Introduction
Alzheimer's disease (AD) is the most frequent,
heterogeneous and severe form of dementia; it is characterized by
chronic, gradual and progressive memory loss, and a decline in two
or more cognitive functions. The clinical hallmarks of AD include
memory deficits and the associated deterioration of attention,
executive function, cognitive ability and behavioral abilities. AD
is a progressive and complex neurodegenerative disorder, which
eventually causes social or occupational impairment (1–3).
In 2020, AD accounted for 60–80% of all dementia cases out of the
50 million patients with dementia worldwide (4). The literature has demonstrated that
the neuro- and histopathological hallmarks expressively include the
buildup of extracellular amyloid-β (Aβ) peptides as amyloid plaques
and intracellular aggregates of hyperphosphorylated tau protein in
the form of neurofibrillary tangles, which disturb microtubule
organization and cholinergic dysfunction (3,5).
Furthermore, granulovacuolar degeneration (6), neuroinflammation (7), oxidative stress (8), reactive oxygen species (ROS)
(9), glutamate dyshomeostasis
(10), immunosenescence (11), aggregation of misfolded proteins
(12), and mitochondrial
oxidative and nitrosative stress (13) also affect the central nervous
system, promoting neural dysfunction and synaptic loss, thus
leading to increased vulnerability to neuronal degeneration and
cell death in AD (6–12). In addition, aging remains a major
pathological risk factor for AD (14). These clinicopathological entities
ultimately lead to neurodegeneration, synaptic dysfunction,
hippocampal degeneration and atrophy, thus culminating in memory,
cognitive and functional decline (10,15–17).
Researchers have been increasingly interested in
examining reliable novel imaging techniques [i.e., functional
magnetic resonance imaging (fMRI) and positron emission tomography
(PET)] (18) and in vivo
biomarkers (such as β-amyloid and tau protein) (19) involved in the various pathologies
of AD, and numerous molecular marker tests [Aβ positron emission
tomography (PET), cerebrospinal fluid (CSF) total or phosphorylated
tau and tau PET)] (19) have been
developed to detect such pathologies. The outcomes of neuro-imaging
technique and blood-based biomarkers will be important in
identifying the molecular mechanisms and pathological pathways
responsible for the neurodegenerative progression and development
of AD. Since Aβ peptides and phosphorylated tau proteins are highly
present in AD, these molecules are considered to be biomarkers that
can be used for the neurochemical diagnosis of AD (20). The cerebrospinal fluid
concentration, and blood and plasma levels of Aβ and phosphorylated
tau are the most accurate biological markers for diagnosing AD
(21–23).
Over the past few decades, there has been increasing
interest in biological markers to understand and diagnose AD via
imaging techniques. The application of neuroimaging biomarkers has
become a standard tool for understanding the preclinical stages of
AD and for periodic follow-up, as well as for diagnosing AD
(24). Various neuroimaging
biomarkers, including amyloid positron emission tomography imaging
(25), MRI (26) and optical coherence tomography
(27), have been used for the
diagnosis of AD. Over the past two decades, noninvasive brain
stimulation (NIBS) with electromagnetic fields (EMFs) has received
much interest regarding neuropsychiatric disorders, and this
research area has progressed greatly (28). Among the NIBS techniques,
transcranial magnetic stimulation (TMS) has emerged as a potential
method providing a promising avenue to treat cognitive impairment,
such as AD (2,29). A number of experimental studies on
animal models and clinical trials have demonstrated the beneficial
therapeutic effects of TMS on neurodegenerative disorders (30,31), including AD (32,33). Increasing evidence indicates that
TMS treatment permits the neurophysiological (including motor
cortex and neuronal activities) (34,35) and neurochemical (BDNF, TrkB)
(36,37) functions to work more precisely,
and TMS also regulates biomarkers level and further improves the
accurate and precise functioning of neurons in AD (Fig. 1). In addition, research suggests
that TMS improves neural branching, cortical excitability and
cognitive processes in AD (38).
Repetitive TMS (rTMS) provides a safe and noninvasive technique,
which modulates cortical excitability, neurochemical functions and
neuronal polarization (39,40). However, to the best of our
knowledge, the precise molecular mechanism behind the
neurorestorative effects of TMS is not yet fully understood. The
neurological changes, including inflammatory, neurodegenerative,
apoptotic, neuroprotective and genetic changes, during and after
TMS treatment in patients with AD are also not precisely known. The
present review focuses on TMS and rTMS, as an efficient technique,
giving an overview of the changes in inflammatory and apoptotic
mechanisms, mitochondrial and enzymatic activities, and modulation
of gene expression [or microRNA (miRNA/miR) expression profiles] in
patients with AD. The present review also examines the clinical and
neurochemical changes associated with rTMS in patients with AD.
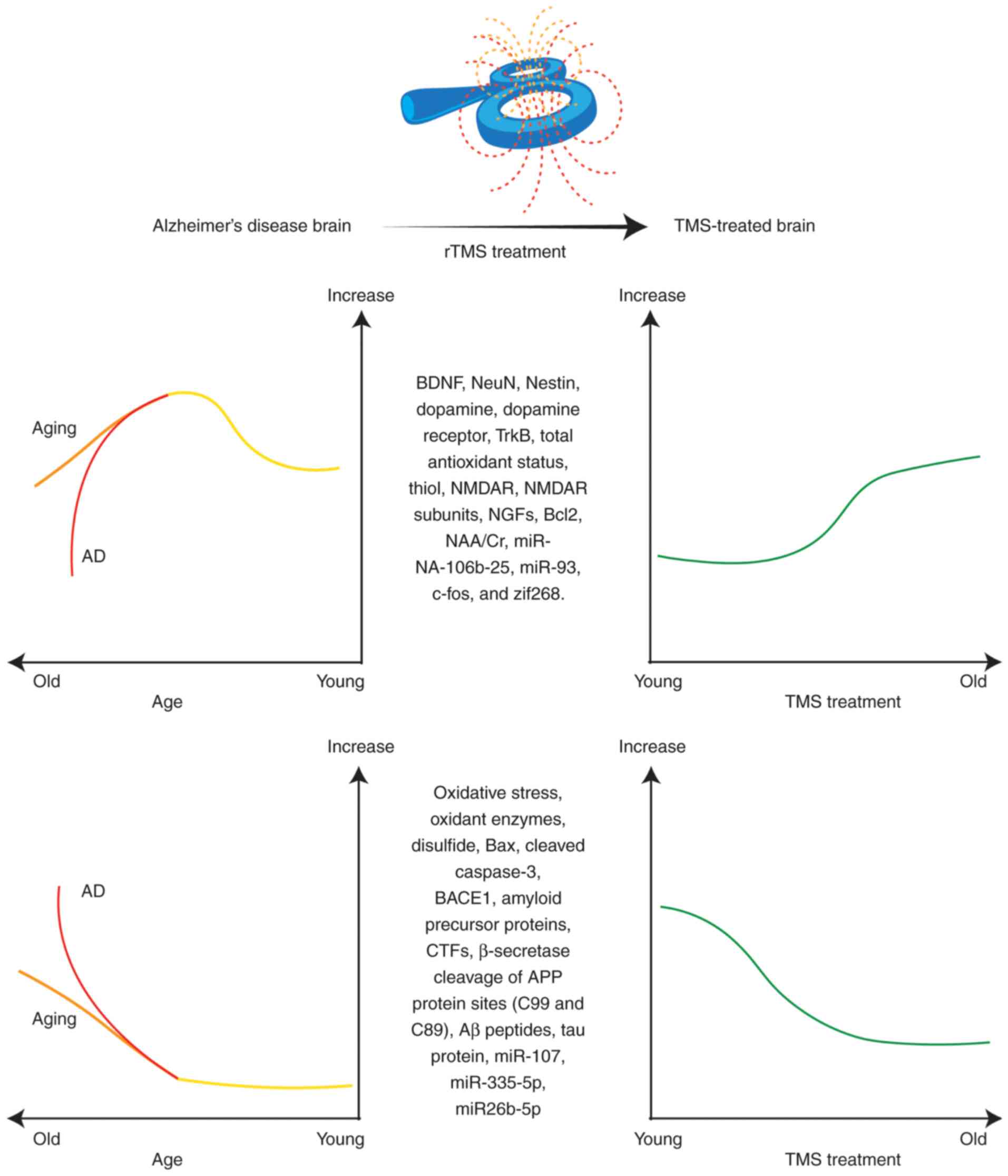 | Figure 1.Schematic representation of the
proposed paradigm demonstrating neurochemical changes in normal
aging and AD, and the effects of TMS on these neurobiological
changes, indicating that TMS may restore brain function. Aβ,
amyloid-β; AD, Alzheimer's disease; APP, amyloid-β precursor
protein; BACE1, β-site APP-cleaving enzyme 1; BDNF, brain-derived
neurotrophic factor; CTFs, C-terminal fragments; NAA/Cr,
N-acetylaspartate/creatine; NeuN, neuronal nuclear protein;
NGFs, nerve growth factors; NMDAR, N-methyl-D-aspartate receptor;
rTMS, repetitive transcranial magnetic stimulation; TrkB,
tropomyosin receptor kinase B; zif268, Zinc finger-containing
transcription factor 268. |
TMS
NIBS techniques are emerging and revolutionizing
neuroscience research. NIBS, particularly by EMFs, allows the study
of the relationship between the brain and certain behaviors. NIBS
techniques include TMS, transcranial direct current stimulation and
electroconvulsive therapy (39,41). TMS is a well-known
neurophysiological NIBS technique that was first introduced in 1985
(42). NIBS using TMS does not
require any surgery, anesthetic agents, skin preparation or
intravenous systems, and it is a painless technique (43), and thus, is rapidly becoming an
efficient therapeutic tool in cognitive neuroscience research. At
present, TMS is a Food and Drug Administration (FDA)-approved
therapy for treating major depressive disorder (44,45), treatment-resistant
obsessive-compulsive disorder (46) and migraine headaches (47). However, a number of animal models
and clinical trials have demonstrated promising results in treating
cognitive and neurodegenerative disorders (43), including AD (48,49) and Parkinson's disease (30,50,51). It has been suggested that TMS
could be used to treat between 70 and 80% of AD cases (52). The therapeutic value of TMS may be
achieved by applying EMFs to the predetermined cortical target
based on Faraday's principle of electromagnetic induction, which
was established in the latter half of the nineteenth century
(53). It involves the
application of time-varying MRI-strength magnetic fields near the
scalp and superficial layer of the cerebral cortex, inducing focal
electric currents, known as ‘Eddy currents’, which run in the
opposite direction to the current in the coil and generate a
magnetic field that induces currents (54,55). When the stimulation of the
magnetic coil occurs tangentially near the M1 region, an
appropriately strong stimulus is administered, and the powerful
magnetic field penetrates the scalp and skull, where it activates
underlying neurons and synapses, depolarizing axons in the targeted
brain areas, and thus, stimulating the brain region (56–58).
Types of TMS
TMS can be applied either in single pulses of
stimulation [single-pulse TMS (sTMS)], pairs of stimuli
[paired-pulse TMS (ppTMS)] separated by variable intervals
[interstimulus interval (ISI)] or trains of repetitive stimuli
(rTMS) that repeatedly pulse the EMFs at variable frequencies
applied to the brain regions (59).
sTMS is used to map cortico-motor outputs and assess
central motor conduction time, motor-evoked potential (MEP) and
motor cortical outputs. sTMS is delivered in single pulses of
stimulation that are separated by time intervals of 4–8 sec
(59).
ppTMS, which runs alternate to conventional TMS, is
used to measure intracortical facilitation, cortico-cortical
connection excitability, motor cortex connectivity (inhibition and
facilitation) and motor cortical pathways. ppTMS utilizes two
successive pulse stimuli, conditioning the stimulus with a test
stimulus that is separated by an ISI. A short ISI lasts for a few
milliseconds, and a long ISI ranges between tens and hundreds of
milliseconds (54,59,60).
rTMS has gained much interest from neuroscientists
due to its positive effects on cognitive tasks, and behavioral and
normal brain functioning (61).
rTMS induces trains of electric currents to the predetermined brain
region that are delivered through pulsating magnetic fields with a
time interval of a maximum of 2 sec (54). High-frequency rTMS (HF-rTMS; 10–20
Hz) tends to increase cortical excitability, intercellular
interactions and MEP amplitude. Low-frequency rTMS (LF-rTMS; 1–5
Hz) reduces cortical excitability and MEP amplitude (62). HF-rTMS and LF-rTMS have opposite
effects on brain regions but both have potential therapeutic
effects. It has been suggested that rTMS exerts long-lasting
effects on cortical excitability and plasticity (59,63).
