Introduction
Ovarian cancer is ranked as one of the most
dangerous gynecological cancers, which is associated with a high
rate of mortality (1). According
to the World Health Organization, ~313,959 cases of ovarian cancer
are diagnosed annually and >207,252 deaths are recorded, making
ovarian cancer the seventh most common type of cancer and the fifth
most common cause of cancer-associated death worldwide (2–5).
Notably, >70% of all ovarian cancer cases are diagnosed at a
late clinical stage (stage III or IV) according to the
International Federation of Gynecology and Obstetrics (FIGO)
classification (1,6,7).
The reason for the late diagnosis of ovarian cancer is the
asymptomatic course of the disease in the early stages, the
non-specificity of clinical symptoms and the lack of parameters
useful for early diagnosis. The incidence of ovarian cancer is
increasing, particularly in developed countries; therefore, there
is a need for further research to better understand the mechanisms
involved in the pathogenesis of this disease (5,8,9).
An important role in the formation and development
of ovarian cancer is attributed to disturbances in the immune
system, particularly involving interactions between immune cells
and tumor cells. Interactions occurring in the tumor
microenvironment include both direct interactions and indirect
actions involving soluble mediators, including chemokines and their
receptors. Numerous studies have reported the involvement of
chemokines and their receptors in several physiological and
pathological processes, including tumorigenesis and chronic
inflammation (10–13). In the body, inflammatory mediators
aim to eliminate pathogenic agents and restore homeostasis;
however, excessive inflammation can lead to overproduction of
cytokines and chemokines, which result in the formation of a
network of interrelationships that can directly affect tumor
development. Through these networks, the signaling process is
disrupted, surrounding cells are stimulated, new blood vessels are
formed and, consequently, tumors can grow (14–16). Furthermore, it has been shown that
in the course of a number of malignancies, cancer cells have the
ability to secrete the chemokine C-X-C motif chemokine ligand 8
(CXCL8, also Interleukin 8-IL-8) in an autocrine or paracrine
manner (13). Chemokines can also
be produced by tumor-infiltrating leukocytes and tumor-associated
fibroblasts. Cancer cells are also capable of taking control of
host cell signaling and regulatory mechanisms responsible for the
synthesis of various growth factors using chemokine and receptor
pathways (17).
The CXCL8 chemokine is regulated through two
specific receptors, C-X-C chemokine receptor (CXCR)1 and CXCR2, and
has an important role in the pathological mechanism of ovarian
cancer. Notably, via its autocrine action on cells, CXCL8 can
affect ovarian cancer cell proliferation, invasion and angiogenesis
(18). CXCL8 is a chemokine that
belongs to the CXC family. Its function is to activate neutrophil
granulocytes and recruit granulocytes to sites of inflammation
(19). CXCL8 is secreted by a
large group of cells, including circulating monocytes in the blood,
macrophages present in the alveoli, fibroblasts, endothelial cells
and epithelial cells. CXCL8 synthesis occurs under the influence of
several factors, including: tumor necrosis factor-α, interleukin
(IL)-1, IL-6, and stressors of environmental and chemical origin,
such as hypoxia and reactive oxygen species (20,21).
CXCL8-mediated signaling depends on the
extracellular binding of the chemokine to CXCR1 or CXCR2, which are
both coupled to G protein (20).
In addition, CXCR1 has a high specificity to the chemokine CXCL8
compared with CXCR2, which can bind to other ILs (22). CXCR1 and CXCR2 are found on the
surface of a variety of cells, both normal and cancerous (23). The interaction between CXCL8 and
CXCR1 or CXCR2 has a significant function in the development of the
inflammatory process and thus affects different stages of
carcinogenesis, leading to the promotion, progression and
metastasis of cancer, including ovarian cancer (11–13,24). Notably, the CXCL8-CXCR1/2
signaling axis may serve an important role in tumorigenesis and the
formation of secondary tumor foci by controlling the proliferation
and self-renewal of cancer stem cells (20). Furthermore, the CXCL8-CXCR1
signaling pathway has been reported to primarily enhance cancer
cell proliferation, whereas the CXCL8-CXCR2 pathway can affect
angiogenesis (19).
Disturbances in the immune system serve an important
role in the formation and development of ovarian cancer,
particularly those involving chemokines and their receptors.
Understanding the relationship between the coexistence of
inflammatory and neoplastic processes may help to elucidate the
involvement of the studied parameters in tumor pathogenesis and
could lead to improved clinical applications. Therefore, the aim of
the present study was to analyze the levels of CXCL8, and its
receptors CXCR1 and CXCR2, in the serum and peritoneal fluid of
women with ovarian cancer. In addition, the association between the
expression levels of CXCL8, CXCR1 and CXCR2, and the degree of
histological differentiation, was assessed in ovarian cancer.
Materials and methods
Patients
The present study included 32 patients aged 28–89
years (mean age, 61.3415.55 years), who were hospitalized at the
Gynecology and Obstetrics Department with Pregnancy Pathology and
Gynecology Oncology Subdivisions, Provincial Specialist Hospital
Blessed Virgin Mary (Częstochowa, Poland) and were diagnosed with
ovarian serous cystadenocarcinoma III C according to FIGO. In 12
patients, the neoplasm was of G1 histological differentiation
grade, in 10 patients it was of G2 histological differentiation
grade, and in the remaining 10 patients it was of G3 histological
differentiation grade. Patients and control individuals were
recruited between May 2019 and February 2022.
