Introduction
The ductus venosus (DV) is a blood vessel specific
to the fetal period and belongs to an important blood circulatory
network. DV blood flow allows oxygenated blood from the placenta to
bypass the liver (1). In 1991,
using ultrasound, Kiserud et al (2) observed the DV in fetuses between
middle and late pregnancy, investigating the spectrum of the blood
flow. A previous study investigated the association between fetal
DV and chromosomal abnormalities in the first trimester of
pregnancy (8–14 weeks) (3).
The most common aneuploidy-associated syndromes are:
Down syndrome caused by trisomy 21 (T21), Patau syndrome, caused by
trisomy 13 (T13), and Edwards syndrome, caused by trisomy 18 (T18)
(4). Nuchal translucency (NT)
thickness is an established method for the prediction of all three
diseases (5–7). A previous study suggested that
abnormal DV may be the cause for the increased NT thickness in the
case of aneuploidy (8). DV
assessment may improve early detection of congenital heart defects
compared with NT measurement alone (9). In addition, Maiz et al
(10) demonstrated that abnormal
DV was associated with T21, T18 or T13. Maiz et al (10) observed that ~7.7% of fetuses
presented abnormal DV, and these fetuses exhibited a thicker NT.
Therefore, NT and DV may be used for the early diagnosis of
trisomy.
Although multiple previous studies tested the
feasibility of combining NT and DV for the prediction of the three
trisomies (T21, T18 and T13), the results were variable (Table I). The association between abnormal
DV and T21 varied between 38.3 and 92.1%, depending on the
population examined (11,12). Furthermore, previous studies tested
the reliability of integrating NT and DV for the diagnosis of T21
in the Chinese population (13),
and in the diagnosis of the other two trisomies (T18 and T13)
(10). In the present study, a
multi-level analysis was performed to test the reliability of
combining NT with DV for the prediction of T21, T18 and T13 in the
Western Chinese population. The present study aimed to provide
novel statistical analyses to the field of prenatal diagnosis in
the Western Chinese population.
 | Table I.Previous studies demonstrating
various co-occurrence rates of abnormal DV and trisomies. |
Table I.
Previous studies demonstrating
various co-occurrence rates of abnormal DV and trisomies.
| Author, year | n | T21 | T18 | T13 | Population
examined | (Refs.) |
|---|
| Maiz et al,
2009 | 19,800 | 81/122
(66.4%) | 21/36
(58.3%) | 11/20 (55%) | British | (10) |
| Prefumo et
al, 2005 |
572 | 18/47
(38.3%) | – | – | British | (11) |
| Matias et
al, 1998 |
486 | 35/38
(92.1%) | 12/12
(100%) | 5/7
(71.4%) | Mixed | (12) |
| Hsiao et al,
2014 | 20,586 | 12/25
(48.0%) | – | – | Chinese,
Taiwanese | (13) |
| Murta et al,
2002 |
372 | 18/18
(100%) | 1/1
(100%) | 2/2
(100%) | Brazilian | (18) |
| Zoppi et al,
2002 |
325 | 14/20 (70%) | 6/7
(85.7) | 1/1
(100%) | Italian | (19) |
| Borrell et
al, 2003 |
3,382 | 36/48 (75%) | 17/24 (71%) | – | Spanish | (20) |
| Antolin et
al, 2001 |
924 | 5/7
(71.4%) | 3/3
(100%) | – | Spanish | (21) |
| Toyama et
al, 2004 |
1,097 | 5/7
(71.4) | 3/5
(60%) | 1/1
(100%) | Brazilian | (22) |
| Stressig et
al, 2011 |
3,648 | 5/35
(14.3%) | – | – | German | (23) |
| Wagner et
al, 2016 |
4,641 | – | 32/40 (80%) | 8/13
(61.5%) | German | (24) |
Materials and methods
Study design
Pathway analysis was conducted to derive association
data from literature. Subsequently, Bayes' theorem-based
statistical analysis was performed to calculate the conditional
probabilities. The formulas based on Bayes' theorem describe how to
calculate the probability of an event, based on its association
with another event (14).
Additionally, a statistical analysis was performed based on
clinical data from 1,962 first-trimester pregnant women from
Western China.
Pathway analysis
Data regarding the associations between diseases and
genes, and among various diseases were obtained from the Pathway
Studio (www.pathwaystudio.com; version 12.0)
(15) generated by the
MedScan® text-mining tool (16). The Pathway Studio database contains
all abstracts from PubMed and millions of full-text articles from
journals belonging to Elsevier B.V. (Amsterdam, The
Netherlands).
