Introduction
Intestinal malrotation is a congenital aberrant
positioning of the bowel that is usually accompanied with anomalous
bowel fixation through mesenteric bands or a lack of fixation in
parts of the bowel (1). Intestinal
malrotation was first described by William Ladd in 1936 and later
classified as non-rotation, mixed or incomplete rotation, reversed
rotation, or mesocolic hernia (2,3).
Typically, ≤ one in 200 newborns are estimated to have asymptomatic
rotational anomaly (3,4). Symptomatic malrotation affects 1 in
6,000 live births and often occurs in the first few weeks of life,
resulting in elevated risk of bowel obstruction, midgut volvulus
and necrosis in the bowel (3,5,6).
Currently, upper gastrointestinal (UGI) series is the preferred
imaging technique for malrotation diagnosis. Nevertheless, both
false positive and false negative interpretations occur, with
reported false positive rates of ≤15% (1,7,8).
When the duodenojejunal junction position is ambiguous based on UGI
series, further examination is necessary. A barium enema might
prove helpful in such cases; however, the first pass of barium
through the duodenum is often overlooked (9). The duodenal anatomy is hard to
recognize with inadequate amounts of barium, while excessive barium
could cause rapid and uncontrolled passage of barium through the
duodenum or vague visualization. Moreover, the use of sonography in
malrotation diagnosis often requires the opinion of experienced
radiologists, who may not always available at most centers
(10,11). Therefore, the diagnosis of
intestinal malrotation is often an intricate and complex process,
and a more effective and ideally non-invasive diagnostic method is
needed (6,11,12).
MicroRNAs (miRNAs) are a group of non-coding RNA
molecules, usually 19–25 nucleotides long, which are abundantly and
stably expressed in plasma and other bodily fluids (13,14).
Differential expression of specific miRNAs has been identified in
numerous diseases, and an increasing body of evidence indicates
that miRNAs could serve as promising biomarkers for diagnostic use
(15–17). For example, previous studies have
identified miRNAs associated with various types of cancer,
highlighting an opportunity to use these circulating
disease-related miRNAs as biomarkers (18,19).
In cardiovascular diseases, it was demonstrated that the combined
use of multiple miRNAs could improve the predictive efficiency of
traditional diagnostic methods (20,21).
Thus, understanding the potential role of miRNAs in intestinal
malrotation may provide invaluable insight into improved diagnostic
approaches, as demonstrated in other diseases (22–24).
Previously, a mutation in the forkhead box F1 gene
was demonstrated to be associated with intestinal malrotation
(25). However, to the best of the
authors' knowledge, no studies have evaluated epigenetic changes
during the pathogenesis of intestinal malrotation (26). In the present study, it was
hypothesized that the expression of specific miRNAs might be
dysregulated in newborns with intestinal malrotation. Thus, the aim
of the present study was to determine whether such differentially
expressed miRNAs could be used for improved diagnosis of intestinal
malrotation.
Materials and methods
Study design and sample
collection
Ten children with intestinal malrotation (age range,
5 days to month) and ten sex- and age-matched controls (age range,
4 days to 1 month) admitted to The Children's Hospital of Nanjing
Medical University (Nanjing, China) between February 2018 and July
2019 were enrolled in the present study, and their plasma samples
were collected prospectively. Children with immunological
disorders, cardiovascular diseases and other congenital digestive
tract abnormalities were excluded, as these pathological factors
can affect serum miRNA levels. Plasma samples were collected in a
plasma separator tube prior to any treatment and stored at −80°C
until use. The study was approved by the Institutional Ethics
Committee of The Children's Hospital of Nanjing Medical University
(approval no. 201701025). Written informed consent was obtained
from a parent of each patient.
RNA extraction
Total RNA was extracted from plasma samples using
TRIzol® reagent (Invitrogen; Thermo Fisher Scientific,
Inc.) according to the manufacturer's protocol. In addition, 5 µl
of 200 nM cel-miR-39 (Guangzhou RiboBio Co., Ltd.) was added to
each sample to serve as an external control (27). RNA concentration and quality was
assessed using a NanoDrop 2000 spectrophotometer (Thermo Fisher
Scientific, Inc.). RNA was stored at −80°C until use.
Illumina HiSeq sequencing
A total of six plasma samples (three patients with
intestinal malrotation and three controls) were used for
sequencing. miRNA-seq library was constructed using NEBNext Small
RNA kit (NEB, cat. no. E7300S). DNA integrity was measure using an
Agilent 2100 Bioanalyzer with the Agilent DNA 1000 kit (Agilent
Technologies, Inc.; cat. no. 5067-1504). Sequencing was performed
on the Illumina HiseqX platform (Illumina, Inc.; 150 cycles;
paired-end). HiSeq X Ten Reagent kit v2.5 (Illumina, Inc.; cat. no.
FC-501-25) was used for sequencing. The concentration of DNA was
30–40 nM, which was measured by real-time PCR. Ligation of 5′ and
3′ adaptors was carried out following manufacturer's instructions.
Small RNAs were amplified by PCR (17 cycles) using adaptor-specific
primers according to the manufacturer's protocol The PCR products
(fragments of ~90 bp) were purified by 8% PAGE. The size
distribution of molecules in each sample were evaluated using an
Agilent 2100 Bioanalyzer. Subsequently, amplification of the
eligible RNAs was conducted to generate the cluster on the flow
cell, which was then sequenced using the HiSeq 2000 System (single
end; Illumina, Inc.), following the manufacturer's instructions.
miRNAs were considered to be significantly differentially expressed
if P<0.05 and log2 (fold-change) ≥8 for upregulated
miRNAs, or log2 (fold-change) ≤-8 for downregulated
miRNAs in the intestinal malrotation group, compared with the
control group. These criteria applied to the average of the three
samples.
Gene Ontology (GO) and Kyoto
Encyclopedia of Genes and Genomes (KEGG) pathway enrichment
analysis
GO functional enrichment analysis (http://geneontology.org/docs/go-enrichment-analysis/)
and KEGG pathway enrichment analysis (http://www.genome.jp/kegg/pathway.html) of DEGs were
performed using DIANA TOOLS MirPath version 3 (http://diana.imis.athena-innovation.gr/DianaTools/index.php).
GO has three functional categories: Molecular function (MF);
biological process (BP); and cellular component (CC). P<0.05 was
considered as a statistically significant difference.