The clinical staging classification of ovarian
cancer was established based on the FIGO guidelines. The degree of
histological differentiation of cancer was graded according to the
following criteria: G1, highly differentiated; G2, moderately
differentiated; G3, poorly differentiated. The diagnosis was based
on clinical symptoms, results of gynecological and
histopathological examinations, laboratory tests and exclusion of
the coexistence of other diseases of reproductive organs. The women
that qualified to the studied group were clinically diagnosed with
ovarian tumors confirmed with a histopathological examination. None
of the examined women were administered pharmacological treatments
in the previous 3 months.
Serum, peritoneal fluid and tumor tissue were
examined for all of the recruited patients. In the study group,
blood was taken from women after establishing the clinical
diagnosis and before surgery. Blood was taken in the morning from
the cubital vein and was added to tube containing a clot activator,
in order to obtain serum; 30 min after blood collection, it was
centrifuged at 1,500 × g for 15 min at room temperature the serum
was obtained and maintained at −80°C until further use. Tumor
tissue intended for molecular examination was collected during the
planned surgery and frozen at −80°C until analyses were performed.
Peritoneal fluid was collected during laparoscopy for
bacteriological examination, was centrifuged at 1,500 × g for 10
min at 4°C, and the obtained supernatant was partitioned and frozen
at −80°C until the remaining determinations were made.
The control group consisted of 15 women aged between
22 and 77 years (mean age, 52.08±18.00 years) who were diagnosed
with a benign lesion (serous cystadenoma). Serum samples were used
as control.
The present study was conducted according to the
guidelines of the Declaration of Helsinki, and was approved by the
Ethics Committee of Medical University of Silesia in Katowice
(Sosnowiec, Poland; protocol code KNW/0022/KB1/49/19). All patients
agreed to participate in the present study and provided written
informed consent.
ELISA analyses
The concentration of CXCL8 in the serum and
peritoneal fluid was determined by sandwich ELISA using the Human
Interleukin-8 ELISA kit (cat. no. RD194558200R; BioVendor LM),
according to the manufacturer's instructions. The sensitivity of
the assay was 0.5 pg/ml. The concentration of CXCR1 and CXCR2 was
determined by sandwich ELISA using the CLOUD-CLONE ELISA kit (cat.
nos. SEA019Hu and SEC006Hu; Cloud-Clone Corp.), according to the
manufacturer's instructions. The sensitivity of the assay for CXCR1
was 0.054 ng/ml, whereas for CXCR2 it was 0.057 ng/ml.
Reverse transcription-quantitative PCR
(RT-qPCR)
Total RNA was extracted from tissue samples using
TRIzol® reagent (Invitrogen; Thermo Fisher Scientific,
Inc.), according to the manufacturer's instructions. Quantitative
analysis of RNA was performed using a nanospectrophotometer
(MaestroNano MN-913; MaestroGen, Inc.). Qualitative analysis was
performed by electrophoresis on a 1% agarose gel. The mRNA
expression levels of CXCL8, CXCR1 and CXCR2 were
evaluated using RT-qPCR. The quantitative analysis was carried out
using LightCycler® 480 System (Roche Diagnostics) and
GoTaq® 1-Step RT-qPCR System (Promega GmbH), according
to the manufacturers' instructions, under the following conditions:
RT at 37°C for 15 min; RT inactivation/Hot-start activation at 95°C
for 10 min; followed by 40 cycles of denaturation at 95°C for 10
sec, annealing at 60°C for 30 sec, elongation at 72°C for 30 sec.
Amplification was performed using KiCqStart SYBR Green
oligonucleotide primers (Sigma-Aldrich; Merck KGaA), as follows:
CXCL8, forward (F) 5-'TGTAAACATGACTTCCAAGC-3′, reverse (R)
5′-AAAACTGCACCTTCACAC-3′; CXCR1, F
5′-TTAAGTCACTCTGATCTCTGAC-3′, R 5′-TGGTTTGATCTAACTGAAGC-3′;
CXCR2, F 5′GTGATAGCTGAGAATATGCAG-3′, R
5′-ACTTAAATCCTGACTGGGTC-3′; and β-actin, F
5′-GACGACATGGAGAAAATCTG-3′ and R 5′-ATGATCTGGGTCATCTTCTC-3′.
Melting curve analysis and 2% agarose gel electrophoresis were used
to confirm the specificity of amplification and the absence of
primer dimers. RT-qPCR data were analysed by the 2−ΔΔCq
method using β-actin as an internal control (25).
Statistical analysis
The obtained results were statistically analysed
using Statistica 13.3 software (StatSoft Polska Sp. z o.o.). The
normality of the distribution of the studied variables was assessed
using the Shapiro-Wilk test. The significance of differences
between two groups was determined with Mann-Whitney U-test. The
significance of differences between more than two groups was
determined by Kruskal-Wallis test, followed by Dunn's post-hoc
analysis. P<0.05 was considered to indicate a statistically
significant difference. Correlation was assessed using Pearson
correlation for logarithmic data (r).
