Introduction
Thyroid hormone resistance syndrome (RTH) is a
disease characterized by a low response to thyroid hormone in
target tissues, which may be caused by a thyroid hormone receptor
(THR) gene mutation. RTH is a rare disease with an incidence of ~1
in 40,000 (1). This disease has a
genetic predisposition, however, a few cases are sporadic (2); sporadic cases are more common in
children and adolescents. The clinical features of RTH are diverse
and are manifested in a number of ways, including hyperthyroidism,
hypothyroidism or non-toxic goiter. However, significantly elevated
blood thyroid hormone is a common clinical feature (3).
According to the different subtypes of mutant
receptors, RTH is classified into thyroid hormone receptor α (THRα)
gene mutation-induced RTH (RTHα) and thyroid hormone receptor β
(THRβ) gene mutation-induced RTH (RTHβ) (4). In total, 85% of RTH cases are caused
by mutations in the THRβ gene (2,5). RTH
is an autosomal dominant heredity disease, with recessive heredity
being less common (6). Gene
sequencing is the gold standard for diagnosing RTH. The present
study identified a rare mutation (p. I275T) in the THRβ gene in a
patient with RTH. This is a novel gene mutation site and, to the
best of our knowledge, there have been no reports of this mutation
before.
Case report
The Ethics Committee of The First Hospital of
Lanzhou University approved the present work. Informed written
consent was obtained from the patient for publication of this case
report and the accompanying images.
The proband (II:1), a Chinese boy of four years and
eight months, visited the hospital due to growth retardation. The
parents of the proband said that their son was born 2 weeks
prematurely by a caesarean section. At 18 months of age, the
proband was often dull and his height was 3–4 cm shorter than his
peers. He was treated at a local hospital. There is no relevant
medical history in the family. The previous medical records of the
proband showed that his nutrition and skin condition was good, that
he had no eye symptoms, his intelligence quotient (IQ) was normal,
that his height and weight were lower than his peers (related data
is shown in Table I), his thyroid
was not large, and his thyroid function showed elevated levels of
thyroid hormone and thyroid stimulating hormone (TSH). A physician
prescribed levothyroxine sodium tablets for the proband. The
proband had visited the doctor many times and the dose of the drug
had been adjusted, however, the thyroid function did not recover
(thyroid function and therapy process are shown in Table II). At present, the proband is
prescribed with oral levothyroxine sodium tablets at a dose of 100
µg/day. The family tree of the proband and his parents are shown in
Fig. 1. Among the two generations,
only the proband had thyroid dysfunction and his parents had no
relevant medical history.
 | Table I.Height and weight of the proband. |
Table I.
Height and weight of the proband.
|
| Age, years |
|---|
|
|
|
|---|
| Variable | 2 | 2.5 | 3 | 3.5 | 4 | 4.5 |
|---|
| Height, cm | 77.2 | 80.1 | 86.3 | 90.5 | 95.2 | 99.6 |
| Weight, kg | 9.5 | 10.8 | 11.9 | 12.5 | 15.0 | 19.4 |
| Table II.Thyroid function and treatment program
for the proband. |
Table II.
Thyroid function and treatment program
for the proband.