Statistical estimation
Besides sensitivity and specificity, the present
study aimed to use Bayes' theorem to estimate the disease
predictive power and disease rejection power considering a
thickened NT, an abnormal DV or the two parameters combined.
Sensitivity using DV, NT or the two
parameters combined
The sensitivity using X to predict Y is described as
a conditional probability p(X/Y), which is calculated using Bayes'
theorem, (Equation i).
p(X/Y)=p(X/Y)/P(Y)
Where X = DV, NT or (DV||NT); Y = T21, T18, T13 and
T. Where (DV||NT) represents one of the combinations of DV or NT,
and T represents any of the three trisomies examined.
Specificity using DV/NT or the two
combined
The specificity of using X to predict Y is described
by the conditional probability (Equation ii).
p(X¯/Y¯)=p(X¯/Y¯)/P(Y¯)
Where X¯=DV¯,NT¯or(NT&DV¯);Y¯=T21¯,T18¯,T13¯orT¯.
Predictive power using DV/NT or the
two combined
According to Bayes' theory, the predictive power of
using X to predict Y is calculated with Equation iii. The
predictive power defines the probability of Y considering that X
occurred.
p(Y/X)=p(XY)/P(X)
Where X = DV, NT, DV&NT and DV¯&NV¯; Y = T21, T18, T13 and T. The
predictive power is associated with the reliability of using X as
an indicator for the prediction of Y.
Rejection power using DV/NT or the two
combined
The rejection power of using X to predict Y is
expressed as a conditional probability (Equation iv), which
indicates the probability of Y based on the fact that X did not
occur.
p(Y/X¯)=p(X¯Y)/P(X¯)
Where X¯=DV¯,NT¯and(DV¯&NT¯); Y = T21, T18,
T13 and T. The conditional probability p(Y/X) is negatively
associated with the rejection power. A high rejection power
indicates high reliability of using X as an indicator for the
prediction of Y.
Clinical data
A total of 2,098 pregnant women were recruited for
the present study. The data obtained were categorized into two
groups (N1 = 960 and N2 =
1,138). In the first group, NT thickness and DV blood flow were
examined. In the second group, only NT thickness was measured. The
inclusion criteria were: Single pregnancy, early fetal NT
examination, 11–13 weeks pregnancy and fetal crown-rump length
(CRL): 45–84 mm. Patients were recruited between January 2010 and
December 2014 in The West China Women and Children Hospital
Affiliated to Sichuan University (Chengdu, China). The exclusion
criteria were: Severe organ dysfunction, lack of follow-up, fetal
chromosomal abnormalities other than the three trisomies examined
in the present study, severe fetal abnormalities and miscarriage.
The present study was approved by The Ethics Committee of Sichuan
University. Informed consent was signed by all patients. Following
removal of the patients meeting the exclusion criteria, the first
group consisted of 903 patients and the second group consisted of
1,059 patients.
NT and DV data acquisition
For the two groups, the morphology of the fetus in
the first trimester was analyzed and NT was measured. The
ultrasonography test was performed by four physicians in the
hospital. Ultrasound examination was performed in 10 min. The
frequency of the probe was 3.5–5.0 MHz. The ultrasound machines
used were: Voluson 730 (GE Healthcare, Chicago, IL, USA), Sequoia
512 (Siemens AG, Munich, Germany) and IU22 (Philips Healthcare,
Andover, MA, USA). The thermal index was <0.8 and the mechanical
index was <0.77. Routine fetal examinations (including number of
fetuses, CRL, placenta and amniotic fluid) were conducted to
confirm the gestational age. The ultrasound results were recorded
prior to NT measurement. NT measurements were performed according
to The Fetal Medicine Foundation system (17). NT was considered abnormal when the
NT was ≥3 mm or when fetal cystic hygroma was detected.
The DV waveforms were measured in the first group
(N1 = 960), and the NT was additionally measured.
The DV blood flow was directed into the atrium and the flow
velocity detected was higher compared with the peripheral vein
blood flow. The sampling frame of 2 mm was placed at the beginning
of the catheter. The sound beam and blood flow direction were close
to 0°, using a Doppler correction angle <60°. Doppler velocity
curve of the venous pulse was examined when the fetus was in
resting state. The average velocity during five cardiac cycles was
automatically calculated and recorded by the built-in software of
the instrument. The total time of detection of the DV was <3
min. In the case of normal DV flow, all waves indicated the forward
direction of blood flow (Fig. 1A).
