Introduction
In Italy, as well as in the majority of developed
countries, the number of females bearing children during the third
and fourth decades of life is increasing, as it is common to
postpone marriage and pregnancy due to career priorities and
advancing education, increased access to contraception and
artificial abortion, and financial concerns (1). Therefore, numerous couples, suffering
from age-related infertility due to a diminished ovarian reserve
(OR), turn to assisted reproductive technologies.
The age related effect on female fertility has been
demon strated in several studies concerning in vitro
fertilization (IVF) treatment in infertile couples, and reports
suggest that the success rate decreases in females aged >35
years (2).
When reduced OR is identified, particularly in
patients of advanced age, the probability of an insufficient
ovarian response, which leads to cycle cancellation, or oocyte
retrieval is high. This condition usually occurs in 9–24% of
females undergoing IVF treatment, and a significant proportion of
these occur in patients, who are considered 'estimated poor
responders' (EPRs) (2–4).
In a previous survey of EPR patients from 196
centres in 45 countries, a gonadotropin-releasing hormone
(GnRH)-antagonist (ant) regimen was used in 53% of IVF cycles, a
short GnRH agonist regimen was used in 20%, a GnRH agonist
micro-dose flare regimen was used in 15% and a long GnRH agonist
regimen was used in 9% (5,6).
The most common disadvantage in the GnRH-ant method
appeared to be the rapid and significant suppression of pituitary
function following the administration of GnRH-ant. Although the use
of GnRH-ant is limited in the last days of gonadotropin ovarian
stimulation, particularly using a flexible scheme, a decline in
serum luteinizing hormone (LH) and estradiol (E2) negatively
affects the number and quality of oocytes retrieved and,
subsequently, the quality of the embryo, resulting in a poor IVF
success rate (5).
Physiologically, the activity of LH is relatively
low during the menstrual period and progressively increases
throughout the mid- to late-follicular phase. During this phase, LH
induces granulosa cell growth and differentiation by promoting
local peptide synthesis and release, induces the production of
epidermal growth factor (EGF) in the thecal interstitial cells and
indirectly promotes E2 release by thse granulosa cells (7).
Shimada et al (7) demonstrated that the LH peak, inducing
the prostaglandin E2 and progesterone dependent pathways in the
granulosa cells, mediates critical events during the ovulation
process, including reprogramming of the gene expression of the
granulosa and cumulus cells during the ovulatory cascade, which
affects cumulus expansion and oocyte maturation.
Despite a previous study, performed in unselected
patients, failing to detect advantages and often reporting
contradictory results of recombinant LH (rLH) supplementation
during treatment using recombinant follicle stimulating hormone
(rFSH), there is now evidence that rLH supplementation improves the
qualitative and quantitative ovarian response, embryo quality and
the fertility rate in a selected cohort of patients (8).
A meta-analysis by Alviggi et al (8) identified this cohort in patients at
risk for poor responsiveness, exhibiting hypo-response to rFSH
alone with advanced reproductive age, treated with GnRH-ant.
At present, to the best of our knowledge, no
investigations have been performed in this cohort of patients to
identify the optimal daily dose of rLH and optimal timing of
supplementation during ovarian stimulation.
The aim of the present study was to establish the
optimal timing, between the beginning of FSH administration and the
beginning of GnRH-ant administration, and the optimal dose (75 IU,
vs. 150 IU) of rLH administration in EPR infertile females
undergoing IVF cycle using GnRH-ant, in order to achieve the
greatest number of retrieved oocytes, optimal oocyte maturation
degree and fertilization rate, optimal embryo quality, optimal
endometrial thickness at embryo-transfer and the highest pregnancy
rate.
Patients and methods
Patient information
A pilot cross-matched study was performed on female
patients undergoing two fresh, non-donor IVF cycles for primary
infertility, with rLH supplementation during ovarian stimulation.
The investigation was performed between July 2012 and July 2013 at
the Assisted Reproductive Unit of the Gynecological and Obstetrics
Clinic, Department of Women's and Children's Health of Padua
University (Padua, Italy).
All enrolled patients were informed of the aim of
the investigation and they consented to the use of their data,
according to the Italian Law for Privacy 675/96 (http://www.garanteprivacy.it/web/guest/home/docweb/-/docweb-display/export/1311248).
All patients agreed to the pilot investigation and provided written
informed consent, which was obtained at enrolment.
Following consultation of the Local Ethical
Committee, the present study was defined exempt from an
Institutional Review Board, as rLH supplementation is routinely
performed in the Assisted Reproductive Unit of Gynecologic and
Obstetrics Clinic, Department of Women's and Children's Health of
Padua University, according to the internal treatment instructions,
and the pilot nature of the investigation.
The predominant focus of the EPR cohort of patients
was their ovarian biological age, rather than their chronological
age, as suggested by the Bologna Criteria (2,3).
Inclusion/Exclusion criteria
Patients were excluded if they had a history of
smoking in the previous 6 months, deep endometriosis with an
elevated CA125 serum value (9), a
previous ART cycle in the last three months, a body mass index
(BMI) >30, abnormalities of karyotype, mutations of the cystic
fibrosis gene, acquired or inherited thrombophilia or immunological
disorders, previous chemotherapy and/or radiotherapy treatment for
cancer, untreated uterine diseases, including endometrial polyps,
submucous myomas, intrauterine synechiae and/or uterine septum
(10,11) or severe qualitative and
quantitative alterations in semen (according to World Health
Organization guidelines) (12).
Patients were also excluded if they had a basal serum LH level
>1.2 IU prior to the beginning of treatment and those who
received low-dose aspirin during treatment (13). In order to avoid a possible bias in
evaluating the pregnancy rate, patients with a personal history of
diabetes and thyroid disorders were also excluded (14,15).
Clinical intervention
All patients underwent GnRH-ant flexible
short-regimen stimulation, according to the methods of the Assisted
Reproductive Unit of Gynecologic and Obstetrics Clinic, Department
of Women's and Children's Health of Padua University. All
stimulation cycles were performed using rFSH (Gonal
F®; Merck-Serono, Geneva,
Switzerland) at 300 IU/day, beginning from the second day of
the menstrual cycle and continuing for 5 days. The subsequent dose
adjustments were determined by the clinicians during the cycles,
according to the biochemical and ultrasound features of the ovarian
response, using transvaginal sonography (TVS; Voluson e6 compact;
GE Healthcare, GE Medical Systems, Ltd., Hertfordshire, UK).
On the sixth day of stimulation, all the patients
were monitored by hormonal serum sampling (17β estradiol,
progesterone and LH) and pelvic ultrasound evaluation. The GnRH-ant
(Cetrotide®; Industria Farmaceutica Serono, Rome, Italy)
at 0.25 mg was administered daily, starting from the TVS detection
of at least one follicle measuring >14 mm in diameter, and was
continued until human chorionic gonadotropin (hCG)
administration.
When an adequate number of follicles (at least three
follicles >18 mm in diameter) were observed, 250 μg
recombinant hCG (Ovitrelle®; Merck-Serono) was
administered to induce ovulation.
Oocyte retrieval was performed in theatre 35 h after
hCG administration. The oocytes were fertilized using an
intracytoplasmic sperm injection technique. On day 3 following
retrieval, the obtained embryos were transferred, ensuring to
transfer three embryos, when obtained.
Pregnancy was confirmed by an increased
concentration of β-hCG 2 weeks after embryo transfer (ET), and TVS
detection of an intrauterine gestational sac 3–4 weeks after ET.
Ongoing pregnancy was defined by the detection of an embryonic
heart beat at the TVS assessment 5–6 weeks following the ET.
As luteal support, vaginal progesterone 200 mg
(Progeffik®, Effik Italia, Milan, Italy) was
administered three times daily until day 14 after retrieval,
terminating the treat ment in the case of a negative β-hCG serum
test (16).
Study protocol
At the first cycle, all eligible patients were
semi-randomized into group A and group B, by progressively and
alternatively assigning patients to a group on recruitment, in
order to examine a different daily dose of rLH supplementation.
The patients in group A received 75 IU rLH
(Luveris®; Merck-Serono). This group was subsequently
randomized 1:1 into two subgroups, based on the timing of rLH
supplementation: Subgroup A1 received the first rLH dose (75 IU) in
concomitance with GnRH-ant (variable day of the cycle) and subgroup
A2 received the first rLH dose (75 IU) in concomitance with rFSH
administration (second day of the cycle).