Quantification of plasma miRNA levels
using reverse transcription-quantitative PCR (RT-qPCR)
Total RNA extracted from 20 plasma samples (10
patients with intestinal malrotation and 10 controls) was reverse
transcribed to cDNA using the PrimeScript™ RT reagent kit (Takara
Bio, Inc.), according to the manufacturer's instructions. RT-qPCRs
were carried out using SYBR Premix Ex Taq (Takara Biotechnology
Co., Ltd.) on a Light Cycler 480 (Roche Diagnostics) to measure
miRNA expression levels. A total of 18 miRNA candidates (15
upregulated and three downregulated miRNAs in intestinal
malrotation) were selected for RT-qPCR analysis. Thermocycling
conditions consisted of an initial denaturation at 95°C for 10 min,
followed by 40 cycles at 94°C for 15 sec and 60°C for 1 min.
Relative expression values were normalized against the spike-in
cel-miR-39 and analyzed using the 2−ΔΔCq method
(28).
Statistical analysis
Statistical analysis was carried out using GraphPad
Prism 8.0 (GraphPad Software, Inc.) and SPSS 23.0 (IBM Corp.). A
two-sided unpaired t-test was used to compare differences in miRNA
expression between the control and intestinal malrotation groups.
Receiver operating curve (ROC) analysis was performed to determine
the area under the curve (AUC) of miRNA expression. SPSS 23.0 (IBM
Corp.) was used to construct and analyze the curves. The final
results were illustrated using GraphPad Prism 8.0 (GraphPad
Software, Inc.). P<0.05 was considered to indicate a
statistically significant difference.
Results
Identification of differentially
expressed serum miRNAs in intestinal malrotation
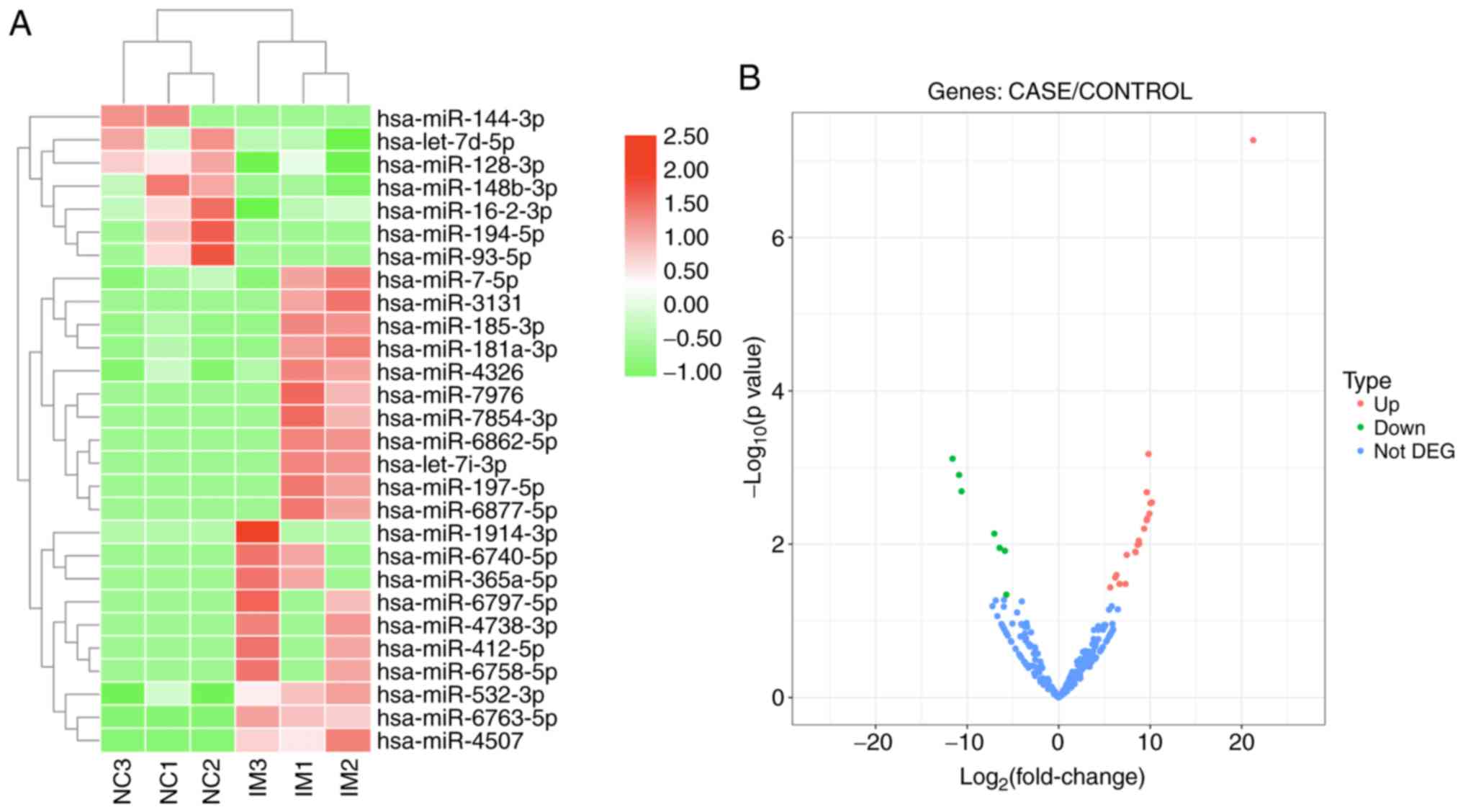
Serum miRNA levels were measured in six plasma
samples (three patients with intestinal malrotation and three
controls) using high-throughput sequencing. Overall, ~2,588 miRNAs
were identified. The profiles of differentially expressed plasma
miRNAs are presented as a heat map and a volcano plot in Fig. 1. Both the heat map and volcano plot
show that patients with intestinal malrotation and healthy controls
displayed markedly different plasma miRNA profiles. A total of 28
miRNAs exhibited significant differential expression, of which 21
were upregulated and 7 down regulated in patients with IM, compared
with controls (Table I).
 | Table I.Dysregulated miRNAs in plasma from
patients with intestinal malrotation and controls. |
Table I.
