Introduction
Metastatic disease remains the predominant
determinant of cancer-related mortality, and previous
population-based analyses indicate that bidirectional dissemination
of cancer cells between the lungs and urological organs is more
frequent than previously appreciated (1). A study by Deng et al (1) reported that, based on data from the
Surveillance, Epidemiology and End Results database (SEER)
(2), 18.4% of patients with de
novo metastatic prostate adenocarcinoma presented with
pulmonary involvement. In this analysis, bone represented the most
common metastatic site, whereas pulmonary involvement was
associated with a distinct prognostic disadvantage. This subset
exhibited a median overall survival (OS) that was 7.3 months
shorter than that of patients with bone-only disease, even after
adjustment for age and Gleason score. The Gleason scoring system is
the standardized histopathological grading system for prostate
adenocarcinoma, ranging from 6 to 10, with higher scores indicating
poorer differentiation and more aggressive disease (3). Comparable patterns of dissemination
have been documented for renal cell carcinoma (RCC); a study
reported by Wei et al (4)
investigated 47,555 RCC cases diagnosed between 2010 and 2018 and
reported that isolated lung-only metastases, defined as lung
involvement without concurrent metastases to other organs, were
detected in 22.1% of patients, whereas isolated visceral metastases
in the kidney, adrenal gland or bladder derived from primary lung
cancers constituted 4.6% of all lung-cancer deaths. These figures
underscore the necessity of considering the pulmonary-urological
axis as a clinically important yet underappreciated route of
metastatic spread. As detailed in Table I (1,4–6),
these epidemiological findings have revealed distinct prognostic
sub-features that complicate clinical management. For example,
patients aged <55 years paradoxically have poorer survival
outcomes of prostate-to-lung metastasis (1), whereas histological
dedifferentiation, as evidenced by the presence of sarcomatoid
features, completely abolishes therapeutic benefits in
renal-to-lung disease (4).
Notably, the concept of metastatic overlap within this axis is
clinically heterogeneous. In the present study, this term has been
defined to encompass three distinct scenarios: i) True cross-organ
metastasis; ii) multiple synchronous primary malignancies (7); and iii) the rare phenomenon of
tumor-to-tumor metastasis (8).
 | Table I.Epidemiological profile of metastatic
overlap between primary lung and urological cancers. |
Table I.
Epidemiological profile of metastatic
overlap between primary lung and urological cancers.
| First author,
year | Primary tumor | Metastatic
direction | Incidence among
m-stage patients | Key prognostic
sub-features | (Refs.) |
|---|
| Deng et al,
2019 | Prostate
adenocarcinoma | Lung | 18.4% | The patients aged
<55 years with prostate-to-lung metastasis were classified as
the ‘younger’ subgroup; this subgroup paradoxically exhibited
shorter overall survival compared with older patients, particularly
in the presence of non-bone co-metastasis. | (1) |
| Wei et al,
2021 | Clear-cell renal
cell carcinoma | Lung-only | 22.1% | Sarcomatoid
dedifferentiation abolishes therapeutic benefits. | (4) |
| Shiota et
al, 2025 | Primary NSCLC | Kidney | 4.6% of all
lung-cancer mortalities | Solitary renal
lesions are frequently misclassified as second primary tumors. | (5) |
| Furubayashi et
al, 2021 | Urothelial
carcinoma | Lung | 15.6% following
platinum-based chemotherapy failure | PD-L1 CPS≥10 almost
doubles ORR from 38 to 68%. | (6) |
Despite the epidemiological importance of this
metastatic overlap, accurate differentiation between the
aforementioned three scenarios, namely true cross-organ metastasis,
multiple synchronous primary malignancies and tumor-to-tumor
metastasis, at the pulmonary-urological anatomical interface
remains challenging. Conventional imaging techniques frequently
fail to discriminate between de novo pulmonary neoplasms and
urological metastases, which is particularly evident in cases
involving solitary lesions. In a multi-institutional series of 312
patients with clear-cell RCC (ccRCC) that developed lung nodules
after nephrectomy, 18% of cases were ultimately re-classified as
synchronous primary non-small cell lung cancer (NSCLC) following
targeted sequencing, leading to notable changes in the systemic
therapy strategies used, as treatment shifted from RCC-directed
regimens (e.g., vascular endothelial growth factor or mammalian
target of rapamycin inhibitors) to NSCLC-specific approaches (e.g.,
tyrosine kinase inhibitors or immune-checkpoint blockade) (7). Conversely, tumor-to-tumor metastasis
from prostate adenocarcinoma into an incumbent lung adenocarcinoma
has been documented, further blurring histogenic boundaries
(8). The resultant diagnostic
uncertainty of tumors along this axis translates into therapeutic
delays; data from SCRUM-Japan MONSTAR SCREEN project, a large-scale
cancer genomic screening initiative showed that the median duration
from radiological suspicion of tumor identity to tissue
confirmation was 42 days longer when urological and lung pathology
overlapped than when metastases occurred within the same organ
system (5). In this cohort,
isolated visceral metastases in the kidney derived from primary
NSCLC accounted for 4.6% of all lung-cancer deaths, and solitary
renal lesions in this setting were frequently misclassified as
second primary tumors, further complicating clinical
decision-making (5).