The patients in group B received 150 IU rLH. As with
group A, group B was also randomized 1:1 into two subgroups:
Subgroup B1 received the first rLH dose in concomitance with
GnRH-ant and subgroup B2 which received the first rLH dose in
concomitance with rFSH administration.
At the second cycle, performed 3 months later,
patients who had not become pregnant in the first cycle were
reassigned to the alternate group, with patients originally in
group A reassigned to group B and vice versa, and were subsequently
randomized into subgroup A1/A2 or subgroup B1/B2, as in the first
treatment cycle.
Data collection
For all patients, the following data were collected:
Age, body mass index (BMI), total dose of rFSH and rLH
administration, days of rLH supplementation, serum levels of 17β E2
and progesterone at hCG administration, number of follicles >10
mm at GnRH-ant administration, number of total follicles and number
of follicles measuring >16 mm at hCG administration, endometrial
thickness at retrieval, total number of oocytes retrieved, numbers
of oocytes at the mature (MII); immature (MI) and germinal vesicle
(GV) stages, number of oocytes fertilized, number of embryos
obtained, quality of embryos obtained and pregnancy rate. According
to Son et al (17) and
Khoudja et al (18),
embryos were classified as good, intermediate or poor quality on
the basis of the blastomere number, difference in size and degree
of fragmentation.
Endpoints
The primary aim of the present study was to assess
differences in all subgroups in follicular growth and the number
and quality of oocytes retrieved/embryos obtained and their
association with the timing and dose of rLH supplementation.
The secondary aim was to compare patients who had
received a low total dose of rLH (<500 IU; termed cohort 1), an
intermediate total dose (500-1200 IU; cohort 2) and a high total
dose (>1,200 IU; cohort 3) in terms of follicular growth and the
number and quality of oocytes retrieved/embryos obtained.
In addition, the effect of the two treatment
procedures and the timing of rLH administration were evaluated in
terms of endometrial thickness at retrieval and the pregnancy
rate.
Statistical analysis
Statistical analysis was performed using SPSS
software version 19 (SPSS, Inc., Chicago, IL, USA) for Windows
using parametric and nonparametric tests, where appropriate. The
Kolmogorov-Smirnov test was performed to assess the normality of
the distribution. Continuous data were assessed using Student's t
test for two independent groups (general features). Analysis of
variance and Bonferroni's post-hoc test were used to compared data
from three or more subgroups. Categorical variables were assessed
using a χ2 test or Fisher's exact test, where
appropriate. The results obtained from the data collection are
expressed in absolute numbers and percentages for discrete
variables and as the mean ± standard deviation for continuous
variables. P<0.05 was considered to indicate a statistically
significant difference.
Results
In the interval duration for the present study, a
total of 40 patients were classified as eligible for involvement.
Among these, 20 patients were assigned to group A, with 10 patients
in subgroup A1 and 10 in subgroup A2, and 20 patients were assigned
to group B, with 10 patients in subgroup B1 and 10 in subgroup B2.
The two groups and the four subgroups were matched in terms of age,
BMI, basal FSH, anti-mullerian hormone, 17β estradiol and antral
follicle count (Table I).
 | Table IGeneral features of participants in
the study: Comparison between groups and subgroups. |
Table I
General features of participants in
the study: Comparison between groups and subgroups.
| Variable | No. patients (n) | Mean ± SD | Range | Subgroup (n) | Mean ± SD |
|---|
| 1st IVF
cycle | | | | | |
| Age | 40 | 40.3±1.48 | 37-42 | A1 (10) | 40.4±1.58 |
| | | | A2 (10) | 40.5±1.58 |
| | | | B1 (10) | 40.2±1.39 |
| | | | B2 (10) | 40.1±1.59 |
| Body mass
index | 40 | 23.1±1.60 | 20-25 | A1 (10) | 23.0±1.89 |
| | | | A2 (10) | 23.2±1.62 |
| | | | B1 (10) | 23.4±1.43 |
| | | | B2 (10) | 22.9±1.66 |
| b-FSH (IU/l) | 40 | 12.7±2.30 | 8.1-16.4 | A1 (10) | 12.7±2.48 |
| | | | A2 (10) | 13.6±2.13 |
| | | | B1 (10) | 12.2±1.81 |
| | | | B2 (10) | 12.3±2.75 |
| b-AMH
(μg/l) | 40 | 0.5±0.28 | 0.1-0.9 | A1 (10) | 0.5±0.29 |
| | | | A2 (10) | 0.5±0.29 |
| | | | B1 (10) | 0.6±0.27 |
| | | | B2 (10) | 0.5±0.28 |
| b-17β estradiol
(nmol/l) | 40 | 0.2±0.06 | 0.29-0.19 | A1 (10) | 0.2±0.06 |
| | | | A2 (10) | 0.2±0.06 |
| | | | B1 (10) | 0.2±0.05 |
| | | | B2 (10) | 0.2±0.05 |
| Antral follicle
count | 40 | 5.0±1.86 | 2-9 | A1 (10) | 4.8±1.81 |
| | | | A2 (10) | 4.3±1.77 |
| | | | B1 (10) | 5.9±1.85 |
| | | | B2 (10) | 5.2±1.93 |
| 2nd IVF
cycle | | | | | |
| Age | 35 | 40.3±1.55 | 37-42 | A1 (8) | 39.6±1.59 |
| | | | A2 (8) | 40.7±1.39 |
| | | | B1 (10) | 40.2±1.68 |
| | | | B2 (9) | 40.6±1.50 |
| Body mass
index | 35 | 23.2±1.58 | 20-25 | A1 (8) | 23.7±1.28 |
| | | | A2 (8) | 23.0±1.51 |
| | | | B1 (10) | 22.7±1.63 |
| | | | B2 (9) | 23.6±1.80 |
| b-FSH (IU/l) | 35 | 12.5±2.19 | 9.2-16.0 | A1 (8) | 12.8±2.32 |
| | | | A2 (8) | 13.3±2.05 |
| | | | B1 (10) | 12.3±2.18 |
| | | | B2 (9) | 11.8±2.31 |
| b-AMH
(μg/l) | 35 | 0.4±0.28 | 0.1-0.9 | A1 (8) | 0.5±0.28 |
| | | | A2 (8) | 0.3±0.31 |
| | | | B1 (10) | 0.5±0.22 |
| | | | B2 (9) | 0.4±0.29 |
| b-17β estradiol
(nmol/l) | 35 | 0.2±0.06 | 0.11-0.29 | A1 (8) | 0.2±0.05 |
| | | | A2 (8) | 0.2±0.06 |
| | | | B1 (10) | 0.2±0.06 |
| | | | B2 (9) | 0.2±0.07 |
| Antral follicle
count | 35 | 4.5±1.85 | 2-9 | A1 (8) | 5.1±1.72 |
| | | | A2 (8) | 3.6±1.50 |
| | | | B1 (10) | 4.9±2.08 |
| | | | B2 (9) | 4.5±1.94 |
In the first and second IVF cycles, no differences
were identified between the subgroups in the duration of
stimulation or the total dose of rFSH (Table II).
| Table IIComparison of the duration of ovarian
stimulation and total dose of rFSH between groups and
subgroups. |
Table II
Comparison of the duration of ovarian
stimulation and total dose of rFSH between groups and
subgroups.
| Variable | No. patients
(n) | Mean ± SD | Range | Subgroup (n) | Mean ± SD |
|---|
| 1st IVF
cycle | | | | | |
| Duration of rFSH
administration (days) | 40 | 11.4±1.25 | 9-13 | A1 (10) | 11.4±1.26 |
| | | A2 (10) | 11.2±1.39 |
| | | | B1 (10) | 11.5±1.43 |
| | | | B2 (10) | 11.4±1.07 |
| Total dose of rFSH
administered (IU) | 40 | 3,875.0±702.85 | 2,475-5,200 | A1 (10) | 3,922.5±649.62 |
| | | A2 (10) | 3,830.0±750.53 |
| | | | B1 (10) | 3,895.0±858.03 |
| | | | B2 (10) | 3,852.5±644.96 |
| 2nd IVF
cycle | | | | | |
| Duration of rFSH
administration (days) | 35 | 10.6±1.19 | 9-13 | A1 (8) | 10.5±1.19 |
| | | A2 (8) | 10.5±1.19 |
| | | | B1 (10) | 10.9±1.29 |
| | | | B2 (9) | 10.5±1.24 |
| Total dose of rFSH
administered (IU) | 35 | 3,652.1±538.80 | 2,700–4,875 | A1 (8) | 3,650.0±662.92 |
| | | A2 (8) | 3,681.2±514.04 |
| | | | B1 (10) | 3,700.0±560.88 |
| | | | B2 (9) | 3,575.0±503.74 |
In the first cycle, statistically significant
differences were identified between subgroups A1 and B, compared
with A2 and B2 regarding the number of follicles measuring >10
mm at GnRH-ant administration (P<0.001) and the number of
follicles measuring >16 mm at hCG administration (P<0.001).
