Introduction
Thalassemia is one of the most common monogenetic
diseases in Southern China, Southeast Asia and the Mediterranean
region (1). The frequency of
carriers in Guangxi, China is 26.9% for α-thalassemia (OMIM 604131)
(omim.org) and 19.9% for β-thalassemia (OMIM 603902)
(2). Thalassemia is a form of
hemolytic anemia caused by an imbalance in the rate of synthesis of
α- and β-globin peptide chains, due to mutation or deletion of the
human α- or β-globin gene (3). The
two most common types of thalassemia are α-thalassemia and
β-thalassemia (1). Genes
associated with α-thalassemia include hemoglobin α locus 2 (HBA2;
OMIM 141850) and HBA1 (OMIM 141800). β-thalassemia is associated
with the hemoglobin subunit β (HBB) gene (OMIM 141900) (4). Moreover, ~7% of the global population
is estimated to carry the genes associated with thalassemia and the
birth rate of children with hemoglobin disorders is >2.4% per
year (5). As thalassemia has no
effective treatment (6), prenatal
diagnosis is an important medical requirement for thalassemia
prevention strategies (7).
Amniocentesis and chorionic villus sampling are two commonly used
invasive prenatal diagnostic procedures. However, these traumatic
operations may cause injury to the fetus, miscarriage or
intrauterine infection (8).
Furthermore, anxiety associated with these invasive procedures has
been reported by numerous pregnant women (9). Therefore, non-invasive prenatal
diagnostic techniques for thalassemia detection are urgently
required.
Since the presence of cell-free fetal DNA (cffDNA)
in maternal plasma during pregnancy was first reported in 1997
(10), great efforts have been
made to use this source of fetal material for non-invasive prenatal
diagnosis (11). Non-invasive
prenatal testing (NIPT) has been established for the detection of
fetal chromosomal abnormalities, such as chromosome 21, 18 or 13
aneuploidy, in the plasma of pregnant women, and major variations
in copy number can be rapidly detected for clinical prenatal
screening and diagnosis (12,13).
In addition to NIPT for fetal aneuploidies, non-invasive testing
techniques for monogenic diseases are also being developed
(14). A challenge facing this
field is the need to target low concentrations of fetal mutations
that differ by only one or a few nucleotides from the overwhelming
background of maternal DNA in the mother's plasma (15,16).
At present, assessing the relative mutation dosage and the relative
haplotype dosage (RHDO) are the main analytical approaches used for
NIPT of monogenic diseases (17–20).
Early attempts to diagnose monogenic diseases focused on approaches
targeting paternally inherited fetal mutations absent from the
maternal genome. This strategy has proven to be successful for the
detection of achondroplasia (21),
myotonic dystrophy (22) and
Huntington's disease (23).
However, to assess fetal mutations in maternal plasma that share
the same genetic identity between the mother and the fetus, more
sophisticated strategies are required. These approaches have been
facilitated by technological advances, including massively parallel
sequencing (24) and digital PCR
(25), which enable the sensitive
and precise measurement of circulating plasma DNA. However, the
large target region used for these methods substantially increase
the cost of sequencing (26), a
factor which may impede their clinical application. Furthermore,
these methods have not yet been applied for the detection of large
deletion mutations.
In the present study, a technique was described for
non-invasive prenatal detection of paternal and maternal mutations
associated with α- and β-thalassemia using multiplex PCR or target
capture combined with next-generation sequencing (NGS).
Furthermore, the present study demonstrated the feasibility of
using NGS data to detect targeted copy number variations (CNVs) and
single nucleotide variations (SNVs) (3).
Materials and methods
Sample collection and DNA
extraction
A total of eight families were recruited at The
Third Affiliated Hospital of Sun Yatsen University. A total of 24
samples of peripheral blood (~10 ml per sample) of known
thalassemia genotypes were collected. There were 13 female and 11
male patients with thalassemia, with an age range of 2–38 years
(mean age, 15 years). The maternal plasma of pregnant women was
collected at an average gestation period of 20 weeks for
non-invasive prenatal diagnostic assays. A total of ~10 ml amniotic
fluid was also collected for direct molecular diagnosis. In
addition, ~5 ml peripheral blood from the parents and their first
child was collected into EDTA tubes. For each sample, genomic DNA
(gDNA) was extracted using the DNeasy Blood and Tissue kit (Qiagen
Sciences, Inc.). genomic DNA was extracted using the DNeasy Blood
and Tissue kit (Qiagen Sciences, Inc.), according to the
manufacturer's instructions.
Moreover, ~2 ml plasma was separated in two steps
from each sample obtained from a pregnant woman. First, 5 ml
peripheral blood from the pregnant women was centrifuged at 1,600 ×
g for 15 min at 4°C. Subsequently, ~2 ml supernatant was
centrifuged at 16,000 × g for 10 min at 4°C. The plasma cffDNA was
extracted using the QIAamp Circulating Nucleic Acid kit (Qiagen
Sciences, Inc.), according to the manufacturer's instructions.,
then quantified using a Qubit® fluorometer (Thermo
Fisher Scientific, Inc.) and stored at −20°C until further use.
Molecular genetic diagnosis of
thalassemia
DNA extracted from amniotic cells of pregnant women
was amplified with the α-thalassemia Genetic Deletion diagnostic
kit using the gap-PCR method (Daan Gene Co., Ltd.). The
thermocycling conditions were as follows: i) 96°C for 5 min, 98°C
for 45 sec; ii) 10 cycles at 65°C for 1.5 min, 72°C for 3 min; iii)
25 cycles at 98°C for 30 sec, 65°C for 45 sec and 72°C for 3 min;
and iv) 13 min at 72°C in a reaction volume of 25 µl with 50 ng
genomic DNA (primer sequences not commercially available). The
target products detected by agarose gel electrophoresis are shown
in Table SI.
For samples in which HBA2 levels were below the
normal range (2.5–3.5%) a β-thalassemia Mutation Genetic diagnostic
kit (DaAN Gene Co., Ltd.) was used. The thermocycling conditions
were: i) 50°C for 15 min; ii) 95°C for 10 min; iii) 94°C for 1 min;
iv) 35 cycles at 55° for 30 sec, 72°C for 30 sec; and v) 5 min at
72°C in a reaction volume of 25 µl with 50 ng genomic DNA (primer
sequences not commercially available). The PCR products were
hybridized with the membrane strip at 43°C for 2 h, and
subsequently the membranes were washed (washing reagent supplied as
part of the kit) for 15 min, incubated at 25°C for 30 min, shaken
and washed twice for 10 min. The film was subsequently washed for 2
min, then according to the instructions of the present solution and
displayed at 25°C for 15 min. The results were determined by
observing the presence of blue spots over the whole membrane, with
blue spots at the mutation site representing the presence of the
mutation.
