Recurrent pregnancy loss (RPL) is usually
characterized as ≥3 miscarriages before 20 weeks of gestation, but
an increasing number of researchers describe it as ≥2 spontaneous
abortions (1). The etiology of RPL
is multifactorial (2), including
chromosomal abnormalities, genetic issues (3), congenital uterine defects, acquired or
hereditary thrombotic diseases, endocrine issues, infections,
autoimmune diseases and male factors (4). However, ~50% of patients with RPL do
not have a definite etiology (5).
Patients with RPL may also have autoimmune abnormalities or
alloimmune problems (2). The former
mainly includes antiphospholipid antibodies (APAs) (6), antithyroid antibodies (7) and antinuclear antibodies (ANAs)
(8,9), while the latter mainly refers to
cellular immune problems, such as increased natural killer (NK)
cells (10–12) or decreased inhibitory T cells
(13). Therefore, the success of
pregnancy depends to a large degree on the development of an
appropriate immune response (14).
It has been suggested that in patients, RPL, is
largely associated with immune abnormalities (14), thereby contributing to the
development and use of different forms of immunomodulatory
therapies (1). Prednisone has been
reported to help women who have multiple consecutive abortions by
reducing inflammation and inhibiting the function of multiples
types of immune cells, including T cells (15,16).
Moreover, plaquenil can be useful in the treatment of RPL as a drug
with comprehensive protection identified during pregnancy (17). The therapeutic role of plaquenil is
associated with pharmacological properties, such as antithrombotic
activity, vascular defense, immunomodulation, improved glucose
resistance, hypolipidemic activity and anti-infection function
(17). Several studies have
revealed that intravenous immunoglobulin modulated immune
dysfunction and contributed to positive pregnancy outcomes in women
with RPL, although controversial results have been reported
(18–23).
In humans, vitamin D is involved in the metabolism
of numerous elements, such as calcium and phosphorus (24). Vitamin D is a crucial modulator of
essential biological effects, such as immune function and hormone
secretion via the vitamin D receptor (VDR) (25). Vitamin D affects the innate and
acquired immune response (26), as
well as exerts an inhibitory function on the adaptive immune system
(27). In comparison, it inhibits T
helper (Th)1 cytokines (such as IFN-γ), and promotes the response
of Th2 by both downregulating IFN-γ and upregulating IL-4 (26). As VDR is expressed in the placenta,
and it has been suggested that vitamin D has a major function on
the mechanism of immunomodulation at the maternal-fetal interface
(28). In the clinical setting,
multiple patients with RPL have vitamin D deficiency (VDD)
(29). As a result, these women
have impaired cellular immune systems, including elevated
peripheral NK levels, NK cytotoxicity and higher Th1/Th2 ratios
(30–32). Moreover, women with low vitamin D
(VDL) levels are more susceptible to autoimmune defects (29). For example, the decreased expression
of vitamin D is associated with a higher occurrence of APAs, ANAs,
anti-single stranded DNA and thyroid peroxidase antibodies
(anti-TPO) in patients with RPL (27).
As an autoimmune disease, APS is closely associated
with adverse obstetrical outcomes (32,35).
APS is a systemic autoimmune disease characterized by thrombosis
(36). It has been well documented
that the increased susceptibility to the thrombosis of blood
vessels in APS may lead to microvascular thrombus in the placenta,
as well as the reduction of blood flow at the maternal-fetal
interface (6,37). A significant crosstalk between
inflammation and coagulation involves the complement system and
tissue factor (TF), and both mice and humans experience APS-related
pregnancy complications (38–40).
As aforementioned, complement activation serves a
critical function in adverse outcomes of pregnancy, including RPL
with APS in both mice and humans (41–46).
Vitamin D can enhance the level of complement inhibitor CD55 in
human monocytes (47). Moreover,
the related inhibitory effect of complement activation can prevent
preterm birth observed in APS (47). In patients with APS, vitamin D
exerts a suppressive effect on anti-β2 glycoprotein expression,
thus decreasing the risk of thrombosis (48,49).
Furthermore, as shown in in vitro studies, APA-induced TF
expression was suppressed by vitamin D (36,48).
Another study reported that vitamin D regulated TF in vascular
smooth muscle cells (50). In
addition, abnormal TF/protease activated receptor 2 signaling was
considered to be involved in the pathogenesis of
pregnancy-associated complications, which included abortions in an
APS murine model (38). The
frequency of APS antibodies in women with RPL is 15–20% (51). Researchers have confirmed that VDD
in APS women with RPL was more common relative to normal controls
(49.5 vs. 30%; P<0.05) (48).