TMS is a widely accepted and well-established
technique allowing for the assessment and modulation of neural
excitability and neuroplasticity of pre-specified brain regions.
TMS is an effective and promising neuromodulation treatment, as it
enhances the functional recovery of cortical and neural function
(64). At the molecular level, it
has been proposed that TMS modifies neural excitability, the
functional integrity of neural circuits, neuroplasticity, synapses
and normal brain activity (43).
TMS-evoked therapeutic effects can spread to the interconnected
cortical region, subcortical structures, spinal cord and roots
(59). TMS could potentially be
used to treat neurological disorders, including AD; however, the
underlying cellular processes and mechanisms of its therapeutic
effects are still not clearly understood.
AD and NIBS by TMS
AD is a neurodegenerative disorder that is
characterized by cognitive decline and brain neuronal loss of an
unknown etiology. Early studies have provided a basic and molecular
understanding the pathogenesis of AD (1,65).
AD neuropathology is considered to be commonly associated with
altered neuroplasticity, neurotrophic impairment, neurotransmitter
failure and synaptic loss. Furthermore, synaptic dysfunction is
noted in the early stages of AD and has become a therapeutic target
for pharmaceutical agents (1,65).
However, more research is required to clarify the pathogenesis of
AD. A pioneering field of research in AD is brain stimulation via
EMFs, which may have clinical and therapeutic benefits. Numerous
studies and a few clinical trials have demonstrated the potential
therapeutic effects of NIBS, particularly TMS, on patients with AD
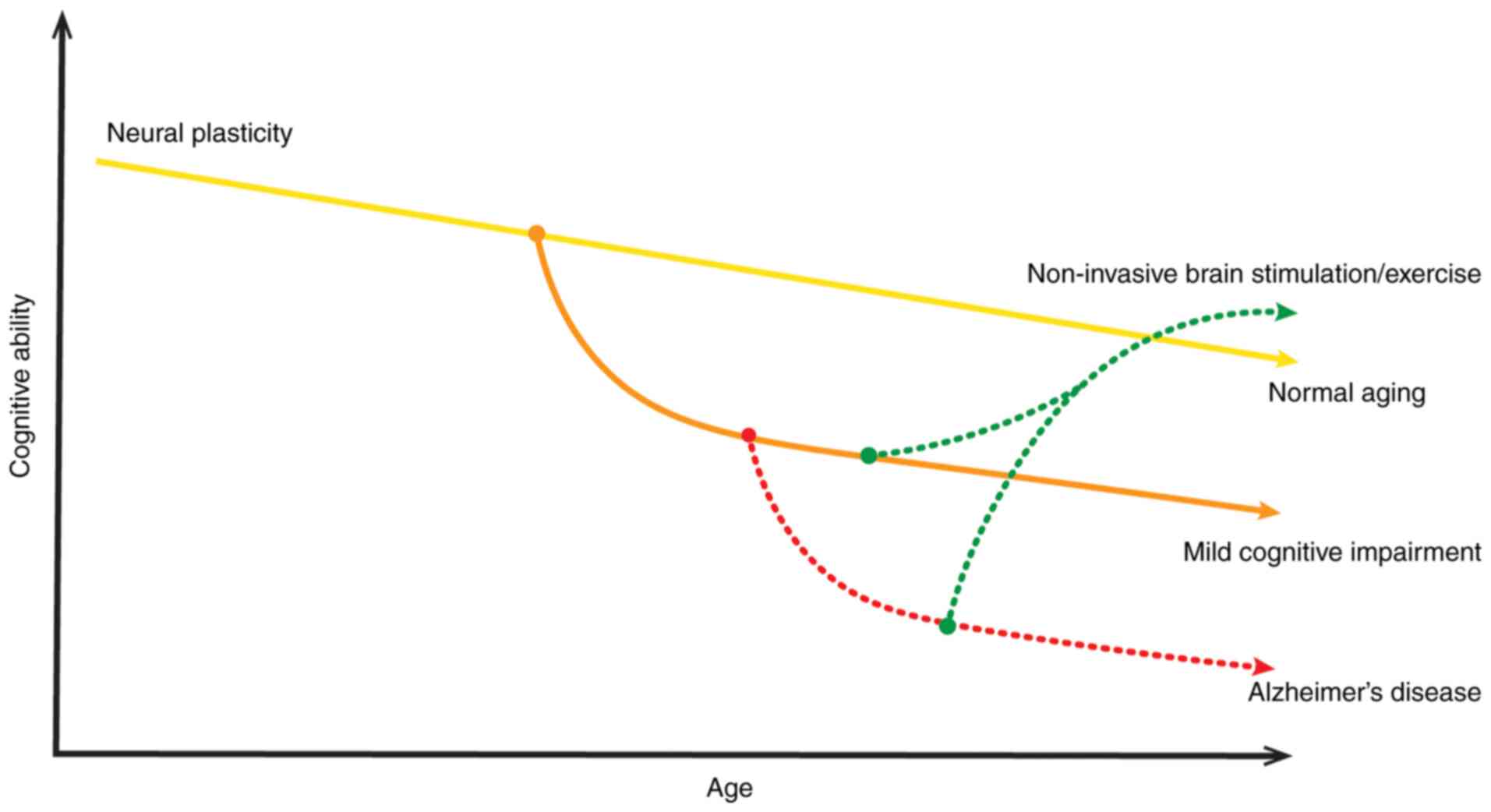
(2,36,66). Due to the ageing process, the
cognitive decline and deterioration of neural plasticity occurs,
which may worsens by MCI or AD. However, TMS improves cognitive
ability and increases neural plasticity. Therefore, NIBS techniques
exerts a neuroprotective effect on AD (Fig. 2). Although TMS treatment is
approved by the FDA for depression (44), it is still an experimental therapy
for AD. Extensive research has indicated that TMS might be an
effective treatment for patients with AD (67,68). TMS promote synapses, neurogenesis
and normal brain functioning stability that aid in the treatment of
AD (63). To the best of our
knowledge, the basic mechanism behind the neurorestorative effects
of treatment with EMFs in patients with AD is still elusive.
Furthermore, the neurological and neurochemical changes during and
after TMS treatment in patients with AD are not clearly explained.
Previous studies have suggested that changes in inflammatory and
apoptotic mechanisms, mitochondrial enzymatic activities, and
modulation of gene expression (miRNA expression profiles) may be
associated with TMS or sham procedures (69,70).
Neurobiological changes associated with TMS
in AD
The present review identifies neurobiological
changes, including the inflammatory, neurodegenerative, apoptotic,
neuroprotective and genetic changes, associated with TMS treatment
in patients with AD.
Neural restoration by TMS
Neurotrophic factors (NTFs) regulate the growth,
survival, proliferation, migration and differentiation of neurons
(71). Therefore, NTFs have been
extensively studied in the context of neurodegenerative disorders,
including AD (72). In AD, the
altered expression and gradual dysregulation of NTFs, such as nerve
growth factor (NGF), brain-derived neurotrophic factor (BDNF),
glial cell line-derived neurotrophic factor (GDNF) and ciliary
neurotrophic factor (CNTF), have been observed in different brain
areas (73,74). Numerous experimental studies have
indicated the reduction of NTFs in affected brain regions (72,73). These changes in NTFs in AD are
critical for neurodegenerative processes. Studies have observed
that cognitive decline and the underlying pathologies of AD are
associated with neurodegeneration in various regions of the brain,
especially cholinergic neurons of the basal forebrain and their
projections for the hippocampus and cortex (72,75,76). It has been suggested that the loss
of NTFs may be a mechanism involved in the pathogenesis of AD
(77). The regulation of NTFs
could be a suitable therapeutic target for AD treatment.
As a noninvasive neuromodulatory intervention, TMS
or rTMS treatment may potentially regulate the expression of NTFs
in the AD brain (Fig. 1),
promoting neuronal differentiation and survival (78), and thus, exerting neurorestorative
effects. Notably, a number of studies have indicated an increase in
endogenous neurotrophic content (BDNF) in the affected brain
regions after TMS therapy (2,74).
BDNF is a neurotrophin involved in synaptic plasticity changes and
improves learning, memory and cognitive functions via the
BDNF-tropomyosin receptor kinase B (TrkB) signaling pathway
(32,74). Therefore, BDNF serves a critical
role in memory formation and synapsis. However, deficits in BDNF
signaling are associated with AD (79). Furthermore, the expression levels
of BDNF are altered in neurodegenerative disorders, for example the
BDNF levels are decreased in AD (80). A study by Choung et al
(32) revealed an increase in
BDNF expression, as well as neuronal nuclear protein (NeuN) and
neuroepithelial stem cell protein (Nestin), after 20 Hz HF-rTMS
compared with the non-rTMS group or sham group in the hippocampus
and cerebral cortex regions. It was concluded that rTMS exerted
neurogenic and neuroprotective effects and promoted neurogenesis
(Table I) (32). A similar increase in BDNF has also
been observed after rTMS treatment in a number of other studies
(36,81). Additionally, rTMS treatment
positively regulates the BDNF receptor TrkB. Chen et al
(81) observed an increase in
TrkB in the AD brain after 5 Hz HF-rTMS. In addition, LF-rTMS also
regulates BDNF levels in AD (Table
I) (82). A previous study
revealed that 1 Hz LF-rTMS upregulates BDNF content in the
hippocampal region of the AD brain (82). Tan et al (82) also reported the effects of LF-rTMS
on another NTF, NGF, which is essential for growth, development,
survival and neuronal population. The expression of NGFs has been
found to be altered in AD (Table
I). The 1 Hz LF-rTMS treatment upregulates NGF content in AD
(Aβ injected mice) group compared to control (saline injected)
group (82). Similar results have
also been published by Chen et al (83), who applied both 1 and 10 Hz rTMS
and observed that both frequencies of rTMS regulated the brain
levels of NTFs (BDNF and NGF), and these increased with increased
frequency. Furthermore, glial cells, astrocytes and neurons secrete
BDNF and NGF, which could be increased following rTMS treatment,
therefore rescue memory deficit (82) In contrast to that in AD, various
studies have indicated that rTMS application tends to decrease BDNF
levels in healthy volunteers (84,85). However, the precise mechanisms of
direct evaluation of BDNF levels in humans after TMS treatment
remain unclear (86). BDNF levels
are associated with TMS treatment, both during and after treatment.
Briefly, these findings suggest that BDNF could be an ideal
biomarker for TMS treatment for patients with AD.
 | Table I.Neurobiological changes and
neurobiological biomarkers associated with the potential
disease-modifying and anti-AD effects of TMS. |
Table I.