Primer and probe design
For α-thalassemia, primers and probes were designed
using the reference sequence for chromosome 16 (GenBank accession
no. NC_000016.9; range, 222,846-223,709). For β-thalassemia, the
reference sequence for chromosome 11 was used (GenBank accession
no. NC_000011.9; range, 5,246,696-5,248,301). Reference sequences
were obtained from the GenBank repository (ncbi.nlm.nih.gov/genbank). The up- and downstream 10
kb regions of HBA and HBB, with 195 single nucleotide polymorphisms
(SNPs) associated with α-thalassemia and 275 SNPs with
β-thalassemia, were screened from the dbSNP database (ncbi.nlm.nih.gov/SNP/) using Ion AmpliSeq Designer
(ampliseq.com/) and the Agilent Sure Design
website (earray.chem.agilent.com/suredesign/home.htm). The
SNP site selection criteria used in the database were: i) SNP loci
in the 1,000 Genomes Project database
(gloshospitals.nhs.uk/about-us/research-our-hospitals/100000-genomes-project/)
from North and South China; ii) minor allele frequency (MAF) ≥20%;
iii) location of the SNP 100 bp sequence within a specific region;
iv) no homology identified in the genome; v) guanine-cytosine
content >45 and <70%; and vi) the SNP did not result in three
consecutive identical bases. The Ion AmpliSeq Thalassemia panel was
manufactured by Thermo Fisher Scientific, Inc., which consisted of
four primer pools comprising 1,354 pairs of primers for
α-thalassemia and 361 pairs of primers for β-thalassemia. The
thalassemia probes were constructed by Agilent Technologies, Inc.,
with a target region size of ~274 kb
Library construction
gDNA from the parents was used for library
construction using the Life Technologies™ Ion AmpliSeq Library kit
v. 2.0 (Thermo Fisher Scientific, Inc.), as follows: 10 ng gDNA, 4
µl 5X Ion AmpliSeq HiFi mix, 10 µl 2X Ion AmpliSeq primer pool and
4 µl nuclease-free water were mixed per reaction to amplify the
target regions. Subsequently, 2 µl FuPa reagent was added to each
amplified sample to partially digest the primer sequences, and each
library was ligated to a unique barcode and universal adapter in
the form of Life Technologies™ Ion Xpress™ barcode adapters (Thermo
Fisher Scientific, Inc.). Each library was purified using AMPure XP
beads (Beckman Coulter, Inc.) and quantified using a Life
Technologies™ Qubit® 3.0 fluorometer (Thermo Fisher
Scientific, Inc.). The size distributions of the libraries were
verified using a High Sensitivity DNA kit with a 2100 Bioanalyzer
(both Agilent Technologies, Inc.).
Libraries were constructed from cffDNA extracted
from the plasma of pregnant women using the Life Technologies™ Ion
Plus Fragments Library kit (Thermo Fisher Scientific, Inc.) with
the SureSelect Target Enrichment kit PTN Hyb Module Box2 and
SureSelect TE Reagent kit (both Agilent Technologies, Inc.). First,
30 µl cffDNA, 9.5 µl 5X End Repair buffer, 0.5 µl End Repair enzyme
and 10 µl nuclease-free water were mixed per reaction for end
repair of the cffDNA. Subsequently, the library was ligated to a
unique barcode and universal adapter using Life Technologies™ Ion
Xpress™ barcode adapters (Thermo Fisher Scientific, Inc.). Each
library was concentrated to 3.4 µl, and then 13 µl Hybridization
Buffer mix, 5.6 µl SureSelect Block mix and 2 µl SureSelect Library
were added, followed by incubation for 16 or 24 h at 65°C to
capture the target regions. Each positive library was enriched
using Life Technologies™ Dynabeads MyOne Streptavidin T1 (Thermo
Fisher Scientific, Inc.). The purified libraries were quantified
using a Qubit® 3.0 fluorometer. The size distributions
of the libraries were verified using a High Sensitivity DNA kit
with a 2100 Bioanalyzer (Agilent Technologies, Inc.).
Template preparation and enrichment
and NGS
Each library was diluted to 100 pM based on its
concentration quantified with the Qubit® 3.0
fluorometer. Subsequently, ten libraries (for blood samples) or
four libraries (for plasma) were mixed equally and diluted to 100
pM, respectively. The diluted sample was amplified through emulsion
PCR on Ion Proton™ HiQ™ ion sphere particles (ISPs) using a Life
Technologies™ Ion OneTouch™ 2 Instrument according to the
manufacturer's instructions. Template-positive ISPs were enriched
using a Life Technologies™ Ion OneTouch™ ES Instrument, according
to the manufacturer's instructions.
The enriched templates were loaded onto a Life
Technologies™ Ion PI™ chip kit V2 and sequenced on the Life
Technologies™ Ion Torrent Proton semiconductor sequencing platform.
All instruments and reagents were from Thermo Fisher Scientific,
Inc.
Haplotype
Sequences with a high quality of Q≥20 were mapped to
the human reference sequence hgl9 (Genome Reference Consortium,
GRCh37) (sanger.ac.uk/science/data/genome-reference-consortium).
The generated BAM files were then subjected to the quality control
process using the analysis system of Proton semiconductor
sequencing platform. The significance index, which must be met for
continued analysis, is achieved when the fraction of the target
region with coverage in excess of 30X >85% (27). Variants associated to Ion AmpliSeq
Thalassemia panel were screened using the Genome Analysis Toolkit
(GATK; version 3.4) (broadinstitute.org/gatk/) (28). Variants were annotated using the
bioinformatics software tool Annovar
(docopenbio.readthedocs.io/projects/annovar/en/latest/) as well as
in-house ad hoc bioinformatics tools (28). The detected variants were subjected
to a rigorous manual curation process that included querying
variant databases [e.g., dbSNP (ncbi.nlm.nih.gov/SNP/), Exome Aggregation Consortium
(exac.broadinstitute.org), 1,000 Genomes
(gloshospitals.nhs.uk/about-us/research-our-hospitals/100000-genomes-project/)
and Clinvar databases (ncbi.nlm.nih.gov/clinvar/)] and a literature review.
Common variation loci were screened in samples from the parents and
their first child, according to the exclusion criterion MAF
>0.1%. Subsequently, genotype information was used to determine
the parental haplotype and its linkage to the pathogenic allele,
following the rules of Mendelian inheritance.
RHDO sequential probability ratio test
(SPRT)
High quality plasma sequence data were mapped to the
human reference sequence hgl9 (Genome Reference Consortium GRCh37),
and variants were called using GATK (version 3.4) (29) with parameters optimized for
thalassemia. First, gDNA samples from the mother, father and
proband (‘trio’) were subjected to analysis of the target region.
For paternal inheritance, SNPs that were homozygous in the mother
and heterozygous in the father were used. Paternal haplotypes that
were inherited by the proband or absent in the proband were thus
identified. For maternal inheritance, SNPs that were heterozygous
in the mother and homozygous in the father were used. Maternal
haplotypes (linked or not linked to the proband's mutation) were
determined. Secondly, the target region of the pregnant mother was
determined from the plasma cffDNA. Detection of paternal specific
alleles in the maternal plasma revealed the inheritance of the
paternal haplotype, which could be either linked or not linked to
the proband's mutation, from the father. Maternal inheritance was
determined through RHDO analysis as previously described (24). Using the fractional fetal DNA
concentration, SPRT classification was used to determine the
statistical significance of the allelic imbalance within a
haplotype block for RHDO analysis. Cumulative sequencing counts of
SNP alleles from plasma cffDNA were inputted to the SPRT in order
of chromosomal position (30),
until a classification was possible. The SPRT curve was calculated
according to the following formula:
Upper boundary=(ln1200)/N−ln dln gLower
boundary=(ln 1/1200)/N−ln dln g,
Where
d=1−q11−q0
and
g=q1(1−q0)q0(1−q1)
‘Upper boundary’ and ‘lower boundary’ refer to the
upper and lower bounds, respectively (3). N is the number of samples for all
sites used for classification. q0 represents fetal inheritance of
maternal haplotype 2, based on statistics from the haplotype 1
ratio. q1 is the case of fetal inheritance of maternal haplotype 1,
from statistics of the haplotype 1 ratio. Haplotype 1 was defined
as the upper bound in this assay, and haplotype 2 as the lower
bound. Using the SPRT algorithm, the filtered points were used to
calculate the cumulative depth and cumulative frequency of
variations.