|
| Thyroid function |
|
|---|
|
|
|
|
|---|
| Date | FT3 (3.1–6.8
pmol/l) | FT4 (9.8–22
pmol/l) | TSH (0.31–5.3
mIU/l) | Treatment program
(Levothy-roxine, µg/day) |
|---|
| 12/22/2015 | 6.85 | 14.10 | >150 | 25.0 |
| 01/22/2016 | 5.97 | 12.63 | >150 | 37.5 |
| 03/22/2016 | 5.93 | 18.77 | >150 | 50.0 |
| 07/19/2016 | 4.63 | 13.52 | >150 | 50.0 |
| 10/05/2016 | 6.56 | 18.31 | >100 | 62.5 |
| 11/12/2016 | 7.78 | 26.40 | 25.72 | 75.0 |
| 12/26/2016 | 9.22 | 36.94 | 0.90 | 87.5 |
| 04/24/2017 | 7.63 | 25.59 | 6.64 | 87.5 |
| 06/17/2017 | 9.16 | 29.31 | 6.82 | 87.5 |
| 04/02/2018 | 9.07 | 39.08 | 7.20 | 100.0 |
| 07/30/2018 | 7.90 | 36.80 | 9.44 | 100.0 |
| 08/11/2018 | 7.84 | 32.8 | 35.06 | 100.0 |
Comprehensive examinations of proband and his
parents were performed. Information about the age, height and
weight, and heart rate of the proband and his parents is shown in
Table III. The proband was
shorter than his peers, however, other measurements for the proband
were within the normal range. The thyroid function of the parents
of the proband are shown in Table
IV. The free triiodothyronine (FT3), free thyroxine (FT4) and
TSH levels in the proband were higher than normal, while the
thyroid function of his parents were normal. Peripheral blood
examinations showed the following: Platelets, 348×109/l
in routine blood tests (reference value, 100–300); trace element
results, Zn 4.95 mg/l (reference value, 57.5–78), Ca 56.6 mg/l
(reference value, 57.5–78), Fe 327 mg/l (reference value, 301–530),
Mg 30.1 mg/l (reference value, 27–46), Pb 45.6 µg/l (reference
value, 0–100), Cu 0.85 mg/l (reference value, 0.64–1.4); growth
hormone 0.23 ng/ml (reference value, <3.0); insulin-like growth
factor-1,151.00 ng/ml (reference value, 51–303); vitamin D 13.21
ng/ml (reference value, 30–60); intact parathyroid hormone 28.00
pg/ml (reference value, 16–87); bone alkaline phosphatase 210 U/l