Neurobiological changes and
neurobiological biomarkers associated with the potential
disease-modifying and anti-AD effects of TMS.
| First author/s,
year | Study subject | Neurobiological
marker observed | TMS parameters | Results | TMS outcomes | (Refs.) |
|---|
| Choung et
al, 2021 |
Intracerebroventricular Aβ42-induced mouse
model of AD | Dopamine, BDNF,
DR4, Nestin and NeuN | 20 Hz HF-rTMS and 1
Hz LF-rTMS | DR4, BDNF, Nestin
and NeuN increased in the Hr-AD group compared with that in the
Lr-AD and Nr-AD groups. | Enhanced spatial
working memory, improved neurocognitive progress, increased
neurogenesis, and neurogenic, neuroprotective and neuroregenerative
effects. | (32) |
| Chen et al,
2020 | APP/PS1
double-mutant transgenic mouse model of AD | BDNF, TrkB,
synaptic plasticity-related proteins (PSD95 and SYN), p-AKT, LC3II,
LC3I, ApoE and p62 | 5 Hz HF-rTMS | No differences in
SYN, PSD95 and p-AKT. BDNF, BDNF-TrkB signaling and LC3II/LC3I
ratio increased, and ApoE and p62 decreased. | Reduced the
cognitive impairment of learning and memory, lessened the AD
pathology progression and AD-like dysfunctions, enhanced the
hippocampal autophagy level and enhanced the cognitive
function. | (81) |
| Tan et al,
2013 | Aβ1-42-induced
toxicity rat model of AD | Neurotrophins (NGF
and BDNF) and NMDA-receptor levels (NR1, NR2A and NR2B) | 1 Hz LF-rTMS | BDNF, NGF, NR1,
NR2A and NR2B increased. | Increased
hippocampal neurotrophins and NMDA-receptor contents, enhanced
hippocampal LTP, reversed memory deficits, and improved spatial
memory retrieval ability. | (82) |
| Chen et al,
2019 | Aβ1-42-induced
toxicity rat model of AD | BDNF, NGF, GSK-3β,
p-GSK-3β, Tau, p-Tau, β-catenin and p-β-catenin, cleaved caspase-3,
Bax, and Bcl-2 | 10 Hz HF-rTMS and 1
Hz LF-rTMS | BDNF, NGF, GSK-3β,
Tau, Bcl-2, β-catenin increased. P-GSK-3β, p-Tau, cleaved
caspase-3, Bax and p-β-catenin decreased. | Improved cognitive
function, decreased neuron apoptosis, increased neuronal viability,
promoted the survival of neurons and improved cognitive
function. | (83) |
| Velioglu et
al, 2021 | Patients with
AD | BDNF, total
antioxidant status, total thiol, native thiol, total oxidant
status, oxidative stress index, oxidant enzyme activity and
disulfide level | 20 Hz HF-rTMS | BDNF, total
antioxidant status, total thiol and native thiol increased. Total
oxidant status, oxidative stress index, oxidant enzyme activity and
disulfide levels decreased. | Increased visual
recognition memory functions, decreased oxidant status, increased
anti-oxidant levels and improvement in familiarity-based
cognition. | (36) |
| Zhang et al,
2019 | Patients with
AD | Ratio of NAA/Cr,
Cho/Cr and mI/Cr | 10 Hz rTMS | NAA/Cr increased.
Cho/Cr and mI/Cr remained unchanged. | Prevented neuronal
functional deterioration, improved cognitive function and
ameliorated agitation and apathy. | (134) |
| Huang et al,
2017 | APP23/PS45
double-mutant transgenic mouse model of AD | APP, CTFs (C99 and
C89) and BACE1 | 1 Hz LF-rTMS | APP,
β-secretase-β-secretase-cleaved C-terminal fragments of amyloid
precursor protein. (C99, C89), and BACE1 decreased. | Improved spatial
learning and memory, rescued impaired hippocampal LTP, reduced
AD-related neuropathology, inhibited β-secretase cleavage of APP
proteins and reduced neuritic plaque formation. | (136) |
| Perez et al,
2021 | Primary human brain
cultures | Aβ40 and Aβ42
levels | Repeated
electromagnetic field stimulation (3 mT; 75 Hz) | Aβ40 and Aβ42
decreased. | Decreased Aβ
toxicity. | (154) |
| Capelli et
al, 2017 | Peripheral blood
mononuclear cells from peripheral blood of patients with AD | miRNAs (miR-107,
miR-335-5p and miR26b-5p) and BACE1 | 75 Hz low-frequency
pulsed electromagnetic field | BACE1 and miRNAs
decreased with increasing time of exposure. | Modulated the
expression of miRNAs, stimulated epigenetic regulation, and
regulated brain signaling and synaptic plasticity. | (70) |
Antioxidant effects of TMS
application
Oxidative stress serves a key role in the etiology
and pathogenesis of AD. The imbalance in cell redox status, ROS
production and impaired antioxidant defense lead to oxidative
stress (87). These forms of
damage serve a pivotal role in cellular dysfunction, potentially
harming the neurons in aging and neurodegenerative disorders,
including AD. AD research has revealed that oxidative stress and
free radical damage are associated with histopathological hallmarks
of AD, such as amyloid plaques and neurofibrillary tangles
(88,89). ROS are free radical oxygen
byproducts containing an unpaired electron in their valence shell,
and these are generated as a result of cellular respiration. The
excessive buildup of ROS, including oxygen radical superoxide and
hydrogen peroxide, in the cells or neurons causes DNA or RNA
oxidative damage, leading to cell death and tissue damage (87). Mitochondrial dysfunction generates
excessive ROS as the byproduct of the electron transport chain,
ameliorating the risk of AD (90,91). Therefore, oxidative stress and
mitochondrial dysfunction adversely affect the brain, leading to
aging and neurodegenerative disorders, particularly AD.
Furthermore, studies have indicated that oxidative stress and BDNF
are associated with each other (89,92). In addition, oxidative stress could
be considered a promising biomarker of AD prognosis (93). In line with this, TMS treatment
noninvasively modulates and balances BDNF and oxidative stress
levels, thus exerting beneficial antioxidant effects in patients
with AD (Fig. 1) (36). Some studies have reported that
rTMS increases BDNF levels and decreases oxidative stress in
treatment-resistant depression (94), stroke (95) and experimental autoimmune
encephalomyelitis (96). However,
there are a limited number of experimental studies in the
literature demonstrating the effects of TMS on oxidative stress in
AD. Only a recent study by Velioglu et al (36) has analyzed the beneficial effects
of rTMS on BDNF and oxidative stress levels in patients with AD.
For this purpose, 20 Hz rTMS was applied to the lateral parietal
cortex in patients with AD. The levels of BDNF, total antioxidant
status, total thiol levels and native thiol levels were increased
after 20 Hz rTMS treatment. Furthermore, the total oxidant status,
oxidative stress index, oxidant enzyme activity and disulfide
levels were decreased following left lateral parietal rTMS
(Table I) (36). Oxidative stress could be an
effective target for the treatment of neurodegenerative disorders;
however, there remains a large research gap in terms of
investigating the influence of TMS on oxidative stress, antioxidant
defense systems, total oxidant/antioxidant status and antioxidant
enzymes. More studies are required to fill this research gap.
TMS facilitates synapsis by regulating
neurotransmitters
The onset of AD also negatively influences the
metabolism, levels and functioning of synaptic neurotransmitters.
There are important contributions of cholinergic and noncholinergic
neurotransmitter systems behind the pathophysiological signaling in
AD (97). Neurotransmitters are
chemical messengers that are released from a nerve to stimulate
other nerves across the synapse. Neurotransmitters, including
dopamine, glutamate, aspartate and γ-aminobutyric acid (GABA),
serve a key role in cognitive control, learning and memory
development (98). Therefore,
alterations in the metabolism and expression of neurotransmitters
lead to synaptic dysfunction, cognitive impairment, learning
disabilities and memory deficits. A number of studies have
emphasized that the expression of neurotransmitters and receptors
is markedly reduced in patients with AD (97,99). Therefore, targeting
neurotransmitters, as well as their receptors, could be a rational
approach to overcome AD. NIBS by EMF from TMS has the potential to
minimize symptoms and elucidate AD pathology by positively
regulating neurotransmitter parameters (e.g. dopamine; Fig. 1).
Dopamine is a monoamine neurotransmitter produced in
dopaminergic neurons; it is involved in synaptic plasticity and
regulates mood, emotional stability, and cognitive and motor
function (100). The dopamine
receptors (D1, D2, D3,
D4 and D5) are G-protein-coupled receptors
that are mostly expressed in the limbic system and cortex (101). The dopaminergic system serves a
pivotal role in the pathophysiology of AD (102). The loss and decrease in dopamine
content and its receptors are frequently reported in patients with
AD, causing motor impairment and cognitive decline (99,103,104). TMS increases the levels of
dopamine and dopamine receptors in patients with AD. However, a
limited number of studies have been conducted regarding dopamine
levels after TMS application. Furthermore, in healthy volunteers,
dopamine tends to increase following deep TMS therapy (105). In a recent study by Choung et
al (32), HF (20 Hz) and LF
(1 Hz) rTMS were applied to assess dopamine levels and receptor
concentrations after rTMS application. The findings suggested that
HF-rTMS and LF-rTMS increased the dopamine levels in the
hippocampus. The expression of dopamine receptor 4 (DR4) was
increased after 1 Hz LF-rTMS in the hippocampus and cerebral cortex
of the AD brain compared with that of the LF and non-rTMS AD groups
(32). After TMS therapy, the
dopamine levels are also increased in healthy volunteers (105,106). The increases in dopamine levels
after TMS could allow monitoring of the progress of the brain
stimulation of patients with AD by TMS. The dopamine level also has
the potential to be a biomarker for TMS treatment.
The N-methyl-D-aspartate receptor (NMDAR) is a
critical molecule that serves a key role in synaptic transmission,
synaptic plasticity, hippocampal long-term potentiation (LTP),
learning and memory (107).
NMDAR is a glutamate receptor that is important for excitatory
neurotransmitter transmission, synapsis and memory formation
(108). In AD, Aβ plaques
trigger excessive calcium (Ca2+) influx, which enters
into neurons via NMDARs, leading to gradual synaptic dysfunction
and neuronal cell death (109).
However, NMDAR is downregulated in patients with AD (110). Battaglia et al (111) observed neocortical plasticity
impairment in patients with AD and amyloid precursor protein
(APP)/presenilin-1 mice, which could cause functional deficits of
NMDAR. It has been observed that TMS application can regulate
neurotransmitters, including NMDAR expression, effectively
affecting cognitive function (112). Low-frequency (1 Hz) rTMS
increases NMDAR expression, also increasing NMDAR subunits (NR1,
NR2A and NR2B) in the hippocampus, thus facilitating LTP and memory
formation (82). Furthermore, an
increase in NMDAR and vascular endothelial growth factor (VEGF)
expression has been observed in a rat model of vascular dementia
(VaD) following 5 Hz rTMS treatment (112) and 1 Hz rTMS (69). The increase in NMDAR-related amino
acids has also been observed after LF-rTMS (1 Hz) by Niimi et
al (113) in patients after
stroke. Furthermore, it has been observed that upregulation of
NMDAR contributes to enhanced neurotrophic effects (107). Therefore, treating memory
deficits promotes synaptic plasticity, hippocampal plasticity and
memory formation. Impaired NMDAR function could alter plasticity in
AD. An improved understanding of AD pathophysiology would
facilitate the development of a novel treatment that regulates
NMDAR function and improves plasticity, learning and memory
deficits in patients with AD. Furthermore, an increase in NMDAR
expression facilitates neuronal recovery following rTMS.
TMS suppresses apoptosis and exerts
neuroprotective effects
In neurodegenerative disorders, particularly AD,
excessive neuronal loss is considered to be common due to
apoptosis, which acts as a major cell death pathway in neurons
(114,115). In AD, the levels of
apoptosis-related Bcl-2 are downregulated, while those of Bax and
cleaved caspase-3 are upregulated (116). TMS noninvasively regulates and
balances the apoptotic pathways, thus exerting its beneficial
effects on the brains of patients with AD (Fig. 1) (33,82,83). TMS suppresses the apoptotic
pathways by inhibiting several members of the Bcl-2 family,
particularly Bad, Bax and Bcl-XL, which enhances
apoptosis. rTMS (1 and 10 Hz) treatment in AD mouse models
increased apoptosis, as reflected by enhanced Bcl-2 expression and
decreased levels of Bax and cleaved caspase-3 (83). Similarly, in a VaD rat model, 1 Hz
rTMS was found to increase Bcl-2 expression and suppress Bax
expression (69). A study on a
middle cerebral artery occlusion rat model revealed that 10 Hz rTMS
treatment markedly upregulated Bcl-2 expression and decreased the
levels of Bax and TUNEL-positive cells in the ischemic hippocampus
(117). Studies have
demonstrated that rTMS suppresses the apoptosis and apoptotic
pathways, and thus, rTMS may improve cognitive impairment and exert
neuroprotective effects on neurons in an affected brain,
particularly in AD (78,83,118). rTMS regulates Bcl-2 and Bax
expression, which can promote the functional recovery of cognitive
impairments and enhance the protective mechanisms of learning and
memory with increased synaptic plasticity; this mechanism may be
mediated by the BDNF signaling pathway (117). More research is required to
study the effects of TMS on apoptosis in AD pathology. However, TMS
could be a promising candidate for the clinical treatment of
AD.