Additionally, women with VDD were found to have enhanced levels of
several autoantibodies, including APAs (29). The prevalence of total APA in women
with RPL was substantially increased in VDL relative to a normal
vitamin D (VDN) group (39.7 vs. 22.9%; P<0.05; odds ratio =
2.22; 95% CI, 1.0–4.7) (29). In
brief, VDD is more common in RPL cases with APS. Moreover, an
increased percentage of patients with RPL and VDD are at risk of
autoimmune abnormalities, including APS (29).
Accumulating evidence has suggested that thyroid
autoimmunity is the cause of miscarriage during pregnancy (52,53).
An increased morbidity of VDD was observed among patients with
AITDs, in particular, Hashimoto's thyroiditis (54). Although the mechanisms underlying
the relation between vitamin D and AITDs are not fully understood,
the causes may be associated with anti-inflammatory and
immunomodulatory functions (55).
An opposite relationship between vitamin D and anti-TPO levels has
been identified in women with AITD (56). Decreased levels of anti-TPO result
in lower incidence of preterm birth and reduced rates of pregnancy
loss (57). Antithyroid antibodies
are more prevalent in patients with VDD compared with those with
high levels of vitamin D (43 vs. 17%, respectively; P<0.001)
(54). Women with abnormal thyroid
autoantibodies also had lower levels of vitamin D compared with
healthy controls (54). Lower
thyroid stimulating hormone levels are directly associated with a
higher vitamin D level (54). Ozkan
et al (58) revealed that
25(OH)-D in follicular fluid could independently predict successful
pregnancy during the in vitro fertilization cycle. For women
whose vitamin D levels in follicular fluid were <10 ng/ml, the
presence of clinical pregnancy reduced significantly, while for
patients whose vitamin D levels in follicular fluid increased by 1
ng/ml, the rate of clinical pregnancy was enhanced by 6% (58). Moreover, vitamin D can activate HOX
genes, including HOXA10, which is essential for the process of
implantation (59).
Vitamin D suppresses the proliferation of Th1 cells
and restricts the secretion of cytokines, including IFN-γ, IL-2 and
TNF-α (29). Moreover, vitamin D
postpones subsequent antigen presentation and the accumulation of T
lymphocytes by suppressing the transcription of IFN-γ, which is the
main positive response symbol for antigen-presenting cells
(60). Vitamin D also prevents the
activation and spread of IL-2, which is the autocrine growth factor
for T lymphocytes (61). By
decreasing the synthesis of IL-2 and IFN-γ and inducing the
polarization of CD4+ T lymphocytes to a Th2 reaction, as
well as finally reducing the autoimmune response, vitamin D
increases the secretion of Th2 cytokines (62), including IL-4, IL-5, IL-6, IL-9,
IL-10 and IL-13 (63,64). In a trial with mice, there was an
increased accumulation of Th2 cells and higher counts of cytokines
(IL-4, IL-5 and IL-10) when 1,25(OH)2D3 was
administered (65). The
1,25(OH)2D3-related functions on the augment
of Th2 cells were mainly regulated via IL-4 (62). The phenomenon could also be
confirmed in the mouse model (66).
Excessive inflammatory response and lower levels of
vitamin D are found in women with RPL (67). As observed in a previous study,
patients with VDD showed an notable higher percentage of
TNF-α-secreting Th cells relative to individuals with normal
vitamin D levels (35.1±10.2 vs. 28.3±4.8%; P<0.05), whereas the
difference between vitamin D insufficient group (VDI) and VDN was
negligible (2). In women with
elevated vitamin D concentrations, the mean serum TNF-α was
substantially lower compared with those with low vitamin D
expression (0.79±0.11 vs. 1.22±0.11 pg/ml; P=0.02) (68).
Other studies have suggested that vitamin D could
exert a vital influence on preventing excessive adaptive immune
response among patients with RPL (2,29,69).
In one study, women with RPL were classified into three groups
based on vitamin D level in serum: VDN, VDI and VDD groups
(2). The definition of VDD was a
level of 25(OH)D at <20 ng/ml, and VDI was defined as levels
between 20–30 ng/ml, according to previously published literature
(70). In 35 VDI cases, 0.5 µg/day
1,25(OH)2D was applied for 2 months, and two patients
with VDD were treated with the same amount of
1,25(OH)2D. There was a substantial decrease in the
proportion of TNF-α-producing Th cells following treatment compared
with that observed before treatment, whereas there was no obvious
difference in the proportion of IFN-γ-producing Th cells between
pre- and post-treatment (2).
However, other research regarding CD4+ T cells in human
has indicated that 1,25(OH)2D could decrease both the
production of IFN-γ and the numbers of IFN-γ+
CD4+ T cells (71,72).
Decreased Treg cells and increased Th17 cells serve
a vital role in the pathogenesis of RPL (73). Due to VDD in pregnancy, the activity
of Treg cells is disrupted (74).