Analysis of amniotic fluid
All amniotic fluid samples were specifically
amplified as aforementioned using the α-thalassemia genetic
diagnostic kit by gap-PCR and the thalassemia RDB genotyping assay
kit (both DaAN Gene Co., Ltd.), according to the manufacturer's
instructions. Subsequently, the target products of gap-PCR were
detected by agarose gel electrophoresis.
Results
Hematological parameters and genotypes
of eight recruited families with thalassemia
Thalassemia screening generally includes the
detection of mean corpuscular volume (MCV), mean corpuscular
hemoglobin (MCH), HBA (α2β2) and HBA2 (α2δ2). The MCV reference
value usually falls within the range 80–100 fl while the MCH
reference value is in the 27–34 pg range. In addition, the HBA
reference value is within 96.5–97.5%, and the HBA2 reference value
2.5–3.5%.
The results for hypochromic anemia in all families
are presented in Table I. The MCV
and MCH values of all the subjects were found to be lower than
normal values. The HBA2 values of four individuals were lower than
normal values. The HBA2 values of another two individuals were
normal and the HBA2 values of ten individuals were higher than
normal values.
 | Table I.Results of hypochromic anemia
analysis for all families. |
Table I.
Results of hypochromic anemia
analysis for all families.
| Family number | Family member | MCV, fl | MCH, pg | HBA, % | HBA2, % | Type |
|---|
| 1 | Mother | 62.2 | 19.7 | 97.9 | 2.5 |
αQSα/αα |
|
| Father | 69.4 | 20.2 | 97.8 | 2.2 |
--SEA/αα |
| 2 | Mother | 64.6 | 19.6 | 97.7 | 2.3 |
--SEA/αα |
|
| Father | 63.4 | 18.9 | 95.9 | 2.2 |
-α3.7/αα |
| 3 | Mother | 72.5 | 22.4 | 94.2 | 5.2 |
βN/β+
(−28A>G) |
|
| Father | 76.9 | 23.9 | 92.0 | 5.7 | βN/β°
(IVS-2-654) |
| 4 | Mother | 58.5 | 20.2 | 93.6 | 6.0 | βN/β°
(CD41-42_CTTT) |
|
| Father | 63.7 | 22.2 | 95.5 | 4.5 |
βN/β+
(−28A>G) |
| 5 | Mother | 79.9 | 25.4 | 97.1 | 2.9 |
αCSα/αα |
|
| Father | 63.2 | 19.9 | 97.9 | 2.1 |
--SEA/αα |
| 6 | Mother | 65.0 | 21.0 | 93.2 | 6.5 |
--SEA/αα& βN/β°
(CD41-42_CTTT) |
|
| Father | 61.8 | 19.7 | 92.5 | 5.9 | βN/β°
(CD41-42_CTTT) |
| 7 | Mother | 66.8 | 21.1 | 93.2 | 6.0 |
βN/β0N(CD71-72+A) |
|
| Father | 72.4 | 22.2 | 95.1 | 4.9 |
βN/β+
(−28A>G) |
| 8 | Mother | 60.4 | 18.5 | 94.0 | 6.0 | βN/β°
(CD41-42_CTTT) |
|
| Father | 59.9 | 19.1 | 92.1 | 5.9 | βN/β°
(CD17A>T) |
The results for microcytic anemia in all families
are shown in Table I. Moreover, in
total, three families exhibited α-thalassemia, four families had
β-thalassemia and one family had both α- and β-thalassemia
(Figs. S1–S3).
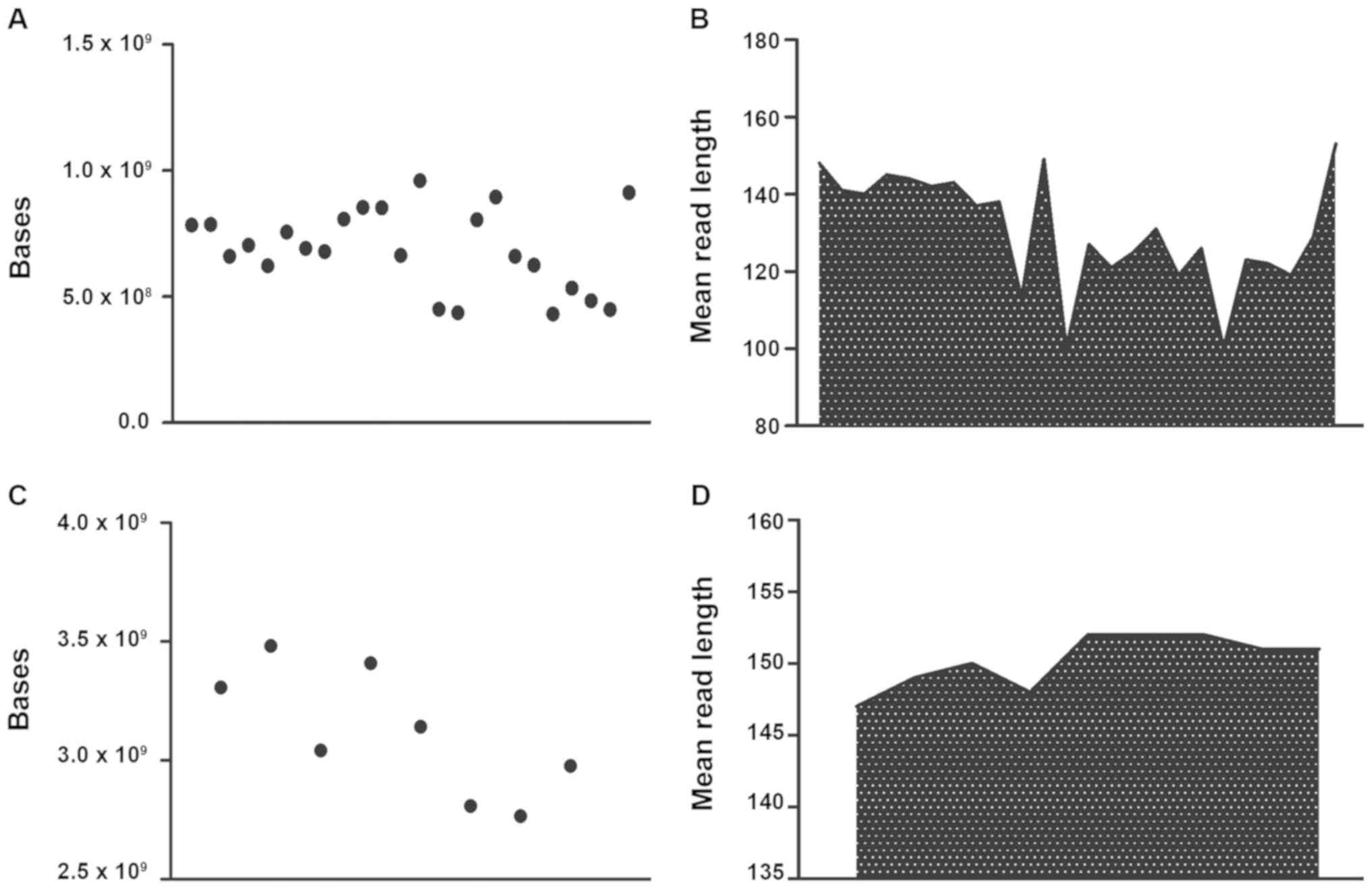
Sequencing statistics
For blood DNA samples, the average number of total
raw bases was 728,011,603 (range, 431,538,785-1,100,881,706). The
average read length was 137 bp. The mean percentage of sequencing
reads mapped to the reference hg19 genome was 98%. After the
filtering of low-quality reads, polyclonal reads and primer dimer
reads, the number of sequenced bases with Q≥20 ranged between
345,306,892-921,298,977 (Fig. 1A and
B). After mapping to the hg19 genome and the removal of Q<20
reads, polyclonal reads and primer dimer reads, the remaining
sequences were mapped to the target regions, containing 195 SNPs
for α-thalassemia and 275 SNPs for β-thalassemia (data not shown).