These waves include the ventricular contraction wave, the
ventricular diastolic and the atrial contraction wave (A wave). DV
blood flow was considered abnormal when the absence or the reversal
of the A-waves were detected (Fig.
1B).
Other examinations and follow-up
Pregnant women exhibiting the following fetal
chromosomal abnormality risk factors: Thickened NT, >35 years
old, serological abnormalities, adverse reproductive history,
adverse pregnancy exposure history and family history of genetic
disease, were recommended to undergo a karyotype test following
amniocentesis or cordocentesis. A follow-up study was conducted by
a team composed of an obstetrician, a pediatrician and
ultrasonologists, with the aim to analyze the results of the
karyotype test, neonatal examination and, in case of miscarriage,
examination of the fetus following labor induction. Communication
by telephone, face-to-face interviews and hospital records were
used to conduct the follow-up study.
Results
Pathway analysis
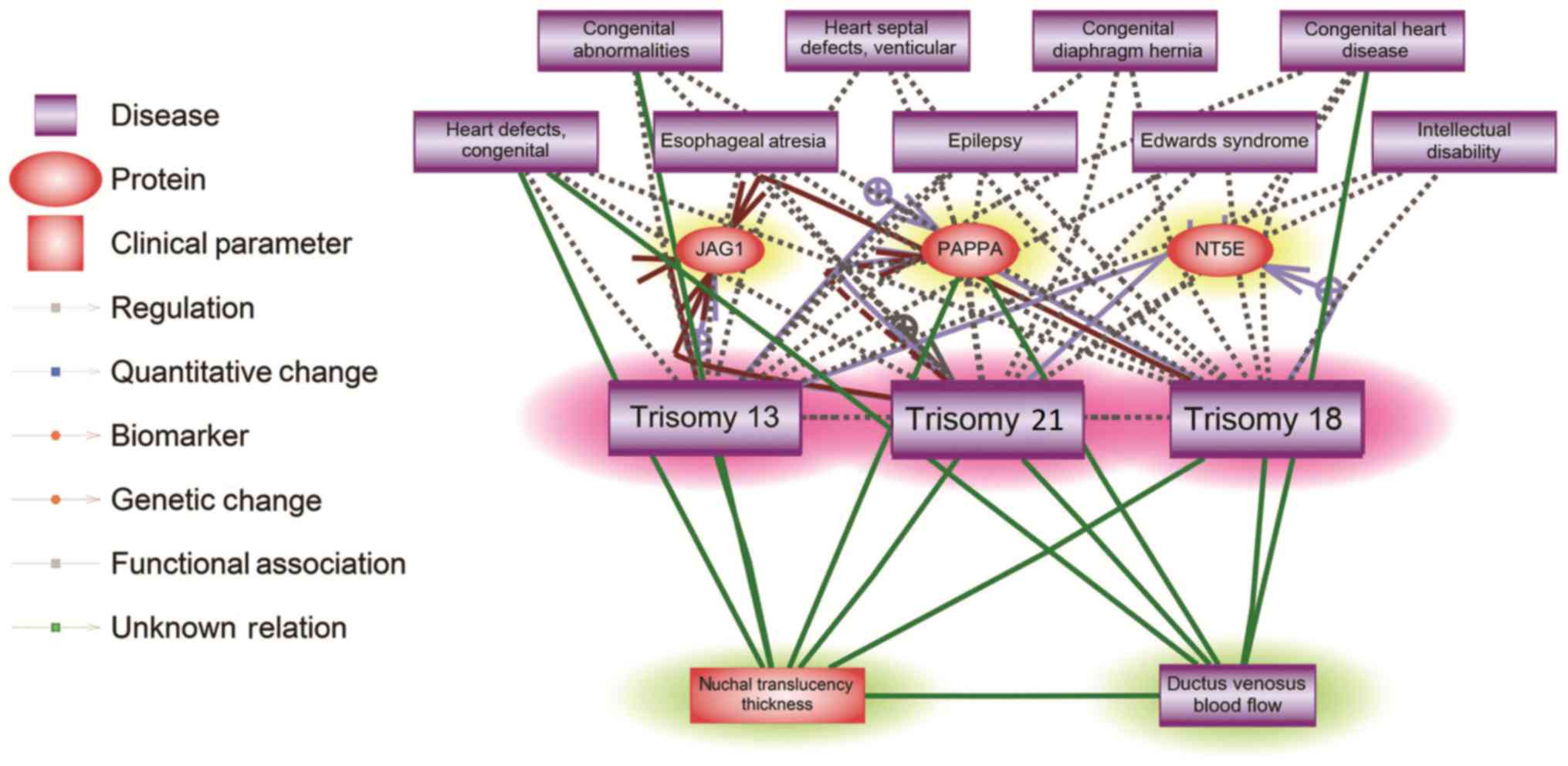
The pathway analysis suggested that three genes,
jagged 1, pappalysin 1 (PAPPA) and 5′-nucleotidase ecto, and nine
diseases were associated with all three trisomies (T21, T18 and
T13). Furthermore, certain genes and diseases identified were
associated with NT and DV (Fig.