Molecular profiling has begun to clarify whether the
appearance of additional tumors along the lung-urological axis
represents genuine cross-organ colonization or the emergence of an
anatomically adjacent second primary. In a study reported by
Steindl et al (9),
whole-exome sequencing was performed on 28 primary RCC samples and
paired brain or lung metastases; the study observed a mean Jaccard
index value of 0.78 for shared mutations, indicating that
metastases were the result of monoclonal dissemination. Similar
clonality was observed in prostate cancer: In a study reported by
Shiota et al (5), ctDNA was
analyzed from 194 patients with castration-resistant prostate
cancer enrolled in the SCRUM-Japan MONSTAR SCREEN project. The
study found that the same androgen receptor (AR)-ligand
binding-domain alteration detected in primary tumors was present in
86% of concurrent pulmonary metastases, whereas this modification
was absent in 12 of 13 synchronous primary lung cancers identified
in the same cohort. These findings supported the concept of
molecular convergence, in which distinct primary tumors exploit
common signaling axes, such as the C-X-C chemokine receptor
(CXCR)4/C-X-C motif chemokine ligand (CXCL)12, hepatocyte growth
factor (HGF)/mesenchymal-epithelial transition factor (c-MET) and
tyrosine-protein kinase receptor UFO/growth arrest-specific protein
6 pathways, to establish pulmonary or urological sanctuary sites
(10,11).
The therapeutic implications of this molecular
overlap have been well-documented. A study reported by Furubayashi
et al (6) retrospectively
evaluated 92 patients with metastatic urothelial carcinoma who
received the immune-checkpoint inhibitor (ICI) pembrolizumab after
platinum failure; objective response rates (ORRs) in lung lesions
mirrored those in lymph-node sites, which were observed to be 38
and 35% respectively, whereas renal parenchymal lesions responded
to treatment in only 14% of cases. In this study, lung metastases
were present in 15.6% of patients following platinum-based
chemotherapy failure, and a programmed death-ligand 1 (PD-L1)
combined positive score (CPS) of ≥10 was associated with a marked
improvement in ORR, increasing from 38 to 68% in this subgroup
(6). These findings suggested that
the pulmonary microenvironment may be particularly amenable to
immune-checkpoint blockade. Conversely, targeted agents
conventionally restricted to NSCLC have shown notable activity in
urological metastases. Treatment with the MET inhibitor savolitinib
induced a partial response in 42% of pulmonary metastases arising
from papillary RCC in a single-arm phase II trial, a value that
parallels the 44% response rate observed in primary lung tumors
harboring MET exon 14 skipping alterations (12). Such findings exemplify the shift
from organ-centric to mechanism-centric therapy and highlight the
necessity for robust biomarkers that can reliably identify tumor
origin.
Emerging technologies have shown promise in
resolving this diagnostic bottleneck, namely the difficulty in
accurately distinguishing between primary lung neoplasms and
urological metastases when lesions present along the
pulmonary-urological axis. In a study reported by Wang et al
(13), a 10-CpG locus methylation
classifier was developed using ctDNA that distinguished pulmonary
metastases of RCC from primary NSCLC tumors with an area under the
curve (AUC) value of 0.92, outperforming the classical
transcription termination factor 1 (TTF-1)/paired box 8 (PAX8)
immunohistochemistry (IHC) panel (AUC, 0.79). Furthermore,
single-cell RNA sequencing has revealed metastatic
trajectory-specific signatures. CD103-positive cancer stem
cell-derived exosomes enriched in microRNA (miR)-19b-3p have been
shown to prime pulmonary endothelial cells for metastatic docking
in ccRCC, whereas miR-210-3p-enriched exosomes derived from
prostate cancer favored renal cortical colonization (13,14).
These approaches are orthogonal in that the 10-CpG methylation
classifier provides a diagnostic tool based on epigenetic DNA
modifications, whereas exosomal miRNA profiling offers mechanistic
insights into non-coding RNA-mediated metastatic signaling;
together, these orthogonal approaches not only refine current
insights into metastatic organotropism but also provide
non-invasive platforms for longitudinal monitoring.
In summary, epidemiological data have demonstrated
that bidirectional metastatic spread between the lungs and
urological organs is common and prognostically important, yet
recognition of this event is hampered by inherent diagnostic
ambiguity. Molecular evidence has indicated that metastasis of this
nature frequently represents genuine clonal dissemination driven by
shared genomic and epigenetic programs. Integrating these molecular
insights with evolving liquid-biopsy technologies offers a rational
framework for early detection, precise tumor identification and
mechanism-based therapies, which represents an imperative step
towards improving outcomes in this challenging clinical
scenario.
Hallmarks of metastasis: A shared toolkit
for dissemination
Irrespective of primary organ, metastatic
progression follows a stereotypical sequence: i) Local invasion;
ii) intravasation; iii) survival in circulation; iv) extravasation;
and v) secondary colonization. Accumulating evidence indicates that
lung and urological cancers exploit the same functional modules
during these steps (15–17). This implies that therapeutic
interception of the shared toolkit may confer cross-organ efficacy.
Table II (15–24)
juxtaposes the activity of specific molecular effectors, such as
profilin-2 in lung cancer and circPRRC2A in renal cancer, in
pulmonary and urological cancers to demonstrate how distinct
molecules achieve identical functional outcomes, such as vascular
permeability and immune evasion, across different tumor types.
| Table II.Shared metastatic toolkit in lung and
urological cancers. |
Table II.