It has been reported that population of Treg cells was lower
(maternal, 0.2±0.01; cord, 0.63±0.03) in 25(OH)D3
deficient pregnant women (≤19 ng/ml; n=80) compared with
insufficient (20–29 ng/ml; n=55; maternal, 0.34±0.01; cord,
1.05±0.04) and sufficient (≥30 ng/ml; n=18; maternal, 0.45±0.02;
cord, 1.75±0.02) pregnant women (P<0.05) (74). When compared with insufficient and
sufficient vitamin D levels, TGF-β and IL-10 levels were decreased
in the 25(OH)D3 deficient pregnancy group (74). Other studies have revealed that 1,25
vitamin D treatment significantly augmented the percentage of Tregs
from baseline in the patients with RPL compared with the same
percentage in the control group (69,75,76).
Further research revealed an association between the
ratio of Treg/Th17 and vitamin D, as well as the impact on the
balance between Treg and Th17, among patients with RPL who were
given vitamin D (76). This study
found that the expression of vitamin D had a strong association
with the proportion of Treg cells, a negative association with the
proportion of Th17 cells and a positive association with the ratio
of Treg to Th17 in the RPL group (76). Moreover, the results were reversed
in the control group (76). It has
also been revealed that, relative to the control decidual tissues,
25(OH) D was significantly decreased among patients with RPL
(78). Furthermore, correlation
analysis indicated that there was a significantly negative
correlation between 25(OH) D and IL-23. On the contrary, IL-23
increased the expression of IL-17 (78). Vitamin D can also be a beneficial
medication by decreasing the amount of IL-23 (78). In addition, a study analyzing the
impact of women with RPL given vitamin D found that vitamin D could
decrease not only serum IL-23 but also the frequency of miscarriage
(79).
It has been reported that the levels of VEGF and
granulocyte colony-stimulating factor (G-CSF) can be induced by
vitamin D in NK cells (29). These
two factors may induce weak angiogenesis and complications of
pregnancy; for instance, in RPL, NK cells decrease the production
of VEGF at the maternal fetal interface (29). The receptor of G-CSF exists in the
trophoblast cells. It has been identified that G-CSF exerts
significant impacts on autocrine and paracrine activities in both
the decidua and placenta, and increased G-CSF markedly decreased
the risk of pregnancy loss in a human trial (81). Vitamin D could also be a possible
therapeutic alternative to avoid RPL by increasing the levels of
VEGF and G-CSF.
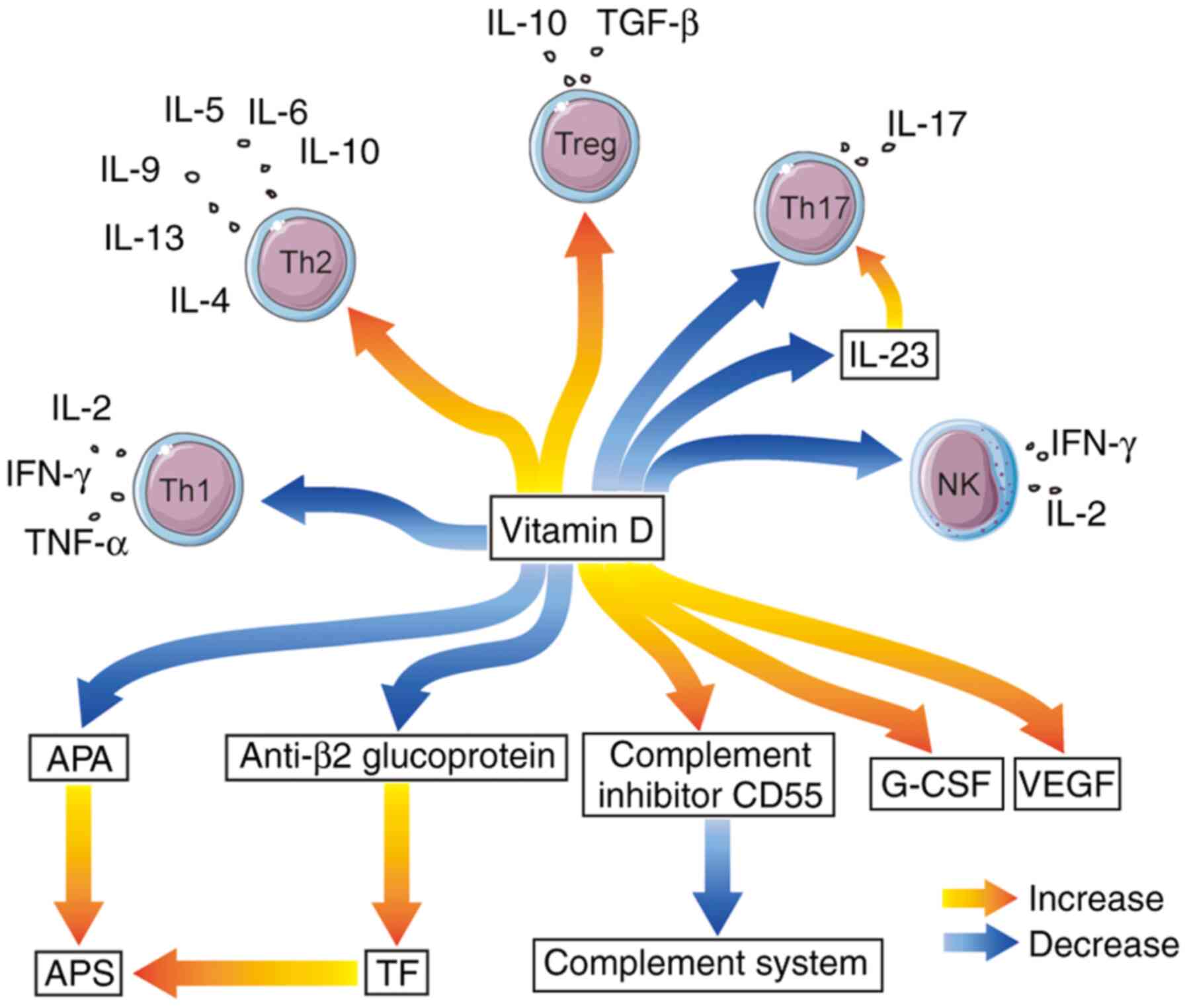
In conclusion, vitamin D can significantly affect
both autoimmunity and cellular immunity in RPL based on previously
published studies (Table I;
Fig. 1). Vitamin D is proposed to
be available as a potential therapy for RPL. For patients with RPL
or high risk factors, appropriate vitamin D supplement could be
given, and the serological level of vitamin D should be detected