However, no differences were observed between the subgroups in the
total number of follicles at hCG administration. Notably, at hCG
administration, subgroup B1 exhibited the highest mean E2 serum
value (P<0.001), while subgroup B2 exhibited the highest mean
progesterone serum value (P<0.001). On the day of retrieval,
subgroup B2 exhibited increased endometrial thickness, compared
with subgroup A1 (P<0.001). A similar trend was observed in the
second IVF cycle (Table
III).
| Table IIIComparison of transvaginal sonography
and hormonal response, and endometrium between groups and
subgroups. |
Table III
Comparison of transvaginal sonography
and hormonal response, and endometrium between groups and
subgroups.
| Variable | No. patients
(n) | Mean ± SD | Range | Subgroup (n) | Mean ± SD | P-value |
|---|
| 1st IVF
cycle | | | | | | |
| Follicles >10
mm at GnRH- ant administration (n) | 40 | 3.3±1.42 | 1-6 | A1 (10) |
4.1±1.29a | <0.001 |
| | | A2 (10) |
2.1±0.74b | |
| | | | B1 (10) |
4.5±0.85c | |
| | | | B2 (10) |
2.5±1.08d | |
| Total follicles at
hCG administration (n) | 40 | 5.9±1.96 | 3-9 | A1 (10) | 6.0±2.00 | n.s. |
| | | A2 (10) | 5.2±1.75 | |
| | | | B1 (10) | 7.2±1.75 | |
| | | | B2 (10) | 5.1±1.85 | |
| Follicles >16
mm at hCG administration (n) | 40 | 2.9±1.37 | 1-6 | A1 (10) |
3.2±1.13e | <0.001 |
| | | A2 (10) |
2.2±0.79f | |
| | | | B1 (10) |
4.5±1.08g | |
| | | | B2 (10) |
2.0±0.81h | |
| Serum value of 17β
estradiol at hCG day (nmol/l) | 40 | 5.1±1.78 | 2.45-9.05 | A1 (10) |
4.3±1.11i | <0.001 |
| | | A2 (10) |
3.9±0.69j | |
| | | | B1 (10) |
7.7±0.94k | |
| | | | B2 (10) |
4.3±0.81l | |
| Serum value of
progesterone at hCG day (nmol/l) | 40 | 3.0±0.75 | 1.59-4.76 | A1 (10) |
2.2±0.32m | <0.001 |
| | | A2 (10) |
3.2±0.60n | |
| | | | B1 (10) |
3.0±0.50o | |
| | | | B2 (10) |
3.6±0.64p | |
| Endometrial
thickness at retrieval (mm) | 40 | 11.8±1.49 | 11.3-12.2 | A1 (10) |
10.2±0.41q | <0.001 |
| | | A2 (10) |
11.5±0.74r | |
| | | | B1 (10) |
11.4±0.93s | |
| | | | B2 (10) |
13.8±0.68t | |
| 2nd IVF
cycle | | | | | | |
| Follicles >10
mm at GnRH- ant administration (n) | 35 | 3.4±1.40 | 1-6 | A1 (8) |
4.0±1.60a | <0.01 |
| | | A2 (8) |
2.4±1.06b | |
| | | | B1 (10) |
4.4±0.85c | |
| | | | B2 (9) |
2.9±0.78d | |
| Total follicles at
hCG administration (n) | 35 | 6.4±1.54 | 3-9 | A1 (8) | 6.5±1.51 | n.s. |
| | | A2 (8) | 6.2±1.49 | |
| | | | B1 (10) | 6.8±1.32 | |
| | | | B2 (9) | 6.1±1.96 | |
| Follicles >16
mm at hCG administration (n) | 35 | 3.2±1.35 | 1-6 | A1 (8) |
3.5±1.07e | <0.001 |
| | | A2 (8) |
2.5±0.75f | |
| | | | B1 (10) |
4.6±1.07g | |
| | | | B2 (9) |
2.1±0.78h | |
| Serum value of 17β
estradiol at hCG day (nmol/l) | 35 | 4.9±1.55 | 1.60-8.10 | A1 (8) |
5.0±1.37i | <0.01 |
| | | A2 (8) |
4.0±1.15j | |
| | | | B1 (10) |
6.1±1.20k | |
| | | | B2 (9) |
4.2±1.57l | |
| Serum value of
progesterone at hCG day (nmol/l) | 35 | 3.1±0.76 | 1.52-4.35 | A1 (8) |
2.3±0.48m | <0.001 |
| | | A2 (8) |
3.1±0.56n | |
| | | | B1 (10) |
2.9±0.57o | |
| | | | B2 (9) |
4.0±0.24p | |
| Endometrial
thickness at retrieval (mm) | 35 | 11.9±1.58 | 11.3-12.5 | A1 (8) |
10.4±1.01q | <0.001 |
| | | A2 (8) |
11.2±1.00r | |
| | | | B1 (10) |
12.1±1.10s | |
| | | | B2 (9) |
13.7±1.09t | |
Comparison among the subgroups in the
quantitative/qualitative ovarian response revealed a greater number
of retrieved oocytes and MII oocytes that patients in the subgroup
B1, compared with those in the other subgroups, with a consequently
lower number of MI/GV oocytes (P<0.001). In the remaining
subgroups, a higher number of total oocytes and MII oocytes were
identified in subgroup A1, compared with subgroups A2 and B2
(P<0.01).
Similar statistical difference, to those described
above were found between the subgroups in the number of embryos
obtained, with the highest number of embryos obtained in subgroup
B1 and the lowest number obtained in subgroup A2. This trend was
also observed in the second IVF cycle (Table IV).
| Table IVData regarding
quantitative/qualitative ovarian response and embryos obtained
following ICSI technique: Comparison between groups and
subgroups. |
Table IV
Data regarding
quantitative/qualitative ovarian response and embryos obtained
following ICSI technique: Comparison between groups and
subgroups.
| Variable | No. patients
(n) | Mean ± SD | Range | Subgroups (n) | Mean ± SD | P-value |
|---|
| 1st IVF
cycle | | | | | | |
| Total oocytes
retrieved (n) | 40 | 3.9±1.46 | 2-7 | A1 (10) |
4.2±1.13a | <0.001 |
| | | A2 (10) |
2.6±0.52b | |
| | | | B1 (10) |
5.7±0.95c | |
| | | | B2 (10) |
3.1±0.74d | |
| MII oocytes
(n) | 40 | 2.9±1.48 | 0-6 | A1 (10) |
3.1±0.74e | <0.001 |
| | | | A2 (10) |
1.6±0.70f | |
| | | | B1 (10) |
4.9±0.74g | |
| | | | B2 (10) |
2.0±0.82h | |
| MI/GV oocytes
(n) | 40 | 1.0±0.68 | 0 -2 | A1 (10) | 1.1±0.74 | n.s. |
| | | | A2 (10) | 1.0±0.67 | |
| | | | B1 (10) | 0.8±0.63 | |
| | | | B2 (10) | 1.1±0.74 | |
| Total embryos
obtainedafter ICSI (n) | 40 | 2.0±1.19 | 1.67-2.43 | A1 (10) |
2.1±0.74i | <0.001 |
| | | A2 (10) |
1.1±0.74j | |
| | | | B1 (10) |
3.6±0.70k | |
| | | | B2 (10) |
1.4±0.70l | |
| 2nd IVF
cycle | | | | | | |
| Total oocytes
retrieved (n) | 35 | 3.9±1.50 | 1-7 | A1 (8) |
4.1±1.24a | <0.001 |
| | | A2 (8) |
2.8±0.99b | |
| | | | B1 (10) |
5.4±1.07c | |
| | | | B2 (9) |
3.2±1.30d | |
| MII oocytes
(n) | 35 | 2.8±1.57 | 0-6 | A1 (8) |
3.0±0.92e | <0.001 |
| | | | A2 (8) |
1.5±0.75f | |
| | | | B1 (10) |
4.7±0.95g | |
| | | | B2 (9) |
1.9±1.05h | |
| MI/GV oocytes
(n) | 35 | 1.1±0.63 | 0 -2 | A1 (8) | 1.1±0.64 | n.s. |
| | | | A2 (8) | 1.4±0.52 | |
| | | | B1 (10) | 0.7±0.67 | |
| | | | B2 (9) | 1.3±0.50 | |
| Total embryos
obtainedafter ICSI (n) | 35 | 2.4±1.28 | 1.93-2.81 | A1 (8) |
2.4±0.74i | <0.001 |
| | | A2 (8) |
1.5±0.75j | |
| | | | B1 (10) |
3.8±0.92k | |
| | | | B2 (9) |
1.6±1.01l | |
Concerning the quality of the 165 embryos obtained
from the two treatment groups, 88 grade 1 embryos (53.3%), 65 grade
2 embryos (39.3%) and 12 grade 3 embryos (7.4%) were identified.