Shared metastatic toolkit in lung and
urological cancers.
| Metastatic
step | Core mechanism | Examples in lung
cancer | Examples in
urological cancers | (Refs.) |
|---|
| Invasion and
EMT | Loss of epithelial
features, gain of motility and. invasiveness | α5-nAChR
overexpression triggers Jab1-mediated EMT, accelerating renal
colonization. | Androgen receptor
loss activates TGF-β1 signaling, driving EMT and pulmonary seeding
in castration-resistant prostate cancer. | (15,18) |
| Intravasation and
CTCs | Penetration of the
endothelial barrier to enter circulation. | Profilin-2-enriched
exosomes remodel the actin cytoskeleton, promoting intravasation
and bone-marrow dissemination. | circPRRC2A-loaded
exosomes downregulate TIMP2 and activate VEGFA/VEGFR2 signaling,
enhancing vascular permeability in ccRCC. | (16,19) |
| CTC survival | Evasion of shear
stress and immune surveillance in circulation. | Resveratrol
restores NK-cell cytotoxicity, diminishing CTC viability in a
melanoma lung-metastasis model. | Cathepsin K
blockade suppresses IL-17-mediated EMT and polarizes macrophages
from the M2 to M1 phenotype, reducing lung metastasis in prostate
cancer. | (17,20) |
| Extravasation | Exit from the
vasculature at the distant site. | Bevacizumab, an
anti-VEGF therapeutic agent, normalizes tight junctions,
attenuating brain extravasation. | Inhibition of
apelin/APJ signaling stabilizes tight junctions, reducing renal
cortex extravasation of prostate CTCs. | (21,22) |
| Colonization and
MET | Re-establishment of
epithelial features to proliferate and form metastases. | The PP4R1-HMGA2
interactionsustains ERK-dependent EMT, accelerating renal
metastasis; ERK inhibition restores the epithelial phenotype. | KLF5-mediated MET
enables prostate cancer cells to proliferate within pulmonary
alveoli after dissemination. | (23,24) |
Invasion and epithelial-mesenchymal
transition (EMT)
EMT constitutes a conserved molecular switch that
confers motility and proteolytic capacity (15). In prostate cancer, AR loss in
epithelial cells activates TGF-β1 signaling, leading to classical
E-cadherin downregulation and vimentin upregulation; this shift has
been shown to increase pulmonary seeding of metastases in
castration-resistant models (15).
Concordantly, NSCLC cells that overexpress neuronal acetylcholine
receptor α5 (α5-nAChR) have been shown to trigger Jun activation
domain-binding protein 1 (Jab1)-mediated EMT, accelerating renal
parenchymal colonization (18).
Although the upstream inducers differ (TGF-β1 in prostate cancer
vs. α5-nAChR/Jab1 in lung cancer), the downstream transcriptional
effectors converge on shared regulators of EMT, including TGF-β,
Jab1 and Snail (encoded by SNAI1), which operate in both directions
of the lung-urological axis.
Despite this convergence, transitional kinetics
differ. Prostate tumors display a gradual EMT trajectory that
permits micrometastatic dormancy within alveoli, whereas
EGFR-mutant lung adenocarcinoma has been shown to undergo a rapid,
complete transition, which facilitates immediate renal cortical
infiltration (25). Such temporal
heterogeneity is attributable to lineage-specific chromatin
landscapes (25), but the
downstream EMT effectors remain shared. Clinically, this dictates
that the timing of EMT-targeted therapies must be synchronized with
these distinct kinetic profiles; rapidly transitioning lung tumors
likely require upfront, concurrent blockade to prevent immediate
seeding, whereas the indolent chromatin states of prostate-derived
micrometastases may be more suitably managed via maintenance
strategies targeting epigenetic plasticity.
Intravasation and circulating tumor
cells (CTCs)
Once cancer cells acquire motility, they penetrate
the endothelial barrier. Small-cell lung cancer-derived exosomes
are enriched in profilin-2, which remodels the actin cytoskeleton
of recipient cancer cells, promoting intravasation and subsequent
bone marrow dissemination (19). A
parallel mechanism has been observed in ccRCC, in which
circPRRC2A-loaded exosomes increase vascular permeability by
downregulating tissue inhibitor of metalloproteinases 2 and
activating the vascular endothelial growth factor (VEGF)A/VEGF
receptor (VEGFR)2 axis (16). In
both studies, functional read-outs, including enhanced
trans-endothelial migration and increased circulating tumor cell
(CTC) counts, were observed, confirming a shared exosome-mediated
intravasation gateway (16,19).
Survival in circulation
CTCs are subject to both shear stress and immune
surveillance in circulation. In a melanoma lung-metastasis model,
resveratrol has been shown to diminish CTC viability by restoring
natural killer (NK)-cell cytotoxicity (20). Similarly, cathepsin K blockade in
castration-resistant prostate cancer has been found to suppress
IL-17-mediated EMT and reduce lung metastasis by polarizing M2
macrophages towards an M1 phenotype (17). Collectively, these findings imply
that immunomodulatory checkpoints, notably programmed death-ligand
1 (PD-L1), constitute a conserved ‘survival module’ for CTCs of
divergent origins.
Extravasation and endothelial
activation
Exit from the vasculature requires endothelial
activation. Bevacizumab-mediated VEGF blockade has been shown to
attenuate brain extravasation of lung cancer cells by normalizing
tight-junction architecture (21).
Similarly, inhibition of apelin/apelin receptor signaling has been
shown to reduce renal cortex extravasation of prostate CTCs through
the same junctional stabilization mechanism (22). Targeting VEGFs or their cognate
receptors therefore constitutes a cross-organ strategy for impeding
extravasation in the lung-urological metastatic route.
Colonization and reversible MET
Successful colonization hinges on tumor cells
re-establishing epithelial characteristics via MET. In lung
adenocarcinoma, the protein phosphatase 4 regulatory subunit 1-high
mobility group AT-hook protein 2 interaction has been shown to
sustain ERK-dependent EMT and accelerate renal parenchymal
metastasis; conversely, ERK inhibition restores the epithelial
phenotype and reduces colonization (23). Concordantly, prostate cancer cells
utilize Krüppel-like factor 5-mediated MET to proliferate within
pulmonary alveoli after initial dissemination (24). The reversibility of EMT has
therefore emerged as a shared attribute of metastatic colonization
along the lung-urological axis (26). However, the duration required for
MET to occur differs between tumor types, underscoring the need for
lineage-specific scheduling of EMT-targeting agents.
