Introduction
Lung cancer (LC) is the most prevalent malignancy
worldwide, affecting individuals of all sexes, with ~2.5 million
new cases diagnosed in 2022. It remains the leading cause of
cancer-related mortality, accounting for >1.8 million deaths
globally in the same year (1).
Despite notable advances in treatment, the overall 5-year survival
rate remains poor, not exceeding 17% (2). LC is broadly classified into
non-small cell LC (NSCLC), which represents ~80% of cases and
small-cell LC, which accounts for the remaining 20%. According to
the 2015 World Health Organization classification (3), NSCLC is further subdivided into three
major histological subtypes: Lung adenocarcinoma (LUAD), lung
squamous cell carcinoma (LSCC) and large cell carcinoma (3).
The pathogenesis of LC is complex, involving both
genetic susceptibility and environmental exposure. In addition, its
development is driven by dysregulated oncogenes and tumor
suppressor genes (4), contributing
to the highly aggressive nature of lung tumors and the frequent
occurrence of metastases at diagnosis (5).
Management of LC typically involves a multimodal
approach that includes surgery, radiotherapy (RT), chemotherapy and
immunotherapy. RT, used either as a stand-alone modality or in
combination with systemic therapies, is a cornerstone of LC
treatment (6). Of patients with
LC, ~77% are estimated to have a clinically justified indication
for RT during their disease course (7). However, the lung is one of the most
radiosensitive organs, rendering it highly susceptible to
radiation-induced toxicity (8).
Advances in imaging, dose delivery and treatment planning have
enabled more precise targeting of tumor tissue, reducing exposure
of surrounding healthy tissue and broadening therapeutic
possibilities. This evolution toward adaptive RT allows for the
delivery of higher doses while minimizing side effects (9).
Despite these technological improvements,
radioresistance remains a major obstacle in LC management (10). Clinical outcomes are often
unsatisfactory due to intrinsic or acquired resistance, leading to
local recurrence and metastasis (11). Radioresistance is particularly
problematic in NSCLC, where only a subset of patients achieve a
durable response to RT (12).
Furthermore, radioresistant tumor cells actively promote metastasis
and recurrence following treatment (13).
The biological basis of radioresistance is
multifaceted, involving aberrant DNA damage response, dysregulated
cell-cycle checkpoints, impaired apoptosis, altered autophagy,
genetic mutations and disrupted signaling pathways (14). Resistance can be classified as
intrinsic, where tumors are refractory to initial therapy, or
acquired, developing after repeated radiation fractions during
treatment (15).
Genomic and molecular biomarker research offers the
potential to guide RT decisions and identify radiosensitization
strategies (16). Biomarkers such
as genetic polymorphisms, gene expression signatures and protein
expression profiles can provide crucial insights into tumor biology
and predict differential responses to RT (17). In radiation oncology, these
biomarkers enable stratification of patients, inform treatment
intensity and help spare patients unnecessary toxicity, thereby
improving outcomes and quality of life (18–20).
The present review summarized key molecular
biomarkers with potential clinical utility in radiation oncology,
emphasizing their role in optimizing LC management and enabling
precision medicine approaches.
Predictive biomarkers in radiation-based
personalized medicine for LC
Advances in molecular technologies have transformed
cancer management, including in LC, by enabling faster and more
precise diagnostic and therapeutic interventions. Genomic
sequencing, whether whole-genome, whole-exome or targeted, has been
instrumental in advancing precision medicine (21).
According to the U.S. National Institutes of Health,
precision medicine is defined as an approach to disease prevention
and treatment that accounts for interindividual variability in
genes, environment and lifestyle (22). In the context of radiation
oncology, the identification of genetic signatures that predict
prognosis and/or response to RT offers substantial clinical value.
Such biomarkers could inform the personalization of fractionation
schedules, optimization of radiation doses and integration, or
deliberate avoidance, of systemic therapies. Together, these
strategies hold the potential to enhance therapeutic efficacy while
mitigating the toxicities associated with conventional anticancer
regimens (23).
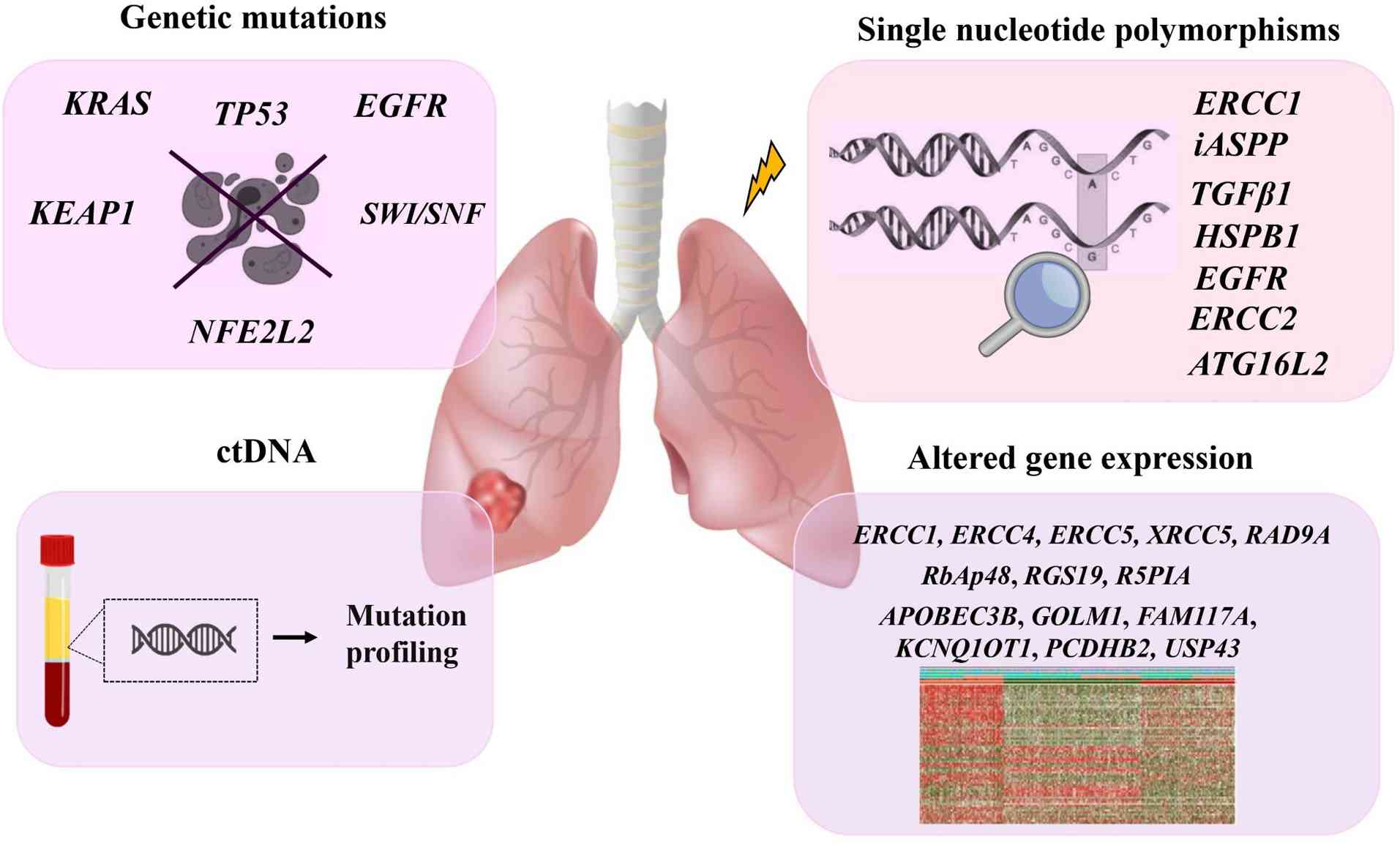
Genetic biomarkers
Individual variability in RT outcomes is largely
attributable to the intrinsic genetic landscape of the tumor
(Fig. 1). Compelling evidence has
indicated that multiple DNA repair genes modulate the cellular
response to RT (24), consistent
with the fact that the primary cytotoxic effect of ionizing
radiation is the induction of DNA double-strand breaks (25). Genetic variations in
radiosensitivity-associated genes contribute to molecular
heterogeneity at specific genomic loci, ultimately influencing key
cellular processes, including the extent of DNA damage sustained
and the efficiency of DNA repair pathways (26).
Mutations associated with radiation
resistance
In NSCLC, KRAS mutations have been strongly
linked to radioresistance (27).
Accumulating evidence has indicated that KRAS-mutant NSCLC
constitutes a heterogeneous group characterized by diverse,
tumor-specific mechanisms of resistance (28,29).
Consistent with this complexity, a study using heterotopic NSCLC
xenograft models has shown that co-mutation of KRAS and
TP53 is associated with reduced local tumor control
following standard RT regimens. This co-mutation may therefore
serve as a predictive biomarker for patient stratification,
informing dose escalation strategies or the addition of molecular
agents targeting the EGFR signaling pathway. More broadly, these
findings underscore the need for biomarker-driven clinical trials
that integrate comprehensive genomic profiling with clinically
relevant endpoints to refine and personalize RT strategies
(30).
The predictive value of EGFR mutations remains
controversial. In patients with EGFR-mutant stage III
adenocarcinoma, concurrent chemoradiation improved local control
but was paradoxically associated with shorter progression-free
survival (PFS) compared with EGFR wild-type patients,
primarily due to relapse or distant metastasis (31). Conversely, another study reported
improved local control following chemoradiation in patients with
EGFR-mutant, locally advanced nonsquamous NSCLC (32). These discordant results may reflect
differences in patient demographics, smoking status (which
influences tumor biology), RT dose and fractionation schemes,
sequencing or concurrency of chemotherapy, or the criteria used to
define treatment response and failure. Such variability highlights
the need for standardized methodologies and better stratified
studies to clarify the true predictive value of EGFR
mutations in RT outcomes.
Parallel clinical trials have explored combining
targeted therapies with RT to improve outcomes in
EGFR-mutant NSCLC. Notably, the phase II trial NCT03667820
evaluated osimertinib with consolidative RT for residual lesions in
advanced EGFR-mutant NSCLC. Among the 42 patients enrolled,
76% of whom received stereotactic RT, the combination yielded a PFS
of 32.3 months and an OS of 45 months, with a favorable safety
profile. These results suggest that integrating third-generation
tyrosine kinase inhibitors with local RT may prolong disease
control, offering a viable alternative to more intensive first-line
regimens for this patient subgroup (33). Collectively, these data illustrate
how EGFR mutations serve not only as potential predictors of
radioresistance but also as guides for incorporating targeted
therapies into combined-modality treatment strategies.
Additional mutations have also been implicated in
radioresistance. Binkley et al (34) demonstrated that mutations in
Kelch-like ECH-associated protein 1 (KEAP1) and nuclear
factor erythroid 2-related factor 2 (NFE2L2) are predictive
of radioresistance and are associated with high rates of local
recurrence in localized NSCLC. Notably, this resistance could be
mitigated with CB-839, a small-molecule glutaminase inhibitor that
potentiates radiation-induced DNA damage by reducing the
free-radical scavenging capacity of cancer cells. Furthermore,
sequencing of peripheral blood samples has revealed that mutations
in the SWI/SNF chromatin-remodeling complex may serve as
stratification biomarkers, as they are enriched in RT-sensitive
patient cohorts (35). Table I provides an overview of the key
mutations associated with differential radiosensitivity in lung
cancer.
 | Table I.Effect of genetic mutations on
outcomes of lung cancer radiotherapy. |
Table I.