Furthermore, an average depth of coverage of 118X (range, 70-178X)
was obtained for all 470 SNPs across the 24 blood samples (data not
shown).
For plasma DNA samples, the average number of total
raw bases was 2,986,588,135 (range, 2,509,364,780-3,482,168,649).
The average read length was 151 bp. The mean percentage of
sequencing reads mapped to the reference hg19 genome was 98%. After
filtering of low-quality reads, polyclonal reads and primer dimer
reads, the number of sequenced bases with Q-values ≥20 ranged
between 2,157,982,851-2,975,281,429 (Fig. 1C and D). Finally, an average depth
of coverage of 836X (range, 702–975X) was obtained for all 470 SNPs
across the eight plasma samples.
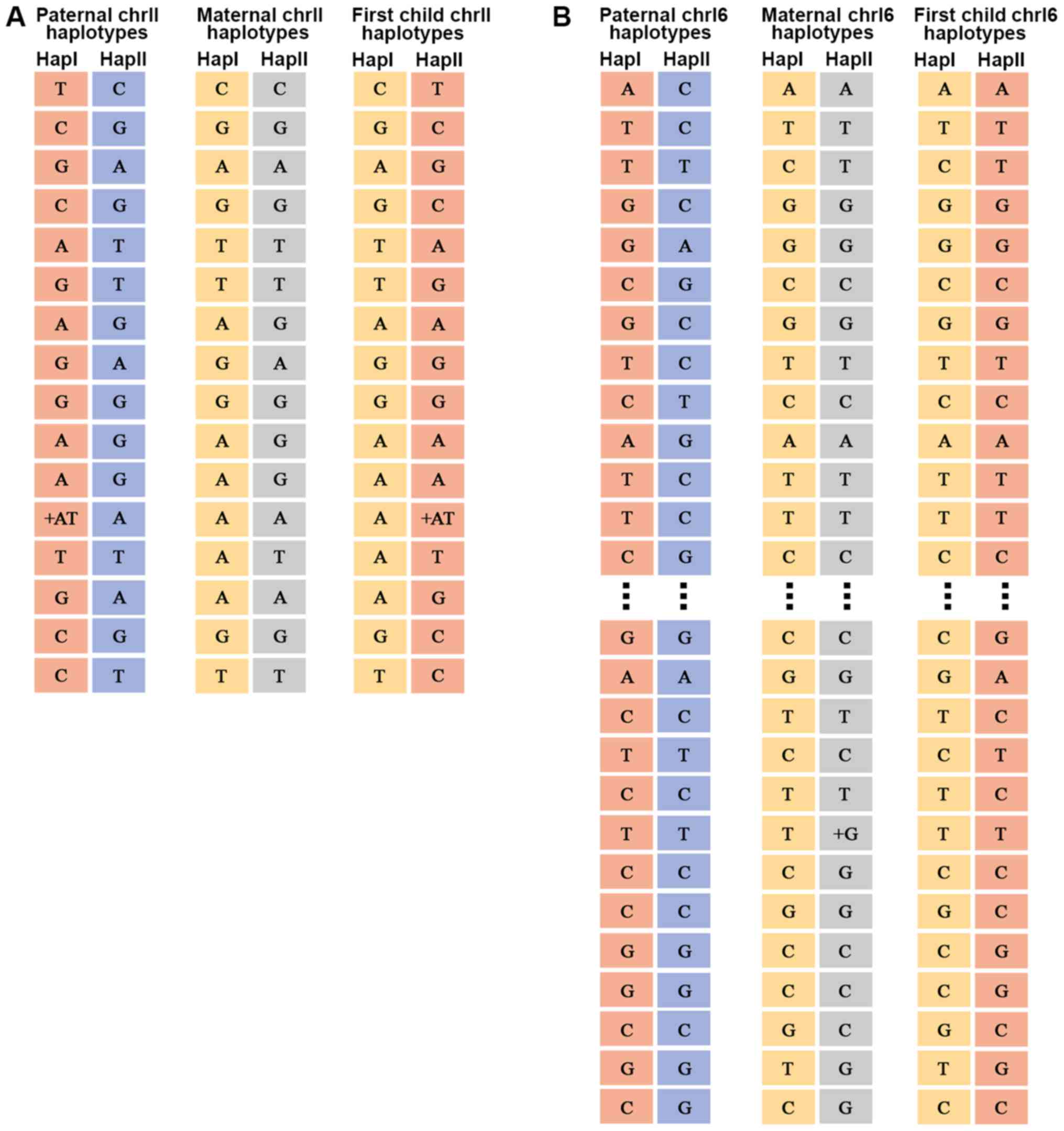
Haplotypes
The fractional fetal DNA concentration in the
maternal plasma, f, can be calculated from sequencing data as
f=2p/(p + q), where p is the number of sequenced reads of the fetal
specific allele and q is the read count of the other allele, which
is shared by the maternal and fetal genomes (31). The average percentage of fetal DNA
in maternal plasma was found to be 17.3% (range, 15–19%) (data not
shown). For the father, mother and child, the chromosome 11 and 16
haplotypes were sorted into 16 and 87 different SNP categories,
respectively (data not shown). An example of chromosome 11 and 16
haplotypes for a family is illustrated in Fig. 2. The genotype information of the
parents was used to determine the parental haplotype and its
linkage to the pathogenic allele according to Mendelian inheritance
laws (32). Detailed information
regarding the haplotypes associated with the pathogenic allele is
provided in Table II.
| Table II.Haplotypes associated with the
pathogenic allele. |
Table II.
Haplotypes associated with the
pathogenic allele.
| Family number | Maternal
haplotype | Paternal
haplotype |
|---|
| 1 | Hap II | Hap II |
| 2 | Hap I | Hap I |
| 3 | Hap II | Hap II |
| 4 | Hap II | Hap I |
| 5 | Hap II | Hap II |
| 6 | α: Hap I; β: Hap
II | Hap II |
| 7 | Hap I | Hap II |
| 8 | Hap II | Hap I |
Genetic analysis of paternal and
maternal genotypes
The genetic results for the father were based on an
analysis of SNPs that were heterozygous in the plasma, while being
homozygous in the mother and heterozygous in the father, or
homozygous in both, but with different genotypes. Overall, the
eight fetuses inherited haplotype I of their father (Table III). For maternal inheritance,
SNPs were analyzed where the mother was heterozygous and the father
was homozygous, allowing the detection of slight allelic imbalances
in the maternal plasma using RHDO and SPRT.
| Table III.Parental genetic source results for
family 1. |
Table III.