Molecular drivers of site-specific
tropism
Molecular determinants of metastatic site preference
between lung and urological cancers collectively involve the
TGF-β1/EMT, CXCR4/CXCL12, HGF/c-MET and CXCL8/CXCR2 signaling axes.
Notably, the CXCR4/CXCL12 and CXCL8/CXCR2 axes are predominantly
engaged in pulmonary tropism (from urological primaries to the
lung), whereas the HGF/c-MET and TGF-β1/EMT axes mediate
bidirectional signaling, collectively establishing site-specific
tropism through lineage-specific exosomal cargo and stromal
reprogramming (9,26). These reciprocal tropism pathways
represent potential therapeutic targets and have been graphically
summarized in Fig. 1. This figure
visually reconstructs the ‘seed and soil’ interaction, contrasting
the intrinsic ‘seed’ factors, such as CXCR4 upregulating and
miR-210 secretion, against the ‘soil’ priming mechanisms, for
example IL-30-mediated recruitment of myeloid-derived suppressor
cells (MDSCs) and fibronectin deposition. By mapping these
bidirectional signals, Fig. 1
illustrates how soluble factors and exosomes create a permissive
pre-metastatic niche long before macroscopic colonization
occurs.
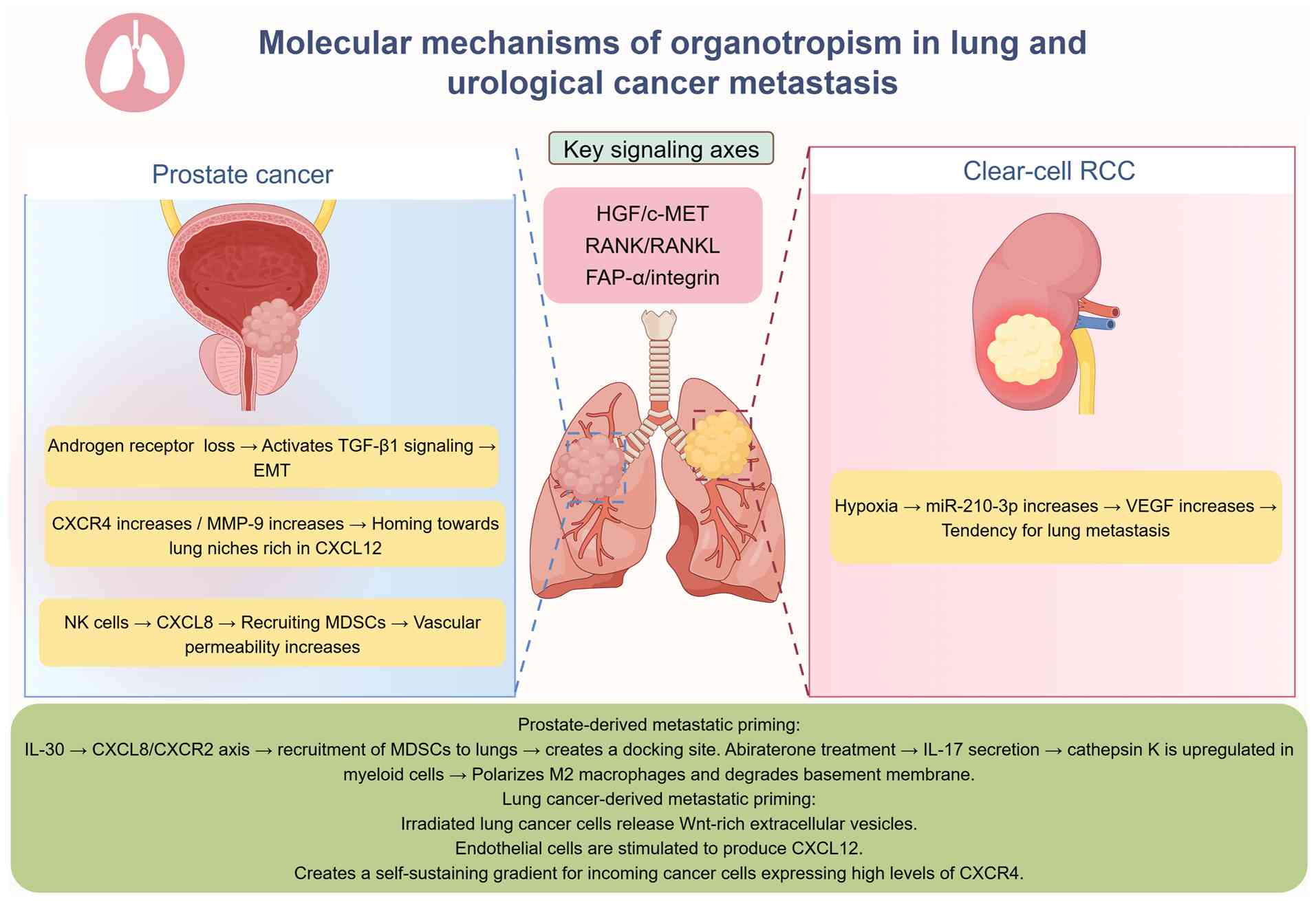 | Figure 1.Molecular drivers of site-specific
tropism in lung and urological metastases. EMT,
epithelial-mesenchymal transition; HGF, hepatocyte growth factor;
c-MET, mesenchymal-epithelial transition factor; RANK, receptor
activator of NF-κB; RANKL, receptor activator of NF-κB ligand;
FAP-α, fibroblast activation protein-α; CXCR, C-X-C chemokine
receptor; MMP-9, matrix metalloproteinase-9; CXCL, C-X-C motif
chemokine ligand; MDSC, myeloid-derived suppressor cell; NK,
natural killer; miR, microRNA; VEGF, vascular endothelial growth
factor. The figure was created with Figdraw (www.figdraw.com). |
‘Seeds’: Cancer-cell-intrinsic tropism
factors
Prostate cancer deficient in epithelial AR has been
shown to switch from an epithelial to a mesenchymal phenotype via
TGF-β1-driven EMT, concurrently upregulating CXCR4 and matrix
metalloproteinase (MMP)-9; the CXCR4/CXCL12 chemokine-receptor pair
guides circulating cells toward pulmonary niches rich in CXCL12 and
fibronectin, whereas MMP-9 contributes to extracellular matrix
remodeling during invasion (26).