For each single treatment, 1.16±1.0 grade 1 embryos, 0.88±0.7 grade
2 embryos and 0.16±0.4 grade 3 embryos (Table Va) were detected.
| Table VEmbryos, pregnancy and their
stratification according to groups and sub-groups of treatment. |
Table V
Embryos, pregnancy and their
stratification according to groups and sub-groups of treatment.
A, Embryo quality
and stratification according to treatment groups and subgroups
(considering 1st and 2nd IVF cycles)
|
|---|
| Patient | Grade 1 embryos
| Grade 2 embryos
| Grade 3 embryos
| Total number |
|---|
| Number | % | Number | % | Number | % |
|---|
| Subgroup |
| A1 | 22a | 55.0 | 15 | 37.5 | 3 | 7.5 | 40 |
| A2 | 9b | 39.1 | 10e | 43.5 | 4 | 17.4 | 23 |
| B1 | 48c | 64.9 | 24f | 32.4 | 2 | 2.7 | 74 |
| B2 | 9d | 32.1 | 16 | 57.1 | 3 | 10.8 | 28 |
| Total embryos
(n) | 88 | 53.3 | 65 | 39.3 | 12 | 7.4 | 165 |
B, Pregnancies and
stratification according to treatment groups and subgroups
|
|---|
| Patient | Not pregnant
| Pregnant
| Total number |
|---|
| Number | % | Number | % |
|---|
| 1st IVF
cycle |
| Subgroup |
| A1 | 9 | 90.0 | 1 | 10.0 | 10 |
| A2 | 8 | 100.0 | 0 | 0.0 | 8 |
| B1 | 7 | 70.0 | 3 | 30.0 | 10 |
| B2 | 8 | 88.9 | 1 | 11.1 | 9 |
| Total for
grade | 32 | 86.5 | 5a | 13.5 | 37 |
| 2nd IVF
cycle |
| Subgroup |
| A1 | 7 | 87.5 | 1 | 12.5 | 8 |
| A2 | 7 | 100.0 | 0 | 0.0 | 7 |
| B1 | 8 | 80.0 | 2 | 20.0 | 10 |
| B2 | 6 | 85.7 | 1 | 14.3 | 7 |
| Total for
grade | 28 | 87.5 | 4a | 12.5 | 32 |
Statistically significant differences were found
between the subgroups in embryo grading for grade 1 (P<0.001)
and grade 2 (P<0.05), but not for grade 3 (Table Va).
Following the first treatment cycle, only five
patients, all of which were in subgroup B1, produced more than
three embryos. This included four patients producing four embryos