Dysregulated miRNAs in plasma from
patients with intestinal malrotation and controls.
| miR | log2
(FC) | P-value | Expression |
|---|
|
hsa-miR-1914-3p | 21.2605 | 0.00053635 | Upregulated |
|
hsa-miR-6763-5p | 9.8136 | 0.00066362 | Upregulated |
| hsa-miR-194-5p | −11.6088 | 0.00076538 | Downregulated |
| hsa-miR-144-3p | −10.8903 | 0.00124557 | Downregulated |
| hsa-miR-93-5p | −10.6228 | 0.00204004 | Downregulated |
| hsa-miR-185-3p | 9.6254 | 0.00209648 | Upregulated |
|
hsa-miR-4738-3p | 10.1860 | 0.00284375 | Upregulated |
| hsa-miR-3131 | 10.0151 | 0.00290713 | Upregulated |
|
hsa-miR-6797-5p | 9.9124 | 0.00399543 | Upregulated |
|
hsa-miR-6740-5p | 9.6671 | 0.00463324 | Upregulated |
| hsa-miR-412-5p | 9.6234 | 0.00487532 | Upregulated |
|
hsa-miR-6758-5p | 9.3378 | 0.00625270 | Upregulated |
|
hsa-miR-16-2-3p | −7.0390 | 0.00726665 | Downregulated |
|
hsa-miR-6862-5p | 8.7506 | 0.00897906 | Upregulated |
|
hsa-miR-365a-5p | 8.8099 | 0.00986631 | Upregulated |
| hsa-miR-197-5p | 8.6241 | 0.01019434 | Upregulated |
| hsa-let-7d-5p | −6.4675 | 0.01114899 | Downregulated |
|
hsa-miR-148b-3p | −5.8861 | 0.01219763 | Downregulated |
|
hsa-miR-6877-5p | 8.3920 | 0.01254641 | Upregulated |
| hsa-let-7i-3p | 8.3746 | 0.01255295 | Upregulated |
| hsa-miR-7976 | 8.4149 | 0.01268761 | Upregulated |
| hsa-miR-4507 | 7.4372 | 0.01375498 | Upregulated |
| hsa-miR-7-5p | 6.3143 | 0.02523047 | Upregulated |
| hsa-miR-4326 | 6.1695 | 0.02722018 | Upregulated |
|
hsa-miR-181a-3p | 6.6420 | 0.03291677 | Upregulated |
|
hsa-miR-7854-3p | 7.2962 | 0.03293265 | Upregulated |
| hsa-miR-532-3p | 5.6365 | 0.03647876 | Upregulated |
| hsa-miR-128-3p | −5.7314 | 0.04537403 | Downregulated |
Gene Ontology and Kyoto Encyclopedia
of Genes and Genomes (KEGG) pathway enrichment analysis
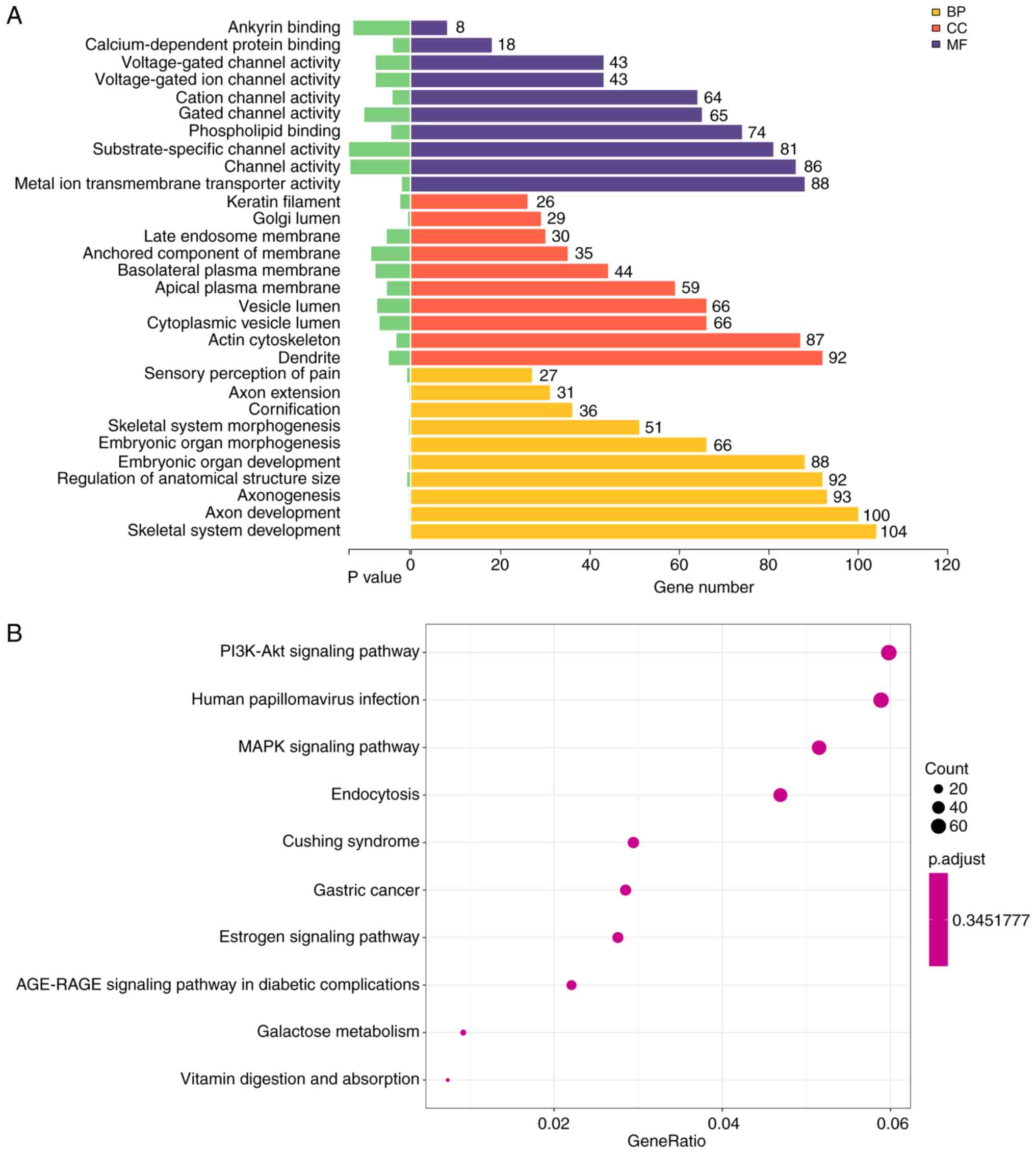
GO analysis suggested that the differentially
expressed miRNAs were mainly involved in involved in ‘skeletal
system development’, ‘axon development’ (Fig. 2A, Table II). These miRNAs were mainly
localized or exerted their functions in dendrites and the actin
cytoskeleton (Fig. 2A, Table III). Moreover, these miRNAs were
involved in ‘metal ion transmembrane transporter activity’,
‘channel activity’ and ‘substrate-specific channel activity’ and
other molecular functions (Fig.
2A; Table IV).
| Table II.Top 10 significantly enriched GO
biological processes. |
Table II.
Top 10 significantly enriched GO
biological processes.
| GO term | Description | P-value | Count |
|---|
| GO:0070268 | Cornification | 0.00000056 | 36 |
| GO:0001501 | Skeletal system
development | 0.00000277 | 104 |
| GO:0061564 | Axon
development | 0.00000467 | 100 |
| GO:0007409 | Axonogenesis | 0.00000507 | 93 |
| GO:0048562 | Embryonic organ
morphogenesis | 0.00000752 | 66 |
| GO:0048675 | Axon extension | 0.00000985 | 31 |
| GO:0048705 | Skeletal system
morphogenesis | 0.00002872 | 51 |
| GO:0048568 | Embryonic organ
development | 0.00002935 | 88 |
| GO:0090066 | Regulation of
anatomical structure size | 0.00009987 | 92 |
| GO:0019233 | Sensory perception
of pain | 0.00010642 | 27 |
| Table III.Top 10 significantly enriched GO
cellular components. |
Table III.