Cognitive rehabilitation and
improvement in memory and executive functions by TMS
AD is associated with progressive and irreversible
loss of memory, decline in cognitive function, and deterioration of
attention, executive function, thinking and behavioral abilities.
In AD, language, reasoning, social behavior, verbal and auditory
naming, and the ability to carry out simple tasks are also severely
impaired due to underlying neurodegenerative processes (119–121). Executive functions, including
working memory and selective attention, are typically associated
with the dorsolateral prefrontal cortex (DLPFC). Impaired DLPFC
neuroplasticity is associated with the physiopathology of AD,
severely affecting the executive functions in patients with AD
(122,123). Some studies have assessed DLPFC
plasticity in patients with AD using paired associative stimulation
(PAS), a TMS paradigm, as a measure of DLPFC and potentiation of
cortical-evoked activity (124).
PAS is the combination of repeated pairing of single pulses of
peripheral nerve electrical stimulation with single pulses of TMS
of the contralateral cerebral cortex. PAS (TMS with
electroencephalography) results in short-term modulation of
corticospinal excitability and induces LTP-like plasticity in the
different pathological stages of AD (122,124,125). Furthermore, the impaired
LTP-like cortical plasticity could be a potential biomarker for the
prognosis of AD (126). A recent
study revealed that 20 Hz rTMS improved cognition in AD (29). Cortical LTP-like plasticity is
associated with cognitive function improvement in patients with AD
following rTMS (49). In view of
this, TMS positively regulates executive function, cognitive
ability and visuospatial learning behavior in DLPFC (127).
Numerous studies have highlighted the fact that TMS
can improve cognitive and executive functions, memory and language
ability in patients with AD (29,33,66,128). However, to the best of our
knowledge, the molecular and metabolic changes following rTMS are
still unknown. The effects of LF-rTMS and HF-rTMS on neuronal
plasticity and the learning process in memory tasks have been
studied extensively. Cappa et al (129) reported that 20 Hz rTMS activates
the DLPFC, facilitating object and action naming. Similarly,
high-frequency (20 Hz) rTMS applied to the left and right DLPFC
improves naming performance not only in mild AD (130), but also in severe AD (131). rTMS may enable the intrinsic
ability of the brain to recover damaged function (131). Another study by Cotelli et
al (132) suggested that
rhythmic HF-rTMS over DLPFC exerts beneficial effects on sentence
comprehension and may be used to treat language dysfunction in
patients with AD. However, the exact underlying mechanisms involved
in rTMS improving naming and speech are still elusive. Ahmed et
al (133) demonstrated that
(20 Hz) HF-rTMS for five daily sessions over the left and right
DLPFC improved cognitive functions in patients with mild to
moderate AD. Zhang et al (134) combined HF-rTMS with cognitive
training (rTMS-CT), revealing that the ratio of
N-acetylaspartate/creatine (NAA/Cr) increased in the left
DLPFC of AD patients. Furthermore, the choline (Cho)/Cr and
myoinositol (mI)/Cr ratios remained unchanged in the rTMS-CT group
compared to sham group (sham rTMS with CT). The study also proposed
that rTMS-CT may improve cognitive function in patients with AD who
are in a mild to moderate stage (134). On the other hand, low-frequency
(1 Hz) rTMS applied over the left DLPFC of patients with AD has
been found to facilitate no change in memory performance. However,
when applied to the right DLPFC, low-frequency (1 Hz) rTMS improves
recognition memory function (135). Additionally, 20 Hz rTMS on the
lateral parietal cortex in patients with AD increases visual
recognition memory (36).
Furthermore, 1 Hz LF-rTMS could potentially rescue spatial learning
and memory deficits accompanied by impaired LTP-plasticity in the
hippocampal CA1 region in an APP23/PS45 double transgenic mouse
model of AD (136). Future
studies will also investigate the short- and long-term effects of
rTMS on AD and cognitive functions (48). Furthermore, rTMS improves spatial
working memory in mouse models of AD (32), visuospatial reasoning, and trained
associative memory in patients with AD (137). Accordingly, these studies have
concluded that rTMS could be beneficially and therapeutically
effective for NIBS, behavioral recovery and cognitive
rehabilitation, as well as a well-tolerated therapy for patients
with AD. The cortical changes induced by rTMS can improve synapsis
and neuronal plasticity (138).
In addition, there are only limited experimental studies
highlighting the neurobiological changes during cognitive
rehabilitation by rTMS (134).
We hypothesize that changes in metabolites or other molecular
indices could serve as biomarkers following rTMS, allowing for
further improvement of the accurate and precise functioning of
neurons in AD. Therefore, future studies should focus on the levels
of metabolites and NAA/Cr, Cho/Cr and mI/Cr ratios after TMS
treatment to further explore the therapeutic effects of rTMS on
cognitive rehabilitation in AD.
TMS modulates gene expression and
miRNA expression profiles in AD
miRNAs are novel, short (~22 nucleotides),
evolutionarily conserved, noncoding RNA molecules that are
post-transcriptional regulators of gene expression, cell
proliferation, differentiation and apoptosis (139,140). miRNAs serve an important role in
regulating the translation and stability of mRNAs, are involved in
pathological processes, and inhibit their translation by guiding
RNA-induced silencing complex and complement binding or interacting
with the 3′-untranslated region of mRNA (141,142). An increasing number of studies
have demonstrated that approximately one-half of the miRNAs are in
proximity to other miRNAs and regulate the activity of 60% of all
protein-coding genes (140,143). A single miRNA regulates almost
400 different mRNAs (144). It
has also been reported that miRNAs serve a pivotal role in synaptic
formation, development function, plasticity and neuronal processes,
such as neural proliferation, differentiation, maturation and
migration (145–147). Studies have demonstrated that
miRNAs contribute to the development of numerous diseases and
neurodegenerative disorders, including AD (141,147). The changes in the levels of
miRNAs could also serve as diagnostic biomarkers for AD (148,149). Different miRNAs have been found
to be associated with the accumulation of Aβ peptides and tau
phosphorylation (141,150), leading to the pathophysiology of
AD. Furthermore, miRNAs also regulate oxidative stress and vice
versa (142).
TMS might also have the ability to regulate miRNA
expression in AD (Fig. 1). In
line with this, future studies are required to clarify whether TMS
regulates gene expression and miRNAs. However, a few studies have
reported the effects of TMS on miRNAs. Liu et al (151) investigated the effects of rTMS
on the proliferation of neural stem cells (NSCs) and their
association with miRNAs expression in vivo. The 10 Hz rTMS
treatment was associated with the upregulation of the miRNA-106b-25
cluster and miR-93, the downregulation of p21 protein and enhanced
NSC proliferation (151). Liu
et al (152) also
investigated the effects of rTMS on the proliferation of neural
progenitor cells (NPCs) and the association with miR-106b
expression when 10 Hz rTMS was applied to the NPCs cultured from a
rat hippocampus. The results revealed that rTMS enhanced NPC
proliferation by upregulating miR-106b expression by inhibiting p21
expression (152). Another study
by Aydin-Abidin et al (153) examined the effects of
low-frequency (1 Hz) rTMS, high-frequency (10 Hz) rTMS and
intermittent theta-burst stimulation (iTBS) on the expression of
immediate early gene (IEG) proteins c-Fos and zinc finger protein
268 (zif268) in the rat brain. It was observed that LF-rTMS and
HF-rTMS increased c-Fos protein expression in the cortical areas.
LF-rTMS did not regulate zif268 expression, but HF-rTMS increased
zif268 expression in the primary motor and sensory cortices.
Additionally, iTBS increased c-Fos expression in limbic cortices
only and zif268 levels in all cortical areas (153). One study investigated the
effects of a low-frequency pulsed EMF (LF-PEMF) on protein (BACE1)
and miRNA expression involved in AD (70). It was revealed that 75 Hz LF-PEMF
modulated the expression of miR-107, miR-335-5p and miR26b-5p in an
experimental cell model of peripheral blood mononuclear cells from
patients with AD. miR-107 regulates β-site APP-cleaving enzyme 1
(BACE1), which serves a role in the amyloidogenic pathway of the
APP pathway. An increasing LF-PEMF exposure time reduced miRNAs
expression and BACE1 level (Table
I) (70). Recently, Perez
et al (154) reported
that repeated EMF stimulation reduces Aβ40 and Aβ42 peptides in
primary human brain cultures. In a similar vein, another study
reported that low-frequency (1 Hz) rTMS progressively downregulated
APP and its C-terminal fragments (CTFs) in the AD mouse brain. The
decrease in β-secretase generated C99 and C89 fragments, and BACE1
could be observed following 1 Hz rTMS application in transgenic
mice (136). Accordingly, it was
also demonstrated that rTMS may suppress β-secretase cleavage of
APP proteins, contributing toward the decrease in Aβ
neuropathology, such as neuritic plaque formations, APP processing
and BACE1 expression, which may contribute to the amelioration of
cognitive functioning and synaptic plasticity (136). Therefore, TMS exerts anti-AD
effects by targeting Aβ peptides, modulating gene expression in the
AD brain and reducing AD-related neuropathology in patients with
AD.
Potential side effects associated with TMS
treatment
Although TMS exerts extensive therapeutic effects,
various possible side effects have also been disclosed previously.
Headache (or neck and scalp pain) is considered the common side
effect, which might result in accidental seizures, hypomania or
unwanted psychiatric complications (155). Transient headache is reported by
20–40% of the patients undergoing TMS (both low- and
high-frequency), but seizures (>1%), hypomania and cognitive
changes are very rare or negligible (156). TMS is also unlikely to cause
structural changes, histotoxicity or tissue damage, although
unintended long-term changes in the brain are theoretically
possible (157). Additionally,
the clicking sound of TMS and skin stimulation cause multi-sensory
experiences and trigger shifts of spatial attention (158,159). The incorrect positioning of the
coil may cause a placebo (160)
or unwanted effect, affecting the behavioral, physiological and
cognitive processes. However, the safety guidelines for TMS
suggested by Wassermann (161)
and Chen et al (162)
recommend frequencies, current intensities and trains of stimuli to
prevent side effects of the treatment. In addition, TMS parameters
combined with short trains and long inter-train intervals carry a
lower risk of side effects (163).
Discussion
Aging is the major risk factor behind the
pathogenesis of cognitive decline, dementia and neurodegenerative
disorders, including AD (14).
Being a severe form of dementia, AD is a multifactorial, chronic
and progressive disorder leading toward memory decline and
cognitive dysfunctions (164).
The clinicopathological features of AD brains include proteinopathy
(amyloid plaques neurofibrillary tangles) (164,165). Despite tremendous advancements
in the field of neurology and medical sciences, little is known
regarding the mechanism behind this complex neurodegenerative
disease. AD treatment is still a major challenge for researchers
and physicians. Furthermore, there are no effective drugs or
nondrug treatment options that can cure AD or stop or slow its
progression. Neurons may be damaged or have already died due to
neurodegenerative disorders, but TMS has the potential to treat and
restore them due to its neuroprotective, neuro-regenerative and
disease-modifying effects (32,36). Accordingly, TMS could offer a safe
and noninvasive technique for the treatment of AD. However, the
association between the molecular mechanisms responsible for the
treatment of AD after TMS is still elusive. TMS therefore remains a
topic of research, and much progress has been made to find its
mechanism. Studies are continuously being conducted to elucidate
the mechanisms and effects of TMS on the AD-affected brain. At
present, a number of clinical trials are ongoing to further
investigate the molecular mechanisms behind the disease-modifying
effects of TMS on AD and other neurodegenerative disorders
(www.clinicaltrials.gov; Table II).
| Table II.Ongoing clinical trial in AD
patients' treatment with TMS. |
Table II.