(reference value, 0–200); N-MID BGP (N-MID bone Gla protein) 63.83
ng/ml (reference value, 9.74–39.47); ferritin 96.77 ng/ml
(reference value, 4.63–204), total cholesterol 4.11 mmol/l
(reference value, 3.6–5.7), triglycerides 0.94 mmol/l (reference
value, 0.8–1.8), creatine kinase 85 U/l (reference value, 38–240).
The wrist anterior segment (Fig.
2) suggested that the bone age was less than the actual age.
Thyroid color ultrasound examination showed normal. The thyroid
iodine uptake was 10.2% at 2 h (reference value, 5–15%), 19.2% at 6
h (reference value, 15–25%), 31.8% at 24 h (reference value,
25–40%). The basal metabolic rate was 219 KJ/h. Pituitary nuclear
magnetic imaging plain scan tips showed that the pituitary
morphology was normal. The proband also had a normal
electrocardiogram.
| Table III.Information about the proband and his
parents. |
Table III.
Information about the proband and his
parents.
| Proband/patient | Sex | Age, years | Height, cm | Weight, kg | Heart rate
(beats/min) |
|---|
| I:1 | M | 22 | 170 | 67 | 72 |
| I:2 | F | 22 | 168 | 66 | 78 |
| II:1 | M | 4 | 100 | 20 | 99 |
| Table IV.Thyroid function of the parents of the
proband. |
Table IV.
Thyroid function of the parents of the
proband.
| Date | Parent | FT3 (3.1–6.8
pmol/l) | TT3 (1.14–3.02
nmol/l) | FT4 (9.8–22
pmol/l) | TT4 (75.45–148.18
nmol/l) | TSH (0.31–5.3
mIU/l) |
|---|
| 03/22/2016 | I:1 | 5.91 | 2.91 | 16.93 | 142.01 | 1.58 |
|
| I:2 | 4.83 | 2.87 | 15.72 | 112.40 | 0.83 |
| 08/11/2018 | I:1 | – | 2.89 | – | 145.06 | 1.46 |
|
| I:2 | – | 2.81 | – | 105.97 | 0.72 |
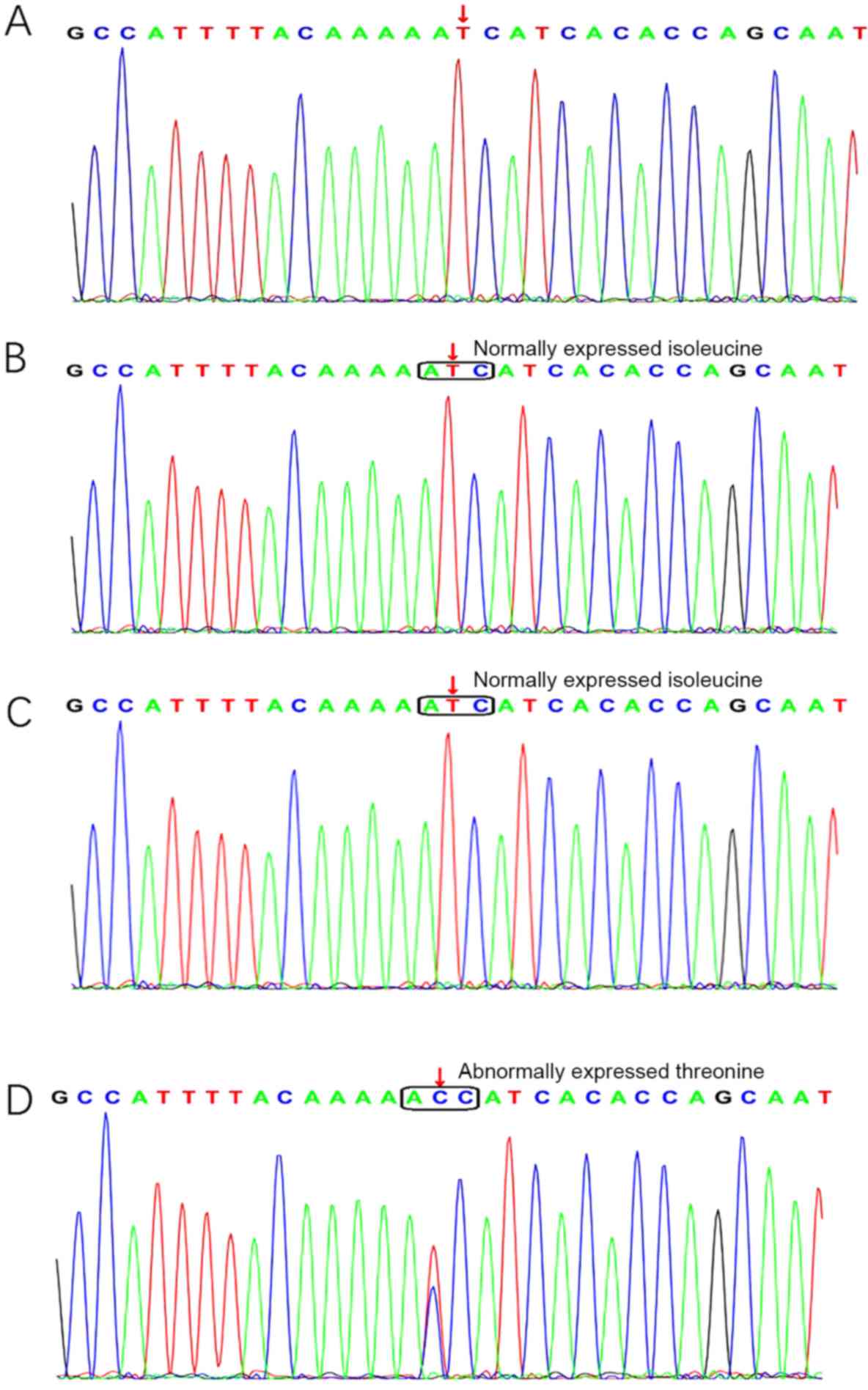
Gene sequencing suggested that the proband had a
point mutation in the 10th exon of the THRβ gene (c. 824 T>C). T
at position 824 of the THRβ gene coding sequence was replaced by C
(Fig. 3), resulting in the
replacement of isoleucine at position 275 with threonine (p.
