The effect of combined NRP1 and MMP2 expression on patient survival
was subsequently analyzed using Kaplan-Meier survival curves, and
it was found that patients with low NRP1 as well as low MMP2
expression exhibited a significantly increased 5-year overall
survival and disease specific survival, compared with patients with
high NRP1 and high MMP2 expression (P=0.01 and 0.03, respectively.
Fig. 5B,C). These data
demonstrated that the concomitant expression of NRP1 and MMP2
exerts a significant influence on the survival of patients with
melanoma.
Discussion
Increased NRP1 expression has been detected in tumor
cell lines and tumor biopsies of various origins (10,25–27).
Furthermore, NRP1 expression correlates with more aggressive tumor
behavior. For example, in breast cancer biopsies NRP1 expression is
a feature of high-grade tumors, and is frequently expressed in
tumors from patients who do not subsequently survive as a result of
their cancer (28). In the present
study, TMA technology and immunohistochemistry were used to
investigate NRP1 expression in 460 cases of pigmented skin lesions
at different stages. To the best of our knowledge, this is the
first study to analyze the correlation between NRP1 expression, and
melanoma progression and patient survival.
The results showed that NRP1 expression was
significantly reduced in common nevi and dysplastic nevi, compared
with primary melanoma and metastatic melanoma. This indicated that
increased NRP1 activity may be a common requirement for the
transformation from benign neoplasia to malignancy, as well as for
tumor progression from primary to metastatic melanoma. This finding
supports that of a separate study, which showed that deletion of
NRP1 in normal epidermis prevents skin tumor initiation (15). The present study also found that
NRP1 expression was positively correlated with the depth of tumor
invasion (thickness ≤2.00) and ulceration of primary melanoma
lesions, which is in accordance with other studies, showing that
overexpression of NRP1 is correlated with tumor growth and
metastasis in other types of cancer, thereby influencing tumor
progression (25,27).
By constructing Kaplan Meier survival curves, it was
shown that increased NRP1 expression was correlated with poor
overall, and disease-specific 5-year survival in patients with
primary and metastatic melanoma, and was correlated with poorer
overall, and disease-specific 10-year survival in all melanoma
patients. These correlations were further confirmed by univariate
Cox regression analyses. Furthermore, multivariate Cox proportional
hazard analysis also indicated that NRP1 expression is an
independent prognostic marker for melanoma. These findings,
regarding the function of NRP1 in melanoma, are in accordance with
a previous study, indicating that NRP1 is an enhancer of cancer
invasion, that patients with high expression of NRP1 have shorter
disease-free and overall survival, and that NRP1 is an independent
predictor of cancer relapse and poor survival in patients with
NSCLC (10).
NRP1 is a specific co-receptor for the secreted
VEGF-A165 isoform. VEGF mediates tumor angiogenesis and directly
enhances tumor growth via VEGF/VEGFR autocrine loops. NRP1 forms
complexes with Flk-1/KDR (VEGFR2) to enhance the binding of VEGF165
to VEGFRs, and promotes VEGF165-mediated tumor angiogenesis, cell
migration and tumorigenicity (29,30).
In a preclinical xenograft NSCLC model, administration of a
function-blocking anti-NRP1B antibody in order to block
VEGF binding to NRP1, resulted in marginal tumor growth delay and
additive effects to anti-VEGF therapy in reducing tumor growth.
Further, tumor vascular density is decreased when
anti-NRP1B is combined with murine anti-VEGF (12), which may, therefore, make NRP1 a
potential target for improving the efficacy of anti-VEGF therapy.
Anti-NRP1, a novel antiangiogenesis agent, has been used in two
phase I trials in patients with metastatic breast cancer (31).
Increasing evidence suggests an important role for
MMPs, a large family of secreted peptidases, in tumor invasion and
metastasis (32). MMP2, or
gelatinase A, which digests primarily type IV collagen, is
hypothesized to be involved in melanoma progression (33). Increased MMP2 expression has been
shown to predict adverse outcomes in patients with breast cancer
(17). Recent studies have also
shown that MMP2 is associated with the survival of patients with
melanoma (18,19). Furthermore, it has been shown that
MMP2 expression is closely correlated with VEGF signaling in cancer
cell growth, invasion and metastasis (20,21).
For example, estrogen may increase the expression of VEGF, and thus
activate the ERK1/2 pathway to induce MMP2/9 expression (20). In addition, MMP2 is involved in the
autocrine regulation of VEGF A expression in melanoma cells
(21).