regularly to obtain favorable maternal and fetal outcomes. In the
future, a larger multicenter, prospective controlled study with a
larger sample size is required.
Not applicable.
This manuscript was funded by Natural Science
Foundation of Liaoning Province (grant no. 2020-MS-167).
Not applicable.
HZ and XW wrote the manuscript, and XY revised this
manuscript. All authors read and approved the final version.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Muyayalo KP, Li ZH, Mor G and Liao AH:
Modulatory effect of intravenous immunoglobulin on Th17/Treg cell
balance in women with unexplained recurrent spontaneous abortion.
Am J Reprod Immunol. 80:e130182018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen X, Yin B, Lian RC, Zhang T, Zhang HZ,
Diao LH, Li YY, Huang CY, Liang DS and Zeng Y: Modulatory effects
of vitamin D on peripheral cellular immunity in patients with
recurrent miscarriage. Am J Reprod Immunol. 76:432–438. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang X, Yang E, Wang WJ, He Q, Jubiz G,
Katukurundage D, Dambaeva S, Beaman K and Kwak-Kim J: Decreased
HLA-C1 alleles in couples of KIR2DL2 positive women with recurrent
pregnancy loss. J Reprod Immunol. 142:1031862020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yan X, Wang L, Yan C, Zhang X, Hui L,
Sheng Q, Xue M and Yu X: Decreased expression of the vitamin D
receptor in women with recurrent pregnancy loss. Arch Biochem
Biophys. 606:128–133. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jeve YB and Davies W: Evidence-based
management of recurrent miscarriages. J Hum Reprod Sci. 7:159–169.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rand JH, Wu XX, Andree HA, Lockwood CJ,
Guller S, Scher J and Harpel PC: Pregnancy loss in the
antiphospholipid-antibody syndrome-a possible thrombogenic
mechanism. N Engl J Med. 337:154–160. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mecacci F, Parretti E, Cioni R, Lucchetti
R, Magrini A, La Torre P, Mignosa M, Acanfora L and Mello G:
Thyroid autoimmunity and its association with non-organ-specific
antibodies and subclinical alterations of thyroid function in women
with a history of pregnancy loss or preeclampsia. J Reprod Immunol.
46:39–50. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cavalcante MB, Cavalcante C, Sarno M, da
Silva ACB and Barini R: Antinuclear antibodies and recurrent
miscarriage: Systematic review and meta-analysis. Am J Reprod
Immunol. 83:e132152020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sakthiswary R, Rajalingam S, Norazman MR
and Hussein H: Antinuclear antibodies predict a higher number of
pregnancy loss in unexplained recurrent pregnancy loss. Clin Ter.
166:e98–e101. 2015.PubMed/NCBI
|
|
10
|
Kwak JY, Beaman KD, Gilman-Sachs A, Ruiz
JE, Schewitz D and Beer AE: Up-regulated expression of
CD56+, CD56+/CD16+, and
CD19+ cells in peripheral blood lymphocytes in pregnant
women with recurrent pregnancy losses. Am J Reprod Immunol.