Results
Concentration of CXCL8, and its
receptors CXCR1 and CXCR2, in serum
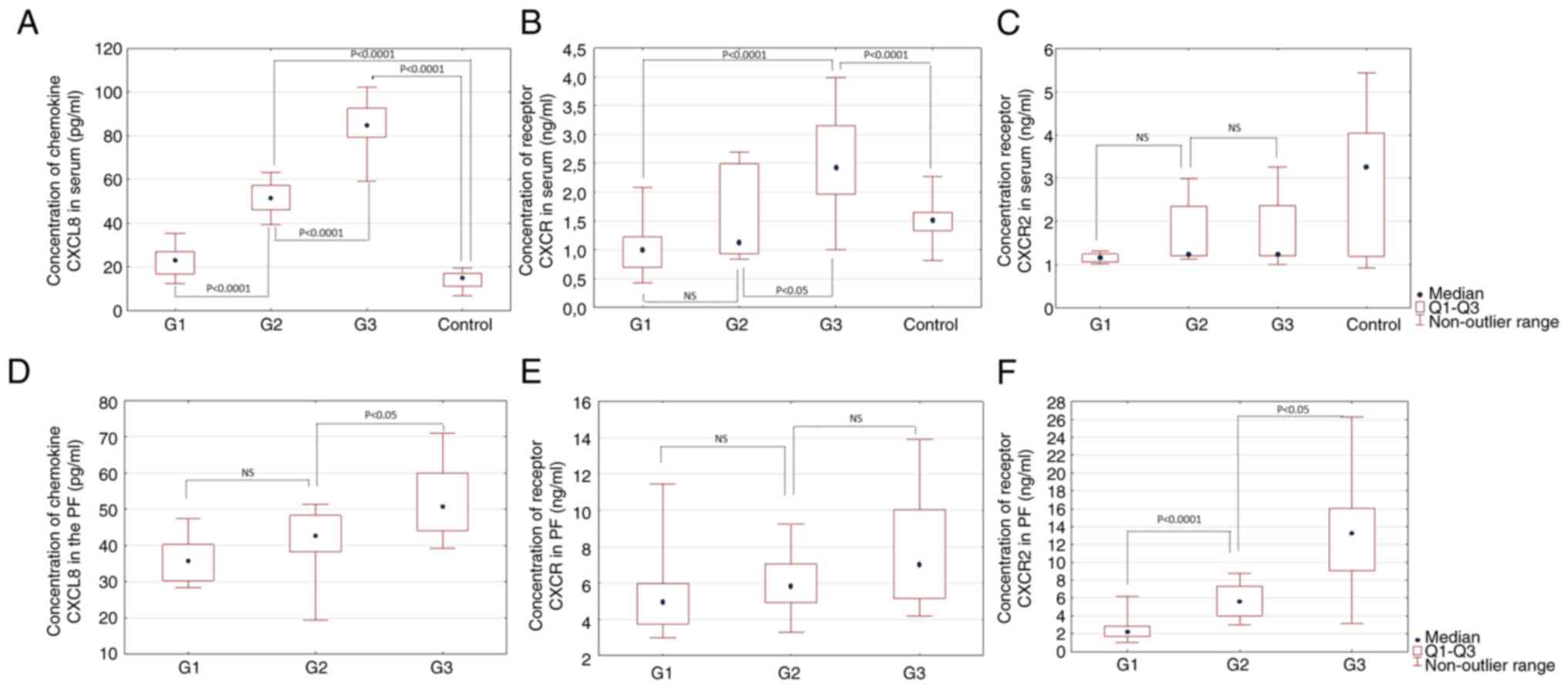
The levels of CXCL8, and its receptors CXCR1 and
CXCR2, in the serum of women with serous ovarian cystadenocarcinoma
were evaluated according to histological differentiation stage. It
was revealed that the concentration of CXCL8 was significantly
increased between G1, G2 and G3 grades (P<0.0001). Analysis of
the concentration of the examined parameter in successive grades of
histological differentiation in comparison with the control group
showed a statistically significant difference only in the G2 and G3
grades (P<0.0001) (Fig. 1A).
Further analysis included evaluation of serum CXCR1 levels
according to histological differentiation stage. There was a
statistically significant difference in these concentrations
between grades G1 and G3 (P<0.001), and between G2 and G3
(P<0.05). Furthermore, when compared with the control group, a
statistically significant difference was shown only in grade G3
(P<0.001) (Fig. 1B). Regarding
serum CXCR2 levels, there were no statistically significant
differences between the different degrees of histological
differentiation, nor between G1-G3 grades and the control group
(Fig. 1C). The obtained results
are also shown in Table I.
 | Table I.Serum concentrations of CXCL8 and its
receptors in women with ovarian cancer and the control group. |
Table I.
Serum concentrations of CXCL8 and its
receptors in women with ovarian cancer and the control group.
| Characteristic | Ovarian cancer
group (n=32) | Control group
(n=15) | P-value |
|---|
| Mean age ± SD,
years | 61.34±15.55 | 52.08±18.00 |
|
| Median serum
CXCL8 | 48.25
(26.26-77.48) | 14.96
(11.03-16.83) | <0.01 |
| concentration
(Q1-Q3), pg/ml |
|
|
|
| Median serum
CXCR1 | 1.19
(0.94-2.26) | 1.51
(1.34-1.65) | NS |
| concentration
(Q1-Q3), ng/ml |
|
|
|
| Median serum
CXCR2 | 1.23
(1.17-1.32) | 3.27
(1.19-4.04) | 0.001 |
| concentration
(Q1-Q3), ng/ml |
|
|
|
Concentration of CXCL8, and its
receptors CXCR1 and CXCR2, in peritoneal fluid
The concentrations of CXCL8, and its receptors CXCR1
and CXCR2, in the peritoneal fluid of women with ovarian cancer
were evaluated according to histological differentiation stage.