Effect of genetic mutations on
outcomes of lung cancer radiotherapy.
| First author/s,
year | Marker | Material | Cohort (size) | Result | Conclusion | (Refs.) |
|---|
| Gurtner et
al, 2020 |
KRAS/TP53 | Tissue | NA | Higher
radioresistance | Radioresistant | (30) |
| Tanaka et
al, 2015 | EGFR | Blood | Unresectable stage
III adenocarcinoma (n=104) | Poor PFS,
metastasis relapse | Radioresistant | (31) |
| Lim et al,
2017 | EGFR | Tissue | Stage III
nonsquamous NSCLC (n=102) | Higher local
control, and a longer duration before progression within the
irradiated field | Radiosensitive | (32) |
| Gurtner et
al, 2020 |
KRAS/TP53 | Tissue | NA | Higher
radioresistance | Radioresistant | (30) |
| Binkley et
al, 2020 |
KEAP1/NFE2L2 | Tissue | Localized NSCLC
(n=232) | High of rates of
local recurrence | Radioresistant | (34) |
| Zhang et al,
2024 | SWI/SNF | Blood | NSCLC (n=13) | Improved RT
response | Radiosensitive | (35) |
Single nucleotide polymorphisms
(SNPs)
SNPs have been extensively investigated for their
potential role in modulating radiosensitivity (Table II). Variants in excision repair
cross-complementation (ERCC)1 and inhibitor of
apoptosis-stimulating protein of p53 (iASPP), both key
mediators of DNA repair, have been associated with differential
responses to chemotherapy and combined chemoradiation in patients
with NSCLC (36). Certain
iASPP polymorphisms may result in decreased protein levels,
leading to activation of ASPP1 and ASPP2 and enhanced p53-mediated
apoptosis, thereby sensitizing tumors to RT (37). A combined SNP signature involving
ERCC2 rs238406 and ERCC1 rs11615 has also been
notably associated with radiosensitivity in LC (38), consistent with the pivotal role of
these genes in the nucleotide excision repair pathway (39).
| Table II.SNPs associated with radiotherapy
outcomes in lung cancer. |
Table II.
SNPs associated with radiotherapy
outcomes in lung cancer.
| First author/s,
year | Marker | dbSNP ID | Cohort (size) | Clinical
relevance | Pathway | Result | (Refs.) |
|---|
| Su et al,
2007 | ERCC1 | rs11615 | Advanced NSCLC
(stages IIIA-IV) (n=154) | Improved RT
response | DNA repair |
Radio-sensitizing | (36) |
| Su et al,
2007 | iASPP | rs3136820 | Advanced NSCLC
(stages IIIA-IV) (n=154) | Improved RT
response | DNA repair |
Radio-sensitizing | (36) |
| Kelsey et
al, 2012 | TGFβ1 | rs1800469 | Lung cancer
(n=39) | Higher radiation
sensitivity | DNA repair |
Radio-sensitizing | (41) |
| Xu et al,
2012 | HSPB1 | rs2868371 | NSCLC (n=224) | Poor OS | Cellular stress
response | Radioresistant | (42) |
| Jin et al,
2015 | ERCC1 | rs11615 | All stage-III NSCLC
(n=92) | Improved RT
response | DNA repair |
Radio-sensitizing | (38) |
| Jin et al,
2015 | ERCC2 | rs238406 | All stage-III NSCLC
(n=92) | Improved RT
response | DNA repair |
Radio-sensitizing | (38) |
| Wen et al,
2018 | ATG16L2 | rs10898880 CC | NSCLC (n=393) | Improved local
recurrence-free survival, PFS and OS | Autophagy |
Radio-sensitizing | (46) |
| Yang and Liu,
2020 | XRCC1 | rs25487 | NSCLC (n=486) | Improved efficacy
and toxicity of RT | DNA repair |
Radio-sensitizing | (40) |
| Yang and Liu,
2020 | XRCC2 | rs3218556 | NSCLC (n=486) | Improved efficacy
and toxicity of RT | DNA repair |
Radio-sensitizing | (40) |
| Yang and Liu,
2020 | XPD | rs13181 | NSCLC (n=486) | Improved efficacy
and toxicity of RT | DNA repair |
Radio-sensitizing | (40) |
| Butkiewicz et
al, 2021 | EGFR | rs712830 CC;
rs2227983 GG; rs712829 TT | Unresectable NSCLC
(n=436) | Worse OS; risk
factor for locoregional recurrence | Receptor tyrosine
kinase signaling | Radioresistant | (44) |
Additional polymorphisms in DNA repair genes,
including X-ray repair cross-complementing protein XRCC1
(rs25487), XRCC2 (rs3218556) and XPD (rs13181), have
been linked to RT response and OS in NSCLC. Notably, the
XRCC1 rs25487 CC genotype and XRCC2 rs3218556 AG/AA
genotypes were more frequently observed among responders than
non-responders (40). These
findings highlight the potential utility of these SNPs as
predictive biomarkers for stratifying patients probably to benefit
from RT.
Polymorphisms in the promoter region of TGFβ1
have also been associated with increased radiosensitivity (41), suggesting their clinical potential
as predictive markers for favorable RT response. Similarly, heat
shock protein β-1 rs2868371 polymorphisms have been shown to
influence treatment outcomes: In U.S. patients with NSCLC, the CC
genotype was associated with poor OS following RT or chemotherapy
(42), whereas in a Chinese
cohort, the C allele was linked to increased radiosensitivity and
improved survival, probably due to reduced Hsp27 expression and
impaired DNA repair capacity (43). These discrepancies underscore the
influence of genetic background, ethnic differences in allele
frequencies and clinical heterogeneity (such as treatment regimens
and disease stage) on study outcomes (42).
Butkiewicz et al (44) reported that EGFR
polymorphisms associated with increased gene expression and
aberrant protein activity may predict clinical outcomes following
DNA-damaging treatments. Specifically, EGFR rs2227983 GG and
rs712829 TT genotypes were associated with tumor recurrence and
acted as independent predictors of poor prognosis, while rs712830
CC genotype was associated with increased mortality risk. Given the
established link between EGFR upregulation, reduced RT
response and shortened survival (45), these findings support the utility
of EGFR genotyping as both a prognostic tool and a predictor
of radioresistance. Incorporating EGFR polymorphism
screening into clinical practice could refine risk stratification
and guide therapeutic decision-making.
Moreover, SNPs in autophagy-related genes have
emerged as promising predictive biomarkers. For example, the
autophagy related 16 like 2 gene rs10898880 CC homozygous variant
has been reported to be associated with improved local
recurrence-free survival, PFS and OS (46).
Despite these advances, most studies have examined
individual SNPs in isolation. RT response is a multifactorial
phenotype shaped by the interplay of multiple genetic variants and
environmental exposures. Interactions between genes regulating DNA
repair, apoptosis and cell-cycle checkpoints can synergistically
influence radiosensitivity, as can gene-environment interactions
such as smoking status, comorbidities and baseline clinical
characteristics. The lack of integrative, systems-level analyses
remains a key limitation in the field. Well-designed studies
incorporating polygenic risk models and environmental data are
needed to improve prediction accuracy and enable clinically
actionable stratification. Furthermore, the underlying mechanisms
by which these SNPs influence RT outcomes remain incompletely
characterized, limiting their current utility as robust predictive
biomarkers. Reliance solely on previously reported functional
variants also risks overlooking rare but clinically meaningful SNPs
that could inform precision RT strategies.
Altered gene expression
Several approaches have been developed to identify
differential gene expression patterns between radiosensitive and
radioresistant samples. One widely cited method is the
radiosensitivity index, proposed by Torres-Roca et al
(47), which quantifies intrinsic
tumor radiosensitivity by measuring the surviving fraction at 2 Gy.
Through gene expression profiling, three genes, RbAp48,
RGS19 and R5PIA, were identified the expression levels
of which were reported to be associated with radiosensitivity,
suggesting their potential as predictive biomarkers for patient
selection prior to RT (47).
Table III summarizes
representative studies identifying gene expression signatures that
influence radiotherapy response in lung cancer.
| Table III.Gene expression signatures associated
with radiotherapy response in lung cancer. |
Table III.
Gene expression signatures associated
with radiotherapy response in lung cancer.
| First author/s,
year | Gene expression
signature | Method of
detection | Regulation | Result | (Refs.) |
|---|
| Torres-Roca et
al, 2005 | RbAp48,
RGS19 and R5PIA | Microarrays,
quantitative PCR | Upregulation | Improved RT
response | (47) |
| Guo et al,
2005 | ERCC1, ERCC4,
ERCC5, XRCC5, RAD9A, DNA-PK, MDM2, PIM2, BCL2 and PKCZ | Microarray
analysis | Upregulation | Lower RT
efficacy | (54) |
| Zhao et al,
2020 | LYNX1, SYNPO,
GADD45B and PDLIM1 | Multiple factor Cox
regression model | Upregulation | Tumor resistance
and repopulation following RT | (52) |
| Ma et al,
2021 | FOLR3, SLC6A11,
ALPP, IGFN1, KCNJ12, RPS4XP22, HIST1H2BH and
BLACAT1 | WGCNA, LASSO Cox
regression analysis | NR | Prediction of
prognosis | (51) |
| Peinado-Serrano
et al, 2022 | APOBEC3B, GOLM1,
FAM117A, KCNQ1OT1, PCDHB2 and USP43 | cDNA
microarrays | Upregulation | Prediction of OS
and PFS | (48) |
| Gao et al,
2022 | SHC1, AURKA
and NAPSA | WGCNA, Cox
regression analysis, RT-qPCR | SHC1/AURKA:
Upregulated; NAPSA: Downregulated | Enhanced
radioresistance | (53) |
| Pustovalova et
al, 2023 | ATRNL1, CA2,
CNR1, FAM189A1, GFRA1, RASGRP1 and RGL3 | RNA sequencing | Upregulation | Lower RT
efficacy | (50) |
| Pustovalova et
al, 2023 | ADGRF1, EPHA7,
LOX, LY6G5C, NSUN7, SLC22A31, SNAI2, TNFRSF11B and
ZNF233 | RNA sequencing | Downregulation | Lower RT
efficacy | (50) |
| Pustovalova et
al, 2023 | CXCL8, IL6
and TGFB2 | RNA sequencing | Upregulation | Lower RT
efficacy | (50) |
| Pustovalova et
al, 2023 | NRG1 | RNA sequencing | Downregulation | Lower RT
efficacy | (50) |
| Xu et al,
2024 | KRT6A | GEO2R analysis,
Kaplan-Meier survival analysis, qPCR, CCK-8 and cell migration
assays | Upregulation | Improved OS | (56) |
| Chen et al,
2025 | APOBEC3B, DOCK4,
IER5L, LBH, LY6K, RERG, RMDN2 and TSPAN2 | WGCNA + DEGs LASSO
regression, Random survival forest and multivariate Cox
regression | Dysregulation | Prediction of
prognosis | (49) |
| Chen et al,
2025 | LBH | In vitro
validation | Upregulation | Increased
radiosensitivity | (49) |
| Li et al,
2025 | ADAMTS3,
FADS2 and RTBDN | RNA sequencing,
DEGs analysis | Dysregulation | Prediction of RT
outcome | (55) |
| Li et al,
2025 | FADS2 | RNA sequencing,
DEGs analysis + in vitro validation | Upregulation | Higher
radioresistance | (55) |
Building on these efforts, Peinado-Serrano et
al (48) used data from The
Cancer Genome Atlas LC cohort to establish a six-gene predictive
signature (APOBEC3B, GOLM1, FAM117A, KCNQ1OT1, PCDHB2 and
USP43) associated with OS and PFS. This gene panel displayed
differential expression according to irradiation phenotype in both
NSCLC cell lines and patients with stage I–III NSCLC treated with
RT, supporting its utility for patient stratification and
prediction of long-term outcomes. Similarly, an eight-gene risk
model (APOBEC3B, DOCK4, IER5L, LBH, LY6K, RERG, RMDN2 and
TSPAN2) was found to independently predict prognosis and
immune infiltration. Among these, LBH has been
experimentally validated as a functional biomarker: Its
upregulation enhances the radiosensitivity of A549 cells, whereas
its silencing restores radioresistance. These findings suggest that
LBH, as well as multi-gene risk scores, hold promise for
prognostic stratification and therapeutic decision-making in NSCLC
(49).
Transcriptome sequencing of p53 wild-type A549 and
p53-deficient H1299 NSCLC cell lines, along with their
radioresistant derivatives (A549IR and H1299IR), has revealed
shared molecular signatures associated with radioresistant
phenotypes (50). Specifically,
seven genes (ATRNL1, CA2, CNR1, FAM189A1, GFRA1, RASGRP1 and
RGL3) were upregulated, whereas nine genes (ADGRF1,
EPHA7, LOX, LY6G5C, NSUN7, SLC22A31, SNAI2, TNFRSF11B and
ZNF233) were downregulated. These dysregulated pathways
represent potential predictive biomarkers and therapeutic
targets.