and one patient producing five embryos. Following the second
treatment cycle, seven patients, all in subgroup B1, produced more
than three embryos; five producing four embryos and two producing
five embryos.
In terms of pregnancy rates, five (13.5%) patients
became pregnant following the first treatment cycle. This limited
number of patients did not enable the detection of statistical
differences between the subgroups, although three of the five
pregnancies (60%) were in subgroup B1, while the remaining two
pregnancies were in subgroup A1 (20%) and subgroup B2 (20%),
respectively (Table Vb).
Regarding the pregnancy rate of the 35 patients who
underwent the second IVF cycle, four patients (12.5%) became
pregnancy. In this case, two of the four pregnancies (50%) were in
subgroup B1, while the remaining two preg nancies were in subgroup
A1 (25%) and subgroup B2 (25%), respectively (Table Vb).
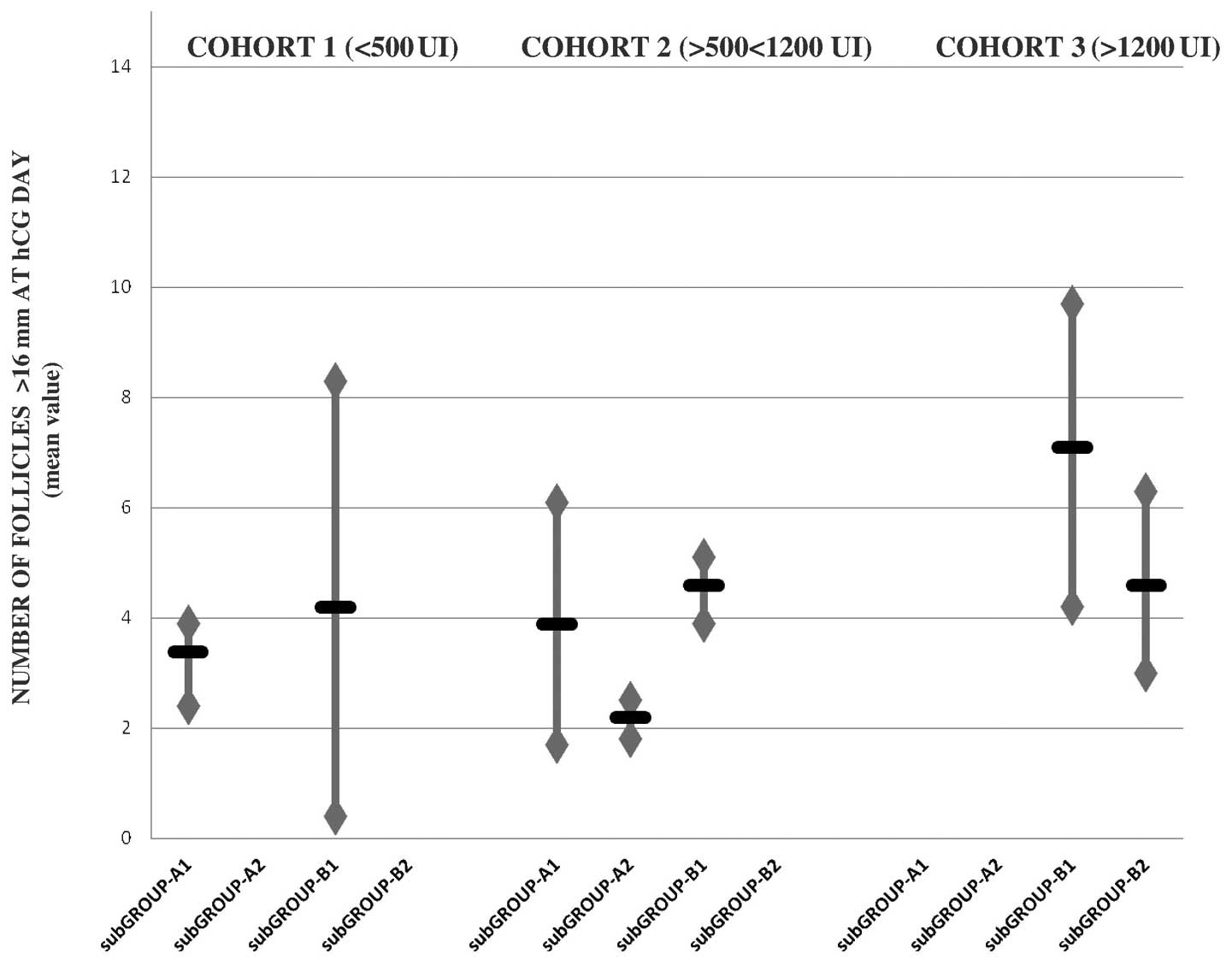
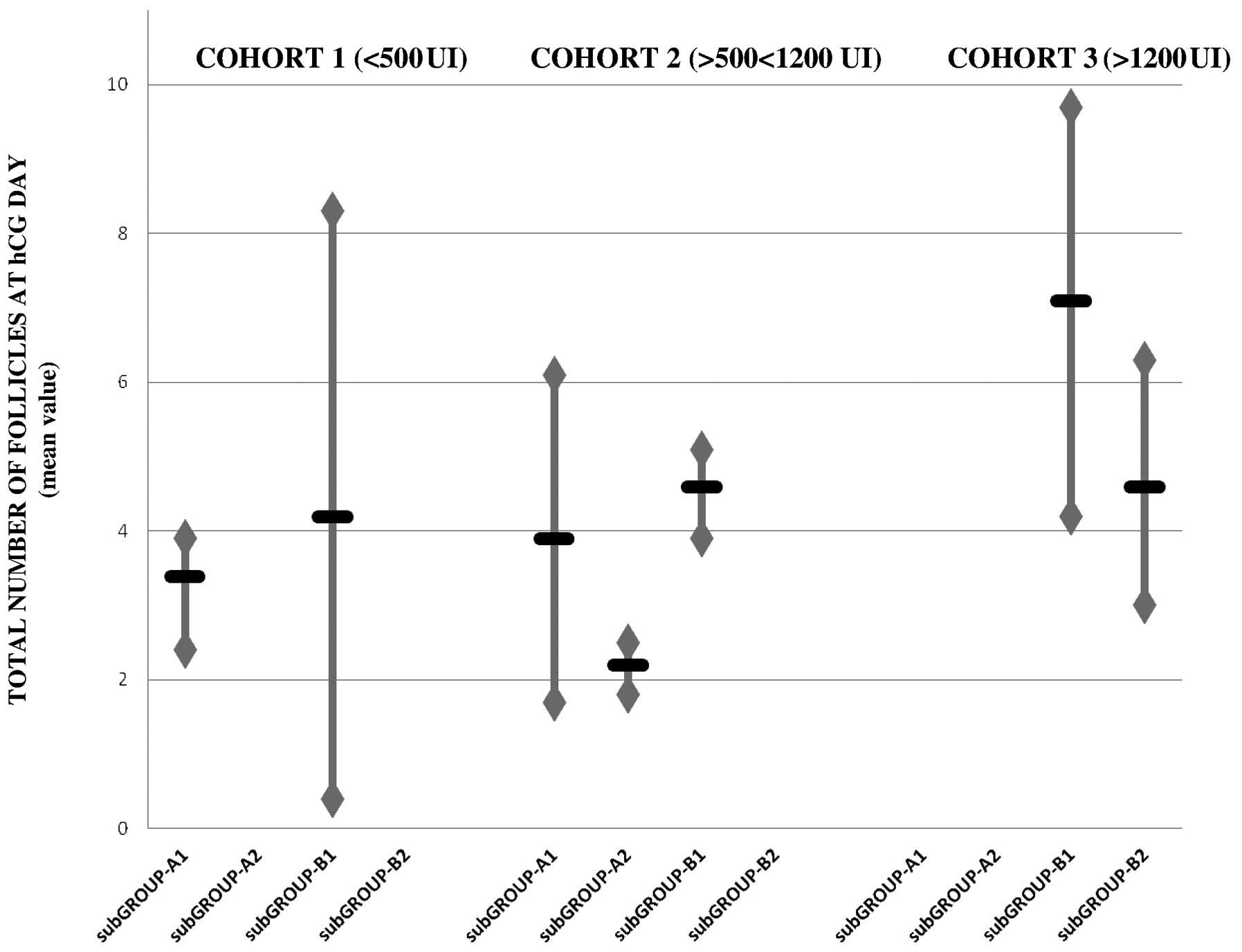
In the stratified data of the total rLH dose
administered in all treatments, no significant differences were
observed between cohorts 1, 2 or 3, in terms of the total number of
follicles at hCG administration (6.1±1.6, vs. 6.3±1.7, vs. 5.9±2.0,
respectively). Notably, subgroup B1 exhibited the optimal results
(7.0±1.52) and the results in subgroups B1 and A1 were better than
those in subgroups B2 and A2 in all of the cohorts (Fig. 1).
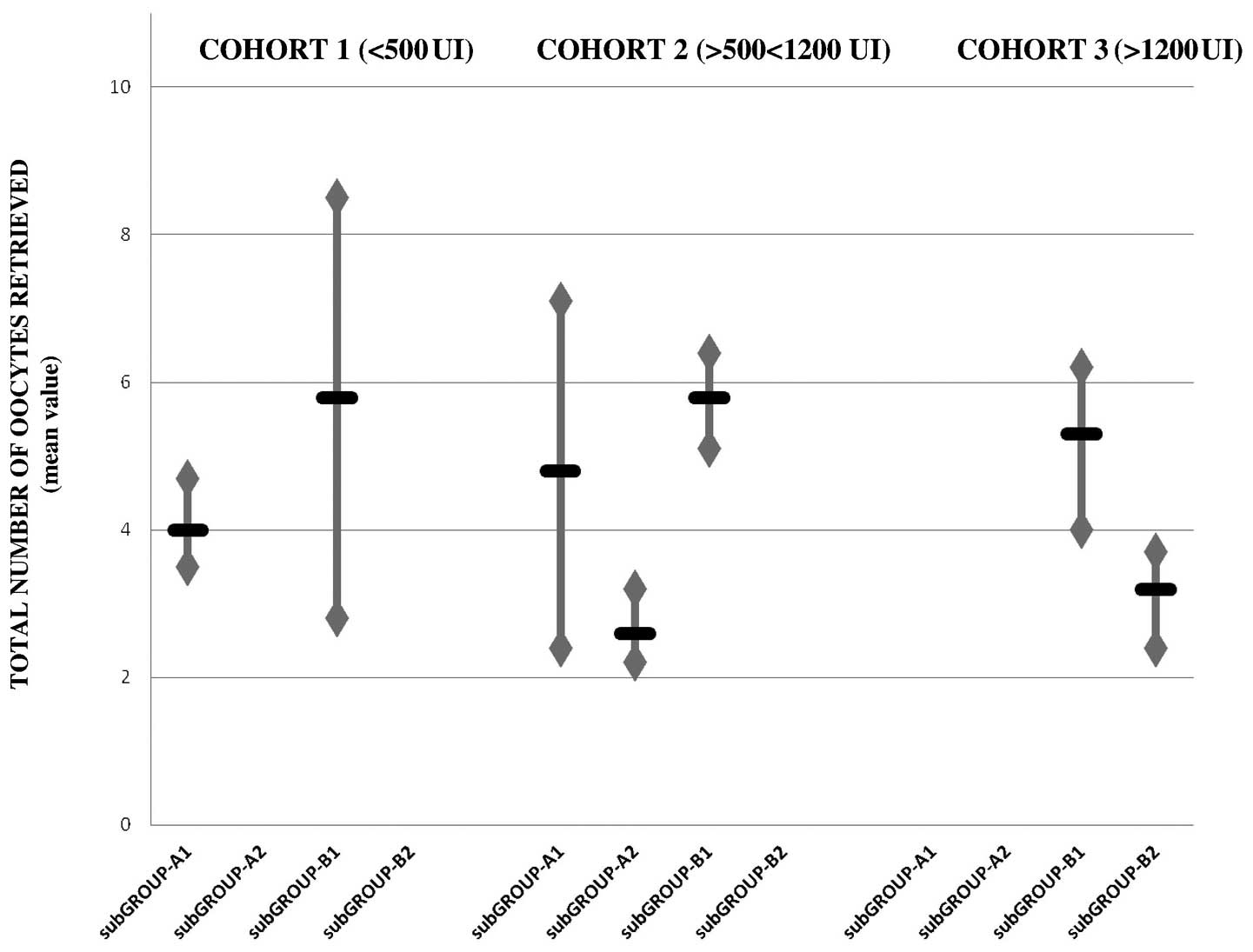
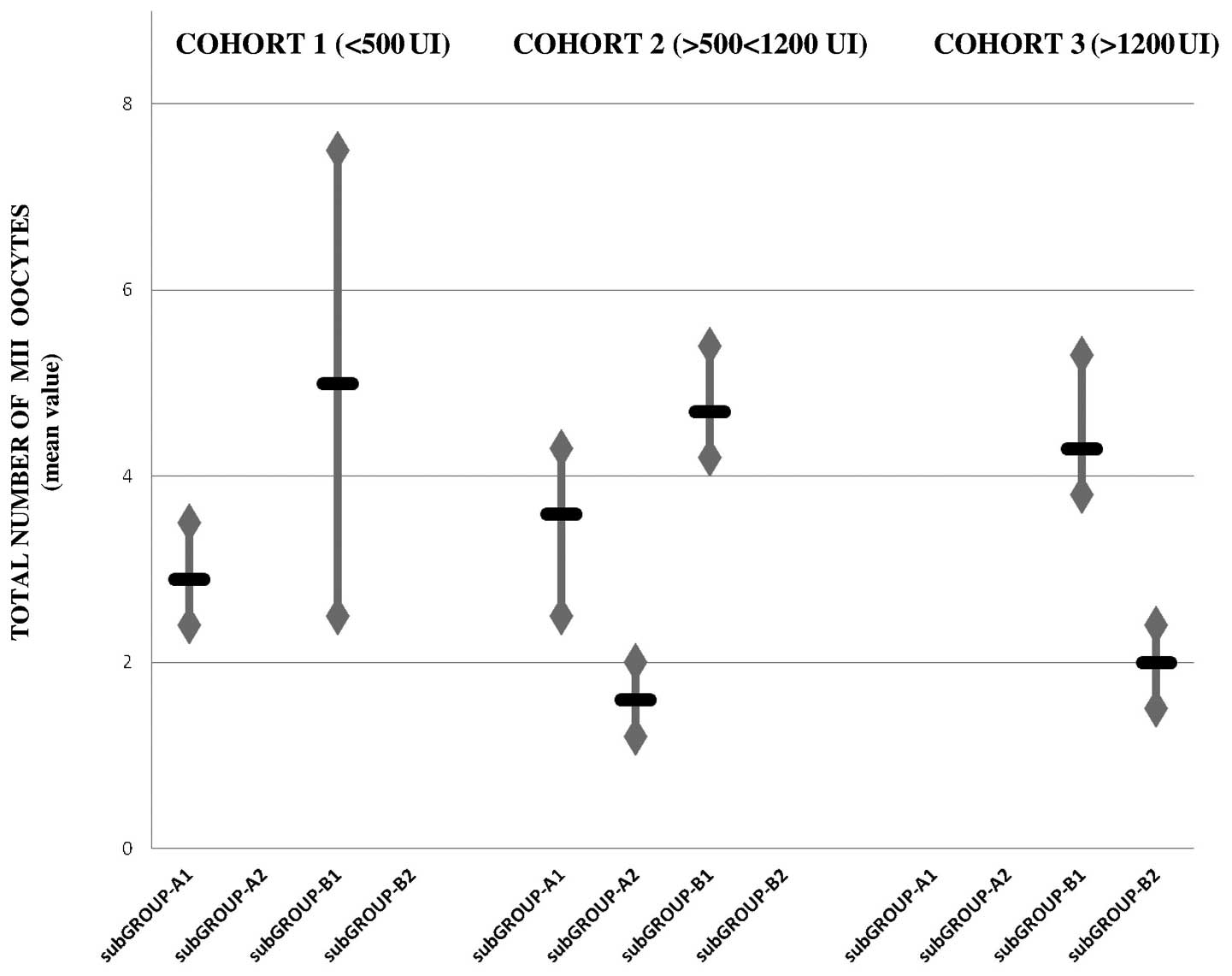
Similar to the results obtained from the total
number of follicles at hCG administration, no significant
differences were observed in the stratified data of the number of
follicles with a diameter >16 mm at hCG administration, the
total number of oocytes retrieved, and the number of MII oocytes