34:93–99. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Aoki K, Kajiura S, Matsumoto Y, Ogasawara
M, Okada S, Yagami Y and Gleicher N: Preconceptional
natural-killer-cell activity as a predictor of miscarriage. Lancet.
345:1340–1342. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yougbaré I, Tai WS, Zdravic D, Oswald BE,
Lang S, Zhu G, Leong-Poi H, Qu D, Yu L, Dunk C, et al: Activated NK
cells cause placental dysfunction and miscarriages in fetal
alloimmune thrombocytopenia. Nat Commun. 8:2242017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sasaki Y, Sakai M, Miyazaki S, Higuma S,
Shiozaki A and Saito S: Decidual and peripheral blood
CD4+CD25+ regulatory T cells in early
pregnancy subjects and spontaneous abortion cases. Mol Hum Reprod.
10:347–353. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Stricker RB, Steinleitner A and Winger EE:
Intravenous immunoglobulin (IVIG) therapy for immunologic abortion.
Clin Appl Immunol Rev. 2:187–199. 2002. View Article : Google Scholar
|
|
15
|
Bansal AS, Bajardeen B and Thum MY: The
basis and value of currently used immunomodulatory therapies in
recurrent miscarriage. J Reprod Immunol. 93:41–51. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Novac N, Baus D, Dostert A and Heinzel T:
Competition between glucocorticoid receptor and NFkappaB for
control of the human FasL promoter. FASEB J. 20:1074–1081. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pasquier E, de Saint-Martin L, Marhic G,
Chauleur C, Bohec C, Bretelle F, Lejeune-Saada V, Hannigsberg J,
Plu-Bureau G, Cogulet V, et al: Hydroxychloroquine for prevention
of recurrent miscarriage: Study protocol for a multicentre
randomised placebo-controlled trial BBQ study. BMJ Open.
9:e0256492019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee SK, Kim JY, Han AR, Hur SE, Kim CJ,
Kim TH, Cho BR, Han JW, Han SG, Na BJ and Kwak-Kim J: Intravenous
immunoglobulin G improves pregnancy outcome in women with recurrent
pregnancy losses with cellular immune abnormalities. Am J Reprod
Immunol. 75:59–68. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim DJ, Lee SK, Kim JY, Na BJ, Hur SE, Lee
M and Kwak-Kim J: Intravenous immunoglobulin G modulates peripheral
blood Th17 and Foxp3(+) regulatory T cells in pregnant women with
recurrent pregnancy loss. Am J Reprod Immunol. 71:441–450. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kwak JY, Quilty EA, Gilman-Sachs A, Beaman
KD and Beer AE: Intravenous immunoglobulin infusion therapy in
women with recurrent spontaneous abortions of immune etiologies. J
Reprod Immunol. 28:175–188. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Han AR, Ahn H, Vu P, Park JC, Gilman-Sachs
A, Beaman K and Kwak-Kim J: Obstetrical outcome of
anti-inflammatory and anticoagulation therapy in women with
recurrent pregnancy loss or unexplained infertility. Am J Reprod
Immunol. 68:418–427. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schwab I and Nimmerjahn F: Intravenous
immunoglobulin therapy: How does IgG modulate the immune system?
Nat Rev Immunol. 13:176–189. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hutton B, Sharma R, Fergusson D, Tinmouth
A, Hebert P, Jamieson J and Walker M: Use of intravenous
immunoglobulin for treatment of recurrent miscarriage: A systematic
review. BJOG. 114:134–142. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Panda DK, Miao D, Tremblay ML, Sirois J,
Farookhi R, Hendy GN and Goltzman D: Targeted ablation of the
25-hydroxyvitamin D 1alpha-hydroxylase enzyme: Evidence for
skeletal, reproductive, and immune dysfunction. Proc Natl Acad Sci
USA. 98:7498–7503. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Brannon PM: Vitamin D and adverse
pregnancy outcomes: Beyond bone health and growth. Proc Nutr Soc.
71:205–212. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mora JR, Iwata M and von Andrian UH:
Vitamin effects on the immune system: Vitamins A and D take centre
stage. Nat Rev Immunol. 8:685–698. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ota K, Dambaeva S, Kim MW, Han AR, Fukui
A, Gilman-Sachs A, Beaman K and Kwak-Kim J: 1,25-dihydroxy-vitamin
D3 regulates NK-cell cytotoxicity, cytokine secretion, and
degranulation in women with recurrent pregnancy losses. Eur J
Immunol. 45:3188–3199. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mulligan ML, Felton SK, Riek AE and
Bernal-Mizrachi C: Implications of vitamin D deficiency in
pregnancy and lactation. Am J Obstet Gynecol. 202:429.e1–e9. 2010.