Pathway-level analyses further highlighted
activation of the WNT signaling cascade, including WNT ligand
biosynthesis, WNT5A-FZD4 internalization and canonical
WNT/β-catenin signaling, together with NF-κB pathway upregulation.
Radioresistant H1299IR cells exhibited elevated β-catenin levels
due to sustained GSK3 activity downstream of AKT, promoting
enhanced cellular motility and invasion. These transcriptomic
alterations were accompanied by a senescence-associated secretory
phenotype, characterized by increased IL6, CXCL8 and
TGFβ2 expression and decreased NRG1 expression,
thereby supporting tumor progression (50).
Other studies have identified additional gene panels
with potential clinical relevance. Eight genes (FOLR3, SLC6A11,
ALPP, IGFN1, KCNJ12, RPS4XP22, HIST1H2BH and BLACAT1)
have been shown to be associated with RT response in patients with
NSCLC (51). Moreover, profiling
of drug-tolerant persister cancer cells has yielded a four-gene
prognostic risk index (LYNX1, SYNPO, GADD45B and
PDLIM1), the co-expression network of which was revealed to
be notably associated with RT response and OS (52).
Given the established link between autophagy and
radioresistance, Gao et al (53) developed a three-gene
autophagy-related prognostic model (SHC1, NAPSA and
AURKA), in which SHC1 and AURKA upregulation,
combined with NAPSA downregulation, predicted enhanced
radioresistance. Furthermore, strong expression of DNA repair genes
(ERCC1, ERCC4, ERCC5, XRCC5, RAD9A, PRKDC and the gene
encoding DNA-PK), as well as proliferation- and apoptosis-related
genes (MDM2, PIM2, BCL2 and PKCZ), has been observed
in radioresistant A549 cells compared with the more radiosensitive
NCI-H446 line, reinforcing their potential as biomarkers for
treatment stratification and combination therapy development
(54).
Emerging evidence has also implicated metabolic
pathways in modulating RT response. A recent study identified a
three-gene lactate metabolism-related risk model (ADAMTS3,
FADS2 and RTBDN) capable of distinguishing
radiosensitive from radioresistant patients, with FADS2
emerging as a key predictive biomarker. Further mechanistic
validation linked this signature to DNA repair modulation and tumor
immune response, highlighting lactate metabolism as a promising
source of novel biomarkers for precision RT (55).
Finally, keratin 6A (KRT6A) expression has
been associated with improved OS in patients with LC. Functional
experiments have shown that KRT6A downregulation reduces
proliferation and invasion in vitro, suggesting that while
KRT6A may not directly mediate radioresistance, it could
serve as a valuable prognostic marker and potential therapeutic
target (56).
Despite these advances, translating radiosensitivity
gene-expression signatures from preclinical models to clinical
practice remains challenging. Cell lines offer a controlled
platform for dissecting radiation response independent of clinical
confounders, but they lack microenvironmental, stromal and immune
interactions, realistic dose-rate effects and intratumoral
heterogeneity. Therefore, validation in physiologically relevant
models, such as patient-derived xenografts (PDXs), organoids and
prospective clinical cohorts, remains essential before these
signatures can be reliably implemented in routine clinical
decision-making.
Circulating tumor DNA (ctDNA)
ctDNA represents a fraction of cell-free DNA
released from tumor cells through necrosis, apoptosis,
macrophage-mediated clearance or direct secretion (57). LC exhibits marked intratumoral
heterogeneity, both spatially, across primary and metastatic sites
and temporally, as molecular characteristics evolve during disease
progression. Consequently, liquid biopsy offers a practical and
minimally invasive strategy for quantifying ctDNA levels in the
bloodstream, providing a dynamic snapshot of tumor burden, stage
and treatment response.
This approach holds particular value in radiation
oncology, as ctDNA measurement enables real-time monitoring of
therapeutic efficacy, detection of resistance emergence and
surveillance of disease progression during RT (58). Changes in ctDNA kinetics during
treatment closely mirror the cytotoxic effects of ionizing
radiation and tumor cell death, positioning ctDNA as a promising
biomarker of radiation response (59).
Recent evidence has demonstrated that a decline in
ctDNA levels during RT in patients with NSCLC is associated with a
reduction in tumor burden and may serve as an early predictor of
treatment response, even in cases where complete ctDNA clearance is
not achieved (35). These findings
support the integration of ctDNA monitoring into clinical practice
to guide adaptive RT strategies and enable timely treatment
modifications.
Proteomic biomarkers
Using a proteomics approach combining
two-dimensional electrophoresis and matrix-assisted laser
desorption ionization-time of flight mass spectrometry, Yun et
al (60) identified several
proteins with notably increased expression in radioresistant H460
cancer stem cell (CSC) lines compared with radiosensitive parental
H460 cells. These candidate biomarkers included fatty acid
synthase, vimentin, glucose-regulated protein 78, plasminogen
activator inhibitor-2, nodal modulator 2, kinesin light chain 4 and
procollagen-lysine, 2-oxoglutarate 5-dioxygenase 3 (PLOD3)
(Fig. 2). Their upregulation may
serve as predictive indicators of RT response, enable pre-treatment
identification of radioresistant tumors and represent promising
therapeutic targets to overcome resistance. Table IV summarizes proteomic biomarkers
identified in multiple studies that are associated with
radioresistance in lung cancer.
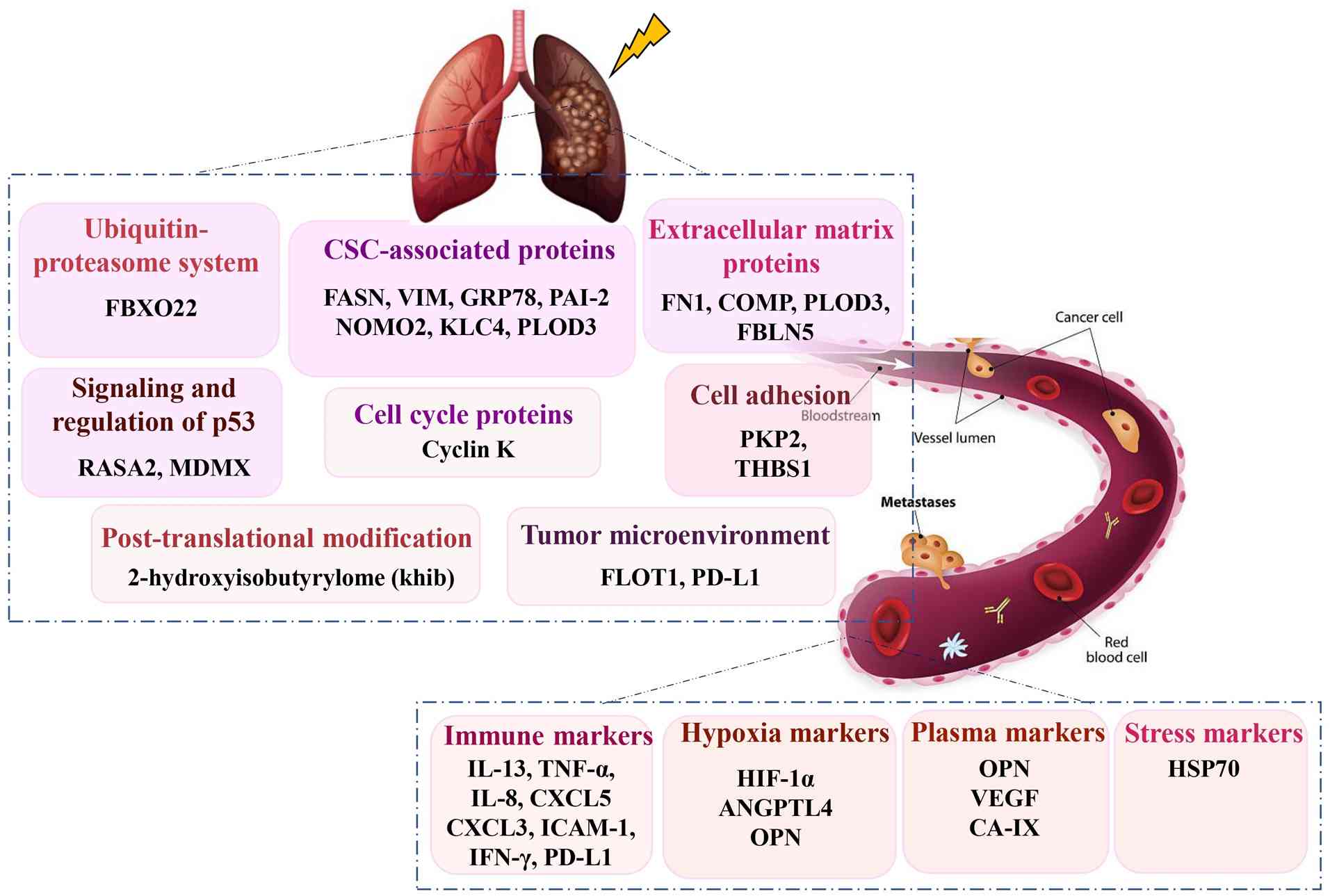 | Figure 2.Summary of proteomic biomarkers
associated with lung cancer radioresistance. FBXO22, F-box protein
22; CSC, cancer stem cell; FASN, fatty acid synthase; VIM,
vimentin; GRP78, glucose-regulated protein 78; PAI-2, plasminogen
activator inhibitor-2; NOMO2, nodal modulator 2; KLC4, kinesin
light chain 4; PLOD3, procollagen-lysine, 2-oxoglutarate
5-dioxygenase 3; FN1, fibronectin 1; COMP, cartilage oligomeric
matrix protein; FBLN5, fibulin-5; RASA2, Ras p21 protein activator;
PKP2, plakophilin 2; THBS1, thrombospondin 1; FLOT1, flotillin-1;
PD-L1, programmed cell death ligand 1; HIF-1α, hypoxia-inducible
factor 1α; ANGPTL4, angiopoietin-like 4 protein; OPN, osteopontin;
CA IX, carbonic anhydrase IX; HSP, heat shock protein. |
| Table IV.Proteomic profiles associated with RT
response in lung cancer. |
Table IV.
Proteomic profiles associated with RT
response in lung cancer.