Ongoing clinical trial in AD
patients' treatment with TMS.
| Trial no.
(www.clinicaltrials.gov) | Study type | Study Samples to be
Enroll | Disease | Aim | Active group
treatment protocol | Control group
treatment |
|---|
| NCT03121066 | Randomized Clinical
Trial | 45 | AD | Impact on cognitive
and emotional functioning, functionality, and brain
connectivity | iTBS protocol:
1,200 pulses per session for 3.12 min | Sham TMS |
| NCT03224988 | Prospective,
observational, case-control study | 60 | Pre-clinical AD
(aMCI or MCI-AD) | To establish the
structural basis for bilateral brain interactions and the temporal
dynamics of cross-hemispheric communication in in MCI-AD patients
or healthy patients using unilateral or bilateral TMS. | Single-pulse TMS,
dual-coil TMS and EEG | Single-pulse TMS,
dual-coil TMS and EEG over healthy patients |
| NCT03846492 | Double blinded
Randomized Clinical Trial | 90 | AD + Agitation
(mild to moderate agitation) | To assess the
mechanisms and treatment of AD and cortical excitation/inhibition
balance in the DPLFC in AD | tDCS: The direct
current will be delivered at 2 mA for 30 min per day for 2 weeks, 5
days/week. Inhibitory stimulation will be delivered to the frontal
lobes. | Sham tDCS on
healthy comparators |
| NCT04260724 | Interventional,
Prospective, Randomized, Evaluator-blind, Single Center Study | 32 | Mild to Moderate AD
patients | To assess the
change of cognition, mood, ADL, brain structural and functional MRI
following TMS | TMS: 1,600 pulses
for 20 min per day, for 4 weeks (5 days per week) | Sham TMS (no
stimulation) |
| NCT04294888 | Randomized Clinical
Trial | 40 | aMCI due to AD | To evaluate changes
in functional network architecture following rTMS treatment | Excitatory iTBS
pattern | Sham rTMS |
| NCT04555941 | Randomized Clinical
Trial | 60 | Mild cognitive
impairment or early dementia due to Alzheimer's disease | To assess the
cognitive functions | iTBS: 10 sessions,
80% Resting Motor Threshold, 2s stimulation 8s inter-stimulus
interval per train, 20 trains per block, 3 blocks per session with
a 5-min break, 1 session per day | Sham iTBS to the
patients |
| NCT04823819 | Randomized Clinical
Trial | 40 | Mild to moderate
AD | Effectiveness and
safety of rTMS + tDCS on long and short term cognitive
functions | rTMS stimulation:
20 sessions of stimulation with increasing intensity, reaching
maximum in the 4th session over the left DLPFC | Sham rTMS &
Sham tDCS |
| NCT04866979 | Double blinded
Randomized Clinical Trial | 200 | MCI & AD | To evaluate the
clinical efficacy of TBS in conjunction with CT. | Combination of cTBS
+ CT; combination of iTBS + CT; cTBS; iTBS TBS delivery of 600
pulses divided into blocks of 3 pulses at 50 Hz, which are applied
at 5 Hz (every 200 ms), with a stimulation intensity equal to 80%
of the motor threshold value at rest | Cognitive training
only (with placebo TBS) |
The present review highlights the effects of TMS on
neurobiological and neurochemical changes in AD. At the molecular
level, TMS facilitates neural restoration, synaptic plasticity,
neurotransmission, neural regeneration, neural development,
neuroprotection and cognitive rehabilitation, and regulates gene
expression in AD. TMS positively regulates inflammatory and
apoptotic mechanisms, mitochondrial enzymatic activities,
modulation of gene expression (miRNA expression profiles), cell
redox status and the amyloidogenic processes (Fig. 1). Following TMS, the expression of
the following neurochemicals increases: BDNF, NeuN, Nestin,
dopamine, DR4 (32), TrkB
(81), total antioxidant status,
total thiol, native thiol (36),
NMDAR, NMDAR subunits (NR1, NR2A, and NR2B), NGF (82), Bcl-2, Tau (83), NAA/Cr (134), miRNA-106b-25, miR-93 (151,152) and IEG proteins (c-Fos and
zif268) (153). Furthermore, TMS
tends to decrease the levels of total oxidant status, oxidative
stress index, oxidant enzyme activity, disulfide (36), Bax, cleaved caspase-3, p-Tau
(83), miR-107, miR-335-5p,
miR26b-5p (70), BACE1, APP,
CTFs, β-secretase-generated C99 and C89, β-secretase cleavage of
APP proteins, and Aβ peptides (136). In addition, the
disease-modifying effects of TMS treatment depend on the frequency
and site of stimulation (166–168). Neurobiological changes have been
observed differentially with different stimulations (low or high
frequency) (153) and
stimulation sites (i.e., DLPFC, left parietal cortex, hippocampus
and cortex) (32,36,133,136). Furthermore, TMS tends to improve
cognitive functioning (134),
cortical plasticity (49), naming
performance (129), language
function (132), recognition
memory function (135), visual
recognition memory (36), spatial
working memory (32),
visuospatial reasoning and trained associative memory (137) in patients with AD. Therefore,
the anti-AD effects of TMS facilitate an increase in cortical
excitability, induce potentiation, stimulate synaptic plasticity,
recover impaired molecular functions, enhance cognitive functions
and re-establish neural connections in patients with AD.
In addition, there are a limited number of
research-based studies in the literature demonstrating TMS-induced
neurochemical and neurobiological changes in AD. We suggest that
future studies on the therapeutic effects of TMS on oxidative
stress, Ca+ ions, non-neural/glial cells
(oligodendrocytes, astrocytes, microglia and further NSCs), NTFs
(NGF, BDNF, GDNF, CNTF and VEGF), nerve growth factors,
neurotransmitters (dopamine, glutamate, aspartate, GABA and NMDA),
apoptosis-related proteins (Bcl-2, Bax, caspases and TUNEL-positive
cells), genetic expression, miRNA expression, protein expression,
enzymatic activity and metabolites, are required to further explore
the beneficial anti-AD mechanism of TMS in patients with AD.
Knowledge of these changes may clarify the structural and
functional changes in the brain, as well as neuroprotection,
neurodevelopmental and neurorestorative correlation with rTMS in
AD.
Conclusion
The main goal of the present review was to
understand the changes in the neurobiological parameters in the
brain following TMS in neurodegenerative disorders, particularly
AD. Although the number of studies investigating TMS-induced
neurochemical and neurobiological changes in AD is still low, the
anti-AD and disease-modifying effects of TMS can open a pathway for
researchers to further explore its molecular mechanism. As the
neurobiological and clinicopathological alterations and
modifications in AD are not well studied following TMS, more
experimental studies comprising inflammatory, apoptotic,
neurodegenerative, genetic and neuroprotective changes, as well as
functional brain imaging, are required to determine the site- and
stimulation-dependent TMS-induced disease-modifying changes in the
brain. TMS-based NIBS has promising effects on functional recovery
through neural restoration, neuroprotection and neural
differentiation.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Data sharing is not applicable to this article, as
no data sets were generated or analyzed during the current
study.
Authors' contributions
SB, MU, TA and MA were responsible for the
conception of the present study. SB, MU and MA searched the
literature. SB, MU, TA, RAK, AN, ZT, WKY, IT, ADT and SM
contributed to writing the manuscript and figure design. TA, RAK,
AN, ZT, WKY, IT, ADT and SM critically revised and corrected the
manuscript. Data authentication is not applicable. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Guarino A, Favieri F, Boncompagni I,
Agostini F, Cantone M and Casagrande M: Executive functions in
Alzheimer disease: A systematic review. Front Aging Neurosci.
10:4372019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Weiler M, Stieger KC, Long JM and Rapp PR:
Transcranial magnetic stimulation in Alzheimer's disease. Are we
ready? eNeuro. 7:2020.PubMed/NCBI
|
|
3
|
Weller J and Budson A: Current
understanding of Alzheimer's disease diagnosis and treatment.
F1000Res. 7:F1000 Faculty Rev. 11612018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
2020 Alzheimer's disease facts and
figures. Alzheimers Dement. 16:391–460. 2020. View Article : Google Scholar
|
|
5
|
Uddin M, Kabir M, Jakaria M,
Sobarzo-Sánchez E, Barreto GE, Perveen A, Hafeez A, Bin-Jumah MN,
Abdel-Daim MM and Ashraf GM: Exploring the potential of
neuroproteomics in Alzheimer's disease. Curr Top Med Chem.
20:2263–2278. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Koper MJ, Van Schoor E, Ospitalieri S,
Vandenberghe R, Vandenbulcke M, von Arnim CAF, Tousseyn T, Balusu
S, De Strooper B and Thal DR: Necrosome complex detected in
granulovacuolar degeneration is associated with neuronal loss in
Alzheimer's disease. Acta Neuropathol. 139:463–484. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hur JY, Frost GR, Wu X, Crump C, Pan SJ,
Wong E, Barros M, Li T, Nie P, Zhai Y, et al: The innate immunity
protein IFITM3 modulates γ-secretase in Alzheimer's disease. Nat
Aust. 586:735–740. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Butterfield DA and Mattson MP:
Apolipoprotein E and oxidative stress in brain with relevance to
Alzheimer's disease. Neurobiol Dis. 138:1047952020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bhatt S, Puli L and Patil CR: Role of
reactive oxygen species in the progression of Alzheimer's disease.
Drug Discov Today. 26:794–803. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Olajide OJ, Gbadamosi IT, Yawson EO,
Arogundade T, Lewu FS, Ogunrinola KY, Adigun OO, Bamisi O, Lambe E,
Arietarhire LO, et al: Hippocampal degeneration and behavioral
impairment during Alzheimer-like pathogenesis involves glutamate
excitotoxicity. J Mol Neurosci. 71:1205–1220. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhao Y, Zhan JK and Liu Y: A perspective
on roles played by immunosenescence in the pathobiology of
Alzheimer's disease. Aging Dis. 11:1594–1607. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Uddin MS, Al Mamun A, Rahman M, Behl T,
Perveen A, Hafeez A, Bin-Jumah MN, Abdel-Daim MM and Ashraf GM:
Emerging proof of protein misfolding and interactions in
multifactorial Alzheimer's disease. Curr Top Med Chem.
20:2380–2390. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Butterfield DA and Boyd-Kimball DA:
Mitochondrial oxidative and nitrosative stress and Alzheimer
disease. Antioxidants (Basel). 9:8182020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sengoku R: Aging and Alzheimer's disease
pathology. Neuropathol Appl Neurobiol. 40:22–29. 2020.
|
|
15
|
Wegiel J, Flory M, Kuchna I, Nowicki K, Ma
SY, Wegiel J, Badmaev E, Leon M, Wisniewski T and Reisberg B:
Clinicopathological staging of dynamics of neurodegeneration and
neuronal loss in Alzheimer disease. J Neuropathol Exp Neurol.
80:21–44. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pei YA, Davies J, Zhang M and Zhang HT:
The role of synaptic dysfunction in Alzheimer's disease. J
Alzheimer's Dis. 76:49–62. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Teipel SJ, Fritz HC and Grothe MJ;
Alzheimer's Disease Neuroimaging Initiative, : Neuropathologic
features associated with basal forebrain atrophy in Alzheimer
disease. Neurology. 95:e1301–e1311. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Amini M, Pedram MM, Moradi A, Jamshidi M
and Ouchani M: Single and combined neuroimaging techniques for
Alzheimer's disease detection. Comput Intell Neurosci.
2021:95230392021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zetterberg H and Burnham SC: Blood-based
molecular biomarkers for Alzheimer's disease. Mol Brain. 12:262019.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jack CR Jr, Bennett DA, Blennow K,
Carrillo MC, Dunn B, Haeberlein SB, Holtzman DM, Jagust W, Jessen
F, Karlawish J, et al: NIA-AA research framework: Toward a
biological definition of Alzheimer's disease. Alzheimer's Dement.