Top 10 significantly enriched GO
cellular components.
| GO term | Description | P-value | Count |
|---|
| GO:0005796 | Golgi lumen | 0.00007119 | 29 |
| GO:0045095 | Keratin
filament | 0.00038711 | 26 |
| GO:0015629 | Actin
cytoskeleton | 0.00054521 | 87 |
| GO:0030425 | Dendrite | 0.00086110 | 92 |
| GO:0016324 | Apical plasma
membrane | 0.00093914 | 59 |
| GO:0031902 | Late endosome
membrane | 0.00094567 | 30 |
| GO:0060205 | Cytoplasmic vesicle
lumen | 0.00123996 | 66 |
| GO:0031983 | Vesicle lumen | 0.00134049 | 66 |
| GO:0016323 | Basolateral plasma
membrane | 0.00140855 | 44 |
| GO:0031225 | Anchored component
of membrane | 0.00158692 | 35 |
| Table IV.Top 10 significantly enriched GO
molecular functions. |
Table IV.
Top 10 significantly enriched GO
molecular functions.
| GO term | Description | P-value | Count |
|---|
| GO:0046873 | Metal ion
transmembrane transporter activity | 0.00032224 | 88 |
| GO:0048306 | Calcium-dependent
protein binding | 0.00068622 | 18 |
| GO:0005261 | Cation channel
activity | 0.00070680 | 64 |
| GO:0005543 | Phospholipid
binding | 0.00075808 | 74 |
| GO:0005244 | Voltage-gated ion
channel activity | 0.00140047 | 43 |
| GO:0022832 | Voltage-gated
channel activity | 0.00140047 | 43 |
| GO:0022836 | Gated channel
activity | 0.00187551 | 65 |
| GO:0030506 | Ankyrin
binding | 0.00233200 | 8 |
| GO:0015267 | Channel
activity | 0.00245557 | 86 |
| GO:0022838 | Substrate-specific
channel activity | 0.00251147 | 81 |
KEGG pathway analysis identified 58 significantly
enriched pathways in the sequenced miRNAs. The 10 most enriched
pathway terms were ‘PI3K-Akt signaling pathway’, ‘human
papillomavirus infection’, ‘MAPK signaling pathway’, ‘endocytosis’,
‘Cushing syndrome’, ‘gastric cancer’, ‘estrogen signaling pathway’,
‘AGE-RAGE signaling pathway in diabetic complications’, ‘galactose
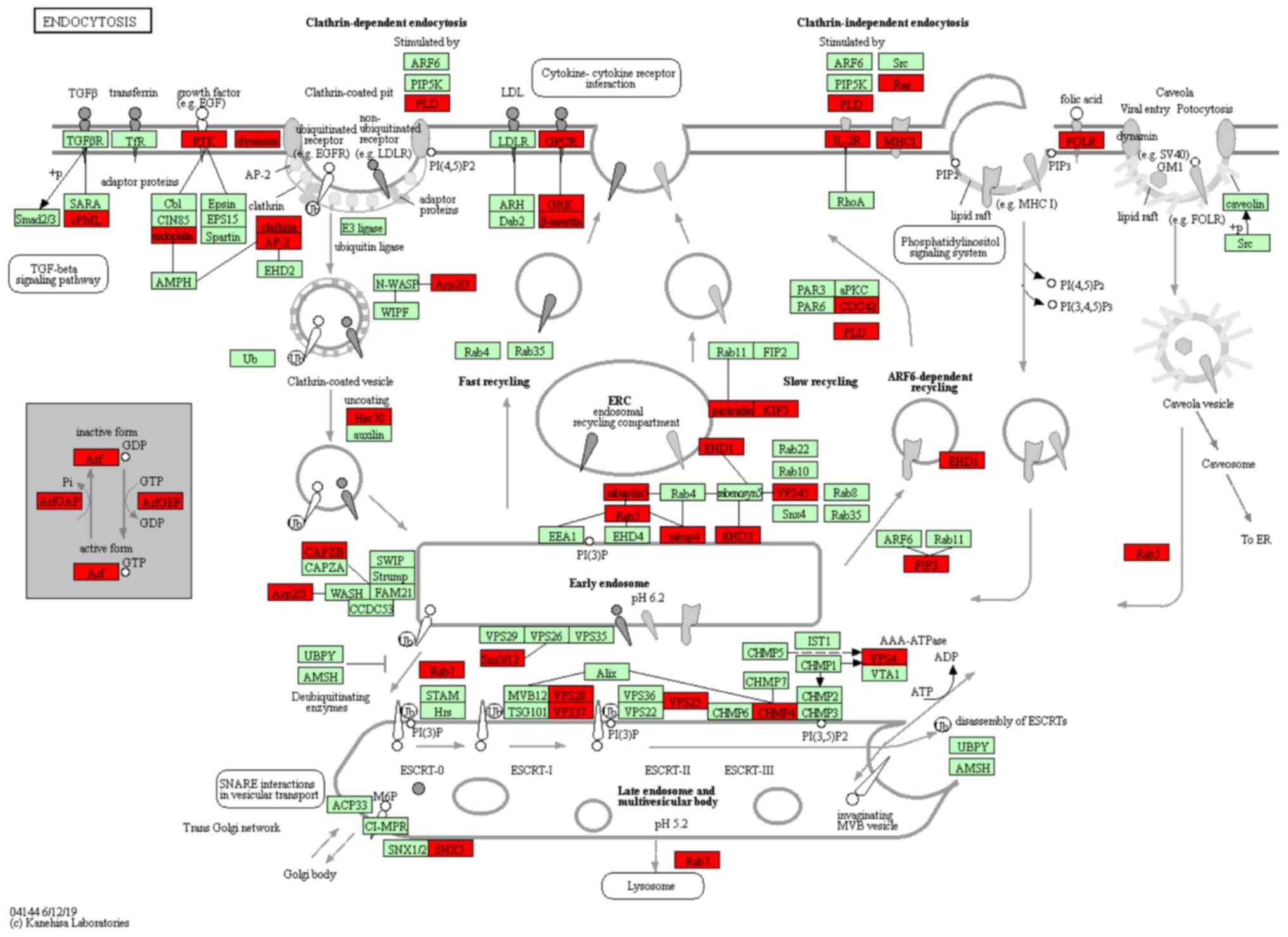
metabolism’ and ‘vitamin digestion and absorption’ (Fig. 2B). The most significant KEGG
pathway was ‘Endocytosis’ (KEGG ID, hsa04144), which involved 51
target genes (P=001; Table V). The
network associated was analyzed, which demonstrated TGF-β signaling
pathway and endosomal recycling compartment were mainly affected
(Fig. 3). Thus, GO and KEGG
analysis provided novel insights into the underlying mechanism by
which plasma miRNAs might participate in the pathogenesis of
intestinal malrotation.
| Table V.Top 10 significantly enriched KEGG
pathways. |
Table V.