| First author/s,
year | Marker | Method of
detection | Cohort (size) | Regulation | Clinical
significance | Pathways | Result | (Refs.) |
|---|
| Dehing-Oberije
et al, 2011 | CEA, IL-6 | ELISA | NSCLC (n=158) | Upregulation | Lower probability
of survival | CEA: Cell adhesion;
IL-6: JAK/STAT signaling |
Radioresistance | (66) |
| Ostheimer et
al, 2014 | VEGF, CA-IX | ELISA | Advanced NSCLC
(n=55) | Upregulation | Poor OS | Hypoxia |
Radioresistance | (65) |
| Ostheimer et
al, 2014 | OPN | ELISA | Advanced NSCLC
(n=55) | Upregulation | Poor OS | Hypoxia |
Radioresistance | (65) |
| Yun et al,
2016 | FASN, VIM, GRP78,
PAI-2, NOMO2, KLC4 and PLOD3 | 2D electrophoresis,
MALDI-TOF mass spectrometry, western blotting | Human H460, A549
and H1299 NSCLC cells | Upregulation | Lower RT
response | Regulation of cell
death, cancer and stem cell proliferation, differentiation and
morphogenesis |
Radioresistance | (60) |
| Ostheimer et
al, 2017 | OPN | ELISA | Advanced NSCLC at
M0 (n=44) | Upregulation | Poor OS | Hypoxia |
Radioresistance | (64) |
| Ostheimer et
al, 2017 | HSP70 | ELISA | Advanced NSCLC at
M0 (n=44) | Upregulation | Poor OS | Tumor protection
from stress-induced programmed cell death |
Radioresistance | (64) |
| Afsar and Uysal,
2019 | HIF-1α | ELISA | Locally advanced
NSCLC (n=80) | Downregulation | Improved RT
response | Response of cells
to hypoxia |
Radiosensitivity | (62) |
| Baek et al,
2019 | PLOD3 | Western
blotting | H460 and A549
cancer cell lines | Upregulation | Poor 5-year
survival | Regulating
apoptosis |
Radioresistance | (71) |
| Yao et al,
2020 | Cyclin K | IHC | A549 and H460 cell
lines | Upregulation | Poor OS | Tumorigenesis via
positive modulation of β-catenin/cyclin D1 |
Radioresistance | (69) |
| Sui et al,
2021 | IL-8 | U-PLEX assay | Locally advanced
inoperable/unresectable NSCLC (n=31) | Upregulation | Improved response
after RT | Regulating
angiogenesis |
Radiosensitivity | (67) |
| Sui et al,
2021 | TNF-α | U-PLEX assay | Locally advanced
inoperable/unresectable NSCLC (n=31) | Upregulation | Improved response
after RT | Antitumor immune
response |
Radiosensitivity | (67) |
| Sui et al,
2021 | PD-L1, ICAM-1 | Luminex assay | Locally advanced
inoperable/unresectable NSCLC (n=31) | Downregulation | Improved response
After RT | T-cell dysfunction,
inflammatory process and tumor metastasis |
Radiosensitivity | (67) |
| Cheng et al,
2021 | PKP2 | CRISPR/Cas9 library
screen | A549 cells | Upregulation | Poor OS and
postprogression survival | PKP2 positively
regulates β-catenin stability to induce transcription of LIG4,
involved in non-homologous end-joining-mediated repair |
Radioresistance | (70) |
| Zhang et al,
2022 | ANGPTL4 | RT-qPCR, western
blotting | In vivo and
in vitro experiments | Upregulation | Worse
radiotherapeutic outcome | Inhibition of
ferroptosis |
Radioresistance | (63) |
| Li et al,
2022 | FN1, THBS1 | Tandem Mass
Tagbased quantitative proteomic analysis | H460 cells | Upregulation | Low survival rates
migration | Adhesion and |
Radioresistance | (68) |
| Wang et al,
2023 | FLOT1 | Western
blotting | A549 and H520 cell
lines | Upregulation | Higher
radioresistance | Positive regulation
of PD-L1 |
Radioresistance | (77) |
| Li et al,
2024 | RASA2 | IHC | Stage IIIa and IVa
LUAD (n=205) | Upregulation | Poor response to
RT | Regulating
apoptosis |
Radioresistance | (72) |
| Chen et al,
2024 | FBXO22 | Western
blotting | Lung cancer cell
lines | Upregulation | Higher
radioresistance | Activation of the
FOXM1/Rad51 axis and DNA repair |
Radioresistance | (73) |
| Ji et al,
2025 | MDMX | IHC | LUAD and LSCC
tissues | Upregulation | Increased
radiosensitivity | Regulation of
P53-mediated autophagy |
Radiosensitivity | (74) |
| Reno et al,
2025 | COMP | RT-qPCR, proteomics
(LC-MS/MS) | A549, NCI-H1975 and
NCI-H1437 cell lines | Upregulation | Increased
proliferation, invasion, migration and viability after
irradiation | Oxidative
phosphorylation and drug resistance |
Radioresistance | (75) |
| Zhang et al,
2025 | FBLN5 | Spatial,
transcriptomics single-cell RNA-sequencing | NSCLC (n=105),
in vitro CAF models | Upregulation | Poor response to
RT | pathways Src-STAT3
pathway, suppression of ferroptosis |
Radioresistance | (76) |
CSCs, a subpopulation within tumors with
self-renewal, differentiation and tumor-initiating capacity, have
been shown to be intrinsically more resistant to both irradiation
and systemic therapies than non-CSCs (61). This property may contribute to
post-RT recurrence and metastasis, highlighting the need for
innovative RT strategies aimed specifically at eradicating CSCs
(60).
Hypoxia-related biomarkers
Hypoxia is a well-recognized driver of
radioresistance. In NSCLC, serial measurements of serum
hypoxia-inducible factor 1α (HIF-1α) before and after
chemoradiotherapy have revealed notable decreases during treatment,
associated with tumor shrinkage. These findings suggest that HIF-1α
could serve as a dynamic biomarker for monitoring tumor response
(62).
Angiopoietin-like 4 protein (ANGPTL4) has also been
implicated in NSCLC radioresistance. Under hypoxic conditions,
ANGPTL4 upregulation suppresses ferroptosis by upregulating
antioxidant proteins, thereby enhancing tumor cell survival after
irradiation. Furthermore, ANGPTL4 is enriched in exosomes secreted
by hypoxic tumor cells, which transfer radioresistance signals to
neighboring normoxic cells through indirect ferroptosis inhibition.
These findings position ANGPTL4 as both a predictive biomarker and
a potential therapeutic target to enhance radiosensitivity
(63).
Other hypoxia-induced molecules include osteopontin
(OPN) and heat shock protein 70 (HSP70). Elevated pre-RT plasma OPN
levels have been associated with poor OS, whereas post-treatment
reductions in HSP70 within 4–6 weeks are associated with tumor
regression. Notably, patients with relatively high post-RT HSP70
levels demonstrate improved treatment responses, probably
reflecting an immunostimulatory effect of extracellular HSP70
released from dying tumor cells (64). Together, these results support the
combined assessment of OPN and HSP70 as predictive and dynamic
biomarkers of treatment response.
Additional hypoxia-related biomarkers, VEGF and
carbonic anhydrase IX, have been linked to poor OS, with their
expression associated with adverse clinical features such as weight
loss, reduced lung function and larger tumor size. These markers
may help identify highly hypoxic, aggressive tumors, supporting
their integration into multi-center validation studies and
personalized treatment planning (65).
Plasma and cytokine biomarkers
Incorporation of blood-based biomarkers into
prognostic models has been shown to notably improve survival
prediction in NSCLC. Among a panel of eight analytes, serum CEA and
IL-6 have been identified as independent predictors of poor
outcomes (66). Similarly,
cytokine profiling of patients undergoing chemoradiotherapy has
revealed that elevated post-treatment levels of IL-13, TNF-α, IL-8,
CXCL5 and CXCL3, together with reduced levels of intercellular
adhesion molecule 1 (ICAM-1), IFN-γ and soluble programmed cell
death ligand 1 (PD-L1), are associated with improved objective
response. Combinations such as IL-8 with ICAM-1 or soluble PD-L1
with TNF-α may further enhance predictive accuracy and IL-8/ICAM-1
levels are associated with PFS (67). These findings highlight plasma
cytokines as valuable tools for stratifying patients and optimizing
RT strategies.
Proteomic and molecular
biomarkers
Proteomic profiling of H460 LC cells pre- and
post-irradiation has identified fibronectin 1 and thrombospondin 1
as key contributors to radioresistance and poor outcomes (68). Yao et al (69) demonstrated that cyclin K may
stabilize β-catenin and promote G2/M checkpoint
activation, thereby enabling DNA repair and survival. By contrast,
silencing cyclin K increased radiosensitivity in vitro and
in vivo by abrogating this checkpoint, suggesting cyclin K
as both a predictive biomarker and therapeutic target.
Cheng et al (70) reported that PRMT1-mediated
methylation of plakophilin 2 (PKP2) can recruit ubiquitin-specific
protease 7, which stabilizes DNA ligase 4 and enhances
non-homologous end-joining repair. Pharmacological inhibition of
PRMT1 has been shown to disrupt this axis and sensitize NSCLC cells
to RT, supporting PKP2 as a novel predictive biomarker and
therapeutic target. Similarly, knockdown of PLOD3 triggers ER
stress and caspase-3-mediated apoptosis, thereby enhancing
radiosensitivity (71).
Ras p21 protein activator, a Ras GTPase-activating
protein, has been demonstrated to promote p53 phosphorylation and
proteasomal degradation, leading to reduced apoptosis and increased
radioresistance. Its expression is associated with poor RT
response, underscoring its value as a biomarker and target for
therapeutic intervention (72).
Upregulation of F-box protein 22 (FBXO22) activates the FOXM1/Rad51
axis to promote homologous recombination repair, whereas its
inhibition, particularly with the small molecule deguelin, restores
radiosensitivity (73).
Conversely, high expression of MDMX has been shown to be associated
with enhanced response to RT and longer OS, implicating it as a
favorable biomarker in LUAD and LSCC (74).
Cartilage oligomeric matrix protein, an
extracellular matrix protein, promotes NSCLC proliferation and
invasion following irradiation, indicating its potential as a
biomarker for identifying patients likely to benefit from
intensified treatment or combination therapy (75).
Tumor microenvironment
(TME)-associated biomarkers
The TME serves a critical role in RT response. High
stromal expression of fibulin-5 (FBLN5) in cancer-associated
fibroblasts (CAFs) activates Src-STAT3 signaling, inhibits
ferroptosis and promotes post-irradiation tumor survival.
Clinically, elevated FBLN5 levels are associated with poor RT
outcomes, supporting its role as a predictive biomarker (76). Similarly, flotillin-1 (FLOT1)
upregulates PD-L1 and promotes epithelial-mesenchymal transition
(EMT), enhancing cell motility and DNA damage tolerance. FLOT1
inhibition sensitizes cells to RT, activates the STING pathway and
enhances CD8+ T-cell recruitment through chemokine
secretion (77).
In a large retrospective study of 328 patients with
stage III NSCLC treated with concurrent chemoradiation and
durvalumab, high PD-L1 expression (TPS ≥90%) and elevated tumor
mutational burden were associated with prolonged disease control,
supporting their use for patient stratification prior to RT and
immunotherapy (78).
Multi-omics and inflammatory
biomarkers
A prior multi-omics analysis comparing parental A549
cells and their radioresistant derivatives has revealed >900
differentially expressed genes and ~700 proteins, including
>30,000 sites of lysine 2-hydroxyisobutyrylation (khib).
Notably, EGFR was shown to be both upregulated and highly
khib-modified in radioresistant cells, suggesting that
khib-regulated EGFR may represent a novel mechanism of
radioresistance and a therapeutic vulnerability (79). Fig.
2 provides a comprehensive summary of proteomic biomarkers
associated with lung cancer radioresistance.
Finally, systemic inflammatory markers such as
neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio,
derived NLR and systemic immune-inflammation index have shown
prognostic and predictive value in locally advanced NSCLC. Low
values of these markers have been shown to be independently
associated with improved PFS, OS and locoregional control and to be
linked to increased radiosensitivity (80). These metrics are inexpensive,
widely accessible and may complement molecular biomarkers in
patient stratification and treatment planning.
Epigenetic biomarkers
Epigenetic regulation serves a pivotal role in
shaping the response to irradiation in LC. Radiosensitive and
radioresistant NSCLC cell lines display distinct methylation
signatures, underscoring the involvement of epigenetic mechanisms
in radioresponse. Genome-wide analysis of CpG methylation patterns
has revealed that several key regulators of radiosensitivity are
epigenetically controlled by CpG methylation (81). Notably, the presence of an
unmethylated promoter in the insulin-like growth factor-binding
protein-3 gene has been associated with poor RT response and
unfavorable clinical outcomes in patients receiving adjuvant
chemoradiotherapy (82).
Furthermore, radiation-induced changes in DNA methylation vary in a
tissue-specific and dose-dependent manner, highlighting the
complexity of epigenetic modulation in RT response (83).