I275T). This is a novel mutation and, to the best of our knowledge,
there have been no previous reports of this mutation. The parents
of the proband had T at this position, which is consistent with the
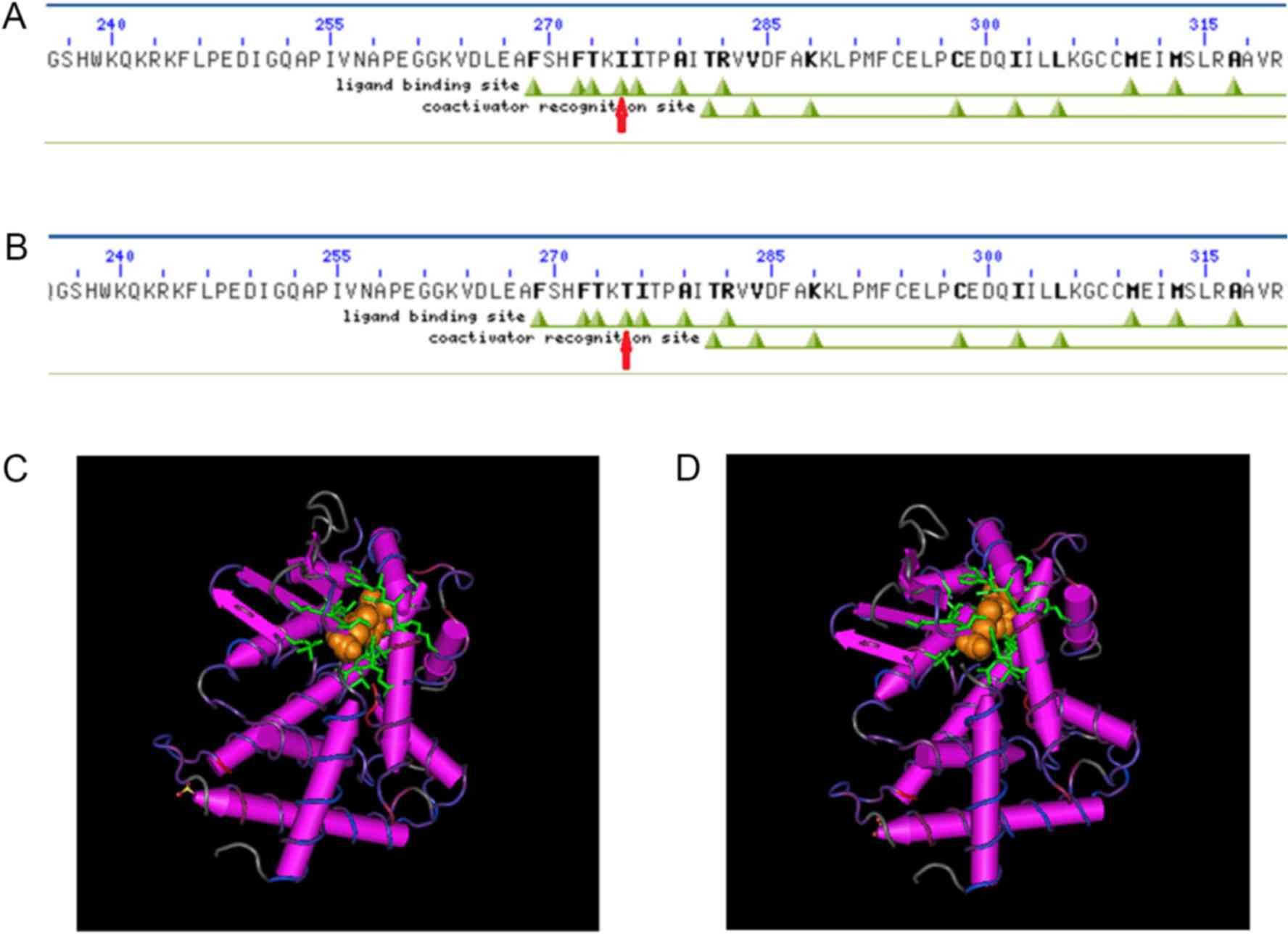
standard sequence. Computational mutation prediction was conducted
(Fig. 4). The crystal structure of
the THRβ-T3 complex was used as a reference wild-type structure.
The THRβ conserved domain was analyzed using the NCBI/Structure/Cdd
tool (https://www.ncbi.nlm.nih.gov/Structure/cdd/wrpsb.cgi).
The amino acid at position 275 is located just inside the ligand
binding site and the co-activation recognition site. The
sequence-based mutation prediction for I275T was found to be
damaging according to NCBI/Structure/Cdd.
Discussion
Refetoff and Dumitrescu (1) first reported a case of RTH in 1967.
It is thought that most cases of RTH are a result of autosomal
dominant or recessive hereditary with familial onset, however,
occasionally it is sporadic. RTH has no gender or ethnic
differences and can occur in all age groups (7). According to the onset and clinical
manifestations of RTH, the disease is divided into three
categories, global resistance (GRTH), pituitary resistance to
thyroid hormone (PRTH) and peripheral resistance to thyroid hormone
(PrRTH). In total, ~80% of patients with RTH belong to the GRTH
type, while PRTH is not common, and only a few cases of PrRTH have
been reported (8). The
pathogenesis of the disease is mainly through THR dysfunction
caused by mutations of the gene encoding THRβ. However, ~10% of
cases of RTH are due to other factors, including decreased number
of THR, absence of THR and unknown causes (9). RTH is associated with the THRβ locus
on chromosome 3 and THRβ gene mutations are considered to be the
most important cause of RTH (10,11).