Conversely, in NSCLC, CXCR4 upregulating facilitates tropism to the
kidney, where renal stromal cells produce CXCL12, creating a
permissive niche for metastatic seeding (9,26).
This bidirectional evidence establishes the CXCR4/CXCL12 axis as a
shared molecular mechanism governing cross-organ dissemination
along the lung-urological axis. Peripheral blood NK cells extracted
from the same patients have been shown to amplify CXCL8 secretion,
recruiting CD11b+ Gr1+ (Gr-1 is the myeloid
differentiation antigen, a classic surface marker for
myeloid-derived suppressor cells and granulocytes in mice) MDSCs
into alveolar septa and increasing vascular leakiness, therefore
providing an ideal docking platform for incoming CTCs (26). In ccRCC, hypoxic regions show an
upregulation of secreted miR-210-3p; serum levels of miR-210-3p
associate with VEGF concentration and independently predict future
pulmonary relapse (14). Thus,
both tumor types have been shown to utilize soluble factors, such
as CXCL8 or miR-210-3p, to pre-program the homing of CTCs to
pulmonary tissues, although the specific molecular cargo differs by
lineage: prostate cancer-derived NK cells secrete CXCL8 to recruit
MDSCs (26), whereas ccRCC-derived
exosomes deliver miR-210-3p to promote angiogenesis and create a
permissive pulmonary niche (14).
‘Soil’: Niche-priming by secreted
factors
Once primary tumors reach a critical mass,
pre-metastatic ‘soil’ tissues are primed. As aforementioned,
prostate cancer-derived IL-30 recruits CD11b+
Gr1+ MDSCs into alveolar septa via CXCL8/CXCR2 signaling
and increases microvascular permeability, creating a pulmonary
docking site for incoming CTCs (26). Abiraterone-treated prostate tumors
have been shown to secrete IL-17 that upregulates cathepsin K in
CD11b+ myeloid cells; cathepsin K in turn polarizes M2 macrophages
and degrades the alveolar basement membrane, doubling pulmonary
tumor burden in orthotopic mice (27). Conversely, irradiated lung cancer
cells secrete Wnt-enriched extracellular vesicles that stimulate
neighboring endothelial cells to produce CXCL12, thereby creating a
self-sustaining gradient for incoming prostate CTCs exhibiting
elevated levels of CXCR4 (28).
These findings indicate that bidirectional ‘soil’ preparation
relies on common effector classes, such as cytokines and
extracellular vesicles (EVs), even though upstream triggers are
tumor-type specific, for example androgen-deprivation (27) vs. radiotherapy (28).
Signaling axes governing cross-organ
tropism
Three signaling cascades repeatedly appear in both
tropism directions along the pulmonary-urological axis: i) The
HGF/c-MET pathway; ii) the receptor activator of NF-κB (RANK)/RANK
ligand (RANKL) signaling pathway; and iii) the fibroblast
activation protein (FAP)-α/integrin signaling pathway.
Functionally, these axes are not redundant with the primary
determinants (TGF-β1/EMT, CXCR4/CXCL12 and CXCL8/CXCR2) outlined in
the introductory paragraph of this section. Rather, the
CXCR4/CXCL12 and TGF-β1/EMT axes serve as the dominant drivers for
initial site-specific homing, whereas the HGF/c-MET, RANK/RANKL,
and fibroblast activation protein-α (FAP-α)/integrin pathways act
as secondary, context-dependent mechanisms that primarily
facilitate metastatic niche establishment, colonization, and
progression following initial seeding (29,30).
Regarding the HGF/c-MET axis, MET amplification in papillary RCC
has been shown to increase pulmonary colonization, whereas HGF
produced by pulmonary fibroblasts reciprocally stimulates c-MET on
NSCLC cells, accelerating renal parenchymal invasion (29). Similarly, osteoblast-derived RANKL
has been found to attract prostate cancer cells exhibiting high
levels of CXCR4 to bone tissue, whereas RANKL expressed by renal
tubular cells has been shown to foster pulmonary metastatic foci
(26). Finally, imaging with
[68Ga] DATA-conjugated fibroblast activation protein inhibitor
(Ga-DATA-FAPi) has shown that FAP-positive cancer-associated
fibroblasts (CAFs) are enriched in both lung and renal
pre-metastatic sites; pharmacological inhibition of FAP-α decreases
tumor cell adherence under flow conditions (30,31).
Convergence on these axes suggests that targeting stromal rather
than tumoral components may abrogate organotropism regardless of
primary tumor location.