Top 10 significantly enriched KEGG
pathways.
| KEGG pathway | Description | P-value | Count |
|---|
| hsa04144 | Endocytosis | 0.00132301 | 51 |
| hsa05165 | Human
papillomavirus infection | 0.00253633 | 64 |
| hsa04933 | AGE-RAGE signaling
pathway in diabetic complications | 0.00411644 | 24 |
| hsa04915 | Estrogen signaling
pathway | 0.00688242 | 30 |
| hsa00052 | Galactose
metabolism | 0.00689000 | 10 |
| hsa04010 | MAPK signaling
pathway | 0.00724133 | 56 |
| hsa04151 | PI3K-Akt signaling
pathway | 0.00865405 | 65 |
| hsa05226 | Gastric cancer | 0.01159650 | 31 |
| hsa04934 | Cushing
syndrome | 0.01168848 | 32 |
| hsa04977 | Vitamin digestion
and absorption | 0.01228429 | 8 |
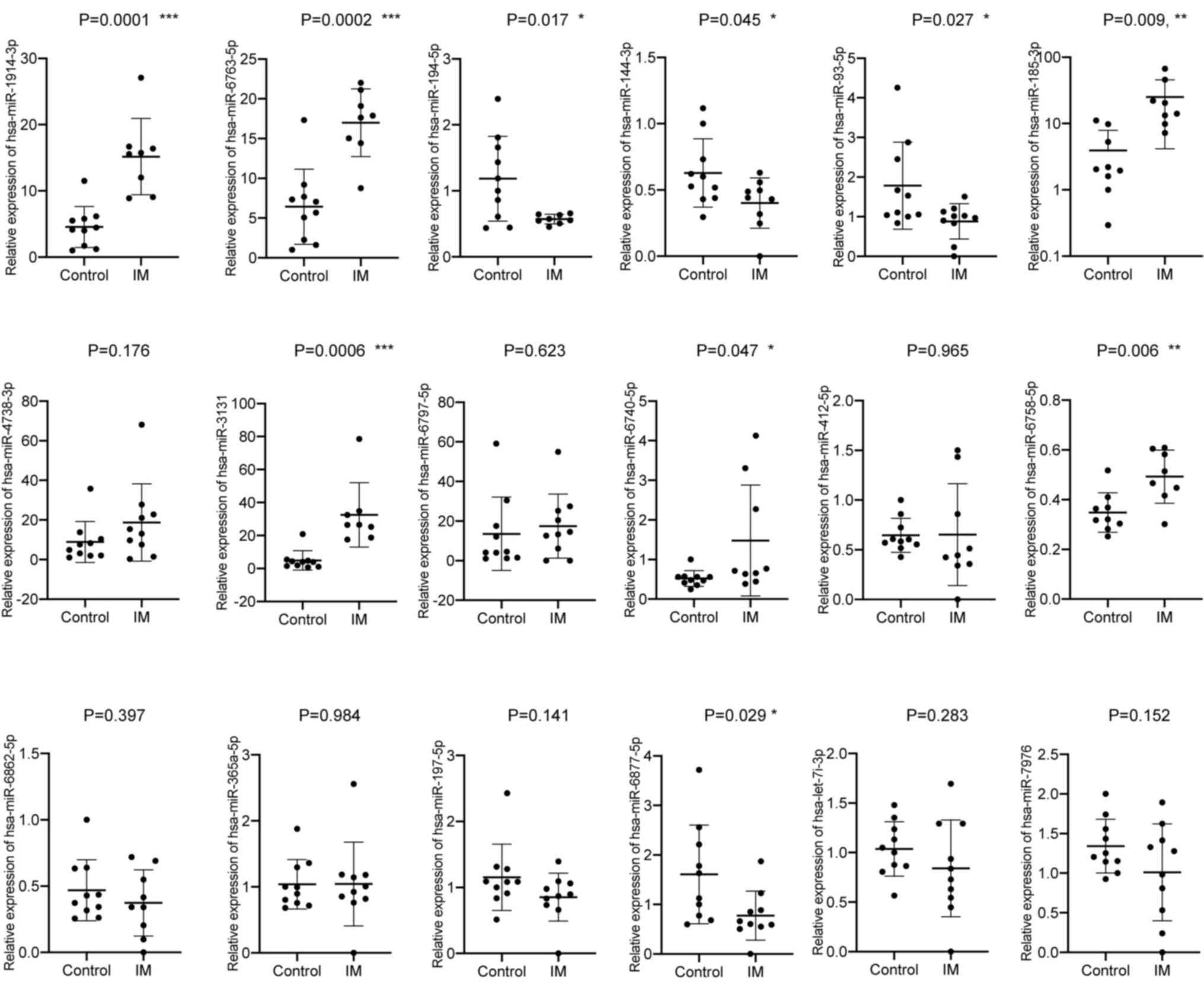
Selection and validation of potential
plasma miRNA biomarkers for intestinal malrotation
A total of 18 miRNAs were differentially expressed.
Of these, 15 miRNAs were upregulated, including, hsa-miR-1914-3p,
miR-6763-5p, miR-185-3p, miR-4738-3p, miR-3131, miR-6797-5p,
miR-6740-5p, miR-412-5p, miR-6758-5p, miR-6862-5p, miR-365a-5p,
miR-197-5p, miR-6877-5p, let-7 and miR-7976. Moreover, three were
downregulated, hsa-miR-194-5p, −144-3p and −93-5p (Table I) and were selected for further
validation. The expression levels of all 18 candidates were
measured in a larger sample size (10 patients with intestinal
malrotation and 10 controls) by RT-qPCR. In total, nine miRNAs were
confirmed to be differentially expressed. Of these, six were
upregulated, compared with the control group, including
hsa-miR-1914-3p, −6763-5p, −185-3p, −3131, −6740-5p and −6758-5p.
In addition, three were downregulated, hsa-miR-194-5p, −144-3p and
−93-5p (Fig. 4; Table VI).
| Table VI.Relative expression of nine candidate
miRNAs validated by reverse transcription-quantitative PCR from
patients with IM and controls. |
Table VI.