Parental genetic source results for
family 1.
| Chr | Position | Hap I of
father | Hap II of
father | Hap I of
mother | Hap II of
mother | Fetal | Inherited |
|---|
| Chr11 | 4178706 | T | C | C | C | C:T | Hap I |
| Chr11 | 4186666 | T | C | C | C | C:T | Hap I |
| Chr11 | 4415266 | C | A | A | A | A:C | Hap I |
| Chr11 | 4415319 | A | G | G | G | G:A | Hap I |
| Chr11 | 5452526 | G | A | A | A | A:G | Hap I |
| Chr11 | 5546041 | C | G | G | G | G:C | Hap I |
| Chr11 | 5550754 | C | G | G | G | G:C | Hap I |
| Chr11 | 5554559 | C | G | G | G | G:C | Hap I |
| Chr11 | 5573193 | T | A | A | A | A:T | Hap I |
| Chr16 | 142200 | A | G | G | G | G:A | Hap I |
| Chr16 | 218532 | C | SEA | T | T | T:C | Hap I |
| Chr16 | 219497 | G | SEA | G | G | G:A | Hap I |
| Chr16 | 248418 | C | T | T | T | T:C | Hap I |
| Chr16 | 306062 | G | C | C | C | C:G | Hap I |
| Chr16 | 326525 | C | A | A | A | A:C | Hap I |
| Chr16 | 754288 | T | C | C | C | C:T | Hap I |
| Chr16 | 893160 | A | G | G | G | G:A | Hap I |
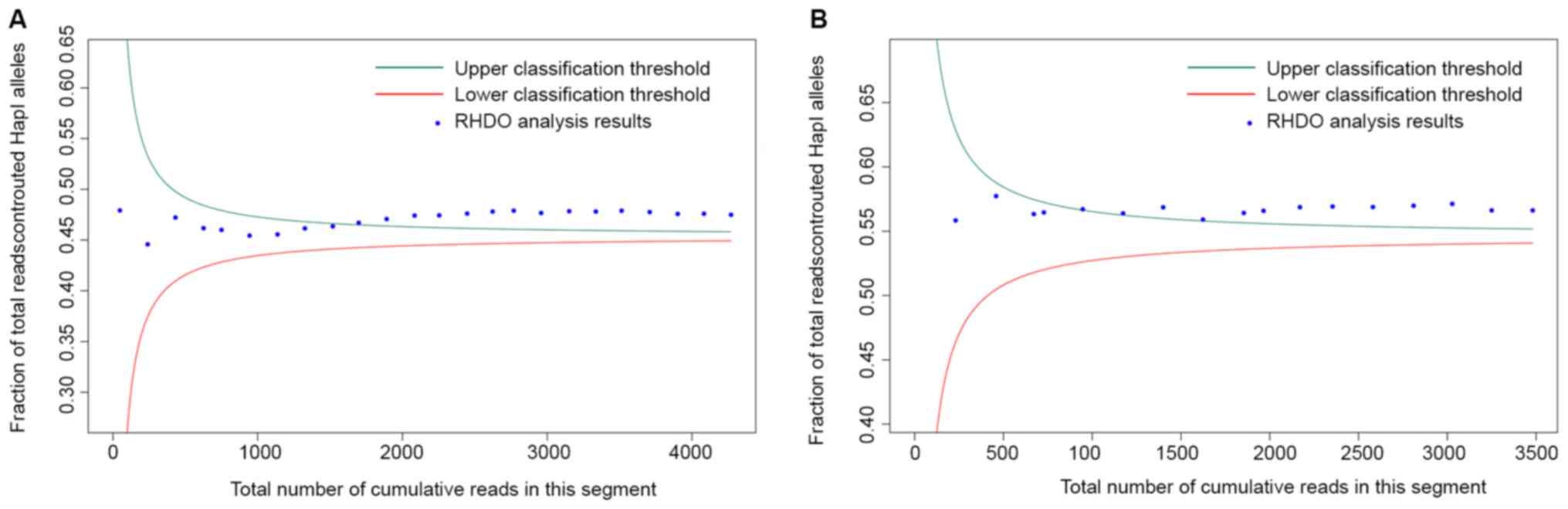
In total, eight fetuses inherited haplotype I from
their mother. The results of RHDO SPRT for family 1 are illustrated
in Fig. 3 and Tables IV and V. A summary of the results for all eight
fetal genotypes is shown in Table
VI. It was found that three fetuses (from family 1, family 3
and family 5) had no inheritance of their parents' pathogenic
sites; three fetuses (from family 4, family 7 and family 8) only
inherited the pathogenic site of one parent; and one fetus (family
2) inherited the pathogenic sites of both parents.
| Table IV.SPRT classification process for
relative haplotype dosage analysis of type α single nucleotide
polymorphisms near the p-ter of chromosome 16 in family 1. |
Table IV.
SPRT classification process for
relative haplotype dosage analysis of type α single nucleotide
polymorphisms near the p-ter of chromosome 16 in family 1.
| Position | Hap I count | Hap II count | Hap I cum. | Hap II cum. | Total reads | Hap I fraction | Upper boundary | Lower boundary | SPRT |
|---|
| 234632 | 23 | 25 | 23 | 25 | 48 | 0.4792 | 0.8506 | 0.0569 | Unclassified |
| 256278 | 84 | 108 | 107 | 133 | 240 | 0.4458 | 0.5331 | 0.3744 | Unclassified |
| 281299 | 97 | 95 | 204 | 228 | 432 | 0.4722 | 0.4978 | 0.4096 | Unclassified |
| 281885 | 85 | 109 | 289 | 337 | 626 | 0.4617 | 0.4842 | 0.4233 | Unclassified |
| 306243 | 56 | 68 | 345 | 405 | 750 | 0.4600 | 0.4791 | 0.4283 | Unclassified |
| 311853 | 84 | 110 | 429 | 515 | 944 | 0.4544 | 0.4739 | 0.4336 | Unclassified |
| 312253 | 89 | 104 | 518 | 619 | 1,137 | 0.4556 | 0.4705 | 0.4370 | Unclassified |
| 312635 | 94 | 95 | 612 | 714 | 1,326 | 0.4615 | 0.4681 | 0.4394 | Unclassified |
| 315557 | 92 | 101 | 704 | 815 | 1,519 | 0.4635 | 0.4663 | 0.4412 | Unclassified |
| 317393 | 89 | 90 | 793 | 905 | 1,698 | 0.4670 | 0.4650 | 0.4425 | Hap I |
| 319761 | 97 | 96 | 890 | 1,001 | 1,891 | 0.4707 | 0.4638 | 0.4437 | Hap I |
| 336660 | 98 | 95 | 988 | 1,096 | 2,084 | 0.4741 | 0.4629 | 0.4446 | Hap I |
| 377617 | 81 | 89 | 1,069 | 1,185 | 2,254 | 0.4743 | 0.4622 | 0.4453 | Hap I |
| 390780 | 96 | 97 | 1,165 | 1,282 | 2,447 | 0.4761 | 0.4615 | 0.4460 | Hap I |
| 423420 | 89 | 87 | 1,254 | 1,369 | 2,623 | 0.4781 | 0.4610 | 0.4465 | Hap I |
| 427516 | 72 | 74 | 1,326 | 1,443 | 2,769 | 0.4789 | 0.4606 | 0.4469 | Hap I |
| 641445 | 84 | 105 | 1,410 | 1,548 | 2,958 | 0.4767 | 0.4602 | 0.4473 | Hap I |
| 651517 | 98 | 96 | 1,508 | 1,644 | 3,152 | 0.4784 | 0.4598 | 0.4477 | Hap I |
| 674029 | 87 | 97 | 1,595 | 1,741 | 3,336 | 0.4781 | 0.4594 | 0.4480 | Hap I |
| 678843 | 88 | 90 | 1,683 | 1,831 | 3,514 | 0.4789 | 0.4592 | 0.4483 | Hap I |
| 878161 | 88 | 106 | 1,771 | 1,937 | 3,708 | 0.4776 | 0.4589 | 0.4486 | Hap I |
| 880431 | 85 | 109 | 1,856 | 2,046 | 3,902 | 0.4757 | 0.4586 | 0.4489 | Hap I |
| 928867 | 87 | 94 | 1,943 | 2,140 | 4,083 | 0.4759 | 0.4584 | 0.4491 | Hap I |
| 940706 | 85 | 102 | 2,028 | 2,242 | 4,270 | 0.4749 | 0.4582 | 0.4493 | Hap I |
| Table V.SPRT classification process for
relative haplotype dosage analysis of type β single nucleotide
polymorphisms near the p-ter of chromosome 16 in family 1. |
Table V.