14:535–562. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee JC, Kim SJ, Hong S and Kim Y:
Diagnosis of Alzheimer's disease utilizing amyloid and tau as fluid
biomarkers. Exp Mol Med. 51:1–10. 2019. View Article : Google Scholar
|
|
22
|
Park JE, Lim DS, Cho YH, Choi KY, Lee JJ,
Kim BC, Lee KH and Lee JS: Plasma contact factors as novel
biomarkers for diagnosing Alzheimer's disease. Biomark Res.
9:52021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zetterberg H: Blood-based biomarkers for
Alzheimer's disease-An update. J Neurosci Methods. 319:2–6. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Young PNE, Estarellas M, Coomans E,
Srikrishna M, Beaumont H, Maass A, Venkataraman AV, Lissaman R,
Jiménez D, Betts MJ, et al: Imaging biomarkers in
neurodegeneration: Current and future practices. Alzheimers Res
Ther. 12:492020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
O'Dell RS, Mecca AP, Chen MK, Naganawa M,
Toyonaga T, Lu Y, Godek TA, Harris JE, Bartlett HH, Banks ER, et
al: Association of Aβ deposition and regional synaptic density in
early Alzheimer's disease: A PET imaging study with
[11C]UCB-J. Alzheimer's Res Ther. 13:112021. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sujathakumari B, Shetty MC, Lakshitha H,
Mehulkumar PJ and Suma S: Predictive analysis for early detection
of Alzheimer's disease. Data Intelligence and Cognitive
Informatics. Springer; pp. 709–723. 2021, View Article : Google Scholar
|
|
27
|
Song A, Johnson N, Ayala A and Thompson
AC: Brain Optical coherence tomography in patients with Alzheimer's
disease: What can it tell us? Eye. 13:1–20. 2021.
|
|
28
|
Segal Y, Segal L, Blumenfeld-Katzir T,
Sasson E, Poliansky V, Loeb E, Levy A, Alter A and Bregman N: The
effect of electromagnetic field treatment on recovery from ischemic
stroke in a rat stroke model: Clinical, imaging, and pathological
findings. Stroke Res Treat. 2016:69419462016.PubMed/NCBI
|
|
29
|
Lefaucheur JP, Aleman A, Baeken C,
Benninger DH, Brunelin J, Di Lazzaro V, Filipović SR, Grefkes C,
Hasan A, Hummel FC, et al: Evidence-based guidelines on the
therapeutic use of repetitive transcranial magnetic stimulation
(rTMS): An update (2014–2018). Clinical neurophysiology.
131:474–528. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ba M, Ma G, Ren C, Sun X and Kong M:
Repetitive transcranial magnetic stimulation for treatment of
lactacystin-induced Parkinsonian rat model. Oncotarget.
8:50921–50929. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tasset I, Medina FJ, Jimena I, Agüera E,
Gascón F, Feijóo M, Sánchez-López F, Luque E, Peña J, Drucker-Colín
R and Túnez I: Neuroprotective effects of extremely low-frequency
electromagnetic fields on a Huntington's disease rat model: Effects
on neurotrophic factors and neuronal density. Neuroscience.
209:54–63. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Choung JS, Kim JM, Ko MH, Cho DS and Kim
M: Therapeutic efficacy of repetitive transcranial magnetic
stimulation in an animal model of Alzheimer's disease. Sci Rep.
11:4372021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chou YH, Ton That V and Sundman M: A
systematic review and meta-analysis of rTMS effects on cognitive
enhancement in mild cognitive impairment and Alzheimer's disease.
Neurobiol Aging. 86:1–10. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Weise K, Numssen O, Thielscher A,
Hartwigsen G and Knösche TR: A novel approach to localize cortical
TMS effects. NeuroImage. 209:1164862020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zorzo C, Higarza SG, Méndez M, Martínez
JA, Pernía AM and Arias JL: High frequency repetitive transcranial
magnetic stimulation improves neuronal activity without affecting
astrocytes and microglia density. Brain Res Bull. 150:13–20. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Velioglu HA, Hanoglu L, Bayraktaroglu Z,
Toprak G, Guler EM, Bektay MY, Mutlu-Burnaz O and Yulug B: Left
lateral parietal rTMS improves cognition and modulates resting
brain connectivity in patients with Alzheimer's disease: Possible
role of BDNF and oxidative stress. Neurobiol Learn Mem.
180:1074102021. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Luo J, Zheng H, Zhang L, Zhang Q, Li L,
Pei Z and Hu X: High-frequency repetitive transcranial magnetic
stimulation (rTMS) improves functional recovery by enhancing
neurogenesis and activating BDNF/TrkB signaling in ischemic rats.
Int J Mol Sci. 18:4552017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Heath A, Taylor J and McNerney MW: rTMS
for the treatment of Alzheimer's disease: Where should we be
stimulating? Expert Rev Neurother. 18:903–905. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Bashir S, Mizrahi I, Weaver K, Fregni F
and Pascual-Leone A: Assessment and modulation of neural plasticity
in rehabilitation with transcranial magnetic stimulation. PM R. 2
12 Suppl 2:S253–S268. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Mann SK and Malhi NK: Repetitive
transcranial magnetic stimulation. StatPearls StatPearls Publishing
Copyright©. 2021, StatPearls Publishing LLC.; Treasure
Island (FL): 2021
|
|
41
|
Miniussi C and Ruzzoli M: Transcranial
stimulation and cognition. Handb Clin Neurol. 116:739–750. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Barker AT, Jalinous R and Freeston IL:
Non-invasive magnetic stimulation of human motor cortex. Lancet.
1:1106–1107. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Uzair M, Abualait T, Arshad M, Yoo WK, Mir
A, Bunyan RF and Bashir S: Transcranial magnetic stimulation in
animal models of neurodegeneration. Neural Regen Res. 17:251–265.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Perera T, George MS, Grammer G, Janicak
PG, Pascual-Leone A and Wirecki TS: The clinical TMS society
consensus review and treatment recommendations for TMS therapy for
major depressive disorder. Brain Stimul. 9:336–346. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
George MS: Transcranial magnetic
stimulation for the treatment of depression. Expert Rev Neurother.
10:1761–1772. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Hawken ER, Dilkov D, Kaludiev E, Simek S,
Zhang F and Milev R: Transcranial magnetic stimulation of the
supplementary motor area in the treatment of obsessive-compulsive
disorder: A multi-site study. Int J Mol Sci. 17:4202016. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Starling AJ, Tepper SJ, Marmura MJ, Shamim
EA, Robbins MS, Hindiyeh N, Charles AC, Goadsby PJ, Lipton RB,
Silberstein SD, et al: A multicenter, prospective, single arm, open
label, observational study of sTMS for migraine prevention (ESPOUSE
Study). Cephalalgia. 38:1038–1048. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Moussavi Z, Rutherford G, Lithgow B,
Millikin C, Modirrousta M, Mansouri B, Wang X, Omelan C, Fellows L,
Fitzgerald P and Koski L: Repeated transcranial magnetic
stimulation for improving cognition in patients with Alzheimer
disease: Protocol for a randomized, double-blind,
placebo-controlled trial. JMIR Res Protoc. 10:e251442021.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Li X, Qi G, Yu C, Lian G, Zheng H, Wu S,
Yuan TF and Zhou D: Cortical plasticity is correlated with
cognitive improvement in Alzheimer's disease patients after rTMS
treatment. Brain Stimul. 14:503–510. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Mi TM, Garg S, Ba F, Liu AP, Liang PP, Gao
LL, Jia Q, Xu EH, Li KC, Chan P and McKeown MJ: Repetitive
transcranial magnetic stimulation improves Parkinson's freezing of
gait via normalizing brain connectivity. NPJ Parkinsons Dis.
6:162020. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Yang X, Song L and Liu Z: The effect of
repetitive transcranial magnetic stimulation on a model rat of
Parkinson's disease. Neuroreport. 21:268–272. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Spielberg B: What is the success rate of
TMS therapy? 2020.
|
|
53
|
Wagner T, Valero-Cabre A and Pascual-Leone
A: Noninvasive human brain stimulation. Annu Rev Biomed Eng.
9:527–65. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Klomjai W, Katz R and Lackmy-Vallée A:
Basic principles of transcranial magnetic stimulation (TMS) and
repetitive TMS (rTMS). Ann Phys Rehabil Med. 58:208–213. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Bolognini N and Ro T: Transcranial
magnetic stimulation: Disrupting neural activity to alter and
assess brain function. J Neurosci. 30:9647–9650. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Cuypers K and Marsman A: Transcranial
magnetic stimulation and magnetic resonance spectroscopy:
Opportunities for a bimodal approach in human neuroscience.
Neuroimage. 224:1173942021. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Chail A, Saini RK, Bhat P, Srivastava K
and Chauhan V: Transcranial magnetic stimulation: A review of its
evolution and current applications. Ind Psychiatry J. 27:1722018.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Habib S, Hamid U, Jamil A, Zainab AZ,
Yousuf T, Habib S, Tariq SM and Ali F: Transcranial magnetic
stimulation as a therapeutic option for neurologic and psychiatric
illnesses. Cureus. 10:e34562018.PubMed/NCBI
|
|
59
|
Eldaief MC, Press DZ and Pascual-Leone A:
Transcranial magnetic stimulation in neurology: A review of
established and prospective applications. Neurol Clin Pract.
3:519–526. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Alomar M, Yoo W-K, Vernet M, Murtaza G,
Rotenberg A and Bashir S: Human brain connectivity in response to
paired pulse TMS paradigm. Brain Stimul. 10:3532017. View Article : Google Scholar
|
|
61
|
Kim TD, Hong G, Kim J and Yoon S:
Cognitive enhancement in neurological and psychiatric disorders
using transcranial magnetic stimulation (TMS): A review of
modalities, potential mechanisms and future implications. Exp
Neurobiol. 28:1–16. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Fried PJ, Jannati A, Davila-Pérez P and
Pascual-Leone A: Reproducibility of single-pulse, paired-pulse, and
intermittent theta-burst TMS measures in healthy aging, type-2
diabetes, and Alzheimer's disease. Front Aging Neurosci. 9:2632017.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Chervyakov AV, Chernyavsky AY, Sinitsyn DO
and Piradov MA: Possible mechanisms underlying the therapeutic
effects of transcranial magnetic stimulation. Front Hum Neurosci.
9:3032015. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Agarwal S, Koch G, Hillis AE, Huynh W,
Ward NS, Vucic S and Kiernan MC: Interrogating cortical function
with transcranial magnetic stimulation: Insights from
neurodegenerative disease and stroke. J Neurol Neurosurg
Psychiatry. 90:47–57. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Jackson J, Jambrina E, Li J, Marston H,
Menzies F, Phillips K and Gilmour G: Targeting the synapse in
Alzheimer's disease. Front Neurosci. 13:7352019. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Wang X, Mao Z, Ling Z and Yu X: Repetitive
transcranial magnetic stimulation for cognitive impairment in
Alzheimer's disease: A meta-analysis of randomized controlled
trials. J Neurol. 267:791–801. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Holczer A, Németh VL, Vékony T, Vécsei L,
Klivényi P and Must A: Non-invasive brain stimulation in
Alzheimer's disease and mild cognitive impairment-a
state-of-the-art review on methodological characteristics and
stimulation parameters. Front Hum Neurosci. 14:1792020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Guerra A, Assenza F, Bressi F, Scrascia F,
Del Duca M, Ursini F, Vollaro S, Trotta L, Tombini M, Chisari C and
Ferreri F: Transcranial magnetic stimulation studies in Alzheimer's
disease. Int J Alzheimers Dis. 2011:2638172011.PubMed/NCBI
|
|
69
|
Yang HY, Liu Y, Xie JC, Liu NN and Tian X:
Effects of repetitive transcranial magnetic stimulation on synaptic
plasticity and apoptosis in vascular dementia rats. Behav Brain
Res. 281:149–155. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Capelli E, Torrisi F, Venturini L, Granato
M, Fassina L, Lupo GFD and Ricevuti G: Low-frequency pulsed
electromagnetic field is able to modulate miRNAs in an experimental
cell model of Alzheimer's disease. J Healthcare Eng.