View Article : Google Scholar
|
|
29
|
Ota K, Dambaeva S, Han AR, Beaman K,
Gilman-Sachs A and Kwak-Kim J: Vitamin D deficiency may be a risk
factor for recurrent pregnancy losses by increasing cellular
immunity and autoimmunity. Hum Reprod. 29:208–219. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lee SK, Na BJ, Kim JY, Hur SE, Lee M,
Gilman-Sachs A and Kwak-Kim J: Determination of clinical cellular
immune markers in women with recurrent pregnancy loss. Am J Reprod
Immunol. 70:398–411. 2013.PubMed/NCBI
|
|
31
|
Fukui A, Kwak-Kim J, Ntrivalas E,
Gilman-Sachs A, Lee SK and Beaman K: Intracellular cytokine
expression of peripheral blood natural killer cell subsets in women
with recurrent spontaneous abortions and implantation failures.
Fertil Steril. 89:157–165. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ford HB and Schust DJ: Recurrent pregnancy
loss: Etiology, diagnosis, and therapy. Rev Obstet Gynecol.
2:76–83. 2009.PubMed/NCBI
|
|
33
|
Tavakoli M, Jeddi-Tehrani M,
Salek-Moghaddam A, Rajaei S, Mohammadzadeh A, Sheikhhasani S,
Kazemi-Sefat GE and Zarnani AH: Effects of 1,25(OH)2 vitamin D3 on
cytokine production by endometrial cells of women with recurrent
spontaneous abortion. Fertil Steril. 96:751–757. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lagana AS, Vitale SG, Ban Frangez H,
Vrtacnik-Bokal E and D'Anna R: Vitamin D in human reproduction: The
more, the better? An evidence-based critical appraisal. Eur Rev Med
Pharmacol Sci. 21:4243–4251. 2017.PubMed/NCBI
|
|
35
|
Chighizola CB, de Jesus GR and Branch DW:
The hidden world of anti-phospholipid antibodies and female
infertility: A literature appraisal. Autoimmun Rev. 15:493–500.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Cyprian F, Lefkou E, Varoudi K and Girardi
G: Immunomodulatory effects of Vitamin D in pregnancy and beyond.
Front Immunol. 10:27392019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Carp HJ and Shoenfeld Y: Anti-phospholipid
antibodies and infertility. Clin Rev Allergy Immunol. 32:159–161.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Redecha P, Franzke CW, Ruf W, Mackman N
and Girardi G: Neutrophil activation by the tissue factor/Factor
VIIa/PAR2 axis mediates fetal death in a mouse model of
antiphospholipid syndrome. J Clin Invest. 118:3453–3461.
2008.PubMed/NCBI
|
|
39
|
Tobaldini LQ, Arantes FT, Saraiva SDS,
Mazetto BM, Colella MP, de Paula EV, Annichino-Bizzachi J and Orsi
FA: Circulating levels of tissue factor and the risk of thrombosis
associated with antiphospholipid syndrome. Thromb Res. 171:114–120.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Tedesco F, Borghi MO, Gerosa M, Chighizola
CB, Macor P, Lonati PA, Gulino A, Belmonte B and Meroni PL:
Pathogenic role of complement in antiphospholipid syndrome and
therapeutic implications. Front Immunol. 9:13882018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Oku K, Atsumi T, Bohgaki M, Amengual O,
Kataoka H, Horita T, Yasuda S and Koike T: Complement activation in
patients with primary antiphospholipid syndrome. Ann Rheum Dis.
68:1030–1035. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Breen KA, Seed P, Parmar K, Moore GW,
Stuart-Smith SE and Hunt BJ: Complement activation in patients with
isolated antiphospholipid antibodies or primary antiphospholipid
syndrome. Thromb Haemost. 107:423–429. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
De Carolis S, Botta A, Santucci S, Salvi
S, Moresi S, Di Pasquo E, Del Sordo G and Martino C: Complementemia
and obstetric outcome in pregnancy with antiphospholipid syndrome.
Lupus. 21:776–778. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Reggia R, Ziglioli T, Andreoli L, Bellisai
F, Iuliano A, Gerosa M, Ramoni V, Tani C, Brucato A, Galeazzi M, et
al: Primary anti-phospholipid syndrome: Any role for serum
complement levels in predicting pregnancy complications?
Rheumatology (Oxford). 51:2186–2190. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Girardi G, Berman J, Redecha P, Spruce L,
Thurman JM, Kraus D, Hollmann TJ, Casali P, Caroll MC, Wetsel RA,
et al: Complement C5a receptors and neutrophils mediate fetal
injury in the antiphospholipid syndrome. J Clin Invest.