SPRT classification process for
relative haplotype dosage analysis of type β single nucleotide
polymorphisms near the p-ter of chromosome 16 in family 1.
| Position | Hap I count | Hap II count | Hap I cum. | Hap II cum. | Total reads | Hap I fraction | Upper boundary | Lower boundary | SPRT |
|---|
| 151136 | 129 | 102 | 129 | 102 | 231 | 0.5584 | 0.6287 | 0.4638 | Unclassified |
| 192314 | 136 | 92 | 265 | 194 | 459 | 0.5773 | 0.5878 | 0.5048 | Unclassified |
| 225159 | 113 | 99 | 378 | 293 | 671 | 0.5633 | 0.5746 | 0.5179 | Unclassified |
| 231541 | 33 | 24 | 411 | 317 | 728 | 0.5646 | 0.5724 | 0.5201 | Unclassified |
| 235660 | 126 | 93 | 537 | 410 | 947 | 0.5671 | 0.5664 | 0.5262 | Hap I |
| 241210 | 125 | 102 | 662 | 512 | 1,174 | 0.5639 | 0.5625 | 0.5300 | Hap I |
| 258741 | 134 | 92 | 796 | 604 | 1,400 | 0.5686 | 0.5599 | 0.5327 | Hap I |
| 326826 | 112 | 112 | 908 | 716 | 1,624 | 0.5591 | 0.5580 | 0.5345 | Hap I |
| 534954 | 138 | 92 | 1,046 | 808 | 1,854 | 0.5642 | 0.5565 | 0.5360 | Hap I |
| 902172 | 66 | 45 | 1,112 | 853 | 1,965 | 0.5659 | 0.5560 | 0.5366 | Hap I |
| 903426 | 122 | 83 | 1,234 | 936 | 2,170 | 0.5687 | 0.5550 | 0.5375 | Hap I |
| 905559 | 106 | 78 | 1,340 | 1,014 | 2,354 | 0.5692 | 0.5544 | 0.5382 | Hap I |
| 922134 | 128 | 99 | 1,468 | 1,113 | 2,581 | 0.5688 | 0.5536 | 0.5389 | Hap I |
| 935560 | 133 | 96 | 1,601 | 1,209 | 2,810 | 0.5698 | 0.5530 | 0.5395 | Hap I |
| 937413 | 129 | 89 | 1,730 | 1,298 | 3,028 | 0.5713 | 0.5526 | 0.5400 | Hap I |
| 945728 | 110 | 112 | 1,840 | 1,410 | 3,250 | 0.5662 | 0.5521 | 0.5404 | Hap I |
| 947817 | 131 | 100 | 1,971 | 1,510 | 3,481 | 0.5662 | 0.5517 | 0.5408 | Hap I |
| Table VI.Results for the eight fetal
genotypes. |
Table VI.
Results for the eight fetal
genotypes.
| Fetus number | Haplotype inherited
from father | Haplotype inherited
from mother | Type |
|---|
| 1 | Hap I | Hap I | αα/αα |
| 2 | Hap I | Hap I |
--SEA/-α3.7 |
| 3 | Hap I | Hap I |
βN/βN |
| 4 | Hap I | Hap I |
β+[-28(A>G)]/βN |
| 5 | Hap I | Hap I | αα/αα |
| 6 | Hap I | Hap I | --SEA/αα,
βN/βN |
| 7 | Hap I | Hap I |
β°[CD71-72(+A)]/βN |
| 8 | Hap I | Hap I |
β°[CD17(AAG>TAG)]/βN |
Accuracy of fetus haplotype
determination
To further verify the accuracy of fetal haplotype
inference for NIPT, the results obtained from maternal plasma DNA
sequencing were validated using gap-PCR and RDB of fetal gDNA
collected from amniotic fluid cells. The non-invasive results were
100% consistent with the gap-PCR and RDB results from amniotic
fluid for these eight samples (Figs.
1 and 2).
Discussion
The discovery of cffDNA in maternal plasma has
allowed for the possibility of non-invasive prenatal diagnosis of
genetic disorders. Applications of cffDNA include screening for
aneuploidies, prenatal diagnosis of mutation based monogenic
diseases, and fetal Rhesus D status determination (33). These techniques are based on
qualitative and quantitative comparisons of cffDNA with the
background of maternal cffDNA in maternal plasma (10). Non-invasive prenatal screening for
aneuploidies based on NGS was rapidly incorporated into routine
clinical practice (30).
Accordingly, guidelines for clinical application and committee
guidance regarding NIPT have been issued by numerous medical
societies, including the Society of Obstetricians and
Gynaecologists of Canada (34),
the Italian College of Fetal Maternal Medicine (35), the American College of Medical
Genetics and Genomics (36), the
National Society of Genetic Counselors and the International
Society for Prenatal Diagnosis (37). Furthermore, genome-wide micro
deletion or micro duplication syndromes have been screened for in
an expanded NIPT protocol.
Maternal plasma cffDNA includes cffDNA and maternal
cffDNA, and half of fetal alleles are inherited paternally. Xiong
et al (38) reported one
case of this type of non-invasive prenatal diagnosis using PCR and
NGS for the detection of a paternal pathogenic mutation. Yan et
al (39) and Ho et al
(40) reported exclusion of fetal
homozygous α-thalassemia based on the presence of the father's SNP
within the break point sequence. However, these methods can only be
used to exclude fetal risk and do not provide the exact genotype of
the fetus. Quantification of specific alleles can provide accurate
fetal genotype results. In this manner, several monogenic diseases
have been successfully detected non-invasively using cffDNA and PCR
based methods (41,42). NGS-based approaches have also been
applied to non-invasive prenatal diagnosis of β-thalassemia through
deduction of the fetal inheritance of maternally transmitted
mutations via the quantification of the relative levels of
haplotypes with SNP alleles in and around the targeted gene.
Recently, Yang et al (43)
reported a robust and versatile NGS-based cffDNA allelic molecule
counting system termed the cffDNA barcode enabled single molecule
test, which was developed for the non-invasive prenatal diagnosis
of β-thalassemia. However, these methods mainly aim to identify
SNV-associated thalassemia and have not been applied to
CNV-associated thalassemia (44).