In total, ~80% of RTH cases are caused by THRβ gene mutations,
however, such mutations are not found in 10–15% of cases (7,8,10).
The THRβ gene consists of 10 exons and 9 introns, encoding a
protein of 461 amino acids. Gene sequencing is the golden standard
for the diagnosis of RTH. To date, all THRβ mutations that have
been identified are located in three hotspot regions between exons
7 and 10 (234–282, 310–353 and 429–461) (12–18).
RTH has various clinical manifestations and is
difficult to diagnose, however, laboratory examinations identify
specific characteristics; thyroid hormone and TSH levels are
elevated during the course of the illness. The thyroid function of
the proband showed that FT3, FT4 and TSH levels were elevated
during the course of the illness. Even in the later period, FT3 and
FT4 were higher than normal after the proband was treated with a
high dose of levothyroxine tablets. Although TSH decreased, it did
not reach normal levels. The THR gene of the proband was sequenced.
The results of sequencing revealed a point mutation in the 10th
exon of the THRβ gene (c. 824 T>C). This variant site is located
within the three hotspot regions between exon 7 and 10. This point
mutation caused the amino acid isoleucine at position 275 to be
replaced with threonine (p. I275T). The physical and chemical
properties of these two amino acids are quite different. Isoleucine
is an aliphatic neutral amino acid, soluble in water and slightly
soluble in ethanol. However, the pH of threonine is 5.0–6.5, it is
soluble in water at high temperatures and insoluble in ethanol. In
the present study, NCBI/Structure/Cdd was used to analyze the
conserved domain of THRβ. The amino acid at position 275 is located
just inside the ligand binding site and the co-activation
recognition site. The sequence-based mutation prediction for I275T
showed that this change was probably damaging to the protein.
Therefore, it is hypothesized that the mutation site in the proband
interferes with the binding of THR to ligands. When isoleucine is
mutated to threonine at this site, the binding capacity of THR to
the ligand may be greatly reduced, resulting in symptoms of
RTH.
According to clinical features, laboratory
examination, gene sequencing and treatment, the proband was
diagnosed with RTH. The proband was treated with 100 µg of oral
levothyroxine sodium daily for 1 year and clinical symptoms were
gradually improved, however, TSH, FT3 and FT4 levels were still
elevated. As the present treatment is effective, drug therapy
continues. The current symptoms of the proband include slow growth
and development, along with other manifestations, such as reduced
activity and intelligence. It could be attributed to oral
administration of a high dose levothyroxine sodium tablets, so the
proband's growth retardation is improved compared to no treatment
and IQ score is normal. As the proband is a child, follow-up
treatment is important to promote growth, bone maturity and mental
development. Therefore, it is recommended that the parents and
physicians continue to observe the growth and mental development of
the proband.
In conclusion, RTH has no specific clinical
features, and may be associated with sinus tachycardia, goiter,
hyperactivity, growth retardation and other symptoms, which makes
diagnosing this disease difficult. Gene sequencing can improve
diagnosis. Therefore, genetic sequencing is recommended for initial
diagnosis and the appropriate treatment of patients with clinically
suspected RTH.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JW conceived the present study, participated in its
design, carried out the molecular genetic studies literature,
helped to draft the manuscript, and carried out and interpreted the
results of the molecular genetic tests. HL jointly conceived the
present study, participated in the coordination, helped to draft
the manuscript and contributed to the interpretation of the
results.
Ethics approval and consent to
participate
The Ethics Committee of The First Hospital of
Lanzhou University approved the present work.
Patient consent for publication
Written informed consent was obtained from the
patient's family for publication of this case report and the
accompanying images, and the use of data for both the patient and
the family.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
FT4
|
free thyroxine
|
|
FT3
|
free triiodothyronine
|
|
RTH
|
thyroid hormone resistance
syndrome
|
|
TSH
|
thyroid stimulating hormone
|
References
|
1
|
Refetoff S and Dumitrescu AM: Syndromes of
reduced sensitivity to thyroid hormone: Genetic defects in hormone
receptors, cell transporters and deiodination. Best Pract Res Clin
Endocrinol Metab. 21:277–305. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Refetoff S: Resistance to thyroid hormone:
One of several defects causing reduced sensitivity to thyroid
hormone. Nat Clin Pract Endocrinol Metab. 4:12008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Beck-Peccoz P and Chatterjee VK: The
variable clinical phenotype in thyroid hormone resistance syndrome.