CXCL8 levels in the peritoneal fluid were only significantly
different between grades G2 and G3 (P<0.05; Fig. 1D). Notably, there were no
statistically significant differences between the concentration of
CXCR1 in the peritoneal fluid between patients with different
degrees of histological differentiation of ovarian cancer (Fig. 1E). By contrast, analysis of CXCR2
concentration in the peritoneal fluid revealed a statistically
significant difference between G1 and G2 grades (P<0.001), and
between G2 and G3 grades (P<0.05) (Fig. 1F).
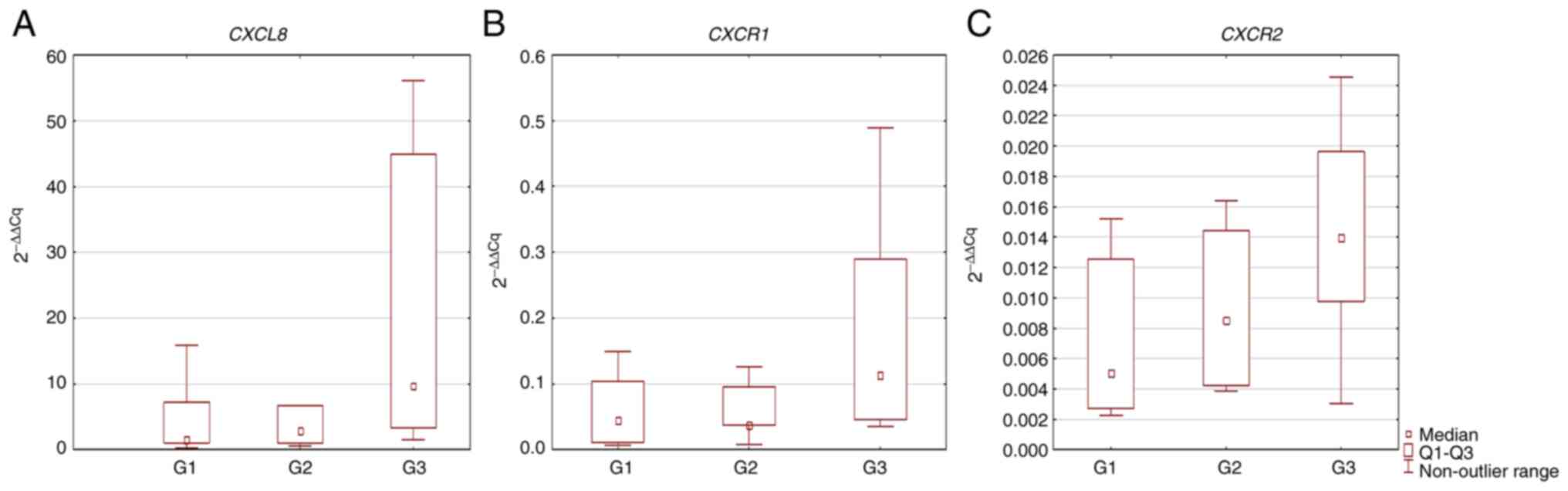
mRNA expression levels of CXCL8, and
its receptors CXCR1 and CXCR2, in tumor tissue
The highest mRNA expression levels of CXCL8,
and its receptors CXCR1 and CXCR2, were detected in
the tumor tissues obtained from patients with G3 grade ovarian
cancer. However, no statistically significant differences were
found (P>0.05; Fig. 2).
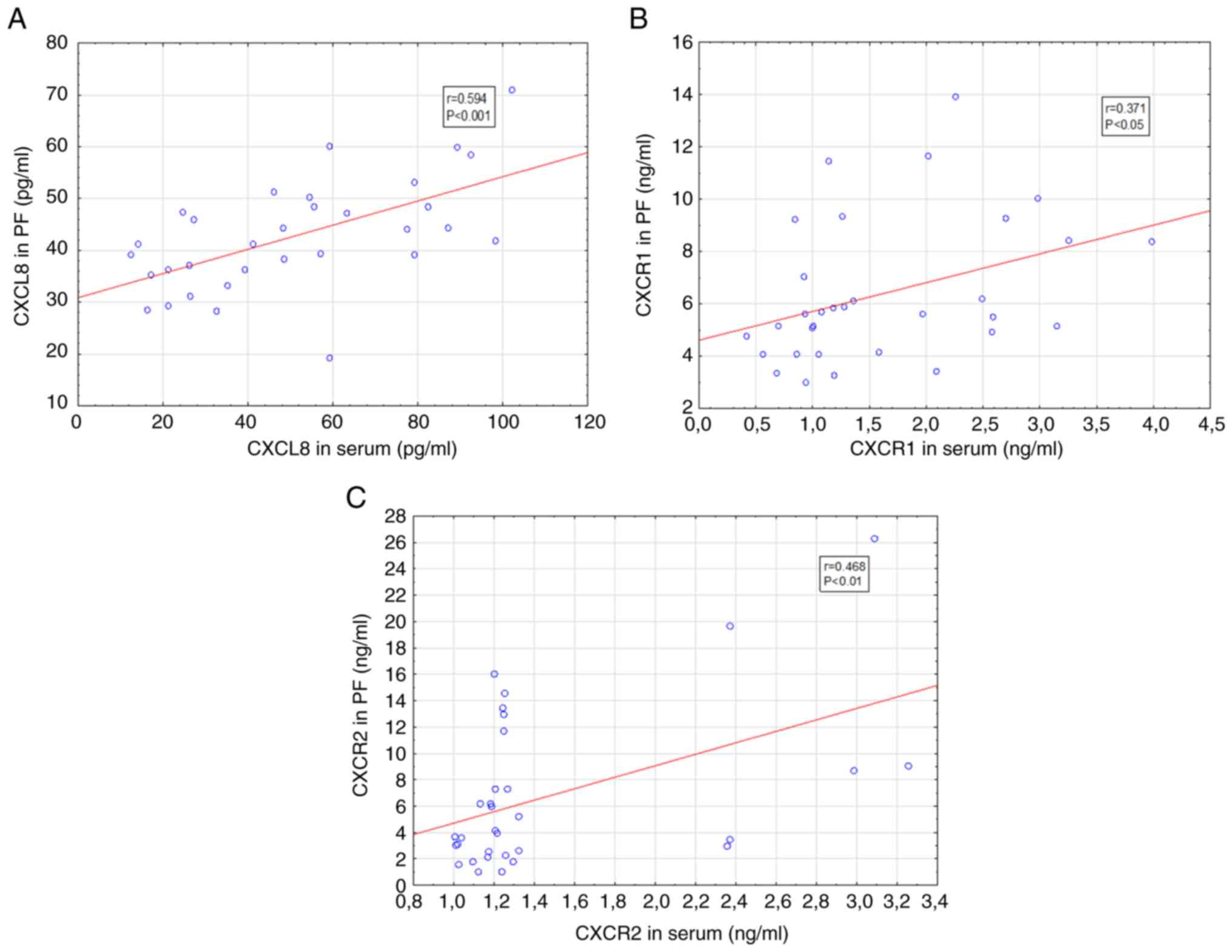
Positive statistically significant correlations were
detected between serum and peritoneal fluid levels of CXCL8, CXCR1
and CXCR2 in women with ovarian cancer (Fig. 3). There were no statistically
significant correlations detected between the serum and tissue
levels, and between the peritoneal fluid and tissue levels, with
regard to CXLC8, CXCR1 and CXCR2 (data not shown).
Discussion
Previous studies have predicted that mortality from
ovarian cancer will continue to increase until 2040 (3,26);
therefore, research into the biology of ovarian cancer continues,
with the aim of understanding the mechanisms involved in its
pathogenesis, which may prove useful in developing new diagnostic
and therapeutic regimens. Previous studies have reported that the
process of ovarian tumorigenesis is accompanied by chronic
inflammation (27,28). In this process, an important role
is attributed to the CXCL8 chemokine system, along with its
receptors CXCR1 and CXCR2, which serve an important role in tumor
formation and development by affecting the different stages of
carcinogenesis, consequently leading to ovarian cancer progression
(10–13).
The aim of the present study was to analyze the
expression of the CXCL8 chemokine, and its receptors
CXCR1 and CXCR2, in tumor tissue, and to evaluate the
levels of these parameters in serum and peritoneal fluid from women
diagnosed with ovarian cancer, taking into account the histological