2). Specifically, NT and DV were associated with congenital
heart defects and with PAPPA. The present results suggested that NT
and DV are associated with all three trisomies, which suggested the
possibility of using NT with DV as a clinical indicator for the
diagnosis of T21, T18 and T13.
Statistical analysis
Mathematical statistical analysis using Bayes'
theorem suggested that combining DV and NT may lead to increased
specificity and sensitivity. However, to improve the prediction and
rejection power using the combination of DV and NT, certain
conditions are required, which were described above in the
‘Prediction power’ and ‘Rejection power’ sections.
X1 was selected to indicate the occurrence of
abnormal NT, and X2 to indicate the occurrence of
abnormal DV. Y indicates the occurrence of any trisomy among T13,
T18 and T21.
Improved sensitivity
As p((NT||DV)&Y) ≥
p(NT&Y), i.e.,
p((X1||X2)&Y)
≥ p(X2&Y), subsequently,
p((X1||X2)/Y)=p(X1||X2&Y)P(Y)≥p(X2Y)P(Y)p(X2/Y)
Where
p((X1||X2)/Y)
refers to the sensitivity of using NT and DV to
predict Y (e.g., when one of the conditions of NT or DV occurs, Y
occurs); p(X2/Y) refers to the
sensitivity of using NT alone to predict Y. Equation v
suggested that combining NT with DV may lead to an improved
sensitivity in predicting the occurrence of trisomies.
Improved specificity
As p(NT&DV¯&Y¯)≥p(NT&Y¯), i.e.,
p(X1&X2¯/Y¯)≥p(X¯2&Y¯),
subsequently,
p(X1&X2¯)/Y¯)=p(X1&X2¯Y¯)P(Y¯)≥p(X2¯Y¯)P(Y¯)=p(X2¯/Y¯)
Where p(X1¯&X¯2/Y¯) is the specificity of
using NT with DV to predict Y; p(X¯2/Y¯) is the specificity for using
NT alone to predict Y. Equation vi suggested that,
theoretically, combining NT and DV may lead to an improved
specificity in predicting the occurrence of trisomies.
Prediction and rejection power
The prediction probability
p(Y/X1) describes the probability
of Y based on the fact that X1 occurs. The
rejection probability p(Y/X¯1)
describes the probability of Y based on the fact that
X1 does not occur. In order to improve the
reliability of the diagnosis, increased predictive power and
decreased rejection probability are required. If p(Y/X1X¯2)<p(Y/X1X2), using
X1 with X2 can lead to improved
predictive power and rejection power compared with
X1 alone. However, clinical data are required to
estimate and test the conditional probabilities derived by Bayes'
theorem.
Clinical results
The occurrence of each trisomy in different cases
are presented in Table II. The
first group was composed of 903 subjects. Among these subjects, 58
presented DV abnormality, 63 exhibited thickened NT, and 44
presented abnormal DV and thickened NT, concomitantly. The second
group was composed of 1,059 patients. A total of 84 patients
exhibited thickened NT. The statistical analyses associated with DV
were performed considering data from the first group. Regarding NT,
data from the two groups were considered. The results of the
statistical analyses performed are presented in Table III. Collectively, the
sensitivity, specificity and the predictive power were calculated,
considering DV alone, NT alone or combining DV and NT.
| Table II.A total of 41 cases of trisomies from
the two groups of 1,962 participants. |
Table II.
A total of 41 cases of trisomies from
the two groups of 1,962 participants.
|
| Group 1
(N1 = 903) | Group 2
(N2 = 1,059) |
|
|---|
|
|
|
|
|
|---|
| T | DV&NT | DV&NT¯ | DV¯&NT¯ | NT | NT¯ | Total |
|---|
| T21 | 10 | 1 | 2 | 13 | 4 | 30 |
| T18 | 3 | 1 | – | 3 | – | 7 |
| T13 | 2 | – | – | 2 | – | 4 |
| Any | 15 | 2 | 2 | 18 | 4 | 41 |
| Table III.Probabilities calculated using the
two datasets. |
Table III.