The present study aimed to develop a system for
non-invasive prenatal detection of paternal and maternal mutations
associated with α- and β-thalassemia. It was demonstrated that
multiplex PCR or target capture combined with NGS of highly
heterozygous SNPs within the 10 kb flanking region of the gene of
interest effectively reduced the target region size for detection
of paternal and maternal mutations. Furthermore, this technique may
be used to detect both α- and β-thalassemia, as well as SNPs and
large deletion mutations. gDNA of the parents and their children
were amplified via multiplex PCR using a thalassemia panel, and
cffDNA was captured with a set of thalassemia probes. The products
were sequenced using NGS. Subsequently, the parental haplotype was
determined using a trio-based strategy. The genetic results for the
father were based on analysis of SNPs that were heterozygous in the
plasma and were also either homozygous in the mother and
heterozygous in the father, or homozygous in both, but of different
genotypes. For maternal inheritance, SNPs were analyzed where the
mother was heterozygous and the father was homozygous, and whether
a slight allelic imbalance was present in maternal plasma was
investigated using RHDO SPRT. In total, three cases of
α-thalassemia, four of β-thalassemia and one case of combined α-
and β-thalassemia were successfully diagnosed using this
non-invasive prenatal diagnosis method, and the results exhibited
high consistency with the traditional invasive method. Fetal
genotypes were successfully deduced non-invasively for eight
families. The non-invasively determined haplotypes of the eight
fetuses were identical with those obtained through invasive
prenatal diagnosis procedures, with an accuracy rate of 100% in the
target region.
In the present study, the average percentage of
fetal DNA was 17.3%. As accuracy is affected by the fetal fraction,
in follow-up studies, additional cases should be tested, especially
using samples collected in early gestation, in order to thoroughly
evaluate the method prior to clinical application. This study,
however, has provided an example of non-invasive prenatal diagnosis
of single gene diseases that can be exploited for other single gene
diseases, such as congenital adrenal hyperplasia, Ellis van Creveld
syndrome, hemophilia and Hunter's syndrome. Overall, multiplex PCR
and target capture combined with NGS of highly heterozygous SNPs
flanking the gene of interest is an effective method to reduce
sequencing costs.
In conclusion, the routine prenatal diagnosis method
for thalassemia currently used clinically is gap-PCR and RDB of
fetal DNA, which can be acquired from ultrasound mediated abdominal
biopsy, amniocentesis or cordocentesis. However, these invasive
procedures may increase the risk of miscarriage and cause anxiety
for pregnant women. The present study demonstrated the feasibility
of non-invasive prenatal diagnosis of thalassemia using cffDNA from
the plasma of pregnant women through target capture and NGS
combined with RHDO analysis. Furthermore, this method can be used
to detect deletion and mutation-based thalassemia at a relatively
lower cost, as well as to investigate other diseases caused by CNVs
and SNVs.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the Science and
Technology Program of Guangzhou (grant nos. 201604020104 and
201704020114), the Key Program for Health Care Collaborative
Innovation of Guangzhou (grant no. 201803040009) and the Natural
Scientific Research Foundation of Guangdong Province (grant no.
2018A030313286).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XY, YCY, XXY and JZ conceived and designed the
study. YCY and DMF performed the experiments. XY, YCY and DMF wrote
the manuscript. XXY and JZ improved the manuscript. DMF, XY, SL ML
and HYH analyzed the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study protocol was approved by the Medical
Ethics Committee of The Third Affiliated Hospital of Sun Yatsen
University, and the Committee on Human Research, Publications and
Ethics of School of Laboratory Medicine and Biotechnology, Southern
Medical University. Prior to recruitment and sample collection,
meetings were held to explain in detail the purpose and procedures
of the study. The inconveniences involved, including blood
sampling, were also explained to the participants. Written informed
consent was obtained from each participant or the participant's
guardian. The study was undertaken according to the principles of
the Helsinki Declaration of 1975 (as revised 2008).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Higgs DR, Engel JD and Stamatoyannopoulos
G: Thalassaemia. Lancet. 379:373–383. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pan HF, Long GF, Li Q, Feng YN, Lei ZY,
Wei HW, Huang YY, Huang JH, Lin N, Xu QQ, et al: Current status of
thalassemia in minority populations in Guangxi, China. Clin Genet.
71:419–426. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lo YM, Chan KC, Sun H, Chen EZ, Jiang P,
Lun FM, Zheng YW, Leung TY, Lau TK, Cantor CR and Chiu RW: Maternal
plasma DNA sequencing reveals the genome-wide genetic and
mutational profile of the fetus. Sci Transl Med. 2:61ra912010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yin A, Li B, Luo M, Xu L, Wu L, Zhang L,
Ma Y, Chen T, Gao S, Liang J, et al: The prevalence and molecular
spectrum of α- and β-globin gene mutations in 14,332 families of
Guangdong province, China. PLoS One. 9:e898552014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cao A and Kan YW: The prevention of
thalassemia. Cold Spring Harb Perspect Med. 3:a117752013.
View Article : Google Scholar
|
|
6
|
Mourad FH, Hoffbrand AV, Sheikh-Taha M,
Koussa S, Khoriaty AI and Taher A: Comparison between
desferrioxamine and combined therapy with desferrioxamine and
deferiprone in iron overloaded thalassaemia patients. Br J
Haematol. 121:187–189. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lidonnici MR and Ferrari G: Gene therapy
and gene editing strategies for hemoglobinopathies. Blood Cells Mol
Dis. 70:87–101. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Allyse M, Minear M, Rote M, Hung A,
Chandrasekharan S, Berson E and Sridhar S: Non-invasive prenatal
testing: A review of international implementation and challenges.
Int J Women's Health. 7:113–126. 2015. View Article : Google Scholar
|
|
9
|
Mujezinovic F and Alfirevic Z:
Procedure-relatedcomplications of amniocentesis and chorionic
villous sampling: A systematic review. Obstet Gynecol. 110:687–694.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lo YM, Corbetta N, Chamberlain PF, Rai V,
Sargent IL, Redman CW and Wainscoat JS: Presence of fetal DNA in
maternal plasma and serum. Lancet. 350:485–487. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Babkina N and Graham JM: New genetic
testing in prenatal diagnosis. Semin Fetal Neonatal Med.
19:214–219. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chiu RW, Akolekar R, Zheng YW, Leung TY,
Sun H, Chan KC, Lun FM, Go AT, Lau ET, To WW, et al: Non-invasive
prenatal assessment of trisomy 21 by multiplexed maternal plasma
DNA sequencing: Large scale validity study. BMJ. 342:c74012011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
You Y, Sun Y, Li X, Li Y, Wei X, Chen F,
Ge H, Lan Z, Zhu Q, Tang Y, et al: Integration of targeted
sequencing and NIPT into clinical practice in a Chinese family with
maple syrup urine disease. Genet Med. 16:594–600. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
McCullough RM, Almasri EA, Guan X, Geis
JA, Hicks SC, Mazloom AR, Deciu C, Oeth P, Bombard AT, Paxton B, et
al: Non-invasive prenatal chromosomal aneuploidy testing-clinical
experience: 100,000 clinical samples. PLoS One. 9:e1091732014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li Y, Zimmermann B, Rusterholz C, Kang A,
Holzgreve W and Hahn S: Size separation of circulatory DNA in
maternal plasma permits ready detection of fetal DNA polymorphisms.