Relative expression of nine candidate
miRNAs validated by reverse transcription-quantitative PCR from
patients with IM and controls.
| miRNA | Controls | Patients with
IM | P-value | Fold change |
|---|
| miR-1914-3p | 4.552 | 15.17 | 0.0001c | 3.333 |
| miR-6763-5p | 6.422 | 16.99 | 0.0002c | 2.646 |
| miR-185-3p | 3.923 | 25.02 | 0.0092b | 6.378 |
| miR-3131 | 4.868 | 32.54 | 0.0006c | 6.684 |
| miR-194-5p | 1.183 | 0.571 | 0.0170a | 0.483 |
| miR-6740-5p | 0.522 | 1.479 | 0.0470a | 2.833 |
| miR-144-3p | 0.628 | 0.401 | 0.0449a | 0.639 |
| miR-6758-5p | 0.349 | 0.493 | 0.0061b | 1.413 |
| miR-93-5p | 1.783 | 0.881 | 0.0272a | 0.494 |
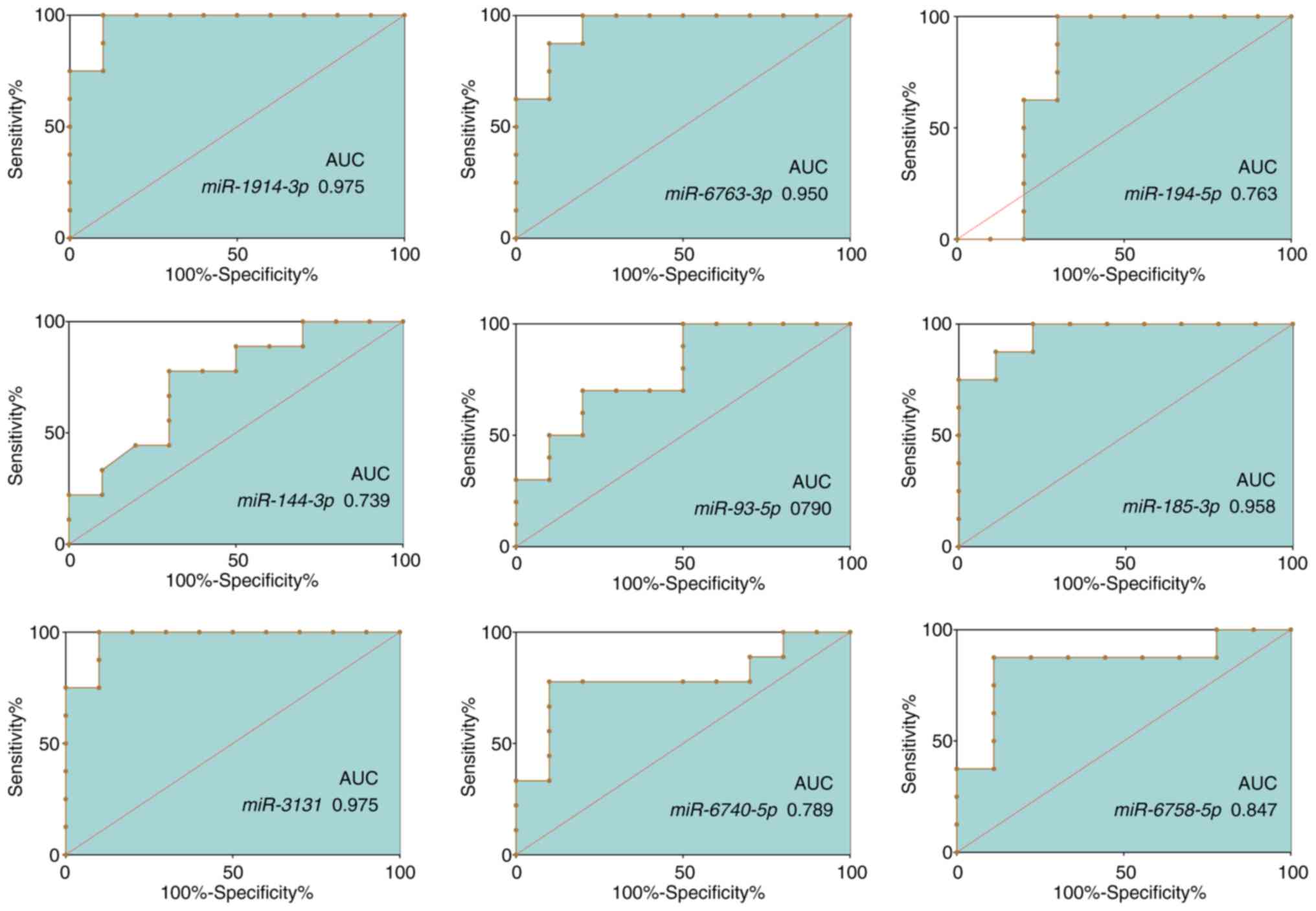
ROC curve analysis
The sensitivity and specificity of the
aforementioned 9 miRNAs as potential diagnostic biomarkers of
intestinal malrotation were determined using ROC curve analysis.
The AUCs of these miRNAs ranged from 0.727-0.975 (Fig. 5; Table VII). MiR-1914-3p (AUC, 0.975; 95%
CI, 0.913-1.000) and miR-3131 (AUC, 0.975; 95% CI, 0.913-1.000)
presented the largest AUCs, followed by miR-185-3p (AUC, 0.958; 95%
CI, 0.873-1.000) and miR-6763-5p (AUC, 0.950; 95% CI,
0.856-1.000).
| Table VII.The respective AUCs of nine candidate
miRNAs. |
Table VII.
The respective AUCs of nine candidate
miRNAs.
| miRNA | AUC | Standard error | Asymptotic
significance | Asymptotic 95%
CI |
|---|
| miR-1914-3p | 0.975 | 0.032 | <0.001 | 0.913-1.000 |
| miR-6763-5p | 0.950 | 0.048 | 0.001 | 0.856-1.000 |
| miR-185-3p | 0.958 | 0.044 | 0.002 | 0.873-1.000 |
| miR-3131 | 0.975 | 0.032 | <0.001 | 0.913-1.000 |
| miR-194-5p | 0.763 | 0.128 | 0.062 | 0.512-1.000 |
| miR-6740-5p | 0.789 | 0.115 | 0.034 | 0.564-1.000 |
| miR-144-3p | 0.739 | 0.116 | 0.079 | 0.512-0.966 |
| miR-6758-5p | 0.847 | 0.106 | 0.016 | 0.639-1.000 |
| miR-93-5p | 0.790 | 0.102 | 0.028 | 0.590-0.991 |
Discussion
Malrotation is a congenital abnormal bowel position
within the peritoneal cavity that usually involves both the small
and the large bowel (29). The
term malrotation encompasses a wide range of rotational and
fixation abnormalities of the intestines, from readily apparent
omphaloceles in newborns to asymptomatic non-rotation in adults
(1). Congenital intestinal
non-rotation and incomplete rotation usually concur with a narrow
base of the mesentery, which might cause duodenal obstruction and
midgut volvulus and manifest as acute symptoms (30). Pediatric patients who do not
present acute symptoms but are not diagnosed before adulthood are
at risk of developing various chronic symptoms later in life,
including vomiting, vague abdominal pain, diarrhea, nausea, early
satiety and bloating, dyspepsia and other functional or psychiatric
disorders (31,32).