exhibited between the cohorts. The optimal results were identified
in subgroup B1, and subgroups B1 and A1 exhibited better results
than subgroups B2 and A2 in all cohorts (Figs. 2Figure 3–4).
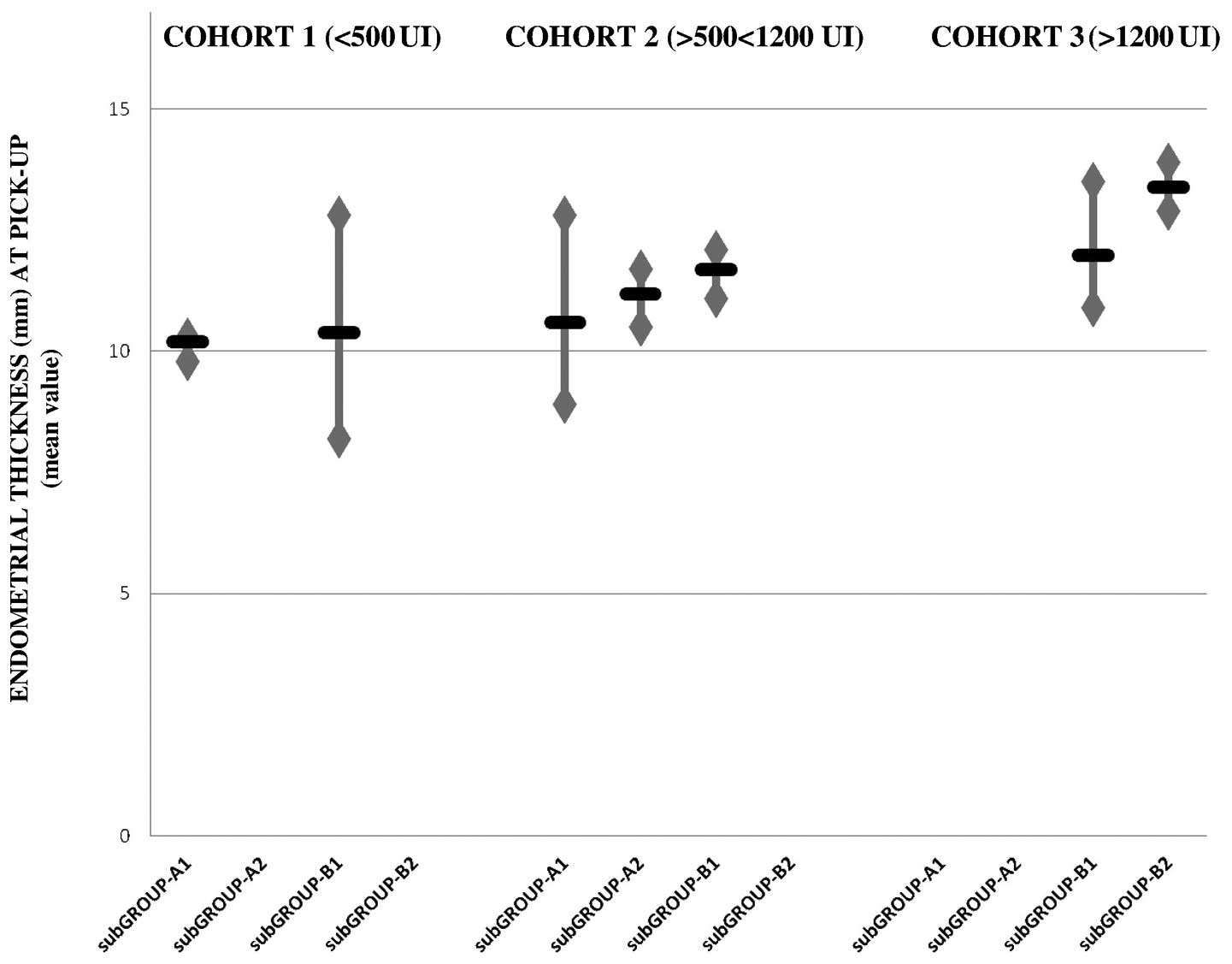
In contrast to the aforementioned findings, the
stratified data of the endometrial thickness at retrieval revealed
a statistically significant difference between the three cohorts,
with the optimum results obtained in cohort 3 and the poorest
results obtained in cohort 1 (P<0.001). Therefore, endometrial
thickness, in contrast to the ovarian response, appeared to exhibit
a greater rLH dose-dependent effect than a time-dependent effect
(Fig. 5).
Discussion
During IVF treatment, controlled ovarian
hyperstimulation is largely performed using rFSH in combination
with a GnRH analogue for the prevention of premature LH surges.
However, the use of GnRH analogues deprive the growing follicles of
LH, which can affect the qualitative and quantitative ovarian
response, as described in the 'two cell two gonadotropin' theory',
LH is required to provide the granulosa cells with androgen
precursors for estradiol biosynthesis by FSH, for the resumption of
meiosis and for progesterone production following ovulation to
sustain the endometrium (19).
Clinical data from the ovarian stimulation suggested
that the majority of the normo-gonadotrophic females achieved
adequate multi-follicular growth by the administration of rFSH
alone since, following pituitary downregulation, the residual
quantity of LH in this cohort appeared capable of sustaining the
local follicular activities required for growth and dominance
(8).
By contrast, in the EPR patients treated using
GnRH-ant in the present study, rLH supplementation appeared to
increase the ovarian response.