Probabilities calculated using the
two datasets.
| Statistics
values | Cases | T21, % | T18, % | T13, % | Any T, % |
|---|
| Sensitivity | p (DV/T) | 84.62 | 100.00 | 100.00 | 89.47 |
|
| p (NT/T) | 76.67 | 85.71 | 100.00 | 80.49 |
|
| p
((NT&DV)/T) | 84.62 | 100.00 | 100.00 | 89.47 |
| Specificity | p (DV¯/T¯) | 94.81 | 93.91 | 93.77 | 95.35 |
|
| p
(NT/T) | 93.58 | 92.79 | 92.7 | 94.07 |
|
| p ((NT&DV¯)/T¯) | 96.27 | 95.36 | 95.32 | 96.71 |
| Predictive
Power | p (T/DV) | 18.97 | 6.90 | 3.45 | 29.31 |
|
| p (T/NT) | 15.65 | 4.08 | 2.72 | 22.45 |
|
| p
(T/(NT&DV)) | 22.73 | 6.82 | 4.56 | 34.09 |
| Rejection
Power | p (T/DV¯) | 0.332 | 0 | 0 | 0.22 |
|
| p
(T/NT) | 0.386 | 0.055 | 0 | 0.44 |
|
| p (T/(NT¯&DV¯)) | 0.27 | 0 | 0 | 0.21 |
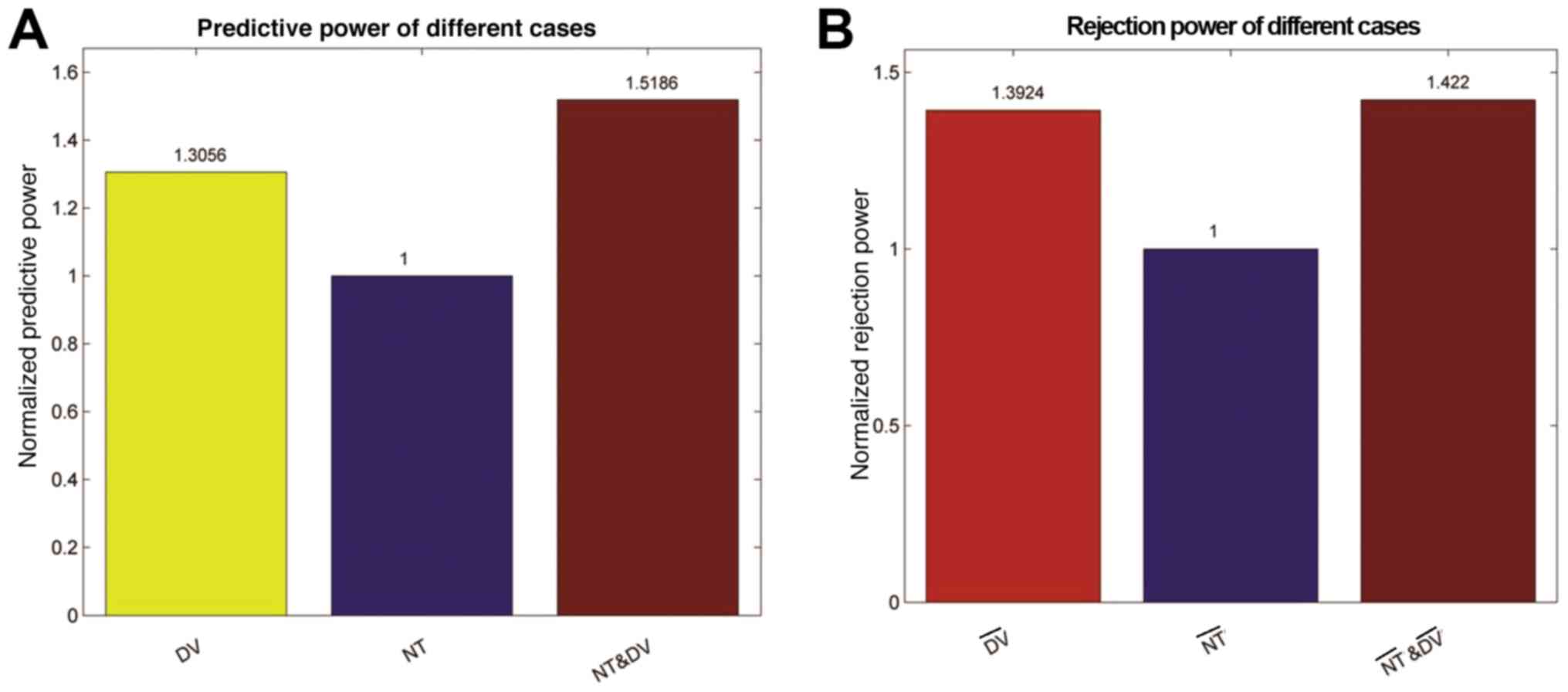
The results presented in Table III suggested that, in order to
predict the occurrence of trisomies, combining DV and NT resulted
in increased sensitivity and specificity compared with one
indicator alone. Accordingly, combining the two indicators
increased the predictive power by over 50%, and the rejection power
increased by over 40%, as presented in Fig. 3.