However, previous evidence suggests that these axes
are not equipotent. Among the multiple signaling axes involved, the
CXCR4/CXCL12 axis functions as the predominant homing mechanism for
initial metastatic seeding, particularly in prostate-to-lung
dissemination, as constitutive high expression of CXCL12 in the
pulmonary vasculature universally attracts CXCR4-positive
circulating tumor cells (26).
Similarly, in lung-to-kidney dissemination, CXCR4-expressing NSCLC
cells home to CXCL12-abundant renal stroma, highlighting the shared
and reciprocal nature of this signaling axis (9,26).
By contrast, the HGF/c-MET pathway represents a more
context-dependent signaling mechanism, predominantly driving
colonization in specific histological subtypes, such as papillary
RCC, or acting as a secondary survival pathway that facilitates
progression rather than initial seeding (29). Other axes, including RANK/RANKL and
FAP-α/integrin signaling, contribute to niche priming and stromal
support but do not serve as primary homing switches (26,30,31).
Therapeutic exploitation of tropic
pathways
Cathepsin K inhibition using odanacatib has been
shown to curb IL-17-mediated M2 polarization and reduce pulmonary
tumor burden in castration-resistant prostate cancer (27). Furthermore, hypoxia-mimetic
19-hydroxybufalin downregulates hypoxia-inducible factor-1α
(HIF-1α), subsequently reducing miR-210-3p secretion and
attenuating ccRCC-induced angiogenesis (32); this implies that oxygen-sensing
modifiers may indirectly blunt lung homing.
Regarding the therapeutic utility of the
CXCR4/CXCL12 axis, clinical positron emission tomography (PET)
using Ga-pentixafor has demonstrated robust CXCR4 upregulation in
pulmonary lesions (33). This
imaging biomarker, reflecting CXCR4 expression levels, provides a
non-invasive method that may predict responsiveness to future
CXCR4-directed therapy in clinical trials targeting prostate cancer
or ccRCC. Treatment with a representative
quinolinoyl-cyanopyrrolidine inhibitor of FAP-α has been shown to
decrease tumor-cell adhesion under physiological flow, and its
combination with standard chemotherapy synergistically suppressed
tumor growth in lung-cancer xenografts (31,34).
Given that FAP-α is predominantly expressed on cancer-associated
fibroblasts in the tumor stroma, these findings suggest that
stromal targeting can override organ-specific ‘soil’ signals.
Finally, resveratrol restores NK-cell cytotoxicity
and suppresses melanoma lung metastasis by modulating sirtuin-1 and
oxidative stress levels (31,35);
since hypoxia-driven reactive oxygen species also govern
prostate-to-lung CTC trafficking (36), the repurposing of antioxidants as
adjuvants may attenuate tropism across the urological-pulmonary
axis. Collectively, these proof-of-concept studies support the
‘seed-and-soil’ paradigm and provide evidence that the processes
involved in this metastatic route represent notable therapeutic
targets, although combination treatments will be required to
counteract compensatory signaling and achieve durable blockade of
site-specific metastasis.
Tumor microenvironment (TME) and immune
contexture at the metastatic site
Metastatic seeding in the lung does not involve the
passive lodging of tumor cells but rather the active remodeling of
the TME, which is orchestrated by CAFs and tumor-associated
macrophages (TAMs) that collectively construct an immune-privileged
niche. Periostin (POSTN)+ and MMP-11+ CAFs
drive collagen cross-linking and T-cell exclusion, whereas
hypoxia-educated M2-like TAMs (i.e., TAMs that acquire an
immunosuppressive phenotype upon activation by hypoxic conditions)
reinforce immunosuppression; the spatial interplay of these cells
has been summarized in Fig. 2.
This figure highlights the immune-exclusion phenotype
(characterized by CD8+ T cells confined to the invasive margins
rather than infiltrating the tumor core) characteristic of these
metastases, showing how the physical barrier formed by activated
CAFs and the functional immune-suppression induced by M2-TAMs
collectively prevent CD8+ T-cell infiltration into the
tumor core, thereby limiting the efficacy of monotherapy.