To the best of our knowledge, there are limited
reports regarding rLH supplementation in short GnRH-an-treated EPR
patients. In addition, the optimal timing of rLH supplementation
and its optimal daily dose remains to be elucidated.
De Placido et al (20) found that, in a cohort of EPR
patients treated using the short GnRH-ant method, rLH
supplementation of 150 IU/day at GnRH-ant administration resulted
in a higher number of MII oocytes, compared with the patients
treated using the short GnRH-agonist with the same total dose of
rLH supplementation.
Bosh et al (21) found that, in a cohort of patients
with normal ovulation cycles treated with GnRH-ant, rLH
supplementation (75 IU) significantly increased the implantation
rate, but not the pregnancy rate in females aged >35 years.
By contrast, in a study by König et al
(22), rLH adminis tration
demonstrated no improvements in ovarian response or
implantation/pregnancy rate in patients aged >35 years treated
with GnRH-ant.
Although all the patients received rFSH and rLH in
the present study, initial analysis of the data revealed
differences in ovarian response, and the quality and number of
oocytes and embryos depending on the timing and daily dose of
administration. In particular, there was a significant improvement
in the two subgroups that received rLH supplementation at GnRH-ant
administration, compared with the subgroups, which received rLH on
the first day of stimulation.
LH supplementation at GnRH-ant administration
compensates for the severe drop in levels of endogenous LH due to
administration of the antagonist itself. In addition, it produces a
gonadotrophic environment more similar to the physiological
environment. During IVF treatment, compared with the physiological
cycle, an LH surge is not necessary to select the dominant
follicle, however, its activity on the molecular cascade of the
granulosa cells persists and remains a fundamental step in
achieving a suitable ovarian response and to induce the meiotic
division of oocytes (23,24).
However, in GnRH-ant treatment, the
co-administration of FSH and LH from the second day of the
menstrual cycle produces an excess of LH, derived from endogenous
and exogenous components. The concept of an 'LH ceiling' has been
widely discussed, which refers to the maximum LH serum level, above
which the follicle is no longer stimulated. It is important to
underline that each follicle has a different ceiling 'ceiling'
level, which depends on its developmental stage. For this reason,
the same LH value may be below the ceiling dose for certain
follicles, promoting their growth, and above the ceiling dose for
other smaller follicles, causing atresia (25).
This concept explains why, when LH was administered
in the early stages of follicular growth in the present study, a
lower number of follicles measuring >10 mm at GnRH ant
administration, a lower number of follicles measuring >16 mm at
ovulation induction, and a lower number of retrieved oocytes were
observed, compared with administration at a later stage..
The data of the present study revealed no
significant differ ences between the subgroups in terms of the
total number of follicles at ovulation induction.
These findings can be explained by evidence
suggesting that the number of growing follicles recruited depends
on the quantity of available follicles (ovarian reserve) and by the
growth stimulus provided by FSH alone. However, the degree of
maturity of the retrieved oocytes was different in these follicles,
and this may be a direct effect of the timing and dose of rLH
supplementation.
During controlled ovarian stimulation, the concept
of 'FSH windows' is exceeded due to the continuous high dose of
rFSH administration in association with the absence of negative
pituitary feedback. This enables the recruitment and support of all
'responder' follicles until the pre ovulatory phase. Therefore, the
substrate of FSH action depends only on the number of primordial
and primary follicles available in the ovarian cortex at the
beginning of the cycle (26).
Concerning oocyte quality, Ruvolo et al
(27) found a lower rate of
cumulus cell apoptosis in patients treated with rFSH and rLH.
Similarly, Barberi et al (28) demonstrated that patients undergoing
stimulation with rFSH supplemented with rLH in the late follicular
phase achieved a higher concentration of RNA expression in the
cumulus cells and higher intra-follicular levels of numerous growth
factors.
The two above-mentioned authors hypothesized that
rLH supplementation results in an improved follicular environment,
enabling a comparable degree of oocyte growth and maturation to
that usually detected in young normal responders. The data of the
present study were in agreement with these findings, suggesting
that a adequate oocyte quality was achieved when rLH was
administered in the mid-follicular phase and positively affected
the number and quality of embryos obtained. Concerning hormonal
patterns, the E2 serum level detected in subgroup B1 confirmed that
the mid-follicular phase was optimal for the timing of rLH
supplementation to obtain a good quantitative and qualitative
ovarian response. By contrast, the higher level of progesterone,
observed in patients who received a high dose of rLH (subgroup B2)
confirmed the positive rLH dose-dependent effect on endometrial
thickening. It is well-established that the endometrial
implantation window is crucial to achieve optimal implantation and
pregnancy rates, however, the association between the endometrial
thickness and the implantation window remains to be elucidated.
Routinely, clinicians attempt to avoid areas of the endometrium
that are too thin or thick at retrieval, in order to reduce the
risk of low implantation rate due to the event of embryo-transfer
prior to or following the implantation windows (16). Kolibianakis et al (29) performed several investigations
regarding the role of serum levels of LH and the implantation rate,
reporting that high LH levels in the early follicular phase, which
increases the production of estrogen by androgens, anticipates the
implantation window and increases the risk of 'post-mature'
endometrium at ovulation, reducing the implantation rate. It has
been demonstrated that a discrepancy of >3 days between
ovulation and the implantation window markedly reduces the
implantation rate and, consequently, the chances of becoming
pregnant (30,31). However, despite confirming that a
high dose of rLH supplementation increased the endometrial
thickness at retrieval, the results of the present study cannot
determine whether this is a clinical advantage, as the overall
number of pregnancies achieved were insufficient and the patients
who received a higher dose of rLH were often administered the
supplement at the beginning of the stimulation.
The strengths of the present study included the
selection of the patient cohort, which appeared to be appropriate
for rLH supplementation during the IVF cycle, the strict inclusion
criteria and the homogeneity between the groups and subgroups for
general features, minimization of possible selection bias and the
use of the same stimulatory methods for all treatments, with the
exceptions of inevitable dose-adjustments during stimulation. The
present study is the first investigation, to the best of our
knowledge, with the aim of detecting the optimal dose and timing of
rLH supplementation in EPR patients, however, it was not without
limitations. The limitations included the limited sample size, and
the low ovarian response and pregnancy rates due to the features of
the patients and the lack of data regarding the possible
differences in intra-follicular growth factors. These factors not
enable the true estimation of the differences between the groups
and subgroups in terms of pregnancy rate, ongoing pregnancy and the
neonatal survival rate.
According to the available data, EPRs undergoing IVF
cycles using GnRH-ant may benefit from rLH supplementation. The
optimal timing to administer rLH appeared to be the mid-follicular
phase, which, in a large proportion of cases, corresponded with
GnRH-ant administration.
The optimal quantitative and qualitative ovarian
response, and the embryo quality were achieved by using rLH (150
IU/day) independently from the total administered dose.
Regarding the effects on the endometrium of rLH
supplementation, the total dose had a greater effect than the
timing of administration in improving endometrial thickness.
However, its impact on the improvement of pregnancy rate remains to
be elucidated.
In addition a larger range of treatments may be
required in this cohort of patients to fully understand the role of
rLH supplementation in increasing the chances of becoming preg nant
in patients with EPR.
Acknowledgments
The authors would like to thank all the staff of the
Assisted Reproductive Unit of Gynaecology and Obstetrics, Univesity
of Padua. The authors would like to acknowledge Dr Monica Lispi and
Dr Chino Giovanni (Merck Serono Group) in particular for their
scientific contribution and support in the conception and critical
data evaluation of this study.
References
|
1
|
Qiao J, Wang ZB, Feng HL, Miao YL, Wang Q,
Yu Y, et al: The root of reduced fertility in aged women and
possible therapentic options: Current status and future perspects.
Mol Aspects Med. 38:54–85. 2014. View Article : Google Scholar
|
|
2
|
Gizzo S, Andrisani A, Esposito F, Oliva A,
Zicchina C, Capuzzo D, et al: Ovarian reserve test: An impartial
means to resolve the mismatch between chronological and biological
age in the assessment of female reproductive chances. Reprod Sci.
21:632–639. 2014. View Article : Google Scholar
|
|
3
|
Ferraretti AP, La Marca A, Fauser BC,
Tarlatzis B, Nargund G and Gianaroli L: ESHRE working group on poor
ovarian response definition. ESHRE consensus on the definition of
'poor response' to ovarian stimulation for in vitro fertilization:
the Bologna criteria. Hum Reprod. 26:1616–1624. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Patrelli TS, Gizzo S, Sianesi N, Levati L,
Pezzuto A, Ferrari B, et al: Anti-Müllerian hormone serum values
and ovarian reserve: can it predict a decrease in fertility after
ovarian stimulation by ART cycles? PLoS One. 7:e445712012.