Approximately 90% of infants with intestinal
malrotation are diagnosed within the first year of life, and ~80%
within the first month (33).
Common diagnostic tools include UGI, ultrasonography, and barium
enema. Although the duodenojejunal junction is usually fixed at the
Treitz ligament and functions as a useful landmark, in some cases
UGI results may be confusing or hard to interpret, and diagnosis of
these cases of malrotation depends on the recognition of anatomic
subtleties (8,34). Both false positive and false
negative findings have been reported (7,8,35,36).
Barium enema can help to some extent in some cases, but challenges
exist in terms of the quantity of barium administered to children
and the observation of the first pass of barium through the
duodenum (5). Moreover, the
interpretation of ultrasonographical findings can be very
subjective, and the presence of an experienced radiologist or
technician, who may not always be available at every hospital or
medical center, is essential (10).
In the present study, potential diagnostic
biomarkers were identified by analyzing plasma miRNA levels in
pediatric patients with intestinal malrotation. A profile of
differentially expressed miRNAs in the plasma of intestinal
malrotation patients was obtained by sequencing plasma miRNAs, and
a number of differentially expressed miRNAs were identified,
including 21 upregulated and seven downregulated miRNAs.
Subsequently, bioinformatics analyses were carried out to
investigate the potential involvement of differentially expressed
miRNAs in intestinal malrotation.
GO enrichment analysis suggested that these miRNAs
were mainly involved in ‘metal ion transmembrane transporter
activity’, ‘calcium-dependent protein binding’, ‘cation channel
activity’ and ‘phospholipid binding’. ‘Metal ion transmembrane
transporter activity’ and ‘calcium-dependent protein binding’ were
the most significantly enriched GO terms with respect to molecular
function. Interestingly, it was previously reported that calcium
channel-blocking drugs could lead to many developmental
abnormalities in Xenopus embryos, including malrotation of
the gut, possibly through dysregulation of calcium ion antagonism
(37). However, the potential link
between plasma miRNA levels and calcium ion antagonism in
intestinal malrotation requires further study to determine where
and how plasma miRNAs interfere with calcium ion. ‘Cornification’
was the most significantly enriched GO term with respect to
biological processes, followed by ‘skeletal system development
cornification’. A previous study reported a higher frequency of
malformations in the skeleton system, including the facial
skeleton, the small pelvis, and the upper and lower extremities,
among pediatric patients with intestinal malrotation (38). The present results indicated that
plasma miRNAs might play a role in this association. The most
enriched KEGG pathway was ‘endocytosis’, which is a critical
process in the intestine that is responsible for the endocytic
uptake of macromolecules from the gut lumen. For instance, but its
role in intestinal malrotation has not yet been studied (39,40).
miRNAs have been demonstrated to play a variety of
roles in numerous intestinal diseases and several could even
function as biomarkers (41–43).
Another important finding of the present study was that plasma
miRNAs have the potential to serve as circulating biomarkers for
intestinal malrotation. Based on the sequencing data and validation
by RT-qPCR in a larger number of samples, nine miRNAs were
differentially expressed, including six upregulated miRNAs
(hsa-miR-1914-3p, −6763-5p, −185-3p, −3131, −6740-5p and −6758-5p)
and three downregulated miRNAs (hsa-miR-194-5p, −144-3p and
−93-5p). The highest AUCs were obtained for miR-1914-3p, −3131,
−185-3p and −6763-5p, suggesting that these miRNAs may serve as
diagnostic biomarkers for intestinal malrotation. As a following
step, studies with larger sample sizes are necessary to validate
the present findings.
In conclusion, a profile of differentially expressed
miRNAs in the plasma of patients with intestinal malrotation was
identified, and the potential molecular functions associated with
these miRNAs were described. Four of the nine confirmed
differentially expressed miRNAs have the potential to improve early
diagnosis of intestinal malrotation. However, these miRNAs
exhibited relatively small 95% CIs, which is a great limitation to
our study and requires further confirmation in the future with much
larger sample size. These results also suggested that plasma miRNAs
play an important role in intestinal malrotation, although this
hypothesis requires further investigation.
Acknowledgements
Not applicable.
Funding
This work was funded by The Natural Science
Foundation of China (grant no. NSFC 81701493) and The Nanjing
Science and Technology Development Project (grant no.
201723006).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XL, HL and CL designed the study. HC and XS
collected the samples and conducted the sequencing. XL and LZ
carried out the PCRs and ROC analysis. XL contributed to writing
the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This study was approved by The Institutional Ethics
Committee of The Children's Hospital of Nanjing Medical University
(approval no. 201701025). Written informed consent was obtained
from a parent of each enrolled patient.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Applegate KE, Anderson JM and Klatte EC:
Intestinal malrotation in children: A problem-solving approach to
the upper gastrointestinal series. Radiographics. 26:3289–1500.
2006. View Article : Google Scholar
|
|
2
|
Blumberg K: Intestinal malrotation.
Radiology. 202:5841997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Coste AH, Waheed A and Ahmad H: Midgut
Volvulus. StatPearls Publishing; Treasure Island, FL: 2019
|
|
4
|
Adams SD and Stanton MP: Malrotation and
intestinal atresias. Early Hum Dev. 90:921–925. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Morris G, Kennedy A Jr and Cochran W:
Small bowel congenital anomalies: A review and update. Curr
Gastroenterol Rep. 18:162016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Graziano K, Islam S, Dasgupta R, Lopez ME,
Austin M, Chen LE, Goldin A, Downard CD, Renaud E and Abdullah F:
Asymptomatic malrotation: Diagnosis and surgical management: An
American Pediatric Surgical Association outcomes and evidence based
practice committee systematic review. J Pediatr Surg. 50:1783–1790.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dilley AV, Pereira J, Shi EC, Adams S,
Kern IB, Currie B and Henry GM: The radiologist says malrotation:
Does the surgeon operate? Pediatr Surg Int. 16:45–49. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Long FR, Kramer SS, Markowitz RI, Taylor
GE and Liacouras CA: Intestinal malrotation in children: Tutorial
on radiographic diagnosis in difficult cases. Radiology.
198:775–780. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Strouse PJ: Malrotation. Semin Roentgenol.