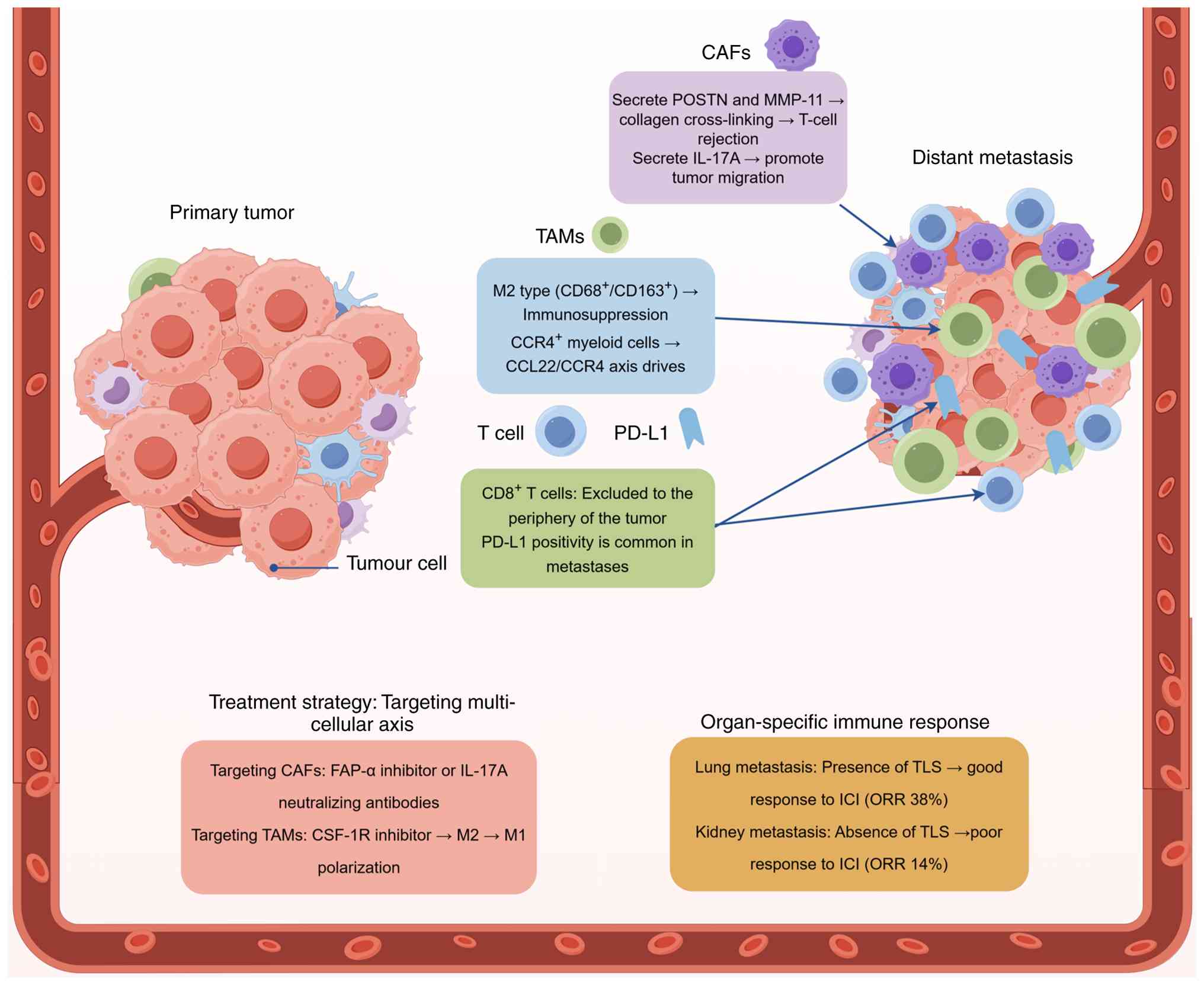 | Figure 2.Tumor microenvironment and immune
contexture at the metastatic site. CAF, cancer-associated
fibroblast; TAM, tumor-associated macrophage; PD-L1, programmed
death-ligand 1; FAP-α, fibroblast activation protein-α; CSF-1R,
macrophage colony-stimulating factor 1 receptor; TLS, tertiary
lymphoid structure; ICI, immune-checkpoint inhibitor; ORR,
objective response rate; POSTN, periostin; MMP, matrix
metalloproteinase; CCR4, C-C chemokine receptor type 4; CCL22, C-C
motif chemokine ligand 22. The figure was created with Figdraw
(www.figdraw.com). |
Cellular architects of the metastatic
niche: CAFs and TAMs
The cellular composition of the metastatic niche is
predominantly shaped by CAFs and TAMs. CAFs positive for markers
such as α-SMA constitute a notable portion of the stromal area in
pulmonary metastases, varying from 25–40%, a frequency comparable
with their primary tumors (9).
Functionally, these CAFs are not inert, but rather actively promote
malignancy. In ccRCC, a subset of CAFs expressing POSTN and MMP-11
has been demonstrated to contribute to collagen cross-linking and
T-cell exclusion, creating a physical and biochemical barrier
against immune attack (13). This
pro-invasive effect, which can inhibitors targeting FAP-α, a key
enzyme expressed on CAFs, validates CAFs as a druggable stromal
component across tumor types (37). In prostate cancer, CAFs have been
shown to promote malignant progression through autophagy induction
and the secretion of pro-inflammatory cytokines, such as IL-17A,
which augment the migratory and invasive capabilities of tumor
cells (37,38).
Concurrently, TAMs exhibit a distinct phenotypic
polarization within lung metastases. In ccRCC pulmonary metastases,
CD68/CD163 double-positive M2-like TAMs have been shown to densely
infiltrate the tumor, often co-localizing with hypoxic niches
marked by HIF-1α, and their presence has been linked to poor
prognosis (9,39). By contrast, pulmonary metastases
derived from prostate cancer have shown a notable enrichment of C-C
chemokine receptor type 4 (CCR4)-positive myeloid cells, a
recruitment pattern driven by the C-C motif chemokine ligand
22/CCR4 axis, which mirrors mechanisms observed in primary prostate
tumors (40,41). The notable role of TAMs in
fostering an immunosuppressive TME is underscored by intervention
studies; depletion of TAMs using macrophage colony-stimulating
factor 1 receptor (CSF-1R) inhibitors has been shown to repolarize
remaining macrophages towards an antitumor M1 phenotype. This shift
synergizes with agents such as sunitinib, leading to prolonged
overall survival in preclinical models. As such, these findings
highlight the central role of TAMs in fostering an
immunosuppressive TME (39,42).
Immune checkpoints and spatial control
of the T-cell response
The immune topography of metastases is characterized
by the spatial segregation of cytotoxic lymphocytes.
CD8+ T cells are largely excluded from the tumor islets
and confined to the invasive margins in a majority of pulmonary
metastases (6,9,43).
This exclusion pattern is associated with high expression levels of
immune checkpoint ligands on the surrounding stromal cells,
including CAFs and TAMs, rather than on the tumor cells
themselves.