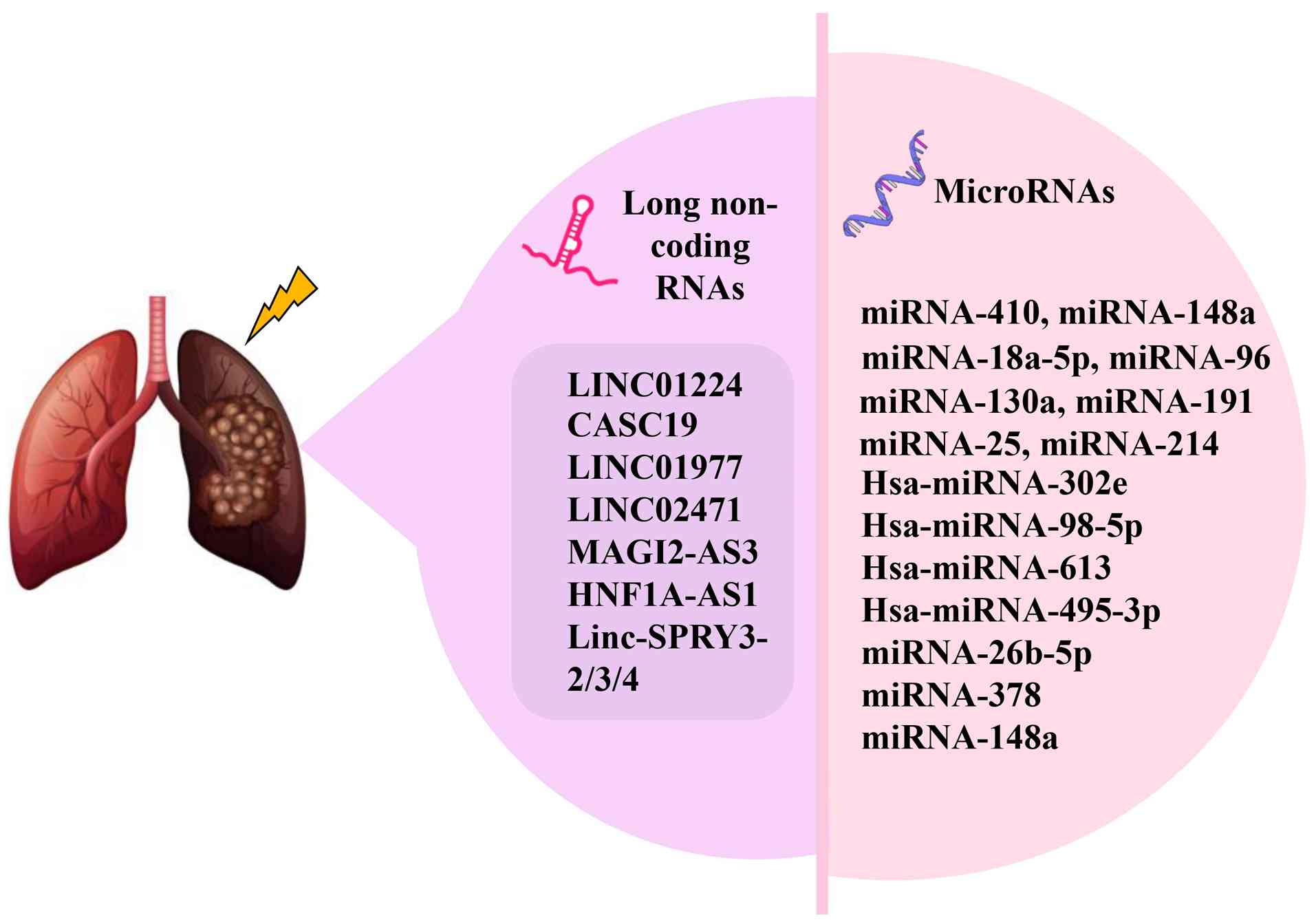
(miRNAs/miRs) as biomarkers of RT
response
miRNAs are short (~22 nucleotides) non-coding RNAs
that post-transcriptionally regulate gene expression by binding to
complementary sequences on target mRNAs (84). Their notable stability in tissues,
plasma and other biofluids makes them attractive candidates for
minimally invasive biomarkers (85). Numerous differentially expressed
miRNAs have been implicated in LC radiosensitivity (Fig. 3).
For example, miR-214 is upregulated in
radioresistant NSCLC cells, where it enhances radioresistance and
inhibits RT-induced apoptosis (86). Similarly, miR-410 promotes EMT and
radioresistance by augmenting DNA damage repair capacity,
suggesting its potential as a therapeutic target (87). Serum levels of miR-130a, miR-191
and miR-25 have been shown to be increased following 2–4 Gy
irradiation in patients with NSCLC, and are associated with
heightened invasiveness of A549 cells in vitro and in
xenograft models, thus supporting their potential role as
biomarkers of RT-induced metastasis (88). Elevated exosomal miR-96 has been
associated with vascular invasion and poor OS, indicating its
prognostic value for radioresistant NSCLC (20).
Plasma miRNA signatures also hold promise for
stratifying patients. Hsa-miR-302e, hsa-miR-98-5p, hsa-miR-613 and
hsa-miR-495-3p have all been linked to radiosensitivity in NSCLC
(89), while miR-18a-5p levels
have been associated with treatment response and could be used to
categorize patients into radiosensitive or radioresistant subgroups
(90). Zhang and Hu (91) identified miR-148a as a candidate
biomarker of radioresistance, whereas miR-26b-5p was found to be
notably downregulated in LUAD tissues, serum and radioresistant
cell lines. Upregulation of miR-26b-5p increases radiosensitivity
in both parental LUAD cells and radiation-resistant LUAD cells
(A549R) by promoting DNA damage and apoptosis, partly through
direct inhibition of activating transcription factor-2. Notably,
exosomal transfer of miR-26b-5p from A549 cells to resistant cells
may restore radiosensitivity, underscoring its value as a
non-invasive predictive marker (92).
Serum exosomal miR-378 has emerged as a clinically
relevant biomarker; its levels are notably decreased after RT and
high baseline expression is associated with poor OS, making it an
independent prognostic factor (93). Similarly, miR-148a, a tumor
suppressor, is downregulated in radioresistant patients but
upregulated following RT in radiosensitive ones. Its upregulation
inhibits proliferation, migration and invasion by targeting SOS2,
thereby improving radiosensitivity and serving as a potential
marker for both prediction and monitoring of RT response (91).
Long non-coding RNAs (lncRNAs) and
radioresistance
LncRNAs (>200 nucleotides) have emerged as key
regulators of carcinogenesis, immune modulation, apoptosis and
therapy response (94). Several
lncRNAs have been implicated in RT outcomes in NSCLC, making them
promising prognostic and predictive markers (Fig. 3).
LINC01224 expression has been associated with RT
response, suggesting its potential as a prognostic indicator
(95). Song et al (96) identified a four-lncRNA signature
(CASC19, LINC01977, LINC02471 and MAGI2-AS3) that was shown to be
associated with radiological response and could accurately predict
patient prognosis.
HNF1A-AS1, a lncRNA upregulated in NSCLC,
contributes to advanced disease stages and radioresistance by
sponging miR-92a-3p, which results in MAP2K4 upregulation and JNK
pathway activation. Silencing HNF1A-AS1 has been reported to reduce
proliferation, induce apoptosis and notably sensitize NSCLC cells
to RT, positioning the HNF1A-AS1/miR-92a-3p/MAP2K4 axis as a
potential biomarker and therapeutic target (97).
Notably, male patients with NSCLC exhibit a unique
pattern of radiosensitivity linked to Y-chromosome loss (LOY) and
dysregulation of Y-linked lncRNAs. Linc-SPRY3-2/3/4 transcripts are
dose-dependently induced after irradiation in radiosensitive cell
lines but absent in LOY radioresistant lines. These transcripts
interact with IGF2BP3 to destabilize oncogenic mRNAs, including
HMGA2 and c-MYC, thereby promoting apoptosis. Loss of
linc-SPRY3-2/3/4 or LOY is associated with poorer OS, suggesting a
male-specific biomarker signature for predicting radiosensitivity
(98).
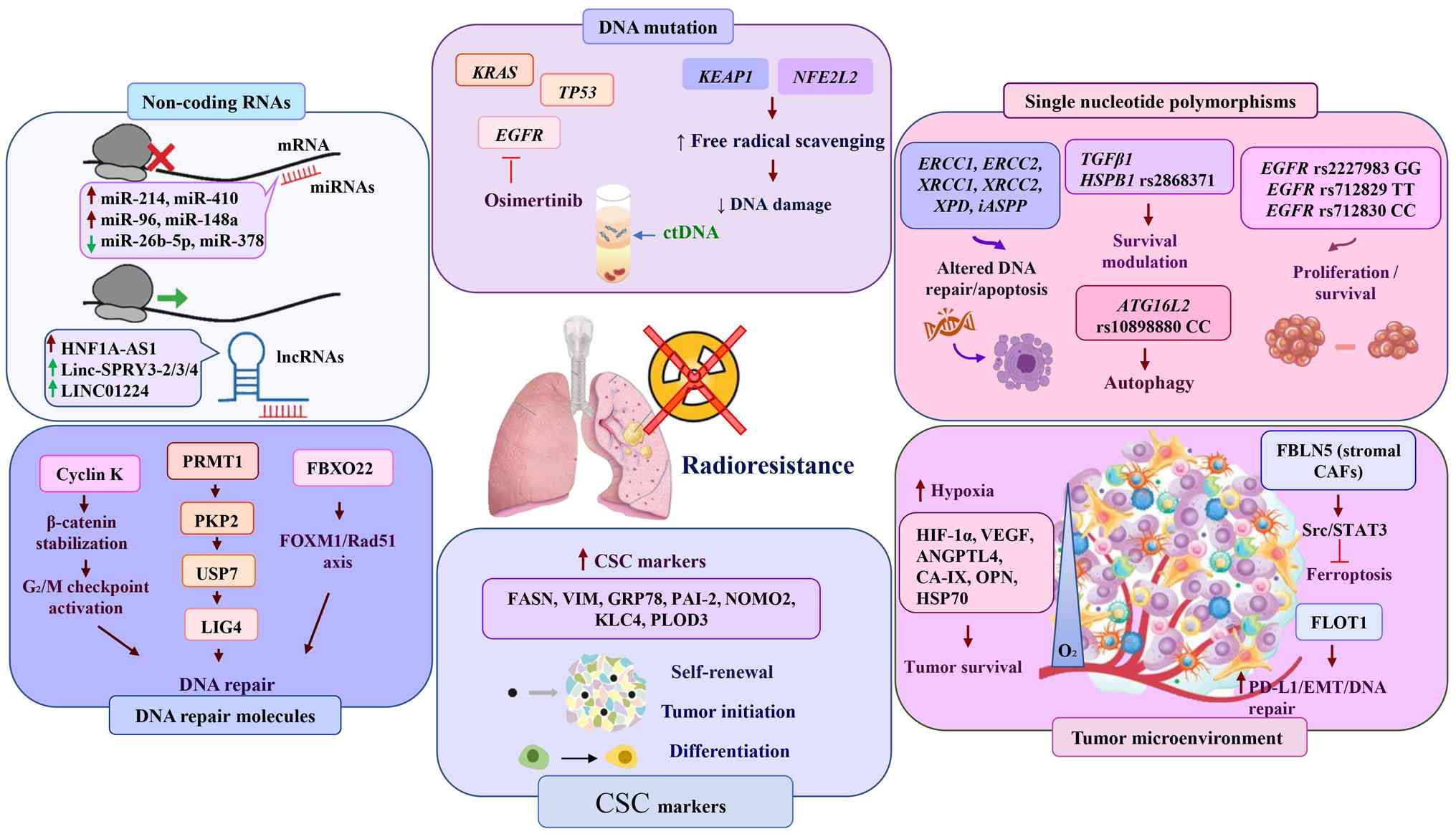
Fig. 4 provides an
integrated overview of the key genetic, epigenetic, circulating and
proteomic biomarkers that have been implicated in LC
radioresistance, highlighting their potential roles in patient
stratification and personalized RT strategies. The figure provides
an overview of the main molecular biomarkers implicated in LC
radioresistance and their associated pathways. It includes genetic
alterations (such as EGFR, KRAS, TP53, KEAP1 and
NFE2L2), DNA repair factors (Cyclin K, PRMT1 and FBXO22),
non-coding RNAs (miRNAs and lncRNAs) and CSC markers. Contributors
to the TME, such as hypoxia, stromal CAFs and key signaling
pathways (HIF-1α, VEGF, PD-L1) are also shown. Collectively, these
biomarkers and pathways interact to promote tumor survival,
treatment resistance and disease progression, underscoring
potential targets for improving RT outcomes.
Limitations and perspectives
Over the past decade, cancer management has evolved
considerably at both conceptual and methodological levels,
propelled by advances in molecular biology and technological
innovation. Modern RT techniques have achieved marked improvements
in tumor targeting and sparing of adjacent healthy tissue; however,
these technological refinements alone are insufficient to overcome
the biological complexity underlying tumor resistance to ionizing
radiation. A major unmet need is the ability to predict which
patients will derive durable benefit from RT and which are probably
to experience treatment failure due to intrinsic or acquired
radioresistance.