Discussion
While NT has been well accepted as prospective
screening indicator of chromosomal abnormalities, recently, DV wave
form has also been suggested as an additional clinical maker for
the early trisomy diagnosis (18).
However, previous studies considering various populations led to
contrasting results, and the number of previous studies analyzing
the Chinese population is limited (3–7,10–13).
The present study investigated the reliability of combining DV and
NT for the early diagnosis of the three most common trisomies in
Western China: T21, T18 and T13. The analyses performed were based
on: Investigation of previous literature, theoretical statistical
analysis and analysis of clinical data.
The pathway analysis suggested that DV and NT were
associated with multiple risk factors, including diseases and gene
dysregulations that were associated with the three trisomies, as
shown in Fig. 2. Note that for
each relation (edge) presented in Fig.
2, there were one or more supporting references. In total,
there were about 825 references supporting the relationships
presented in Fig. 2 (please see
‘Additional data’ available at http://figshare.com/s/8a2728cf0d42502eece4). In
addition to the directly reported relationships (19,20),
other evidences were also presented in the pathway (Fig. 2) in favor of the rationality of
using both NT and DV for the detection of chromosomal
abnormalities. Previous studies suggested that NT thickness, DV
abnormalities and the expression levels of PAPP-A may be considered
in the diagnosis of chromosomal abnormalities to increase the
detection rate and decrease the rate of false positives (21,22).
Both NT screening and DV have been suggested in the detection of
congenital heart defects (21). On
the other hand, fetal heart diseases have been strongly associated
with T21 (22), T18 and T13
(23). That both NT and DV were
clinical markers for trisomy-related diseases (e.g., congenital
heart defects) (18,24,25)
may partially explain the rationality of using NT and DV as
clinical markers for the early diagnosis of all three trisomies.
Mathematical statistical analyses suggested that combining NT with
DV may improve the prediction sensitivity and specificity in the
diagnosis of trisomies. Furthermore, for the purpose of diagnosis,
the predictive power and rejection power are important factors to
consider. The predictive power describes the occurrence probability
of a trisomy when at least one risk factor was detected. The
rejection power represents the occurrence probability of any
trisomy when no risk factors were detected. In order to make an
accurate diagnosis, it is important to increase the prediction
probability and decrease the rejection probability. Unlike
sensitivity and specificity, the analysis of predictive power and
rejection power requires validation using clinical data.
Clinical data from 1,962 Western Chinese patients
were used to calculate sensitivity, specificity, and prediction and
rejection probabilities. The present results suggested that the
combination of NT and DV led to improved sensitivity and
specificity. Specifically, when abnormal NT and DV were observed
concomitantly, the occurrence probability of any trisomy increased,
compared with NT alone (34.09% vs. 22.45%). In case of normal NT
and DV the occurrence probability was decreased by over 50% (0.205%
vs. 0.441%). Additionally, when only NT or DV presented
abnormalities, the occurrence probability of trisomy was 0.80% in
the case of thickened NT alone and 14.29% in the case of abnormal
DV alone (Table III).
Furthermore, compared with NT or DV alone, combining NT and DV
resulted in increased predictive power and rejection power.
Additional statistical parameters were estimated,
including overall abnormal DV rate (6.4%), overall abnormal NT rate
(7.49%) and concomitant abnormal DV and NT rate (4.87%). Notably,
abnormal NT alone led to various occurrence rates of T21, T18 and
T13 (76.67, 85.71 and 100%, respectively). The present estimated
values are consistent with previous studies (8,10,22).