differentiation of ovarian cancer. The analysis of CXCL8 revealed
that the levels were significantly higher in the serum of patients
diagnosed with ovarian cancer compared with those in the control
group (P<0.01), which may indicate the involvement of the
studied cytokine in the pathogenesis of ovarian cancer. Moreover,
statistical significance was demonstrated between the G1, G2 and G3
grades (P<0.0001). These findings indicated that a relationship
may exist between CXCL8 secretion and the degree of histological
differentiation of ovarian cancer. However, when analyzing CXCL8
concentration in the peritoneal fluid, a statistically significant
difference was only found between differentiation grades G2 and G3
(P<0.05). A similar tendency was observed regarding CXCL8
mRNA expression in tumor tissue, where the highest expression
levels were detected in the G3 grade; however, no statistically
significant differences were noted between the studied groups.
In the pathological mechanism of ovarian cancer
development, an important role has been attributed to the
proinflammatory chemokine CXCL8, which has chemotactic effects on
cells expressing CXCR1 and CXCR2. Moreover, CXCL8 interacting with
the tumor microenvironment can positively influence tumor growth,
stimulate new blood vessel formation and promote the formation of
secondary tumor foci (29).
Browne et al (30)
detected significantly elevated levels of CXCL8 in each
histological subtype of ovarian cancer, and demonstrated the
existence of a relationship between CXCL8 chemokine levels and the
clinical stage of ovarian cancer. Analogous results were obtained
by Crispim et al (31);
significantly elevated serum levels of CXCL8 were detected in women
diagnosed with ovarian malignancy and benign tumors compared with
those detected in a group of women without reproductive system
conditions. In addition, the authors revealed that the prognosis of
patients with ovarian cancer was worse when higher levels of the
chemokine persisted during the course of the disease. Furthermore,
Zhang et al (32) analyzed
chemokine levels in the course of ovarian cancer and observed that
the stage of ovarian cancer was correlated with the levels of
CXCL8. In addition, significantly higher serum levels of CXCL8 were
detected in women with stage III and IV ovarian cancer compared
with those in women with stage I and II ovarian cancer, according
to the FIGO classification.