Clin Chem. 50:1002–1011. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chan KC, Zhang J, Hui AB, Wong N, Lau TK,
Leung TN, Lo KW, Huang DW and Lo YM: Size distributions of maternal
and fetal DNA in maternal plasma. Clin Chem. 50:88–92. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hui WW, Jiang P, Tong YK, Lee WS, Cheng
YK, New MI, Kadir RA, Chan KC, Leung TY, Lo YM and Chiu RW:
Universal haplotype-based noninvasive prenatal testing for single
gene diseases. Clin Chem. 63:513–524. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Xu Y, Li X, Ge H, Xiao B, Zhang Y, Ying X,
Pan X, Wang L, Xie W, Ni L, et al: Haplotype-based approach for
noninvasive prenatal tests of Duchenne muscular dystrophy using
cell-free fetal DNA in maternal plasma. Genet Med. 17:889–896.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ma D, Ge H, Li X, Jiang T, Chen F, Zhang
Y, Hu P, Chen S, Zhang J, Ji X, et al: Haplotype-based approach for
noninvasive prenatal diagnosis of congenital adrenal hyperplasia by
maternal plasma DNA sequencing. Gene. 544:252–258. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lo YM, Hjelm NM, Fidler C, Sargent IL,
Murphy MF, Chamberlain PF, Poon PM, Redman CW and Wainscoat JS:
Prenatal diagnosis of fetal RhD status by molecular analysis of
maternal plasma. N Engl J Med. 339:1734–1738. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Saito H, Sekizawa A, Morimoto T, Suzuki M
and Yanaihara T: Prenatal DNA diagnosis of a single-gene disorder
from maternal plasma. Lancet. 356:11702000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Amicucci P, Gennarelli M, Novelli G and
Dallapiccola B: Prenatal diagnosis of myotonic dystrophy using
fetal DNA obtained from maternal plasma. Clin Chem. 46:301–302.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
González-González MC, Trujillo MJ,
Rodríguez de Alba M, García-Hoyos M, Lorda-Sánchez I, Díaz-Recasens
J, Ayuso C and Ramos C: Huntington disease-unaffected fetus
diagnosed from maternal plasma using QF-PCR. Prenatal Diag.
23:232–234. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lam KW, Jiang P, Liao GJ, Chan KC, Leung
TY, Chiu RW and Lo YM: Noninvasive prenatal diagnosis of monogenic
diseases by targeted massively parallel sequencing of maternal
plasma: Application to β-Thalassemia. Clin Chem. 58:1467–1475.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Camunas-Soler J, Lee H, Hudgins L, Hintz
SR, Blumenfeld YJ, El-Sayed YY and Quake SR: Noninvasive prenatal
diagnosis of single-gene disorders by use of droplet digital PCR.
Clin Chem. 64:336–345. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hudecova I and Chiu RW: Non-invasive
prenatal diagnosis of thalassemias using maternal plasma cell free
DNA. Best Pract Res Clin Obstet Gynaecol. 39:63–73. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wenke L, Fengyu L, Siyao Z, Bin C, Na Z,
Yu N, Dao Z and Qian Z: Automatic analysis pipeline of
next-generation sequencing data. Yi Chuan. 36:618–624. 2014.(In
Chinese). PubMed/NCBI
|
|
28
|
De Summa S, Malerba G, Pinto R, Mori A,
Mijatovic V and Tommasi S: GATK hard filtering: Tunable parameters
to improve variant calling for next generation sequencing targeted
gene panel data. BMC Bioinformatics. 18 (Suppl 5):S1192017.
View Article : Google Scholar
|
|
29
|
Bauer DC: Variant calling comparison
CASAVA1.8 and GATK. Nat Prec. 18–Jul;2011.doi:
10.1038/npre.2011.6107.1. View Article : Google Scholar
|
|
30
|
Lo YM, Lun FM, Chan KC, Tsui NB, Chong KC,
Lau TK, Leung TY, Zee BC, Cantor CR and Chiu RW: Digital PCR for
the molecular detection of fetal chromosomal aneuploidy. Proc Natl
Acad Sci USA. 104:13116–13121. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Meng M, Li X, Ge H, Chen F, Han M, Zhang
Y, Kang D, Xie W, Gao Z, Pan X, et al: Noninvasive prenatal testing
for autosomal recessive conditions by maternal plasma sequencing in
a case of congenital deafness. Genet Med. 16:972–976. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Allen S, Young E and Bowns B: Noninvasive
prenatal diagnosis for single gene disorders. Curr Opin Obstet
Gynecol. 29:73–79. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Walsh JM and Goldberg JD: Fetal aneuploidy
detection by maternal plasma DNA sequencing: A technology
assessment. Prenatal Diag. 33:514–520. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Galbiati S, Monguzzi A, Damin F, Soriani
N, Passiu M, Castellani C, Natacci F, Curcio C, Seia M, Lalatta F,
et al: COLD-PCR and microarray: Two independent highly sensitive
approaches allowing the identification of fetal paternally
inherited mutations in maternal plasma. J Med Genet. 53:481–487.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Langlois S and Brock J; Genetics
Committee, : Current status in non-invasive prenatal detection of
down syndrome, trisomy 18, and trisomy 13 using cell-Free DNA in
Maternal Plasma. J Obstetr Gynaecol Can. 35:177–181. 2013.(In
English, French). View Article : Google Scholar
|
|
36
|
Benn P, Borrell A, Chiu RW, Cuckle H,
Dugoff L, Faas B, Gross S, Huang T, Johnson J, Maymon R, et al:
Position statement from the chromosome abnormality screening
committee on behalf of the board of the international society for
prenatal diagnosis. Prenatal Diag. 35:725–734. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Gregg AR, Gross SJ, Best RG, Monaghan KG,
Bajaj K, Skotko BG, Thompson BH and Watson MS: ACMG statement on
noninvasive prenatal screening for fetal aneuploidy. Genet Med.
15:395–398. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Xiong L, Barrett AN, Hua R, Tan TZ, Ho SS,
Chan JK, Zhong M and Choolani M: Non-invasive prenatal diagnostic
testing for β-thalassaemia using cell-free fetal DNA and
next-generation sequencing. Prenat Diagn. 35:258–265. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yan TZ, Mo QH, Cai R, Chen X, Zhang CM,
Liu YH, Chen YJ, Zhou WJ, Xiong F and Xu XM: Reliable detection of
paternal SNPs within deletion breakpoints for non-invasive prenatal
exclusion of homozygous α-thalassemia in maternal plasma. PLoS One.
6:e247792011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ho SS, Chong SS, Koay ES, Ponnusamy S,
Chiu L, Chan YH, Rauff M, Baig S, Chan J, Su LL, et al: Noninvasive
prenatal exclusion of haemoglobin Bart's using foetal DNA from
maternal plasma. Prenat Diagn. 30:65–73. 2010.PubMed/NCBI
|
|
41
|
Devers PL, Cronister A, Ormond KE, Facio
F, Brasington CK and Flodman P: Noninvasive prenatal
Testing/Noninvasive prenatal diagnosis: The Position of the
National Society of Genetic Counselors. J Genet Couns. 22:291–295.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lee ST, Weykamp CW, Lee YW, Kim JW and Ki
CS: Effects of 7 hemoglobin variants on the measurement of
glycohemoglobin by 14 analytical methods. Clin Chem. 53:2202–2205.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yang X, Zhou Q, Zhou W, Zhong M, Guo X,
Wang X and Fan X: A Cell-free DNA Barcode-enabled single-molecule
test for noninvasive prenatal diagnosis of monogenic disorders:
Application to β-thalassemia. Adv Sci. 6:18023322019. View Article : Google Scholar
|
|
44
|
Fan DM, Yang X, Huang LM, Ouyang GJ, Yang
XX and Li M: Simultaneous detection of target CNVs and SNVs of
thalassemia by multiplex PCR and nextgeneration sequencing. Mol Med
Rep. 19:2837–2848. 2019.PubMed/NCBI
|