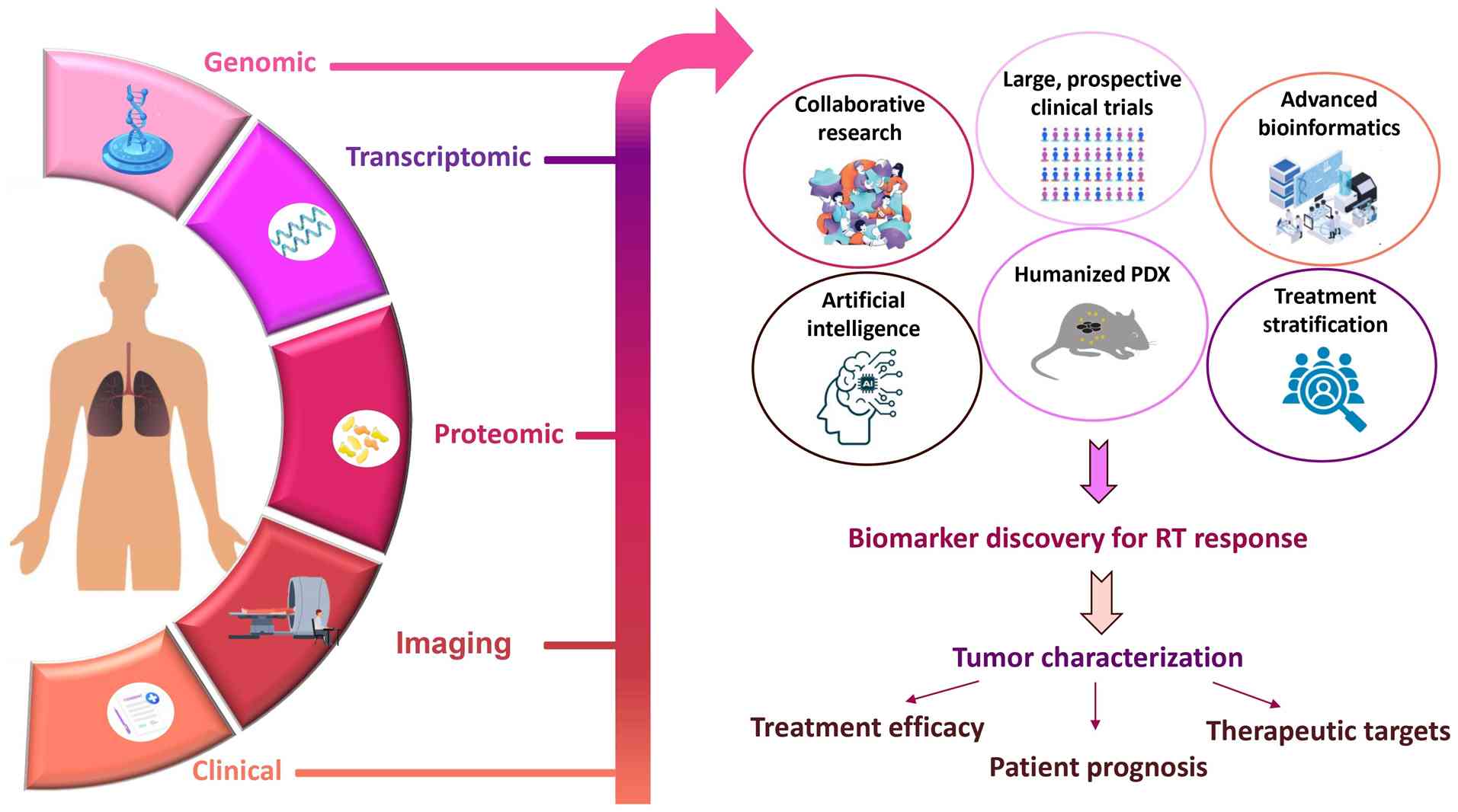
At present, no predictive biomarkers for RT
response in LC have been validated for routine clinical use within
an evidence-based framework. Most reported candidates have emerged
from in vitro studies or small-scale clinical cohorts, often
with limited statistical power and population-specific
applicability. To translate these findings into clinical practice,
several key challenges must be addressed (Fig. 5): i) Lack of biomarker convergence
and validation. Most studies focus on individual biomarkers or
small panels of molecular targets, frequently chosen based on the
specific research interests or preliminary data of a group.
Consequently, few biomarkers have been independently validated
across multiple studies, limiting reproducibility and
comparability. This highlights the need for collaborative,
multicenter efforts and integrative approaches to evaluate
promising candidates in larger, diverse patient populations using
standardized protocols.
ii) Biological complexity of radioresistance.
Radioresistance arises from the interplay of multiple pathways,
including DNA damage repair, oxidative stress responses, hypoxia
signaling, tumor-stroma interactions and immune modulation. A
single biomarker is unlikely to capture this complexity or
accurately predict RT outcomes. Multivariable models integrating
several molecular and cellular determinants are likely to offer
greater predictive accuracy and clinical utility, facilitating
improved patient selection and personalized treatment
strategies.
iii) Integration of multi-omics and artificial
intelligence (AI). Incorporating multidimensional data, including
genomic, transcriptomic, epigenetic, proteomic, imaging and
clinical information, offers the opportunity to build robust
predictive models that reflect the full biological heterogeneity of
lung tumors. Machine learning and AI-driven analytical pipelines
can extract complex patterns from these data, enabling
high-performance prediction models that inform adaptive RT and
precision oncology approaches.
iv) Need for representative preclinical models.
Mechanistic insights and biomarker discovery rely heavily on
preclinical models. PDXs, especially those generated from
radioresistant tumors, are valuable tools for predicting RT
efficacy and conducting ‘co-clinical’ studies. However, current
models have limitations, including replacement of human stroma with
murine stroma and the requirement for immunodeficient hosts, which
prevents assessment of immune-mediated effects. Development of
humanized PDX models that retain tumor-immune interactions will be
critical for advancing translational research (99).
v) Influence of concurrent treatments. A number of
biomarker studies are confounded by concomitant chemotherapy,
particularly platinum-based regimens, making it difficult to
distinguish radiosensitivity-specific effects from combined
chemoradiotherapy responses. Stratifying patients by treatment
regimen or conducting analyses in RT-only cohorts will be necessary
to identify these contributions and avoid false-positive
associations.
vi) Variability in experimental design and
methodology. Differences in sample collection, preparation,
analytical techniques and statistical approaches notably limit
reproducibility and generalizability across studies. Establishing
standardized operating procedures and consensus criteria for
biomarker studies is imperative. Future research should prioritize
large, prospective trials with pre-specified biomarker endpoints,
multicenter validation and integration of bioinformatics pipelines
capable of harmonizing multi-omics and clinical data.
In summary, while the discovery of biomarkers of
radioresistance in LC remains in an early phase, the convergence of
molecular biology, high-throughput technologies and AI-driven
analytics is promising. Overcoming current methodological and
translational challenges will be critical to accelerating the
development and clinical implementation of robust, reproducible
biomarkers. Ultimately, such efforts will enable precision RT
strategies that optimize therapeutic efficacy, minimize toxicity
and improve survival outcomes for patients with LC.
Conclusion
Cancer cell resistance to ionizing radiation
remains a critical obstacle in the management of LC. This
resistance is highly patient-dependent, either arising from
intrinsic genetic predispositions or developing as an adaptive
response during treatment, ultimately contributing to therapeutic
failure. Innate and acquired radioresistance both engage multiple
molecular pathways and reveal a broad spectrum of candidate
biomarkers that could guide precision medicine approaches.
Incorporating such biomarkers into clinical workflows would enable
radiation oncologists to identify patients most likely to benefit
from RT, tailor radiation dose and fractionation schemes and
integrate radiosensitizing agents to enhance therapeutic
efficacy.
Although substantial progress has been made in
characterizing biomarkers of radioresistance, their translation
into routine clinical practice is still limited. Independent
validation in large, prospective cohorts and robust meta-analyses
are urgently needed to confirm their predictive and prognostic
utility.
Advances in multi-omics technologies have greatly
expanded the understanding of the genomic, transcriptomic and
epigenetic alterations that underlie radioresistance, paving the
way for individualized treatment strategies. Ongoing research
continues to explore tumor heterogeneity and the integration of
biomarker data into predictive models, with the ultimate goal of
enabling truly personalized, adaptive RT that improves survival
outcomes and quality of life for patients with LC.
Acknowledgements
Not applicable.
Funding
The publication has been prepared within the framework of the
project funded by Mohammed VI Polytechnic University and OCP
Foundation (TNI 2024 program). The authors would like to thank The
Centre National pour la Recherche Scientifique et Technique (CNRST)
of Morocco for funding Attouahri Fatima Zohra's ‘PhD-ASociate
Scholarship-PASS’.
Availability of data and materials
Not applicable.
Authors' contributions
FZA initially began the review and wrote the first
draft of the manuscript with the help of IC, MAb, AL and MEMz. MAt,
MRT, MO, MEMa, MK, KEn and KEr reviewed, completed and improved the
review according to their respective specialties. Data
authentication is not applicable. All authors have approved the
final the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ANGPTL4
|
angiopoietin-like 4 protein
|
|
ATG16L2
|
autophagy related 16 like 2 gene
|
|
CA-IX
|
carbonic anhydrase IX
|
|
COMP
|
cartilage oligomeric matrix
protein
|
|
CSC
|
cancer stem cell
|
|
ctDNA
|
circulating tumor DNA
|
|
ERCC1
|
excision repair
cross-complementation
|
|
FASN
|
fatty acid synthase
|
|
FBLN5
|
fibulin-5
|
|
FLOT1
|
flotillin-1
|
|
FBXO22
|
F-box protein 22
|
|
FN1
|
fibronectin 1
|
|
FOLR3
|
folate receptor-3
|
|
GRP78
|
glucose-regulated protein 78
|
|
HIF-1α
|
hypoxia-inducible factor 1α
|
|
HSP70
|
heat shock protein 70
|
|
HSPB1
|
heat shock protein β-1
|
|
iASPP
|
inhibitor of apoptosis-stimulating
protein of p53
|
|
ICAM-1
|
intercellular adhesion molecule 1
|
|
KEAP1
|
Kelch-like ECH-associated protein
1
|
|
KLC4
|
kinesin light chain 4
|
|
LIG4
|
DNA ligase 4
|
|
lncRNA
|
long noncoding RNA
|
|
LSCC
|
lung squamous cell carcinoma
|
|
LUAD
|
lung adenocarcinoma
|
|
NFE2L2
|
nuclear factor erythroid 2-related
factor-2
|
|
NOMO2
|
nodal modulator 2
|
|
NSCLC
|
non-small cell lung cancer
|
|
OPN
|
osteopontin
|
|
PAI-2
|
plasminogen activator inhibitor-2
|
|
PD-L1
|
programmed cell death ligand 1
|
|
PFS
|
progression-free survival
|
|
PKP2
|
plakophilin 2
|
|
PLOD3
|
procollagen-lysine, 2-oxoglutarate
5-dioxygenase 3
|
|
RASA2
|
Ras p21 protein activator
|
|
RT
|
radiotherapy
|
|
SNP
|
single nucleotide polymorphism
|
|
THBS1
|
thrombospondin 1
|
|
VIM
|
vimentin
|
|
XRCC1
|
X-ray repair cross-complementing
protein 1
|
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Ruiz-Cordero R and Devine WP: Targeted
therapy and checkpoint immunotherapy in lung cancer. Surg Pathol
Clin. 13:17–33. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Travis WD, Brambilla E, Nicholson AG,
Yatabe Y, Austin JHM, Beasley MB, Chirieac LR, Dacic S, Duhig E,
Flieder DB, et al: The 2015 World Health Organization
Classification of Lung Tumors: Impact of Genetic, Clinical and
Radiologic Advances Since the 2004 Classification. J Thorac Oncol.
10:1243–1260. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schwartz AG and Cote ML: Epidemiology of
lung cancer. Adv Exp Med Biol. 893:21–41. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Popper HH: Progression and metastasis of
lung cancer. Cancer Metastasis Rev. 35:75–91. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vinod SK and Hau E: Radiotherapy treatment
for lung cancer: Current status and future directions. Respirology.
25 (Suppl 2):S61–S71. 2020. View Article : Google Scholar
|
|
7
|
Delaney GP and Barton MB: Evidence-based
estimates of the demand for radiotherapy. Clin Oncol (R Coll
Radiol). 27:70–76. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Giuranno L, Ient J, De Ruysscher D and
Vooijs MA: Radiation-induced lung injury (RILI). Front Oncol.