NRP1 is known to be an important receptor for VEGF.
Therefore, in the present study, greater emphasis was placed on
elucidating the correlation between NRP1 and MMP2 expression
(34). The results showed that in
365 melanoma samples, melanomas with high NRP1 expression also
exhibited a significantly higher percentage of high MMP2 staining.
Furthermore, patients with low NRP1 as well as low MMP2 expression
had better overall and disease-specific 5-year survival compared
with patients who exhibited high NRP1 and high MMP2 expression.
Based on this results, it is hypothesized that a powerful cell
survival regulator, such as NRP1, may be a positive regulator of
MMP2, and therefore promote melanoma progression, invasion and
metastasis.
In conclusion, the current study demonstrated that
NRP1 expression is significantly correlated with the progression of
human melanoma. Notably, high NRP1 expression was correlated with a
poorer 5-year and 10-year survival in patients with melanoma, and
was shown to be an independent prognostic factor. Furthermore,
there was a significant positive correlation between NRP1 and MMP2
expression in melanoma biopsies, and their concomitant expression
was inversely correlated with the survival of patients with
melanoma. These data suggest that NRP1 is involved in melanoma
pathogenesis and that it may serve as a prognostic marker for
patients with this disease.
Acknowledgments
The authors would like to acknowledge Dr Anand Rotte
for his previous research on MMP2. This study was supported by the
Canadian Institutes of Health Research (grant no. CCI-117958), the
Cancer Research Society and the Canadian Dermatology Foundation. Dr
Jing Lu is supported by National Natural Science Foundation of
China (grant no. 81101731).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Trinh VA: Current management of metastatic
melanoma. Am J Health Syst Pharm. 65(Suppl 9): S3–S8. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Miller AJ and Mihm MC Jr: Melanoma. N Engl
J Med. 355:51–65. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Geller AC, Swetter SM, Brooks K, Demierre
MF and Yaroch AL: Screening, early detection and trends for
melanoma: Current status (2000–2006) and future directions. J Am
Acad Dermatol. 57:555–572. 2007. View Article : Google Scholar
|
|
5
|
Prud’homme GJ and Glinka Y: Neuropilins
are multifunctional coreceptors involved in tumor initiation,
growth, metastasis and immunity. Oncotarget. 3:921–939. 2012.
|
|
6
|
Jia H, Cheng L, Tickner M, Bagherzadeh A,
Selwood D and Zachary I: Neuropilin-1 antagonism in human carcinoma
cells inhibits migration and enhances chemosensitivity. Br J
Cancer. 102:541–552. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Banerjee S, Sengupta K, Dhar K, et al:
Breast cancer cells secreted platelet-derived growth factor-induced
motility of vascular smooth muscle cells is mediated through
neuropilin-1. Mol Carcinog. 45:871–880. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Soker S, Takashima S, Miao HQ, Neufeld G
and Klagsbrun M: Neuropilin-1 is expressed by endothelial and tumor
cells as an isoform-specific receptor for vascular endothelial
growth factor. Cell. 92:735–745. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cao Y, Wang L, Nandy D, et al:
Neuropilin-1 upholds dedifferentiation and propagation phenotypes
of renal cell carcinoma cells by activating Akt and sonic hedgehog
axes. Cancer Res. 68:8667–8672. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hong TM, Chen YL, Wu YY, et al: Targeting
neuropilin-1 as an antitumor strategy in lung cancer. Clin Cancer
Res. 13:4759–4768. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Schuch G, Machluf M, Bartsch G Jr, et al:
In vivo administration of vascular endothelial growth factor (VEGF)
and its antagonist, soluble neuropilin-1, predicts a role of VEGF
in the progression of acute myeloid leukemia in vivo. Blood.