An important protumor role has been attributed to
tumor-associated cells, mainly fibroblasts, neutrophils and
macrophages, which can contribute to tumor growth and invasiveness,
and can promote the formation of secondary cancer foci by secreting
pro-inflammatory cytokines. Yang et al (33) evaluated the relationship between
IL-8 and neutrophils during cancer development. Their study showed
that the expression of numerous chemokines, particularly IL-8, was
significantly higher in ovarian cancer with stronger neutrophil
infiltration compared with that in ovarian cancer with little
infiltration of these cells. Additionally, the study revealed that
higher levels of IL-8 were correlated with an increase in
tumor-associated neutrophils; therefore, IL-8 may be involved in
attracting neutrophils toward the tumor microenvironment. Thongchot
et al (34) demonstrated
that tumor-associated fibroblasts have an important role in the
pathological mechanism of ovarian cancer by mobilizing ovarian
cancer cells to form metastases. Moreover, these cells could
secrete CXCL8 more intensively compared with physiological
fibroblasts. This previous study also revealed that increased serum
CXCL8 levels were correlated with disease progression and
negatively affected patient prognosis, and increased CXCL8 levels
in the peritoneal fluid were correlated with ovarian cancer
progression. Furthermore, over-secreted CXCL8 has been reported to
act as a chemotactic factor for ovarian cancer cells, facilitating
the formation of metastasis (34). Alfaro et al (35) reported that CXCL8 was also capable
of attracting other cells that express its specific receptors CXCR1
and CXCR2 on their surface. In addition, Ha et al (20), showed that stimulated cells, for
example those stimulated by various cytokines, were able to produce
and secrete CXCL8 10 to 100 times more than under normal
conditions, in which CXCL8 was mostly undetectable.
In the present study, CXCR1 levels were further
evaluated in the serum and peritoneal fluid. The existence of a
statistically significant difference in serum concentrations was
demonstrated between grades G1 and G3 (P<0.001), and between
grades G2 and G3 (P<0.05), which may indicate the involvement of
CXCR1 in autocrine and paracrine signaling associated with CXCL8 in
tumor development. Further tests, including assessment of patients
with different ovarian cancer stages according to the FIGO
classification, may provide more information on the association
between serum concentration of CXCR1 and the condition of the
patient. In addition, the mRNA expression levels of CXCR1 in
the tumor tissue were highest at G3 grade; however, this difference
was not statistically significant.
Browne et al (30) observed a correlation between the
expression levels of IL-8Ra and cancer stage. By analyzing the
levels of IL-8Rb, no significant association was identified in the
levels of this IL-8 receptor between the study group and the
control group. Their study also revealed that there was a
significant association between the levels of IL-8 and IL-8R and
the type of cancer. The concentration of these compounds was
significantly higher in serous carcinoma, as opposed to the other
histological types of ovarian cancer. Furthermore, increased
expression levels of IL-8, IL-8Ra and IL-8Rb were detected in
benign serous ovarian tumors and benign mucinous tumors. Comparing
the levels of IL-8 and its receptors in benign and malignant
ovarian tumors showed significantly decreased levels during benign
tumor development.
The present study also analyzed the levels of CXCR2;
no statistically significant differences were detected in the serum
levels of CXCR2 between the histological grades. Similarly,
differences at mRNA level were also not statistically significant.
However, in the peritoneal fluid, a statistically significant
difference in CXCR2 levels was identified between the G1 and G2
grades (P<0.001), and between the G2 and G3 grades
(P<0.05).
Notably, Henriques et al (36) evaluated the role of CXCR2 in the
pathogenesis of ovarian cancer. The results of this study revealed
that CXCR2 was upregulated in patients diagnosed with ovarian
cancer. Furthermore, CXCL8 and CXCL2 chemokines regulated by CXCR2,
which is located on ovarian cancer cells, showed autocrine
activity. Elevated levels of both chemokines in the course of
ovarian cancer have been associated with the occurrence of tumor
progression, formation of secondary cancer foci and chemoresistance
to the applied treatment (13,37,38). In addition, Taki et al
(39) indicated a significant
role of CXCR2 in ovarian cancer progression, as determined using
mouse models. The authors demonstrated that CXCR2 not only affected
CXCL8, but also interacted with CXCL1 and CXCL2, resulting in the
observed chemotaxis of myeloid-derived suppressor cells. These
cells in turn may promote tumor metastasis by inducing
epithelial-mesenchymal transition, consequently leading to disease
progression.
The role of CXCL8-CXCR1 and CXCL8-CXCR2 signaling
axes is one of several mechanisms involved in the regulation of the
immune system during the antitumor response (40). According to Liu et al
(19), this pathway may have an
important role not only in the pathogenesis of ovarian cancer, but
also in the formation of numerous other types of cancer, including
breast, prostate, lung, colorectal and gastric cancer, and
melanoma. Researchers have suggested that in breast cancer, CXCL8
can directly affect tumor formation; CXCL8 synthesized by cancer
cells may initiate the process of neovascularization by stimulating
vascular endothelial growth factor. The newly formed blood vessels
can thus initiate the process of breast cancer development, and may
also supply nutrients to distant metastases (19). Liubomirski et al (41) evaluated the role of the
inflammatory process and the involvement of inflammatory mediators,
including the chemokine CXCL8, in the pathological mechanism of
breast cancer development. This previous study showed that CXCL8
directly interacted with cancer cells in triple-negative breast
cancer (TNBC), resulting in increased invasiveness and
aggressiveness. Using a mouse model of TNBC, it was demonstrated
that CXCL8 regulated by CXCR2, and C-C motif chemokine ligand 2
regulated by receptor for chemokine CCL2, interacted with
tumor-associated neutrophils and macrophages, affecting their
migration to the tumor site where they promoted disease course.
In conclusion, local and systemic disturbances of
immune and inflammatory responses involving the CXCL8 chemokine and
its receptors indicate the involvement of these studied parameters
in the pathogenesis of ovarian cancer. Moreover, immunoregulation
of the CXCL8-CXCR1 system may influence the course of the
inflammatory process accompanying ovarian cancer development and
may have a clinical application; however, further studies are
required.