Thyroid. 4:225–232. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Refetoff S, Bassett JH, Beck-Peccoz P,
Bernal J, Brent G, Chatterjee K, De Groot LJ, Dumitrescu AM,
Jameson JL, Kopp PA, et al: Classification and proposed
nomenclature for inherited defects of thyroid hormone action, cell
transport, and metabolism. J Clin Endocrinol Metab. 99:768–770.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reutrakul S, Sadow PM, Pannain S, Pohlenz
J, Carvalho GA, Macchia PE, Weiss RE and Refetoff S: Search for
abnormalities of nuclear corepressors, coactivators, and a
coregulator in families with resistance to thyroid hormone without
mutations in thyroid hormone receptor beta or alpha genes. J Clin
Endocrinol Metab. 85:3609–3617. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Massaad D, Poppe K, Lissens W and
Velkeniers B: A case of thyroid hormone resistance: Prospective
follow-up during pregnancy and obstetric outcome. Eur J Intern Med.
18:253–254. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hamon B, Hamon P, Bovier-Lapierre M,
Pugeat M, Savagner F, Rodien P and Orgiazz J: A child with
resistance to thyroid hormone without thyroid hormone receptor gene
mutation: A 20-year follow-up. Thyroid. 18:35–44. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Agrawal NK, Goyal R, Rastogi A, Naik D and
Singh SK: Thyroid hormone resistance. Postgrad Med J. 84:473–477.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu SY, Sadow PM, Refetoff S and Weiss RE:
Tissue responses to thyroid hormone in a kindred with resistance to
thyroid hormone harboring a commonly occurring mutation in the
thyroid hormone receptor beta gene (P453T). J Lab Clin Med.
146:85–94. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mamanasiri S, Yesil S, Dumitrescu AM, Liao
XH, Demir T, Weiss RE and Refetoff S: Mosaicism of a thyroid
hormone receptor-beta gene mutation in resistance to thyroid
hormone. J Clin Endocrinol Metab. 91:3471–3477. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nagaya T and Seo H: Molecular basis of
resistance to thyroid hormone (RTH). Endocr J. 45:709–718. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kim JH, Park TS, Baek HS, Kim GH, Yoo HW
and Park JH: A newly identified insertion mutation in the thyroid
hormone receptor-beta gene in a Korean family with generalized
thyroid hormone resistance. J Korean Med Sci. 22:560–563. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Refetoff S: Resistance to thyroid hormone
with and without receptor gene mutations. Ann Endocrinol (Paris).
64:23–25. 2003.PubMed/NCBI
|
|
14
|
Collingwood TN, Adams M, Tone Y and
Chatterjee VK: Spectrum of transcriptional, dimerization, and
dominant negative properties of twenty different mutant thyroid
hormone beta-receptors in thyroid hormone resistance syndrome. Mol
Endocrinol. 8:1262–1277. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gurnell M, Rajanayagam O, Agostini M,
Clifton-Bligh RJ, Wang T, Zelissen PM, van der Horst F, van de Wiel
A, Macchia E, Pinchera A, et al: Three novel mutations at serine
314 in the thyroid hormone beta receptor differentially impair
ligand binding in the syndrome of resistance to thyroid hormone.
Endocrinology. 140:5901–5906. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yen PM: Molecular basis of resistance to
thyroid hormone. Trends Endocrinol Metab. 14:327–333. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Parrilla R, Mixson AJ, McPherson JA,
McClaskey JH and Weintraub BD: Characterization of seven novel
mutations of the c-erbA beta gene in unrelated kindreds with
generalized thyroid hormone resistance. Evidence for two ‘hot spot’
regions of the ligand binding domain. J Clin Invest. 88:2123–2130.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Adams M, Matthews C, Collingwood TN, Tone
Y, Beck-Peccoz P and Chatterjee KK: Genetic analysis of 29 kindreds
with generalized and pituitary resistance to thyroid hormone.
Identification of thirteen novel mutations in the thyroid hormone
receptor beta gene. J Clin Invest. 94:506–515. 1994. View Article : Google Scholar : PubMed/NCBI
|