112:1644–1654. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Redecha P, Tilley R, Tencati M, Salmon JE,
Kirchhofer D, Mackman N and Girardi G: Tissue factor: A link
between C5a and neutrophil activation in antiphospholipid antibody
induced fetal injury. Blood. 110:2423–2431. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Izban MG, Nowicki BJ and Nowicki S:
1,25-Dihydroxyvitamin D3 promotes a sustained LPS-induced
NF-κB-dependent expression of CD55 in human monocytic THP-1 cells.
PLoS One. 7:e493182012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Agmon-Levin N, Blank M, Zandman-Goddard G,
Orbach H, Meroni PL, Tincani A, Doria A, Cervera R, Miesbach W,
Stojanovich L, et al: Vitamin D: An instrumental factor in the
anti-phospholipid syndrome by inhibition of tissue factor
expression. Ann Rheum Dis. 70:145–150. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
van den Hoogen LL, van Roon JA, Radstake
TR, Fritsch-Stork RD and Derksen RH: Delineating the deranged
immune system in the antiphospholipid syndrome. Autoimmun Rev.
15:50–60. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Martinez-Moreno JM, Herencia C, Montes de
Oca A, Muñoz-Castañeda JR, Rodríguez-Ortiz ME, Díaz-Tocados JM,
Peralbo-Santaella E, Camargo A, Canalejo A, Rodriguez M, et al:
Vitamin D modulates tissue factor and protease-activated receptor 2
expression in vascular smooth muscle cells. FASEB J. 30:1367–1376.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Santos TDS, Ieque AL, de Carvalho HC, Sell
AM, Lonardoni MVC, Demarchi IG, de Lima Neto QA and Teixeira JJV:
Antiphospholipid syndrome and recurrent miscarriage: A systematic
review and meta-analysis. J Reprod Immunol. 123:78–87. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Matalon ST, Blank M, Ornoy A and Shoenfeld
Y: The association between anti-thyroid antibodies and pregnancy
loss. Am J Reprod Immunol. 45:72–77. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Poppe K, Velkeniers B and Glinoer D:
Thyroid disease and female reproduction. Clin Endocrinol.
66:309–321. 2007. View Article : Google Scholar
|
|
54
|
Kivity S, Agmon-Levin N, Zisappl M,
Shapira Y, Nagy EV, Dankó K, Szekanecz Z, Langevitz P and Shoenfeld
Y: Vitamin D and autoimmune thyroid diseases. Cell Mol Immunol.
8:243–247. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
D'Aurizio F, Villalta D, Metus P, Doretto
P and Tozzoli R: Is vitamin D a player or not in the
pathophysiology of autoimmune thyroid diseases? Autoimmun Rev.
14:363–369. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Shin DY, Kim KJ, Kim D, Hwang S and Lee
EJ: Low serum vitamin D is associated with anti-thyroid peroxidase
antibody in autoimmune thyroiditis. Yonsei Med J. 55:476–481. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Bhattacharyya R, Mukherjee K, Das A,
Biswas MR, Basunia SR and Mukherjee A: Anti-thyroid peroxidase
antibody positivity during early pregnancy is associated with
pregnancy complications and maternal morbidity in later life. J Nat
Sci Biol Med. 6:402–405. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Ozkan S, Jindal S, Greenseid K, Shu J,
Zeitlian G, Hickmon C and Pal L: Replete vitamin D stores predict
reproductive success following in vitro fertilization. Fertil
Steril. 94:1314–1319. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Daftary GS and Taylor HS: Endocrine
regulation of HOX genes. Endocrine Rev. 27:331–355. 2006.
View Article : Google Scholar
|
|
60
|
Cippitelli M and Santoni A: Vitamin D3: A
transcriptional modulator of the interferon-gamma gene. Eur J
Immunol. 28:3017–3030. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Takeuchi A, Reddy GS, Kobayashi T, Okano
T, Park J and Sharma S: Nuclear factor of activated T cells (NFAT)
as a molecular target for 1alpha,25-dihydroxyvitamin D3-mediated
effects. J Immunol. 160:209–218. 1998.PubMed/NCBI
|
|
62
|
van Etten E and Mathieu C:
Immunoregulation by 1,25-dihydroxyvitamin D3: Basic concepts. J
Steroid Biochem Mol Biol. 97:93–101. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Piccinni MP, Scaletti C, Maggi E and
Romagnani S: Role of hormone-controlled Th1- and Th2-type cytokines
in successful pregnancy. J Neuroimmunol. 109:30–33. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Adams JS and Hewison M: Unexpected actions
of vitamin D: New perspectives on the regulation of innate and
adaptive immunity. Nat Clin Pract Endocrinol Metab. 4:80–90. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Boonstra A, Barrat FJ, Crain C, Heath VL,
Savelkoul HF and O'Garra A: 1alpha,25-Dihydroxyvitamin d3 has a
direct effect on naive CD4(+) T cells to enhance the development of
Th2 cells. J Immunol. 167:4974–4980. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Overbergh L, Decallonne B, Waer M,
Rutgeerts O, Valckx D, Casteels KM, Laureys J, Bouillon R and
Mathieu C: 1alpha,25-dihydroxyvitamin D3 induces an
autoantigen-specific T-helper 1/T-helper 2 immune shift in NOD mice
immunized with GAD65 (p524-543). Diabetes. 49:1301–1307. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Gonçalves DR, Braga A, Braga J and Marinho
A: Recurrent pregnancy loss and vitamin D: A review of the
literature. Am J Reprod Immunol. 80:e130222018. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Peterson CA and Heffernan ME: Serum tumor
necrosis factor-alpha concentrations are negatively correlated with
serum 25(OH)D concentrations in healthy women. J Inflamm (Lond).