Acknowledgements
Not applicable.
Funding
This research was funded by the Medical University of Silesia in
Katowice, Poland (grant no. PCN-1-069/K/1/O).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AMP was involved in conceptualization, supervision
of immunology research, investigation and writing (original draft
preparation, review and editing). JMG was involved in
conceptualization, supervision of molecular research,
investigation, and writing, reviewing and editing. MSK and SS
designed and performed immunological research. CKR designed and
performed molecular research. MSK, SS, CKR, DW, PKD and AS
performed the experiments, and participated in data analysis and
interpretation. JS, WS and AW were involved in clinical research
conceptualization and data interpretation. AMP and JMG confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was conducted according to the guidelines
of the Declaration of Helsinki, and was approved by the Ethics
Committee of Medical University of Silesia in Katowice, Poland
(protocol code KNW/0022/KB1/49/19). All patients agreed to
participate in the presnt study and provided written informed
consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jin Y, Lin Q, Fei H, Xue L, Li L, Xi Q and
Jiang H: Bioinformatics analysis of potential therapeutic targets
and prognostic biomarkers amid CXC chemokines in ovarian carcinoma
microenvironment. J Oncol. 2021:88595542021. View Article : Google Scholar
|
|
2
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global Cancer Statistics 2020:
GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36
Cancers in 185 Countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Keyvani V, Farshchian M, Esmaeili SA, Yari
H, Moghbeli M, Nezhad SK and Abbaszadegan MR: Ovarian cancer stem
cells and targeted therapy. J Ovarian Res. 12:1202019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yang C, Xia BR, Zhang ZC, Zhang YJ, Lou G
and Jin WL: Immunotherapy for ovarian cancer: Adjuvant,
combination, and neoadjuvant. Front Immunol. 11:5778692020.
View Article : Google Scholar
|
|
5
|
Gaona-Luviano P, Medina-Gaona LA and
Magaña-Pérez K: Epidemiology of ovarian cancer. Chin Clin Oncol.
9:472020. View Article : Google Scholar
|
|
6
|
Cortez AJ, Tudrej P, Kujawa KA and
Lisowska KM: Advances in ovarian cancer therapy. Cancer Chemother
Pharmacol. 81:17–38. 2018. View Article : Google Scholar
|
|
7
|
Bogani G, Lopez S, Mantiero M, Ducceschi
M, Bosio S, Ruisi S, Sarpietro G, Guerrisi R, Brusadelli C,
Dell'Acqua A, et al: Immunotherapy for platinum-resistant ovarian
cancer. Gynecol Oncol. 158:484–488. 2020. View Article : Google Scholar
|
|
8
|
Arora T, Mullangi S and Lekkala MR:
Ovarian cancer. StatPearls [Internet]. StatPearls Publishing;
Treasure Island, FL: 2022
|
|
9
|
Zhang M, Cheng S, Jin Y, Zhao Y and Wang
Y: Roles of CA125 in diagnosis, prediction, and oncogenesis of
ovarian cancer. Biochim Biophys Acta Rev Cancer. 1875:1885032021.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Atallah GA, Abd Aziz NH, Teik CK, Shafiee
MN and Kampan NC: New predictive biomarkers for ovarian cancer.
Diagnostics (Basel). 11:4652021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gonzalez-Aparicio M and Alfaro C:
Significance of the IL-8 pathway for immunotherapy. Hum Vaccin
Immunother. 16:2312–2317. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Marchewka Z, Gielniak M and Piwowar A: The
role of selected mediators of inflammation in the pathogenesis of
cancer. Postepy Hig Med Dosw. 72:175–183. 2018. View Article : Google Scholar
|
|
13
|
Łukaszewicz-Zając M, Pączek S, Mroczko P
and Kulczyńska-Przybik A: The significance of CXCL1 and CXCL8 as
Well as their specific receptors in colorectal cancer. Cancer Manag
Res. 12:8435–8443. 2020. View Article : Google Scholar
|
|
14
|
Turnquist C, Ryan BM, Horikawa I, Harris
BT and Harris CC: Storms in cancer and COVID-19. Cancer Cell.
38:598–601. 2020. View Article : Google Scholar
|
|
15
|
Kumar S, O'Malley J, Chaudhary AK, Inigo
JR, Yadav N, Kumar R and Chandra D: Hsp60 and IL-8 axis promotes
apoptosis resistance in cancer. Br J Cancer. 121:934–943. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Friedman A and Liao KL: The role of the
cytokines IL-27 and IL-35 in cancer. Math Biosci Eng. 12:1203–1217.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Groblewska M, Litman-Zawadzka A and
Mroczko B: The role of selected chemokines and their receptors in
the development of gliomas. Int J Mol Sci. 21:37042020. View Article : Google Scholar
|
|
18
|
Lane D, Matte I, Rancourt C and Piché A:
Prognostic significance of IL-6 and IL-8 ascites levels in ovarian
cancer patients. BMC Cancer. 11:2102011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Liu Q, Li A, Tian Y, Wu JD, Liu Y, Li T,
Chen Y, Han X and Wu K: The CXCL8-CXCR1/2 pathways in cancer.
Cytokine Growth Factor Rev. 31:61–71. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ha H, Debnath B and Neamati N: Role of the
CXCL8-CXCR1/2 axis in cancer and inflammatory diseases.