Additionally, the clinical results suggested that fetuses with
abnormal DV presented a significant thicker NT (3.9 mm) compared
with fetuses with normal DV (1.4 mm), consistent with the
hypothesis that abnormal DV is associated with thickened NT
(3). Notably, the differences
observed may be specific of the population of patients considered;
the present study only analyzed Western Chinese women. In the
present study, the sensitivity of T21 prediction using only DV
(~84.6%) was different from the previous study of Hsiao et
al (13) (~48.0%), where a
Southern Chinese population was considered. In addition to the
association between T21 and abnormal DV, the possibility of using
abnormal DV to predict the occurrence of T18 and T13 was examined.
This possibility was not investigated by previous studies analyzing
the Chinese population, to the best of the authors' knowledge.
Therefore, the present study may provide novel statistical analyses
to the field of prenatal diagnosis in the Western Chinese
population.
Although combining NT and DV may significantly
increase the predictive power, the prediction probability remains
insufficient (34.09%). Therefore, besides NT and DV, other factors
may exist that influence the occurrence of trisomy-associated
diseases. In the present study, normal NT (and normal DV for group
one) were detected for two fetuses with aneuploidy from group one
and five fetuses from group two. In case of normal NT and DV, the
aneuploidy may be due to the advanced reproductive age or
serological abnormalities of the mother, as recorded in the
clinical data. Therefore, further studies analyzing a number of
clinical datasets are required in order to identify additional
clinical parameters, besides NT and DV, that may be associated with
the occurrence of chromosomal aneuploidy.
The present study is based on a multi-level
analysis, and suggested that, without conducting further screening
and thus increasing the cost of the analysis, combining DV and NT
may increase the predictive power in identifying trisomies (T21,
T18 and T13), leading to an improvement in prenatal diagnoses. The
present results may provide insight into the field of prenatal
diagnosis of chromosome abnormalities in the Western Chinese
population.
Acknowledgements
The authors would like to thank Ms. Lydia Manor
from Children's National Health Hospital for providing the Pathway
Studio association data analysis.
Funding
The present study was supported by The Science and
Technology Bureau of Chengdu, The Huimin Technology R&D Project
(grant no. 2014-HM01-00049-SF; China) and The Science and
Technology Department of Sichuan Province, The Application of Basic
Science Project (grant no. 2017JY0263; China).
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request. The additional data generated during the current study are
available in the Figshare repository (https://figshare.com/s/8a2728cf0d42502eece4).
Authors' contributions
YT and HL contributed to the data collection and
data analysis. YT, HL, DM and GL contributed the study design and
manuscript development. TY, QZ and FY contributed to the clinical
data collection and manuscript development.
Ethics approval and consent to
participate
The present study was approved by The Ethics
Committee of Sichuan University (Chengdu, China). Informed written
consent was obtained from all individual participants included in
the present study.
Patient consent for publication
All patients provided consent for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mavrides E, Moscoso G, Carvalho JS,
Campbell S and Thila-ganathan B: The human ductus venosus between
13 and 17 weeks of gestation: Histological and morphometric
studies. Ultrasound Obstet Gynecol. 19:39–46. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kiserud T, Eik-Nes S, Blass HG and
Hellevik LR: Ultrasonographic velocimetry of the fetal ductus
venosus. Lancet. 338:1412–1414. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hyett JA, Brizot ML, Von Kaisenberg C,
Mckie AT, Farzanah F and Nicolaides KH: Cardiac gene expression of
atrial natriuretic factorand brain natriuretic peptide in trisomic
fetuses. Obstet Gynecol. 87:506–510. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Della Ragione F, Mastrovito P, Campanile
C, Conti A, Papageorgiou EA, Hultén MA, Patsalis PC, Carter NP and
D'Esposito M: Differential DNA methylation as a tool for
noninvasive prenatal diagnosis (NIPD) of X chromosome aneuploidies.