9:8772019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chandra RA, Keane FK, Voncken FEM and
Thomas CR: Contemporary radiotherapy: Present and future. The
Lancet. 398:171–184. 2021. View Article : Google Scholar
|
|
10
|
Wang Y, Gudikote J, Giri U, Yan J, Deng W,
Ye R, Jiang W, Li N, Hobbs BP, Wang J, et al: RAD50 Expression is
associated with poor clinical outcomes after radiotherapy for
resected non-small cell lung cancer. Clin Cancer Res. 24:341–350.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ashrafi A, Akter Z, Modareszadeh P,
Modareszadeh P, Berisha E, Alemi PS, Chacon Castro MDC, Deese AR
and Zhang L: Current landscape of therapeutic resistance in lung
cancer and promising strategies to overcome resistance. Cancers
(Basel). 14:45622022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Salama JK and Vokes EE: New radiotherapy
and chemoradiotherapy approaches for non-small-cell lung cancer. J
Clin Oncol. 31:1029–1038. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee SY, Jeong EK, Ju MK, Jeon HM, Kim MY,
Kim CH, Park HG, Han SI and Kang HS: Induction of metastasis,
cancer stem cell phenotype, and oncogenic metabolism in cancer
cells by ionizing radiation. Mol Cancer. 16:102017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Busato F, Khouzai BE and Mognato M:
Biological mechanisms to reduce radioresistance and increase the
efficacy of radiotherapy: State of the art. Int J Mol Sci.
23:102112022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bivona TG and Doebele RC: A framework for
understanding and targeting residual disease in oncogene-driven
solid cancers. Nat Med. 22:472–478. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kirsch DG, Diehn M, Kesarwala AH, Maity A,
Morgan MA, Schwarz JK, Bristow R, Demaria S, Eke I, Griffin RJ, et
al: The future of radiobiology. J Natl Cancer Inst. 110:329–340.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sørensen BS, Andreassen CN and Alsner J:
Molecular Biomarkers in Radiation Oncology. Radiation Oncology.
Wenz F: Springer International Publishing, Cham; pp. 1–20. 2019,
View Article : Google Scholar
|
|
18
|
Baumann M, Krause M, Overgaard J, Debus J,
Bentzen SM, Daartz J, Richter C, Zips D and Bortfeld T: Radiation
oncology in the era of precision medicine. Nat Rev Cancer.
16:234–249. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Landeck L, Kneip C, Reischl J and
Asadullah K: Biomarkers and personalized medicine: Current status
and further perspectives with special focus on dermatology. Exp
Dermatol. 25:333–339. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zheng Q, Ding H, Wang L, Yan Y, Wan Y, Yi
Y, Tao L and Zhu C: Circulating Exosomal miR-96 as a novel
biomarker for radioresistant Non-Small-Cell lung cancer. J Oncol.
2021:58939812021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Scott JG, Berglund A, Schell MJ, Mihaylov
I, Fulp WJ, Yue B, Welsh E, Caudell JJ, Ahmed K, Strom TS, et al: A
genome-based model for adjusting radiotherapy dose (GARD): A
retrospective, cohort-based study. Lancet Oncol. 18:202–211. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
The Promise of Precision Medicine.
National Institutes of Health (NIH); 2020
|
|
23
|
Peinado-Serrano J and Carnero A: Molecular
radiobiology in Non-small cell lung cancer: Prognostic and
predictive response factors. Cancers (Basel). 14:22022022.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yang WC, Hsu FM and Yang PC: Precision
radiotherapy for non-small cell lung cancer. J Biomed Sci.
27:822020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nickoloff JA, Sharma N and Taylor L:
Clustered DNA Double-strand breaks: Biological effects and
relevance to cancer radiotherapy. Genes (Basel). 11:992020.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gopal P, Yard BD, Petty A, Lal JC, Bera
TK, Hoang TQ, Buhimschi AD and Abazeed ME: The mutational landscape
of cancer's Vulnerability to ionizing radiation. Clin Cancer Res.
28:5343–5358. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhu DQ, Liu Y, Yu ZJ, Zhang RH, Li AW,
Gong FY, Wang W, Xiao W and Fan Q: The diverse analysis identifies
mutated KRAS associated with radioresistance in Non-Small cell lung
cancer. World J Oncol. 13:84–95. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang M, Kern AM, Hülskötter M, Greninger
P, Singh A, Pan Y, Chowdhury D, Krause M, Baumann M, Benes CH, et
al: EGFR-mediated chromatin condensation protects KRAS-mutant
cancer cells against ionizing radiation. Cancer Res. 74:2825–2834.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang M, Han J, Marcar L, Black J, Liu Q,
Li X, Nagulapalli K, Sequist LV, Mak RH, Benes CH, et al: Radiation
resistance in KRAS-mutated lung cancer is enabled by Stem-like
properties mediated by an Osteopontin-EGFR pathway. Cancer Res.
77:2018–2028. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gurtner K, Kryzmien Z, Koi L, Wang M,
Benes CH, Hering S, Willers H, Baumann M and Krause M:
Radioresistance of KRAS/TP53-mutated lung cancer can be overcome by
radiation dose escalation or EGFR tyrosine kinase inhibition in
vivo. Int J Cancer. 147:472–477. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tanaka K, Hida T, Oya Y, Oguri T, Yoshida
T, Shimizu J, Horio Y, Hata A, Kaji R, Fujita S, et al: EGFR
mutation impact on definitive concurrent chemoradiation therapy for
inoperable stage III adenocarcinoma. J Thorac Oncol. 10:1720–1725.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lim YJ, Chang JH, Kim HJ, Keam B, Kim TM,
Kim DW, Paeng JC, Kang KW, Chung JK, Jeon YK, et al: Superior
treatment response and In-field tumor control in epidermal growth
factor Receptor-mutant genotype of stage III nonsquamous Non-small
cell lung cancer undergoing definitive concurrent
chemoradiotherapy. Clin Lung Cancer. 18:e169–e178. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sampath S, Rashdan S, Iyengar P, Mickel
TA, Zhang S, Ahn C, Gao A, Dowell JE, Zhang Y, Westover KD, et al:
Osimertinib plus consolidative radiotherapy for advanced EGFR
mutant non-small cell lung cancer: A multicentre, single-arm, phase
2 trial. EClinicalMedicine. 87:1034352025. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Binkley MS, Jeon YJ, Nesselbush M, Moding
EJ, Nabet BY, Almanza D, Kunder C, Stehr H, Yoo CH, Rhee S, et al:
KEAP1/NFE2L2 mutations predict lung cancer radiation resistance
that can be targeted by glutaminase inhibition. Cancer Discov.
10:1826–1841. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhang X, Huang X, Cao Y, Mao Y, Zhu Y,
Zhang Q, Zhang T, Chang L and Wang C: Dynamic analysis of
predictive biomarkers for radiation therapy efficacy in non-small
cell lung cancer patients by next-generation sequencing based on
blood specimens. Pathol Res Pract. 253:1549722024. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Su D, Ma S, Liu P, Jiang Z, Lv W, Zhang Y,
Deng Q, Smith S and Yu H: Genetic polymorphisms and treatment
response in advanced non-small cell lung cancer. Lung Cancer.
56:281–288. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bergamaschi D, Samuels Y, O'Neil NJ,
Trigiante G, Crook T, Hsieh JK, O'Connor DJ, Zhong S, Campargue I,
Tomlinson ML, et al: iASPP oncoprotein is a key inhibitor of p53
conserved from worm to human. Nat Genet. 33:162–167. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Jin JY, Wang W, Ten Haken RK, Chen J, Bi
N, Sadek R, Zhang H, Lawrence TS and Kong FM: Use a survival model
to correlate single-nucleotide polymorphisms of DNA repair genes
with radiation Dose-response in patients with non-small cell lung
cancer. Radiother Oncol. 117:77–82. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yin M, Yan J, Martinez-Balibrea E,
Graziano F, Lenz HJ, Kim HJ, Robert J, Im SA, Wang WS,
Etienne-Grimaldi MC and Wei Q: ERCC1 and ERCC2 Polymorphisms
predict clinical outcomes of Oxaliplatin-based chemotherapies in
gastric and colorectal cancer: A systemic review and Meta-analysis.
Clin Cancer Res. 17:1632–1640. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yang Z and Liu Z: Potential functional
variants in DNA repair genes are associated with efficacy and
toxicity of radiotherapy in patients with Non-Small-cell lung
cancer. J Oncol. 2020:31327862020. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Kelsey CR, Jackson L, Langdon S, Owzar K,
Hubbs J, Vujaskovic Z, Das S and Marks LB: A polymorphism within
the promoter of the TGFβ1 gene is associated with radiation
sensitivity using an objective radiologic endpoint. Int J Radiat
Oncol Biol Phys. 82:e247–e255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Xu T, Wei Q, Lopez Guerra JL, Wang LE, Liu
Z, Gomez D, O'Reilly M, Lin SH, Zhuang Y, Levy LB, et al: HSPB1
gene polymorphisms predict risk of mortality for US patients after
radio(chemo)therapy for non-small cell lung cancer. Int J Radiat
Oncol Biol Phys. 84:e229–e235. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Guo H, Bai Y, Xu P, Hu Z, Liu L, Wang F,
Jin G, Wang F, Deng Q, Tu Y, et al: Functional promoter-1271G>C
variant of HSPB1 predicts lung cancer risk and survival. J Clin
Oncol. 28:1928–1935. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Butkiewicz D, Krześniak M, Gdowicz-Kłosok
A, Giglok M, Marszałek-Zeńczak M and Suwiński R: Polymorphisms in
EGFR gene predict clinical outcome in unresectable Non-Small cell
lung cancer treated with radiotherapy and Platinum-Based
chemoradiotherapy. Int J Mol Sci. 22:56052021. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Milas L, Fan Z, Andratschke NH and Ang KK:
Epidermal growth factor receptor and tumor response to radiation:
In vivo preclinical studies. Int J Radiat Oncol Biol Phys.
58:966–971. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wen J, Liu H, Wang L, Wang X, Gu N, Liu Z,
Xu T, Gomez DR, Komaki R, Liao Z and Wei Q: Potentially Functional
variants of ATG16L2 predict radiation pneumonitis and outcomes in
patients with non-small cell lung cancer after definitive
radiotherapy. J Thorac Oncol. 13:660–675. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Torres-Roca JF, Eschrich S, Zhao H, Bloom
G, Sung J, McCarthy S, Cantor AB, Scuto A, Li C, Zhang S, et al:
Prediction of radiation sensitivity using a gene expression
classifier. Cancer Res. 65:7169–7176. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Peinado-Serrano J, Quintanal-Villalonga Á,
Muñoz-Galvan S, Verdugo-Sivianes EM, Mateos JC, Ortiz-Gordillo MJ
and Carnero A: A Six-gene prognostic and predictive
Radiotherapy-based signature for early and locally advanced stages
in Non-Small-Cell lung cancer. Cancers (Basel). 14:20542022.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Chen Y, Zhou C, Zhang X, Chen M, Wang M,
Zhang L and Chen Y, Huang L, Sun J, Wang D and Chen Y: Construction
of a novel radioresistance-related signature for prediction of
prognosis, immune microenvironment and anti-tumour drug sensitivity
in non-small cell lung cancer. Ann Med. 57:24479302025. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Pustovalova M, Malakhov P, Guryanova A,
Sorokin M, Suntsova M, Buzdin A, Osipov AN and Leonov S:
Transcriptome-based traits of radioresistant sublines of non-small
cell lung cancer cells. Int J Mol Sci. 24:30422023. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ma Q, Geng K, Xiao P and Zeng L:
Identification and prognostic value exploration of radiotherapy
Sensitivity-associated genes in Non-Small-Cell lung cancer. Biomed
Res Int. 2021:59638682021. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Zhao Y, Song Y, Zhao R, Zhao M and Huang
Q: Gene panel of persister cells as a prognostic indicator for
tumor repopulation after radiation. Front Oncol. 10:6077272020.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Gao J, Lu F, Yan J, Wang R, Xia Y, Wang L,
Li L, Chang L and Li W: The role of radiotherapy-related autophagy
genes in the prognosis and immune infiltration in lung
adenocarcinoma. Front Immunol. 13:9926262022. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Guo W-F, Lin R-X, Huang J, Zhou Z, Yang J,
Guo GZ and Wang SQ: Identification of differentially expressed
genes contributing to radioresistance in lung cancer cells using
microarray analysis. Radiat Res. 164:27–35. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Li Q, Shen L, Yang Y, Tai G, Zhu Q, Liu C,
Ge Q and Yi Q: Investigating the role of Lactate-related genes in
radiotherapy resistance of lung cancer by integrated bioinformatics
and experiment validation. J Cancer. 16:3296–3313. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Xu Q, Yu Z, Mei Q, Shi K, Shen J, Gao G,
Liu S and Li M: Keratin 6A (KRT6A) promotes radioresistance,
invasion, and metastasis in lung cancer via p53 signaling pathway.