2017:25302702017. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Xiao N and Le QT: Neurotrophic factors and
their potential applications in tissue regeneration. Arch Immunol
Ther Exp (Warsz). 64:89–99. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Sampaio TB, Savall AS, Gutierrez MEZ and
Pinton S: Neurotrophic factors in Alzheimer's and Parkinson's
diseases: Implications for pathogenesis and therapy. Neural Regen
Res. 12:549–557. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Budni J, Bellettini-Santos T, Mina F,
Garcez ML and Zugno AI: The involvement of BDNF, NGF and GDNF in
aging and Alzheimer's disease. Aging Dis. 6:331–341. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Miranda M, Morici JF, Zanoni MB and
Bekinschtein P: Brain-derived neurotrophic factor: A key molecule
for memory in the healthy and the pathological brain. Front Cell
Neurosci. 13:3632019. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Ballinger EC, Ananth M, Talmage DA and
Role LW: Basal forebrain cholinergic circuits and signaling in
cognition and cognitive decline. Neuron. 91:1199–1218. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Martinez JL, Zammit MD, West NR, Christian
BT and Bhattacharyya A: Basal forebrain cholinergic neurons:
Linking down syndrome and Alzheimer's disease. Front Aging
Neurosci. 13:7038762021. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Serrano-Pozo A, Frosch MP, Masliah E and
Hyman BT: Neuropathological alterations in Alzheimer disease. Cold
Spring Harb Perspect Med. 1:a0061892011. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Pang Y and Shi M: Repetitive transcranial
magnetic stimulation improves mild cognitive impairment associated
with Alzheimer's disease in mice by modulating the
miR-567/NEUROD2/PSD95 axis. Neuropsychiatr Dis Treat. 17:2151–2161.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Wang ZH, Xiang J, Liu X, Yu SP,
Manfredsson FP, Sandoval IM, Wu S, Wang JZ and Ye K: Deficiency in
BDNF/TrkB neurotrophic activity stimulates δ-secretase by
upregulating C/EBPβ in Alzheimer's disease. Cell Rep.
28:655–669.e5. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Ng TKS, Ho CSH, Tam WWS, Kua EH and Ho RC:
Decreased serum brain-derived neurotrophic factor (BDNF) levels in
patients with Alzheimer's disease (AD): A systematic review and
meta-analysis. Int J Mol Sci. 20:2572019. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Chen X, Dong GY and Wang LX:
High-frequency transcranial magnetic stimulation protects APP/PS1
mice against Alzheimer's disease progress by reducing APOE and
enhancing autophagy. Brain Behavior. 10:e017402020. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Tan T, Xie J, Liu T, Chen X, Zheng X, Tong
Z and Tian X: Low-frequency (1Hz) repetitive transcranial magnetic
stimulation (rTMS) reverses Aβ(1–42)-mediated memory deficits in
rats. Exp Gerontol. 48:786–794. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Chen X, Chen S, Liang W and Ba F:
Administration of repetitive transcranial magnetic stimulation
attenuates A β1-42-induced Alzheimer's disease in mice
by activating β-catenin signaling. Biomed Res Int.
2019:14317602019.PubMed/NCBI
|
|
84
|
Schaller G, Sperling W,
Richter-Schmidinger T, Mühle C, Heberlein A, Maihöfner C, Kornhuber
J and Lenz B: Serial repetitive transcranial magnetic stimulation
(rTMS) decreases BDNF serum levels in healthy male volunteers. J
Neural Transm (Vienna). 121:307–313. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Gaede G, Hellweg R, Zimmermann H, Brandt
AU, Dörr J, Bellmann-Strobl J, Zangen A, Paul F and Pfueller CF:
Effects of deep repetitive transcranial magnetic stimulation on
brain-derived neurotrophic factor serum concentration in healthy
volunteers. Neuropsychobiology. 69:112–119. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Yulug B, Hanoglu L, Khanmammadov E, Duz
OA, Polat B, Hanoglu T, Gunal MY and Kilic E: Beyond the
therapeutic effect of rTMS in Alzheimer's disease: A possible
neuroprotective role of hippocampal BDNF?: A minireview. Mini Rev
Med Chem. 18:1479–1485. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Huang WJ, Zhang X and Chen WW: Role of
oxidative stress in Alzheimer's disease. Biomed Rep. 4:519–522.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Cheignon C, Tomas M, Bonnefont-Rousselot
D, Faller P, Hureau C and Collin F: Oxidative stress and the
amyloid beta peptide in Alzheimer's disease. Redox Biol.
14:450–464. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Chen Z and Zhong C: Oxidative stress in
Alzheimer's disease. Neurosci Bull. 30:271–281. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Perry G, Cash AD and Smith MA: Alzheimer
disease and oxidative stress. J Biomed Biotechnol. 2:120–123. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Butterfield DA and Halliwell B: Oxidative
stress, dysfunctional glucose metabolism and Alzheimer disease. Nat
Rev Neurosci. 20:148–160. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Molinari C, Morsanuto V, Ruga S, Notte F,
Farghali M, Galla R and Uberti F: The role of BDNF on
aging-modulation markers. Brain Sci. 10:2852020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Umeno A, Biju V and Yoshida Y: In vivo ROS
production and use of oxidative stress-derived biomarkers to detect
the onset of diseases such as Alzheimer's disease, Parkinson's
disease, and diabetes. Free Radical Res. 51:413–427. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Durmaz O, Ispir E, Baykan H, Alisik M and
Erel Ö: The impact of repetitive transcranial magnetic stimulation
on oxidative stress in subjects with medication-resistant
depression. J ECT. 34:127–131. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Niimi M, Hashimoto K, Kakuda W, Miyano S,
Momosaki R, Ishima T and Abo M: Role of brain-derived neurotrophic
factor in beneficial effects of repetitive transcranial magnetic
stimulation for upper limb hemiparesis after stroke. PLoS One.
11:e01522412016. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Medina-Fernandez FJ, Escribano BM, Agüera
E, Aguilar-Luque M, Feijoo M, Luque E, Garcia-Maceira FI,
Pascual-Leone A, Drucker-Colin R and Tunez I: Effects of
transcranial magnetic stimulation on oxidative stress in
experimental autoimmune encephalomyelitis. Free Radical Res.
51:460–469. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Snowden SG, Ebshiana AA, Hye A, Pletnikova
O, O'Brien R, Yang A, Troncoso J, Legido-Quigley C and Thambisetty
M: Neurotransmitter imbalance in the brain and Alzheimer's disease
pathology. J Alzheimers Dis. 72:35–43. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Svob Strac D, Muck-Seler D and Pivac N:
Neurotransmitter measures in the cerebrospinal fluid of patients
with Alzheimer's disease: A review. Psychiatr Danub. 27:14–24.
2015.PubMed/NCBI
|
|
99
|
Kaur S, DasGupta G and Singh S: Altered
neurochemistry in Alzheimer's disease: Targeting neurotransmitter
receptor mechanisms and therapeutic strategy. Neurophysiology.
51:293–309. 2019. View Article : Google Scholar
|
|
100
|
Speranza L, di Porzio U, Viggiano D, de
Donato A and Volpicelli F: Dopamine: The neuromodulator of
long-term synaptic plasticity, reward and movement control. Cells.
10:7352021. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
He Z, Jiang Y, Gu S, Wu D, Feng G, Ma X,
Huang JH and Wang F: The aversion function of the limbic
dopaminergic neurons and their roles in functional neurological
disorders. Front Cell Dev Biol. 9:7137622021. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Pan X, Kaminga AC, Wen SW, Wu X,
Acheampong K and Liu A: Dopamine and dopamine receptors in
Alzheimer's disease: A systematic review and network meta-analysis.
Front Aging Neurosci. 11:1752019. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
D'Amelio M, Puglisi-Allegra S and Mercuri
N: The role of dopaminergic midbrain in Alzheimer's disease:
Translating basic science into clinical practice. Pharmacol Res.
130:414–419. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Nobili A, Latagliata EC, Viscomi MT,
Cavallucci V, Cutuli D, Giacovazzo G, Krashia P, Rizzo FR, Marino
R, Federici M, et al: Dopamine neuronal loss contributes to memory
and reward dysfunction in a model of Alzheimer's disease. Nat
Commun. 8:147272017. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Malik S, Jacobs M, Cho SS, Boileau I,
Blumberger D, Heilig M, Wilson A, Daskalakis ZJ, Strafella AP,
Zangen A and Le Foll B: Deep TMS of the insula using the H-coil
modulates dopamine release: A crossover [11C] PHNO-PET
pilot trial in healthy humans. Brain Imaging Behav. 12:1306–1317.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Cho SS and Strafella AP: rTMS of the left
dorsolateral prefrontal cortex modulates dopamine release in the
ipsilateral anterior cingulate cortex and orbitofrontal cortex.
PLoS One. 4:e67252009. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Liu J, Chang L, Song Y, Li H and Wu Y: The
role of NMDA receptors in Alzheimer's disease. Front Neurosci.
13:432019. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Zhang Y, Li P, Feng J and Wu M:
Dysfunction of NMDA receptors in Alzheimer's disease. Neurol Sci.
37:1039–1047. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Kodis EJ, Choi S, Swanson E, Ferreira G
and Bloom GS: Dementia N-methyl-D-aspartate receptor-mediated
calcium influx connects amyloid-β oligomers to ectopic neuronal
cell cycle reentry in Alzheimer's disease. Alzheimers Dement.
14:1302–1312. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Tsang SW, Vinters HV, Cummings JL, Wong
PT, Chen CP and Lai MK: Alterations in NMDA receptor subunit
densities and ligand binding to glycine recognition sites are
associated with chronic anxiety in Alzheimer's disease. Neurobiol.
Aging. 29:1524–1532. 2008.PubMed/NCBI
|
|
111
|
Battaglia F, Wang HY, Ghilardi MF, Gashi
E, Quartarone A, Friedman E and Nixon RA: Cortical plasticity in
Alzheimer's disease in humans and rodents. Biol Psychiatry.
62:1405–1412. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Zhang N, Xing M, Wang Y, Tao H and Cheng
Y: Repetitive transcranial magnetic stimulation enhances spatial
learning and synaptic plasticity via the VEGF and BDNF-NMDAR
pathways in a rat model of vascular dementia. Neuroscience.
311:284–291. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Niimi M, Fujita Y, Ishima T, Hashimoto K,
Sasaki N, Hara T, Yamada N and Abo M: Role of D-serine in the
beneficial effects of repetitive transcranial magnetic stimulation
in post-stroke patients. Acta Neuropsychiatr. 32:1–22. 2020.
View Article : Google Scholar
|
|
114
|
Chi H, Chang H-Y and Sang TK: Neuronal
cell death mechanisms in major neurodegenerative diseases. Int J
Mol Sci. 19:30822018. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Obulesu M and Lakshmi MJ: Apoptosis in
Alzheimer's disease: An understanding of the physiology, pathology
and therapeutic avenues. Neurochem Res. 39:2301–2312. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Paradis E, Douillard H, Koutroumanis M,
Goodyer C and LeBlanc A: Amyloid beta peptide of Alzheimer's
disease downregulates Bcl-2 and upregulates bax expression in human
neurons. J Neurosci. 16:7533–7539. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Guo F, Lou J, Han X, Deng Y and Huang X:
Repetitive transcranial magnetic stimulation ameliorates cognitive
impairment by enhancing neurogenesis and suppressing apoptosis in
the hippocampus in rats with ischemic stroke. Front Physiol.
8:5592017. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Yulug B, Hanoglu L, Kilic E, Polat B and
Rüdiger Schabitz W: The neuroprotective role of repetitive
transcranial magnetic stimulation (rTMS) for neurodegenerative
diseases: A short review on experimental studies. Mini Rev Med
Chem. 16:1269–1273. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Cappa SF, Binetti G, Pezzini A, Padovani
A, Rozzini L and Trabucchi M: Object and action naming in
Alzheimer's disease and frontotemporal dementia [see comment].