J Mol Diagn. 12:797–807. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Syngelaki A, Guerra L, Ceccacci I, Efeturk
T and Nicolaides KH: Impact of holoprosencephaly, exomphalos,
megacystis and high NTT in first trimester screening for
chromosomal abnormalities. Ultrasound Obstet Gynecol. 50:45–48.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vinkesteijn AS, Ursem NT, Struijk PC and
Wladimiroff JW: Fetal heart rate and blood flow velocity
variability in the presence of increased nuchal translucency: A
preliminary study. Ultrasound Obstet Gynecol. 23:19–22. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Witters I and Fryns JR: Fetal nuchal
translucency thickness. Genet Couns. 18:1–7. 2007.PubMed/NCBI
|
|
8
|
Maiz N and Nicolaides KH: Ductus venosus
in the first trimester: Contribution to screening of chromosomal,
cardiac defects and monochorionic twin complications. Fetal Diagn
Ther. 28:65–71. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Martínez JM, Comas M, Borrell A, Bennasar
M, Gómez O, Puerto B and Gratacós E: Abnormal first-trimester
ductus venosus blood flow: A marker of cardiac defects in fetuses
with normal karyotype and nuchal translucency. Ultrasound Obstet
Gynecol. 35:267–272. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Maiz N, Valencia C, Kagan KO, Wright D and
Nicolaides KH: Ductus venosus Doppler in screening for trisomies
21, 18 and 13 and Turner syndrome at 11–13 weeks of gestation.
Ultrasound Obstet Gynecol. 33:512–517. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Prefumo F, Sethna F, Sairam S, Bhide A and
Thilaganathan B: First-trimester ductus venosus, nasal bones, and
down syndrome in a high-risk population. Obstet Gynecol.
105:1348–1354. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Matias A, Gomes C, Flack N, Montenegro N
and Nicolaides KH: Screening for chromosomal abnormalities at 10–14
weeks: The role of ductus venosus blood flow. Ultrasound Obstet
Gynecol. 12:380–384. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hsiao CH, Cheng PJ, Shaw SW, Hsu JJ, Chen
RC, Tseng YJ and Chu WC: Extended first-trimester screening using
multiple sonographic markers and maternal serum biochemistry: A
five-year prospective study. Fetal Diagn Ther. 35:296–301. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jagielski J and Skawiński W: The analysis
and classification of chromosomes. I. Application of the Bayes'
theorem. Mater Med Pol. 10:198–203. 1978.PubMed/NCBI
|
|
15
|
Nikitin A, Egorov S, Daraselia N and Mazo
I: Pathway studio-the analysis and navigation of molecular
networks. Bioinformatics. 19:2155–2157. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Novichkova S, Egorov S and Daraselia N:
MedScan, a natural language processing engine for MEDLINE
abstracts. Bioinformatics. 19:1699–1706. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Harris LH: Rethinking maternal-fetal
conflict: Gender and equality in perinatal ethics. Obstet Gynecol.
96:786–791. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Murta CG, Moron AF, Avila MA and Weiner
CP: Application of ductus venosus Doppler velocimetry for the
detection of fetal aneuploidyin the first trimester of pregnancy.
Fetal Diagn Ther. 17:308–314. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zoppi MA, Putzolu M, Ibba RM, Floris M and
Monni G: First-trimester ductus venosus velocimetry in relation to
nuchal translucency thickness and fetal karyotype. Fetal Diagn
Ther. 17:52–57. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Borrell A, Martinez JM, Seres A, Borobio
V, Cararach V and Fortuny A: Ductus venosus assessment at the time
of nuchal translucency measurement in the detection of fetal
aneuploidy. Prenat Diagn. 23:921–926. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Antolin E, Comas C, Torrents M, Muñoz A,
Figueras F, Echevarria M, Cararach M and Carrera JM: The role of
ductus venosus bloodflow assessment in screening for chromosomal
abnormalities at 10–16 weeks of gestation. Ultrasound Obstet
Gynecol. 17:295–300. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Toyama JM, Brizot ML, Liao AW, Lopes LM,
Nomura RM, Saldanha FA and Zugaib M: Ductus venosus blood flow
assessment at 11 to 14 weeks of gestation and fetal outcome.
Ultrasound Obstet Gynecol. 23:341–345. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Stressig R, Kozlowski P, Froehlich S,
Siegmann HJ, Hammer R, Blumenstock G and Kagan KO: Assessment of
the ductus venosus, tricuspid blood flow and the nasal bone in
second-trimester screening for trisomy 21. Ultrasound Obstet
Gynecol. 37:444–449. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wagner P, Sonek J, Hoopmann M, Abele H and
Kagan KO: First-trimester screening for trisomies 18 and 13,
triploidy and Turner syndrome by detailed early anomaly scan.
Ultrasound Obstet Gynecol. 48:446–451. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Abdelmoez A, Coraça-Huber DC, Thurner GC,
Debbage P, Lukas P, Skvortsov S and Skvortsova II: Screening and
identification of molecular targets for cancer therapy. Cancer
Lett. 387:3–9. 2017. View Article : Google Scholar : PubMed/NCBI
|