5:102008. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Abdollahi E, Saghafi N, Rezaee SA, Rastin
M, Jarahi L, Clifton V and Rafatpanah H: Evaluation of 1,25(OH)2D3
Effects on FOXP3, ROR-γt, GITR, and CTLA-4 Gene expression in the
PBMCs of Vitamin D-Deficient Women with unexplained recurrent
pregnancy loss (URPL). Iran Biomed J. 24:295–305. 2020.PubMed/NCBI
|
|
70
|
Holick MF, Binkley NC, Bischoff-Ferrari
HA, Gordon CM, Hanley DA, Heaney RP, Murad MH and Weaver CM;
Endocrine Society, : Evaluation, treatment, and prevention of
vitamin D deficiency: An Endocrine Society clinical practice
guideline. J Clin Endocrinol Metab. 96:1911–1930. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Jeffery LE, Burke F, Mura M, Zheng Y,
Qureshi OS, Hewison M, Walker LS, Lammas DA, Raza K and Sansom DM:
1,25-Dihydroxyvitamin D3 and IL-2 combine to inhibit T cell
production of inflammatory cytokines and promote development of
regulatory T cells expressing CTLA-4 and FoxP3. J Immunol.
183:5458–5467. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Ibrahim ZM, madany EH, Abdel Aal RM and El
Biely MM: Role of 1,25-dihydroxyvitamin D (vitamin D3) as
immunomodulator in recurrent missed miscarriage. Middle East
Fertility Soc J. 18:171–176. 2013. View Article : Google Scholar
|
|
73
|
Figueiredo AS and Schumacher A: The T
helper type 17/regulatory T cell paradigm in pregnancy. Immunology.
148:13–21. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Vijayendra Chary A, Hemalatha R,
Seshacharyulu M, Vasudeva Murali M, Jayaprakash D and Dinesh Kumar
B: Vitamin D deficiency in pregnant women impairs regulatory T cell
function. J Steroid Biochem Mol Biol. 147:48–55. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Abdollahi E, Rezaee R, Saghafi N, Rastin
M, Clifton V, Sahebkar A and Rafatpanah H: Evaluation of the
effects of 1,25 vitamin D3 on regulatory T cells and T helper 17
cells in Vitamin D-deficient women with unexplained recurrent
pregnancy loss. Curr Mol Pharmacol. 13:306–317. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Ji J, Zhai H, Zhou H, Song S, Mor G and
Liao A: The role and mechanism of vitamin D-mediated regulation of
Treg/Th17 balance in recurrent pregnancy loss. Am J Reprod Immunol.
81:e131122019. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Rafiee M, Gharagozloo M, Ghahiri A,
Mehrabian F, Maracy MR, Kouhpayeh S, Pieper IL and Rezaei A:
Altered Th17/Treg ratio in recurrent miscarriage after treatment
with paternal lymphocytes and Vitamin D3: A Double-blind
placebo-controlled study. Iran J Immunol. 12:252–262.
2015.PubMed/NCBI
|
|
78
|
Li N, Wu HM, Hang F, Zhang YS and Li MJ:
Women with recurrent spontaneous abortion have decreased 25(OH)
vitamin D and VDR at the fetal-maternal interface. Braz J Med Biol
Res. 50:e65272017. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Samimi M, Foroozanfard F, Amini F and
Sehat M: Effect of Vitamin D supplementation on unexplained
recurrent spontaneous abortion: A double-blind randomized
controlled trial. Global J Health Sci. 9:95–102. 2017. View Article : Google Scholar
|
|
80
|
Yang X, Gilman-Sachs A and Kwak-Kim J:
Ovarian and endometrial immunity during the ovarian cycle. J Reprod
Immunol. 133:7–14. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Scarpellini F and Sbracia M: Use of
granulocyte colony-stimulating factor for the treatment of
unexplained recurrent miscarriage: A randomised controlled trial.
Hum Reprod. 24:2703–2708. 2009. View Article : Google Scholar : PubMed/NCBI
|