View Article : Google Scholar
|
|
5
|
Sunkara SK, Coomarasamy A, Faris R, Braude
P and Khalaf Y: Long gonadotropin-releasing hormone agonist vs.
short agonist vs. antagonist regimens in poor responders undergoing
in vitro fertilization: a randomized controlled trial. Fertil
Steril. 101:147–153. 2014. View Article : Google Scholar
|
|
6
|
IVF Worldwide Survey: Poor responders: how
to define, diagnose and treat? Downloadable at: http://www.IVF-Worldwide.com.
(Accessed: 24/02/2014).
|
|
7
|
Shimada M, Hernandez-Gonzalez I,
Gonzalez-Robayna I and Richards JS: Paracrine and autocrine
regulation of epidermal growth factor-like factors in cumulus
oocyte complexes and granulosa cells: key roles for prostaglandin
synthase 2 and progesterone receptor. Mol Endocrinol. 20:1352–1365.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Alviggi C, Clarizia R, Mollo A, Ranieri A
and De Placido G: Who needs LH in ovarian stimulation? Reprod
Biomed Online. 22(Suppl 1): 33–41. 2011. View Article : Google Scholar
|
|
9
|
Patrelli TS, Berretta R, Gizzo S, Pezzuto
A, Franchi L, Lukanovic A, et al: CA 125 serum values in surgically
treated endometriosis patients and its relationships with anatomic
sites of endometriosis and pregnancy rate. Fertil Steril.
95:393–396. 2011. View Article : Google Scholar
|
|
10
|
Saccardi C, Conte L, Fabris A, De Marchi
F, Borghero A, Gizzo S, et al: Hysteroscopic Enucleation in Toto of
Submucous type 2 myomas: Long-term follow-up in women affected by
Menorrhagia. J Minim Invasive Gynecol. 21:426–430. 2014. View Article : Google Scholar
|
|
11
|
Litta P, Cosmi E, Saccardi C, Esposito C,
Rui R and Ambrosini G: Outpatient operative polypectomy using a 5
mm-hysteroscope without anaesthesia and/or analgesia: advantages
and limits. Eur J Obstet Gynecol Reprod Biol. 139:210–214. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
World Health Organization: WHO Laboratory
Manual for the Examination of Human Semen and Sperm-Cervical Mucus
Interaction. Cambridge, UK: Cambridge University Press; 1999
|
|
13
|
Gizzo S, Capuzzo D, Zicchina C, Di Gangi
S, Coronella ML, Andrisani A, et al: Could empirical
low-dose-aspirin administration during IVF cycle affect both the
oocytes and embryos quality via COX 1 2 activity inhibition? J
Assist Reprod Genet. 31:261–8. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gizzo S, Patrelli TS, Rossanese M, Noventa
M, Berretta R, Di Gangi S, et al: An update on diabetic women
obstetrical outcomes linked to preconception and pregnancy glycemic
profile: a systematic literature review. Scientific World Journal.
2013:2549012013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Saccardi C, Gizzo S, Ludwig K, Guido M,
Scarton M, Gangemi M, et al: Endometrial polyps in women affected
by levothyroxine-treated hypothyroidism-histological features,
immunohistochemical findings and possible explanation of
etiopathogenic mechanism: a pilot study. Biomed Res Int.
2013:5034192013. View Article : Google Scholar
|
|
16
|
Gizzo S, Andrisani A, Esposito F, Noventa
M, Di Gangi S, Angioni S, et al: Which luteal phase support is
better for each IVF stimulation protocol to achieve the highest
pregnancy rate? A superiority randomized clinical trial. Gynecol
Endocrinol. 30:1–7. 2014. View Article : Google Scholar
|
|
17
|
Son WY, Chung JT, Henderson S, Reinblatt
S, Buckett W, Chan PT, et al: Fertilization and embryo development
with spermatozoa obtained from testicular sperm extraction into
oocytes generated from human chorionic gonadotropin-primed in vitro
maturation cycles. Fertil Steril. 100:989–993. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Khoudja R, Li T, Ding C, Xu Y, Liu Y, Zhou
W and Zhou C: Effect of co-incubation of oocytes with a decreasing
number of spermatozoa on embryo quality. Reprod Biomed Online.
26:353–359. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mochtar MH, Veen Van der, Ziech M and van
Wely M: Recombinant luteinizing hormone (rLH) for controlled
ovarian hyperstimulation in assisted reproductive cycles. Cochrane
Database Syst Rev. 18:CD0050702007.
|
|
20
|
De Placido G, Mollo A, Clarizia R, Strina
I, Conforti S and Alviggi C: Gonadotropin-releasing hormone (GnRH)
antagonist plus recombinant luteinizing hormone vs. a standard GnRH
agonist short protocol in patients at risk for poor ovarian
response. Fertil Steril. 85:247–250. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bosch E, Labarta E, Crespo J, Simón C,
Remohí J and Pellicer A: Impact of luteinizing hormone
administration on gonadotropin-releasing hormone antagonist cycles:
an age-adjusted analysis. Fertil Steril. 95:1031–1036. 2011.
View Article : Google Scholar
|
|
22
|
König TE, van der Houwen LE, Overbeek A,
Hendriks ML, Beutler-Beemsterboer SN, Kuchenbecker WK, et al:
Recombinant LH supplementation to a standard GnRH antagonist
protocol in women of 35 years or older undergoing IVF/ICSI: a
randomized controlled multicentre study. Hum Reprod. 28:2804–2812.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Filicori M, Cognigni GE, Pocognoli P,
Ciampaglia W and Bernardi S: Current concepts and novel
applications of LH activity in ovarian stimulation. Trends
Endocrinol Metab. 14:267–273. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Willis DS, Watson H, Mason HD, Galea R,
Brincat M and Franks S: Premature response to luteinizing hormone
of granulosa cells from anovulatory women with polycystic ovary
syndrome: relevance to mechanism of anovulation. J Clin Endocrinol
Metab. 83:3984–3991. 1998.PubMed/NCBI
|
|
25
|
Filicori M, Cognigni GE and Ciampaglia W:
What clinical evidence for an LH ceiling? Hum Reprod. 18:1556–1557.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gizzo S, Andrisani A, Noventa M, Quaranta
M, Esposito F, Armanini D, et al: Menstrual cycle length: a
surrogate measure of reproductive health capable of improving the
accuracy of biochemical/sonographical ovarian reserve test in
estimating the reproductive chances of women referred to ART.
Reprod Biol Endocrinol. 13:282015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ruvolo G, Bosco L, Pane A, Morici G,
Cittadini E and Roccheri MC: Lower apoptosis rate in human cumulus
cells after administration of recombinant luteinizing hormone to
women undergoing ovarian stimulation for in vitro fertilization
procedures. Fertil Steril. 87:542–546. 2007. View Article : Google Scholar
|
|
28
|
Barberi M, Ermini B, Morelli MB, Ermini M,
Cecconi S and Canipari R: Follicular fluid hormonal profile and
cumulus cell gene expression in controlled ovarian hyperstimulation
with recombinant FSH: effects of recombinant LH administration. J
Assist Reprod Genet. 29:1381–1391. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kolibianakis EM, Albano C, Camus M,
Tournaye H, Van Steirteghem AC and Devroey P: Initiation of
gonadotropin-releasing hormone antagonist on day 1 as compared to
day 6 of stimulation: effect on hormonal levels and follicular
development in in vitro fertilization cycles. J Clin Endocrinol
Metab. 88:5632–5637. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kolibianakis EM, Albano C, Kahn J, Camus
M, Tournaye H, Van Steirteghem AC, et al: Exposure to high levels
of luteinizing hormone and estradiol in the early follicular phase
of gonadotropin-releasing hormone antagonist cycles is associated
with a reduced chance of pregnancy. Fertil Steril. 79:873–880.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kolibianakis E, Bourgain C, Albano C,
Osmanagaoglu K, Smitz J, Van Steirteghem A, et al: Effect of
ovarian stimulation with recombinant follicle-stimulating hormone,
gonadotropin-releasing hormone antagonists and human chorionic
gonadotropin on endometrial maturation on the day of oocyte
pick-up. Fertil Steril. 78:1025–1029. 2002. View Article : Google Scholar : PubMed/NCBI
|