43:7–14. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Taylor GA: CT appearance of the duodenum
and mesenteric vessels in children with normal and abnormal bowel
rotation. Pediatr Radiol. 41:1378–1383. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tackett JJ, Muise ED and Cowles RA:
Malrotation: Current strategies navigating the radiologic diagnosis
of a surgical emergency. World J Radiol. 6:730–736. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dekonenko C, Sujka JA, Weaver K, Sharp SW,
Gonzalez K and St Peter SD: The identification and treatment of
intestinal malrotation in older children. Pediatr Surg Int.
35:665–671. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kroh EM, Parkin RK, Mitchell PS and Tewari
M: Analysis of circulating microRNA biomarkers in plasma and serum
using quantitative reverse transcription-PCR (qRT-PCR). Methods.
50:298–301. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Patel M, Verma A, Aslam I, Pringle H and
Singh B: Novel plasma microRNA biomarkers for the identification of
colitis-associated carcinoma. Lancet. 385 (Suppl 1):S782015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
van de Vrie M, Deegens JK, Eikmans M, van
der Vlag J and Hilbrands LB: Urinary MicroRNA as biomarker in renal
transplantation. Am J Transplant. 17:1160–1166. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Panico C and Condorelli G: microRNA-132: A
new biomarker of heart failure at last? Eur J Heart Fail. 20:86–88.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liu R, Chen X, Du Y, Yao W, Shen L, Wang
C, Hu Z, Zhuang R, Ning G, Zhang C, et al: Serum microRNA
expression profile as a biomarker in the diagnosis and prognosis of
pancreatic cancer. Clin Chem. 58:610–618. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
McGuire A, Brown JA and Kerin MJ:
Metastatic breast cancer: The potential of miRNA for diagnosis and
treatment monitoring. Cancer Metastasis Rev. 34:145–155. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fabris L, Ceder Y, Chinnaiyan AM, Jenster
GW, Sorensen KD, Tomlins S, Visakorpi T and Calin GA: The potential
of microRNAs as prostate cancer biomarkers. Eur Urol. 70:312–322.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zampetaki A, Willeit P, Tilling L, Drozdov
I, Prokopi M, Renard JM, Mayr A, Weger S, Schett G, Shah A, et al:
Prospective study on circulating microRNAs and risk of myocardial
infarction. J Am Coll Cardiol. 60:290–299. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Barwari T, Joshi A and Mayr M: MicroRNAs
in cardiovascular disease. J Am Coll Cardiol. 68:2577–2584. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lu TX and Rothenberg ME: MicroRNA. J
Allergy Clin Immunol. 141:1202–1207. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kumar S, Vijayan M, Bhatti JS and Reddy
PH: MicroRNAs as peripheral biomarkers in aging and age-related
diseases. Prog Mol Biol Transl Sci. 146:47–94. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Backes C, Meese E and Keller A: Specific
miRNA disease biomarkers in blood, serum and plasma: Challenges and
prospects. Mol Diagn Ther. 20:509–518. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Miranda J, Rocha G, Soares P, Morgado H,
Baptista MJ, Azevedo I, Fernandes S, Brandão O, Sen P and Guimarães
H: A novel mutation in FOXF1 gene associated with alveolar
capillary dysplasia with misalignment of pulmonary veins,
intestinal malrotation and annular pancreas. Neonatology.
103:241–245. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Martin V and Shaw-Smith C: Review of
genetic factors in intestinal malrotation. Pediatr Surg Int.
26:769–781. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sohn W, Kim J, Kang SH, Yang SR, Cho JY,
Cho HC, Shim SG and Paik YH: Serum exosomal microRNAs as novel
biomarkers for hepatocellular carcinoma. Exp Mol Med. 47:e1842015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Powell DM, Othersen HB and Smith CD:
Malrotation of the intestines in children: The effect of age on
presentation and therapy. J Pediatr Surg. 24:777–780. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gross E, Chen MK and Lobe TE: Laparoscopic
evaluation and treatment of intestinal malrotation in infants. Surg
Endosc. 10:936–937. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Durkin ET, Lund DP, Shaaban AF, Schurr MJ
and Weber SM: Age-related differences in diagnosis and morbidity of
intestinal malrotation. J Am Coll Surg. 206:658–663. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lin JN, Lou CC and Wang KL: Intestinal
malrotation and midgut volvulus: A 15-year review. J Formos Med
Assoc. 94:178–181. 1995.PubMed/NCBI
|
|
33
|
Hwang SM, Na YS, Cho Y, You DG and Lee JJ:
Midgut volvulus as a complication of intestinal malrotation in a
term pregnancy. Korean J Anesthesiol. 67 (Suppl):S98–S99. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Beasley SW and de Campo JF: Pitfalls in
the radiological diagnosis of malrotation. Australas Radiol.
31:376–383. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Prasil P, Flageole H, Shaw KS, Nguyen LT,
Youssef S and Laberge JM: Should malrotation in children be treated
differently according to age? J Pediatr Surg. 35:756–758. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Torres AM and Ziegler MM: Malrotation of
the intestine. World J Surg. 17:326–331. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Burgess AM and Vere DW: Teratogenic
effects of some calcium channel blocking agents in Xenopus embryos.
Pharmacol Toxicol. 64:78–82. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Botvin'ev OK, Eremeeva AV, Razumovskaia IN
and Kondrikova EV: Intestinal malrotation: Genetics features and
other congenital malformations in children. Arkh Patol. 73:29–32.
2011.(In Russian).
|
|
39
|
Haq S, Grondin J, Banskota S and Khan WI:
Autophagy: Roles in intestinal mucosal homeostasis and
inflammation. J Biomed Sci. 26:192019. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Bujko A, Atlasy N, Landsverk OJB, Richter
L, Yaqub S, Horneland R, Øyen O, Aandahl EM, Aabakken L,
Stunnenberg HG, et al: Transcriptional and functional profiling
defines human small intestinal macrophage subsets. J Exp Med.
215:441–458. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yoshikawa T, Wu J, Otsuka M, Kishikawa T,
Suzuki N, Takata A, Ohno M, Ishibashi R, Yamagami M, Nakagawa R, et
al: Repression of microRNA function mediates
inflammation-associated colon tumorigenesis. Gastroenterology.
152:631–643. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Xiao L, Wu J and Wang JY, Chung HK,
Kalakonda S, Rao JN, Gorospe M and Wang JY: Long noncoding RNA
uc.173 promotes renewal of the intestinal mucosa by inducing
degradation of microRNA 195. Gastroenterology. 154:599–611. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cao B, Zhou X, Ma J, Zhou W, Yang W, Fan D
and Hong L: Role of miRNAs in inflammatory bowel disease. Dig Dis
Sci. 62:1426–1438. 2017. View Article : Google Scholar : PubMed/NCBI
|