Aging (Albany NY). 16:7060–7072. 2024.PubMed/NCBI
|
|
57
|
Diaz LA and Bardelli A: Liquid biopsies:
Genotyping circulating tumor DNA. J Clin Oncol. 32:579–586. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Perillo A, Olufemi MVA, De Robbio J,
Mancuso RM, Roscigno A, Tirozzi M and Scognamiglio IR: Liquid
biopsy in NSCLC: A new challenge in radiation therapy. Explor
Target Antitumor Ther. 2:156–173. 2021.PubMed/NCBI
|
|
59
|
Osumi H, Shinozaki E, Yamaguchi K and
Zembutsu H: Clinical utility of circulating tumor DNA for
colorectal cancer. Cancer Sci. 110:1148–1155. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Yun HS, Baek JH, Yim JH, Um HD, Park JK,
Song JY, Park IC, Kim JS, Lee SJ, Lee CW and Hwang SG: Radiotherapy
diagnostic biomarkers in radioresistant human H460 lung cancer
stem-like cells. Cancer Biol Ther. 17:208–218. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Nguyen GH, Murph MM and Chang JY: Cancer
stem cell radioresistance and enrichment: Where frontline radiation
therapy may fail in lung and esophageal cancers. Cancers (Basel).
3:1232–1252. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Afsar CU and Uysal P: HIF-1α Levels in
patients receiving chemoradiotherapy for locally advanced non-small
cell lung carcinoma. Rev Assoc Med Bras. 65:1295–1299. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zhang Y, Liu X, Zeng L, Zhao X, Chen Q,
Pan Y, Bai Y, Shao C and Zhang J: Exosomal protein
angiopoietin-like 4 mediated radioresistance of lung cancer by
inhibiting ferroptosis under hypoxic microenvironment. Br J Cancer.
127:1760–1772. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Ostheimer C, Gunther S, Bache M,
Vordermark D and Multhoff G: Dynamics of heat shock protein 70
serum levels as a predictor of clinical response in Non-Small-Cell
lung cancer and correlation with the Hypoxia-Related marker
osteopontin. Front Immunol. 8:13052017. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ostheimer C, Bache M, Güttler A, Kotzsch M
and Vordermark D: A pilot study on potential plasma hypoxia markers
in the radiotherapy of non-small cell lung cancer. Strahlenther
Onkol. 190:276–282. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Dehing-Oberije C, Aerts H, Yu S, De
Ruysscher D, Menheere P, Hilvo M, van der Weide H, Rao B and Lambin
P: Development and validation of a prognostic model using blood
biomarker information for prediction of survival of non-small-cell
lung cancer patients treated with combined chemotherapy and
radiation or radiotherapy alone (NCT00181519, NCT00573040, and
NCT00572325). Int J Radiat Oncol Biol Phys. 81:360–368. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Sui X, Jiang L, Teng H, Mi L, Li B, Shi A,
Yu R, Li D, Dong X, Yang D, et al: Prediction of clinical outcome
in locally advanced Non-Small cell lung cancer patients treated
with chemoradiotherapy by plasma markers. Front Oncol.
10:6259112021. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Li K, Wang S, Li N, Zhao W, He N, Wang J,
Ji K, Zhang M, Song H, Liu Q and Du L: Prognostic biomarkers after
radiotherapy for nonsmall cell lung cancer based on bioinformatics
analysis. Biomed Res Int. 2022:64052282022. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Yao G, Tang J, Yang X, Zhao Y, Zhou R,
Meng R, Zhang S, Dong X, Zhang T, Yang K, et al: Cyclin K interacts
with β-catenin to induce Cyclin D1 expression and facilitates
tumorigenesis and radioresistance in lung cancer. Theranostics.
10:11144–11158. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Cheng C, Pei X, Li SW, Yang J, Li C, Tang
J, Hu K, Huang G, Min WP and Sang Y: CRISPR/Cas9 library screening
uncovered methylated PKP2 as a critical driver of lung cancer
radioresistance by stabilizing β-catenin. Oncogene. 40:2842–2857.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Baek JH, Yun HS, Kwon GT, Lee J, Kim JY,
Jo Y, Cho JM, Lee CW, Song JY, Ahn J, et al: PLOD3 suppression
exerts an anti-tumor effect on human lung cancer cells by
modulating the PKC-delta signaling pathway. Cell Death Dis.
10:1562019. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Li J, Zong Y, Tuo Z and Liu J and Liu J:
The role of RASA2 in predicting radioresistance in lung cancer
through regulation of p53. Transl Lung Cancer Res. 13:587–602.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Chen Y, Zhou Y, Feng X, Wu Z, Yang Y, Rao
X, Zhou R, Meng R, Dong X, Xu S, et al: Targeting FBXO22 enhances
radiosensitivity in non-small cell lung cancer by inhibiting the
FOXM1/Rad51 axis. Cell Death Dis. 15:1042024. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Ji NN, Li SN, Shao L, Li Q, Xu JN and Zeng
YC: MDMX enhances radiosensitivity in lung adenocarcinoma and
squamous cell carcinoma by inhibiting P53-mediated autophagy. Cell
Oncol. 48:1067–1088. 2025. View Article : Google Scholar
|
|
75
|
Reno KE, Costa-Terryll A, Park SH, Hughes
RT, Farris MK, Xing F and Willey JS: Cartilage oligomeric matrix
protein promotes radiation resistance in non-small cell lung cancer
in vitro. Int J Mol Sci. 26:24652025. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Zhang R, Yan W, Yuan J, Ma Y, Ren Z, Chen
X, Lv J, Wu M, Yu J and Chen D: Cancer-associated
fibroblast-derived fibulin-5 promotes radioresistance in
non-small-cell lung cancer. Cell Rep. 44:1160182025. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Wang Y, Meng L, Meng S, Huang L, Luo S, Wu
X and Gong X: Flotillin-1 enhances radioresistance through reducing
radiation-induced DNA damage and promoting immune escape via STING
signaling pathway in non-small cell lung cancer. Cancer Biol Ther.
24:22033322023. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Alessi JV, Ricciuti B, Wang X, Pecci F, Di
Federico A, Lamberti G, Elkrief A, Rodig SJ, Lebow ES, Eicholz JE,
et al: Impact of TMB/PD-L1 expression and pneumonitis on
chemoradiation and durvalumab response in stage III NSCLC. Nat
Commun. 14:42382023. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Lei Z, He J, Yang H, Zhang L, Lai T, Zhou
L, Tang Z, Sui J and Wu Y: Global profiling of transcriptome,
proteome and 2-hydroxyisobutyrylome in radioresistant lung
adenocarcinoma cell. BMC Genomics. 25:9232024. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Delikgoz Soykut E, Kemal Y, Karacin C,
Karaoglanoglu O, Kurt M and Aytac Arslan S: Prognostic impact of
immune inflammation biomarkers in predicting survival and
radiosensitivity in patients with non-small-cell lung cancer
treated with chemoradiotherapy. J Med Imaging Radiat Oncol.
66:146–157. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Kim EH, Park AK, Dong SM, Ahn JH and Park
WY: Global analysis of CpG methylation reveals epigenetic control
of the radiosensitivity in lung cancer cell lines. Oncogene.
29:4725–4731. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Pernía O, Belda-Iniesta C, Pulido V,
Cortes-Sempere M, Rodriguez C, Vera O, Soto J, Jiménez J, Taus A,
Rojo F, et al: Methylation status of IGFBP-3 as a useful clinical
tool for deciding on a concomitant radiotherapy. Epigenetics.
9:1446–1453. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Koturbash I and Griffin RJ: Harnessing
epigenetics and metabolism to modulate tissue response to
radiotherapy. Int J Radiat Biol. 95:379–381. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Hammond SM: An overview of microRNAs. Adv
Drug Deliv Rev. 87:3–14. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Angerilli V, Galuppini F, Businello G, Dal
Santo L, Savarino E, Realdon S, Guzzardo V, Nicolè L, Lazzarin V,
Lonardi S, et al: MicroRNAs as predictive biomarkers of resistance
to targeted therapies in gastrointestinal tumors. Biomedicines.
9:3182021. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Salim H, Akbar NS, Zong D, Vaculova AH,
Lewensohn R, Moshfegh A, Viktorsson K and Zhivotovsky B: miRNA-214
modulates radiotherapy response of non-small cell lung cancer cells
through regulation of p38MAPK, apoptosis and senescence. Br J
Cancer. 107:1361–1373. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Yuan Y, Liao H, Pu Q, Ke X, Hu X, Ma Y,
Luo X, Jiang Q, Gong Y, Wu M, et al: miR-410 induces both
epithelial-mesenchymal transition and radioresistance through
activation of the PI3K/mTOR pathway in non-small cell lung cancer.
Signal Transduct Target Ther. 5:852020. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Lv J, An J, Zhang YD, Li ZX, Zhao GL, Gao
J, Hu WW, Chen HM, Li AM and Jiang QS: A three serum miRNA panel as
diagnostic biomarkers of radiotherapy-related metastasis in
non-small cell lung cancer. Oncol Lett. 20:2362020. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Chen X, Xu Y, Liao X, Liao R, Zhang L, Niu
K, Li T, Li D, Chen Z, Duan Y and Sun J: Plasma miRNAs in
predicting radiosensitivity in non-small cell lung cancer. Tumor
Biol. 37:11927–11936. 2016. View Article : Google Scholar
|
|
90
|
Chen X, Wu L, Li D, Xu Y, Zhang L, Niu K,
Kong R, Gu J, Xu Z, Chen Z and Sun J: Radiosensitizing effects of
miR-18a-5p on lung cancer stem-like cells via downregulating both
ATM and HIF-1α. Cancer Med. 7:3834–3847. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Zhang Y and Hu X: miR-148a promotes cell
sensitivity through downregulating SOS2 in radiation-resistant
non-small cell lung cancer cells. Oncol Lett. 23:1352022.
View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Han F, Huang D, Huang X, Wang W, Yang S
and Chen S: Exosomal microRNA-26b-5p down-regulates ATF2 to enhance
radiosensitivity of lung adenocarcinoma cells. J Cell Mol Med.
24:7730–7742. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Zhang Y and Xu H: Serum exosomal miR-378
upregulation is associated with poor prognosis in non-small-cell
lung cancer patients. J Clin Lab Anal. 34:e232372020. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Santosh B, Varshney A and Yadava PK:
Non-coding RNAs: Biological functions and applications. Cell
Biochem Funct. 33:14–22. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Fu W, Zhao J, Hu W, Dai L, Jiang Z, Zhong
S, Deng B, Huang Y, Wu W and Yin J: LINC01224/ZNF91 promote stem
cell-like properties and drive radioresistance in Non-small cell
lung cancer. Cancer Manag Res. 13:5671–5681. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Song J, Zhang S, Sun Y, Gu J, Ye Z, Sun X
and Tang Q: A Radioresponse-related lncRNA biomarker signature for
risk classification and prognosis prediction in non-small-cell lung
cancer. J Oncol. 2021:43388382021. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Wang Z, Liu L, Du Y, Mi Y and Wang L: The
HNF1A-AS1/miR-92a-3p axis affects the radiosensitivity of non-small
cell lung cancer by competitively regulating the JNK pathway. Cell
Biol Toxicol. 37:715–729. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Brownmiller T, Juric JA, Ivey AD, Harvey
BM, Westemeier ES, Winters MT, Stevens AM, Stanley AN, Hayes KE,
Sprowls SA, et al: Y chromosome LncRNA are involved in radiation
response of male Non-Small cell lung cancer cells. Cancer Res.
80:4046–4057. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Gu A, Li J, Li MY and Liu Y:
Patient-derived xenograft model in cancer: Establishment and
applications. MedComm. 6:e700592025. View Article : Google Scholar : PubMed/NCBI
|