100:4622–4628. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pan Q, Chanthery Y, Liang WC, et al:
Blocking neuropilin-1 function has an additive effect with
anti-VEGF to inhibit tumor growth. Cancer Cell. 11:53–67. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Snuderl M, Batista A, Kirkpatrick ND, et
al: Targeting placental growth factor/neuropilin-1 pathway inhibits
growth and spread of medulloblastoma. Cell. 152:1065–1076. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Straume O and Akslen LA: Increased
expression of VEGF receptors (FLT-1, KDR, NRP-1) and
thrombospondin-1 is associated with glomeruloid microvascular
proliferation, an aggressive angiogenic phenotype, in malignant
melanoma. Angiogenesis. 6:295–301. 2003. View Article : Google Scholar
|
|
15
|
Beck B, Driessens G, Goossens S, et al: A
vascular niche and a VEGF-Nrp1 loop regulate the initiation and
stemness of skin tumours. Nature. 478:399–403. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ruffini F, D’Atri S and Lacal PM:
Neuropilin-1 expression promotes invasiveness of melanoma cells
through vascular endothelial growth factor receptor-2-dependent and
independent mechanisms. Int J Oncol. 43:297–306. 2013.PubMed/NCBI
|
|
17
|
Talvensaari-Mattila A, Pääkkö P and
Turpeenniemi-Hujanen T: Matrix metalloproteinase-2 (MMP-2) is
associated with survival in breast carcinoma. Br J Cancer.
89:1270–1275. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rotte A, Martinka M and Li G: MMP2
expression is a prognostic marker for primary melanoma patients.
Cell Oncol (Dordr). 35:207–216. 2012. View Article : Google Scholar
|
|
19
|
Väisänen AH, Kallioinen M and
Turpeenniemi-Hujanen T: Comparison of the prognostic value of
matrix metalloproteinases 2 and 9 in cutaneous melanoma. Hum
Pathol. 39:377–385. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Shan B, Li W, Yang SY and Li ZR: Estrogen
up regulates MMP2/9 expression in endometrial epithelial cell via
VEGF ERK1/2 pathway. Asian Pac J Trop Med. 6:826–830. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Desch A, Strozyk EA, Bauer AT, et al:
Highly invasive melanoma cells activate the vascular endothelium
via an MM-2/integrin αvβ5-induced secretion of VEGF-A. Am J Pathol.
181:693–705. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dai DL, Martinka M and Li G: Prognostic
significance of activated Akt expression in melanoma: A
clinicopathologic study of 292 cases. J Clin Oncol. 23:1473–1482.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lin H, Wong RP, Martinka M and Li G: Loss
of SNF5 expression correlates with poor patient survival in
melanoma. Clin Cancer Res. 15:6404–6411. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Balch CM, Gershenwald JE, Soong SJ, et al:
Final version of 2009 AJCC melanoma staging and classification. J
Clin Oncol. 27:6199–206. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Parikh AA, Fan F, Liu WB, et al:
Neuropilin 1 in human colon cancer: Expression, regulation, and
role in induction of angiogenesis. Am J Pathol. 164:2139–2151.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rizzolio S and Tamagnone L: Multifaceted
role of neuropilins in cancer. Curr Med Chem. 18:3563–3575. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bagri A, Tessier-Lavigne M and Watts RJ:
Neuropilins in tumor biology. Clin Cancer Res. 15:1860–1864. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Escudero-Esparza A, Martin TA,
Douglas-Jones A, Mansel RE and Jiang WG: PGF isoforms, PLGF-1 and
PGF-2 and the PGF receptor, neuropilin, in human breast cancer:
Prognostic significance. Oncol Rep. 23:537–544. 2010.PubMed/NCBI
|
|
29
|
Bachelder RE, Crago A, Chung J, et al:
Vascular endothelial growth factor is an autocrine survival factor
for neuropilin-expressing breast carcinoma cells. Cancer Res.
61:5736–5740. 2001.PubMed/NCBI
|
|
30
|
Whitaker GB, Limberg BJ and Rosenbaum JS:
Vascular endothelial growth factor receptor-2 and neuropilin-1 form
a receptor complex that is responsible for the differential
signaling potency of VEGF(165) and VEGF(121). J Biol Chem.
276:25520–25531. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Xin Y, Li J, Wu J, et al: Pharmacokinetic
and pharmacodynamic analysis of circulating biomarkers of
anti-NRP1, a novel antiangiogenesis agent, in two phase I trials in
patients with advanced solid tumors. Clin Cancer Res. 18:6040–6048.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Deryugina EI and Quigley JP: Matrix
metalloproteinases and tumor metastasis. Cancer Metastasis Rev.
25:9–34. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hofmann UB, Westphal JR, Van Muijen GN and
Ruiter DJ: Matrix metalloproteinases in human melanoma. J Invest
Dermatol. 115:337–344. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wu K, Fan J, Zhang L, et al: PI3 K/Akt to
GSK3β/β-catenin signaling cascade coordinates cell colonization for
bladder cancer bone metastasis through regulating ZEB1
transcription. Cell Signal. 24:2273–2282. 2012. View Article : Google Scholar : PubMed/NCBI
|