Theranostics. 7:1543–1588. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Waugh DJ and Wilson C: The interleukin-8
pathway in cancer. Clin Cancer Res. 14:6735–6741. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Antonosante A, Brandolini L, d'Angelo M,
Benedetti E, Castelli V, Maestro MD, Luzzi S, Giordano A, Cimini A
and Allegretti M: Autocrine CXCL8-dependent invasiveness triggers
modulation of actin cytoskeletal network and cell dynamics. Aging
(Albany NY). 12:1928–1951. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gales D, Clark C, Manne U and Samuel T:
The chemokine CXCL8 in carcinogenesis and drug response. ISRN
Oncol. 2013:8591542013.
|
|
24
|
Nolen BM and Lokshin AE: Biomarker testing
for ovarian cancer: Clinical utility of multiplex assays. Mol Diagn
Ther. 17:139–146. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Schmittgen TD and Livak KJ: Analyzing
real-time PCR data by the comparative C(T) method. Nat Protoc.
3:1101–1108. 2008. View Article : Google Scholar
|
|
26
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jia D, Nagaoka Y, Katsumata M and Orsulic
S: Inflammation is a key contributor to ovarian cancer cell
seeding. Sci Rep. 8:123942018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Savant SS, Sriramkumar S and O'Hagan HM:
The role of inflammation and inflammatory mediators in the
development, progression, metastasis, and chemoresistance of
epithelial ovarian cancer. Cancers (Basel). 10:2512018. View Article : Google Scholar
|
|
29
|
Wen J, Zhao Z, Huang L, Wang L, Miao Y and
Wu J: IL-8 promotes cell migration through regulating EMT by
activating the Wnt/β-catenin pathway in ovarian cancer. J Cell Mol
Med. 24:1588–1598. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Browne A, Sriraksa R, Guney T, Ramac N,
Van Noordena S, Curryc E, Gabrac H, Stronachc E and El-Bahrawy M:
Differential expression of IL-8 and IL-8 receptors in benign,
borderline and malignant ovarian epithelial tumours. Cytokine.
64:413–421. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Crispim PCA, Jammal MP, Antão PKA, Micheli
DC, Tavares-Murta BM, Murta EFC and Nomelini RS: IL6, IL8, and IL10
in the distinction of malignant ovarian neoplasms and
endometriomas. Am J Reprod Immunol. 84:e133092020. View Article : Google Scholar
|
|
32
|
Zhang L, Liu W, Wang X, Wang X and Sun H:
Prognostic value of serum IL-8 and IL-10 in patients with ovarian
cancer undergoing chemotherapy. Oncol Lett. 17:2365–2369. 2019.
|
|
33
|
Yang M, Zhang G, Wang Y, He M, Xu Q, Lu J,
Liu H and Xu C: Tumour-associated neutrophils orchestrate
intratumoural IL-8-driven immune evasion through Jagged2 activation
in ovarian cancer. Br J Cancer. 123:1404–1416. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Thongchot S, Jamjuntra P, Therasakvichya
S, Warnnissorn M, Ferraresi A, Thuwajit P, Isidoro C and Thuwajit
C: Interleukin-8 released by cancer-associated fibroblasts
attenuates the autophagy and promotes the migration of ovarian
cancer cells. Int J Oncol. 58:142021. View Article : Google Scholar
|
|
35
|
Alfaro C, Teijeira A, Oñate C, Pérez G,
Sanmamed MF, Andueza MP, Alignani D, Labiano S, Azpilikueta A,
Rodriguez-Paulete A, et al: Tumor-produced interleukin-8 attracts
human myeloid-derived suppressor cells and elicits extrusion of
neutrophil extracellular traps (NETs). Clin Cancer Res.
22:3924–3936. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Henriques TB, Dos Santos DZ, Dos Santos
Guimarães I, Tessarollo NG, Lyra-Junior PCM, Mesquita P, Pádua D,
Amaral AL, Cavadas B, Pereira L, et al: Inhibition of CXCR2 plays a
pivotal role in re-sensitizing ovarian cancer to cisplatin
treatment. Aging (Albany NY). 13:13405–13420. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Duckworth C, Zhang L, Carroll SL, Ethier
SP and Cheung HW: Overexpression of GAB2 in ovarian cancer cells
promotes tumor growth and angiogenesis by upregulating chemokine
expression. Oncogene. 35:4036–4047. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Stronach EA, Cunnea P, Turner C, Guney T,
Aiyappa R, Jeyapalan S, de Sousa CH, Browne A, Magdy N, Studd JB,
et al: The role of interleukin-8 (IL-8) and IL-8 receptors in
platinum response in high grade serous ovarian carcinoma.
Oncotarget. 6:31593–31603. 2015. View Article : Google Scholar
|
|
39
|
Taki M, Abiko K, Baba T, Hamanishi J,
Yamaguchi K, Murakami R, Yamanoi K, Horikawa N, Hosoe Y, Nakamura
E, et al: Snail promotes ovarian cancer progression by recruiting
myeloid-derived suppressor cells via CXCR2 ligand upregulation. Nat
Commun. 9:16852018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Han ZJ, Li YB, Yang LX, Cheng HJ, Liu X
and Chen H: Roles of the CXCL8-CXCR1/2 axis in the tumor
microenvironment and immunotherapy. Molecules. 27:1372021.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Liubomirski Y, Lerrer S, Meshel T,
Rubinstein-Achiasaf L, Morein D, Wiemann S, Körner C and Ben-Baruch
A: Tumor-stroma-inflammation networks promote pro-metastatic
chemokines and aggressiveness characteristics in triple-negative
breast cancer. Front Immunol. 10:7572019. View Article : Google Scholar
|