Neurology. 50:351–355. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Almor A, Aronoff JM, MacDonald MC,
Gonnerman LM, Kempler D, Hintiryan H, Hayes UL, Arunachalam S and
Andersen ES: A common mechanism in verb and noun naming deficits in
Alzheimer's patients. Brain Lang. 111:8–19. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
de Almeida RG, Mobayyen F, Antal C,
Kehayia E, Nair VP and Schwartz G: Category-specific verb-semantic
deficits in Alzheimer's disease: Evidence from static and dynamic
action naming. Cogn Neuropsychol. 38:1–26. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Kumar S, Zomorrodi R, Ghazala Z, Goodman
MS, Blumberger DM, Cheam A, Fischer C, Daskalakis ZJ, Mulsant BH,
Pollock BG and Rajji TK: Extent of dorsolateral prefrontal cortex
plasticity and its association with working memory in patients with
Alzheimer disease. JAMA Psychiatry. 74:1266–1274. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Kumar S, Iwata Y, Zomorrodi R, Blumberger
DM, Fischer CE, Daskalakis ZJ, Mulsant BH, Pollock BG,
Graff-Guerrero A and Rajji TK: Dorsolateral prefrontal cortex
metabolites and their relationship with plasticity in Alzheimer's
disease: Biomarkers (non-neuroimaging)/novel biomarkers. Alzheimers
Dement. 16:e0458792020. View Article : Google Scholar
|
|
124
|
Alder G, Signal N, Olsen S and Taylor D: A
systematic review of paired associative stimulation (PAS) to
modulate lower limb corticomotor excitability: Implications for
stimulation parameter selection and experimental design. Front
Neurosci. 13:8952019. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Silverstein J, Cortes M, Tsagaris KZ,
Climent A, Gerber LM, Oromendia C, Fonzetti P, Ratan RR, Kitago T,
Iacoboni M, et al: Paired associative stimulation as a tool to
assess plasticity enhancers in chronic stroke. Front Neurosci.
13:7922019. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Motta C, Di Lorenzo F, Ponzo V,
Pellicciari MC, Bonnì S, Picazio S, Mercuri NB, Caltagirone C,
Martorana A and Koch G: Transcranial magnetic stimulation predicts
cognitive decline in patients with Alzheimer's disease. J Neurol
Neurosurg Psychiatry. 89:1237–1242. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Bashir S, Al-Hussain F, Hamza A, Shareefi
GF, Abualait T and Yoo WK: Role of single low pulse intensity of
transcranial magnetic stimulation over the frontal cortex for
cognitive function. Front Hum Neurosci. 14:2052020. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Nardone R, Tezzon F, Höller Y, Golaszewski
S, Trinka E and Brigo F: Transcranial magnetic stimulation
(TMS)/repetitive TMS in mild cognitive impairment and Alzheimer's
disease. Acta Neurol Scand. 129:351–366. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Cappa SF, Sandrini M, Rossini PM, Sosta K
and Miniussi C: The role of the left frontal lobe in action naming
rTMS evidence. Neurology. 59:720–723. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Cotelli M, Manenti R, Cappa SF, Geroldi C,
Zanetti O, Rossini PM and Miniussi C: Effect of transcranial
magnetic stimulation on action naming in patients with Alzheimer
disease. Arch Neurol. 63:1602–1604. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Cotelli M, Manenti R, Cappa SF, Zanetti O
and Miniussi C: Transcranial magnetic stimulation improves naming
in Alzheimer disease patients at different stages of cognitive
decline. Eur J Neurol. 15:1286–1292. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Cotelli M, Calabria M, Manenti R, Rosini
S, Zanetti O, Cappa SF and Miniussi C: Improved language
performance in Alzheimer disease following brain stimulation. J
Neurol Neurosurg Psychiatry. 82:794–797. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Ahmed MA, Darwish ES, Khedr EM, El Serogy
YM and Ali AM: Effects of low versus high frequencies of repetitive
transcranial magnetic stimulation on cognitive function and
cortical excitability in Alzheimer's dementia. J Neurology.
259:83–92. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Zhang F, Qin Y, Xie L, Zheng C, Huang X
and Zhang M: High-frequency repetitive transcranial magnetic
stimulation combined with cognitive training improves cognitive
function and cortical metabolic ratios in Alzheimer's disease. J
Neural Transm (Vienna). 126:1081–1094. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Turriziani P, Smirni D, Mangano GR,
Zappalà G, Giustiniani A, Cipolotti L and Oliveri M: Low-frequency
repetitive transcranial magnetic stimulation of the right
dorsolateral prefrontal cortex enhances recognition Memory in
Alzheimer's disease. J Alzheimers Dis. 72:613–622. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Huang Z, Tan T, Du Y, Chen L, Fu M, Yu Y,
Zhang L, Song W and Dong Z: Low-frequency repetitive transcranial
magnetic stimulation ameliorates cognitive function and synaptic
plasticity in APP23/PS45 mouse model of Alzheimer's disease. Front
Aging Neurosci. 9:2922017. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Bagattini C, Zanni M, Barocco F, Caffarra
P, Brignani D, Miniussi C and Defanti CA: Enhancing cognitive
training effects in Alzheimer's disease: rTMS as an add-on
treatment. Brain Stimul. 13:1655–1664. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Huerta PT and Volpe BT: Transcranial
magnetic stimulation, synaptic plasticity and network oscillations.
J Neuroeng Rehabil. 6:72009. View Article : Google Scholar : PubMed/NCBI
|
|
139
|
Liu W, Ma R and Yuan Y:
Post-transcriptional regulation of genes related to biological
behaviors of gastric cancer by long noncoding RNAs and MicroRNAs. J
Cancer. 8:4141–4154. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Catalanotto C, Cogoni C and Zardo G:
MicroRNA in control of gene expression: An overview of nuclear
functions. Int J Mol Sci. 17:17122016. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Zhao J, Yue D, Zhou Y, Jia L, Wang H, Guo
M, Xu H, Chen C, Zhang J and Xu L: The role of MicroRNAs in Aβ
deposition and Tau phosphorylation in Alzheimer's disease. Front
Neurol. 8:3422017. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Konovalova J, Gerasymchuk D, Parkkinen I,
Chmielarz P and Domanskyi A: Interplay between MicroRNAs and
oxidative stress in neurodegenerative diseases. Int J Mol Sci.
20:60552019. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Friedman RC, Farh KK, Burge CB and Bartel
DP: Most mammalian mRNAs are conserved targets of microRNAs. Genome
Res. 19:92–105. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Rooda I, Hensen K, Kaselt B, Kasvandik S,
Pook M, Kurg A, Salumets A and Velthut-Meikas A: Target prediction
and validation of microRNAs expressed from FSHR and aromatase genes
in human ovarian granulosa cells. Sci Rep. 10:23002020. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Song M: miRNAs-dependent regulation of
synapse formation and function. Genes Genomics. 42:837–845. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Hu Z and Li Z: miRNAs in synapse
development and synaptic plasticity. Curr Opin Neurobiol. 45:24–31.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Siedlecki-Wullich D, Català-Solsona J,
Fábregas C, Hernández I, Clarimon J, Lleó A, Boada M, Saura CA,
Rodríguez-Álvarez J and Miñano-Molina AJ: Altered microRNAs related
to synaptic function as potential plasma biomarkers for Alzheimer's
disease. Alzheimers Res Ther. 11:462019. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Wei W, Wang ZY, Ma LN, Zhang TT, Cao Y and
Li H: MicroRNAs in Alzheimer's disease: Function and potential
applications as diagnostic biomarkers. Front Mol Neurosci.
13:1602020. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Angelucci F, Cechova K, Valis M, Kuca K,
Zhang B and Hort J: MicroRNAs in Alzheimer's disease: Diagnostic
markers or therapeutic agents? Front Pharmacol. 10:6652019.
View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Amakiri N, Kubosumi A, Tran J and Reddy
PH: Amyloid beta and microRNAs in Alzheimer's disease. Front
Neurosci. 13:4302019. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Liu H, Han XH, Chen H, Zheng CX, Yang Y
and Huang XL: Repetitive magnetic stimulation promotes neural stem
cells proliferation by upregulating MiR-106b in vitro. J Huazhong
Univ Sci Technolog Med Sci. 35:766–772. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Liu H, Li G, Ma C, Chen Y, Wang J and Yang
Y: Repetitive magnetic stimulation promotes the proliferation of
neural progenitor cells via modulating the expression of miR-106b.
Int J Mol Med. 42:3631–3639. 2018.PubMed/NCBI
|
|
153
|
Aydin-Abidin S, Trippe J, Funke K, Eysel
UT and Benali A: High- and low-frequency repetitive transcranial
magnetic stimulation differentially activates c-Fos and zif268
protein expression in the rat brain. Exp Brain Res. 188:249–261.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Perez FP, Maloney B, Chopra N, Morisaki JJ
and Lahiri DK: Repeated electromagnetic field stimulation lowers
amyloid-β peptide levels in primary human mixed brain tissue
cultures. Sci Rep. 11:6212021. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Loo CK, McFarquhar TF and Mitchell PB: A
review of the safety of repetitive transcranial magnetic
stimulation as a clinical treatment for depression. Int J
Neuropsychopharmacol. 11:131–147. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Najib U and Horvath J: Transcranial
magnetic stimulation (TMS) safety considerations and
recommendations. Neuromethods. 89:15–30. 2014. View Article : Google Scholar
|
|
157
|
Wassermann EM: Side effects of repetitive
transcranial magnetic stimulation. Depress Anxiety. 12:124–129.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
158
|
Dhamne SC, Kothare RS, Yu C, Hsieh TH,
Anastasio EM, Oberman L, Pascual-Leone A and Rotenberg A: A measure
of acoustic noise generated from transcranial magnetic stimulation
coils. Brain Stimul. 7:432–434. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
159
|
Varone G, Hussain Z, Sheikh Z, Howard A,
Boulila W, Mahmud M, Howard N, Morabito FC and Hussain A: Real-time
artifacts reduction during TMS-EEG co-registration: A comprehensive
review on technologies and procedures. Sensors (Basel). 21:6372021.
View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Duecker F and Sack AT: Rethinking the role
of sham TMS. Front Psychol. 6:2102015. View Article : Google Scholar : PubMed/NCBI
|
|
161
|
Wassermann EM: Risk and safety of
repetitive transcranial magnetic stimulation: Report and suggested
guidelines from the International Workshop on the Safety of
Repetitive Transcranial Magnetic Stimulation, June 5–7, 1996.
Electroencephalogr Clin Neurophysiol. 108:1–16. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
162
|
Chen R, Gerloff C, Classen J, Wassermann
EM, Hallett M and Cohen LG: Safety of different inter-train
intervals for repetitive transcranial magnetic stimulation and
recommendations for safe ranges of stimulation parameters.
Electroencephalogr Clin Neurophysiol. 105:415–421. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
163
|
Rossi S, Hallett M, Rossini PM and
Pascual-Leone A; Safety of TMS Consensus Group, : Safety, ethical
considerations, and application guidelines for the use of
transcranial magnetic stimulation in clinical practice and
research. Clin Neurophysiol. 120:2008–2039. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
164
|
DeTure MA and Dickson DW: The
neuropathological diagnosis of Alzheimer's disease. Mol
Neurodegener. 14:322019. View Article : Google Scholar : PubMed/NCBI
|
|
165
|
Jellinger KA: Neuropathology of the
Alzheimer's continuum: An update. Free Neuropathol. 1:32. 2020.
|
|
166
|
Speer AM, Kimbrell TA, Wassermann EM, D
Repella J, Willis MW, Herscovitch P and Post RM: Opposite effects
of high and low frequency rTMS on regional brain activity in
depressed patients. Biol Psychiatry. 48:1133–1141. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
167
|
Ilmoniemi RJ, Mäki H, Saari J, Salvador R
and Miranda PC: The frequency-dependent neuronal length constant in
transcranial magnetic stimulation. Front Cell Neurosci. 10:1942016.
View Article : Google Scholar : PubMed/NCBI
|
|
168
|
Freedberg M, Reeves JA, Hussain SJ,
Zaghloul KA and Wassermann EM: Identifying site- and
stimulation-specific TMS-evoked EEG potentials using a quantitative
cosine similarity metric. PLoS One. 15:e02161852020. View Article : Google Scholar : PubMed/NCBI
|