Among immune-evasion checkpoints, the programmed
cell death protein 1 (PD-1)/PD-L1 axis remains the most extensively
characterized. PD-L1 positivity has been detected in a notable
proportion of pulmonary metastases derived from urological cancers,
with observed frequencies aligning with their primary tumors
(6,9). Notably, responses to
immune-checkpoint blockade appear to be organ-specific.
Pembrolizumab monotherapy has demonstrated a higher ORR in lung
metastases derived from urothelial carcinoma at 38% compared with
renal parenchymal lesions at 14%, implying that the pulmonary
microenvironment may be intrinsically more permissive to
T-cell-mediated cytotoxicity following checkpoint inhibition
(6). Further analyses have
revealed that lesions that respond to pembrolizumab often harbor
tertiary lymphoid structures (TLSs), which are defined as organized
clusters of immune cells in non-lymphoid tissues that serve as
sites for local adaptive immune responses, and proliferating
proliferation marker protein Ki-67+ (Ki-67+)
PD-1+ CD8 T cells; however, non-responding lesions are
characterized by an IL-30+ macrophage signature, which
can be therapeutically targeted (6,10).
In addition to the PD-1/PD-L1 axis, other immune
checkpoints, such as lymphocyte activation gene 3 protein (LAG-3)
and T-cell immunoreceptor with Ig and ITIM domains (TIGIT),
contribute to T-cell exhaustion. LAG-3 expression has been detected
in tumor-infiltrating CD4+ T cells in metastatic
prostate cancer models (44).
Fibrinogen-like protein 1 (FGL1), which is secreted by CAFs, has
been identified as a major ligand for TIGIT in ccRCC and may
contribute to TIGIT-mediated immune suppression (45). Preclinical evidence supports
targeting these immune checkpoints; antibody-mediated
neutralization of TIGIT has been shown to restore NK cell-mediated
cytotoxicity and reduce pulmonary tumor burden, indicating the
therapeutic potential of this strategy (46).
Therapeutic implications: Targeting
the multicellular axis of the metastatic niche
The mechanistic interconnections between CAFs, TAMs
and immune cells form a cycle of immune suppression within the
established metastatic niche. This multicellular axis presents a
compelling therapeutic opportunity to dismantle the
tumor-supportive ecosystem rather than solely targeting the cancer
cells themselves. The efficacy of this approach is predicated on
simultaneously disrupting the pro-tumorigenic functions of multiple
stromal components.
The targeting of CAFs has emerged as a viable
strategy of compromising the structural integrity of the metastatic
niche. Pharmacological inhibition of FAP-α, a key enzyme expressed
by CAFs, has been shown to abrogate the pro-invasive effects of
CAF-conditioned media (culture medium containing secreted factors
from cancer-associated fibroblasts) on cancer cells, supporting
FAP-α as a druggable target (37).
CAF plasticity, defined as the capacity of CAFs to switch between
pro-tumorigenic and anti-tumorigenic phenotypes as previously
discussed in this section, suggests that targeting a single
CAF-associated molecule may be insufficient. Therefore, the
combination of FAP-targeted therapies with agents that block
CAF-derived immunosuppressive cytokines represents a rational
strategy to overcome phenotypic adaptation and prevent T-cell
exclusion from the TME (31).
Furthermore, neutralizing CAF-derived cytokines, such as IL-17A,
has been shown to inhibit the pro-migratory signals that facilitate
cancer-cell dissemination and tumoral niche maintenance (38).
Concurrently, reprogramming of the immune contexture
by targeting TAMs has been shown to reverse immunosuppression.
Therapeutic targeting of M2-like TAMs using CSF-1R inhibitors has
been demonstrated to not only reduce the direct immunosuppressive
influence of TAMs but also repolarize the macrophage population
towards an immunostimulatory M1 phenotype (39,42).
This shift has been demonstrated to synergize with anti-angiogenic
agents, such as sunitinib, which can normalize the tumor
vasculature by reversing abnormal vascular hyperpermeability and
disorganized architecture that facilitate both tumor cell
intravasation and extravasation, thereby improving T-cell
infiltration and creating a more favorable microenvironment for
immune attack (39,43).
Emerging clinical efforts are now formally testing
the paradigm of stromal-immune axis disruption. These
next-generation approaches refer to combination strategies designed
to simultaneously target multiple cellular components of the TME,
including CAFs and TAMs, to dismantle the physical and
immunological barriers that protect metastatic lesions.
Representative examples include trials combining CSF-1R inhibitors
with PD-1/LAG-3 blockade, such as trial NCT05577182, or
FAP-α-targeted radioligands with IL-2, e.g. trial NCT06640413,
which exemplify rational, next-generation approaches aimed at
converting the pulmonary metastatic site from an immune sanctuary
into a vulnerable target. Notably, the data from these ongoing
trials remain preliminary, and their clinical utility requires
future confirmation through expanded cohorts and validation in
independent studies. The goal of these combinations is to dismantle
the physical and biochemical barriers erected by the TME, thereby
converting the pulmonary metastatic site from an immune sanctuary
into a vulnerable target. This strategy, focused on targeting the
‘soil’ rather than just the ‘seed’, holds notable promise for
improving outcomes in patients with metastatic disease spanning the
lung-urological axis. However, the clinical translation of these
microenvironmental insights is fundamentally predicated upon the
accurate identification of the origin of tumors. As the molecular
crosstalk and shared features of the TME in pulmonary and
urological cancers frequently blur histological boundaries,
distinguishing between primary lung neoplasms and urological
metastases remains a notable clinical challenge. This challenge
constitutes the first notable bottleneck in treating patients with
pulmonary and urological cancer, necessitating the use of advanced
diagnostic frameworks.
Diagnostic dilemmas and the path to
precision
While molecular drivers and microenvironmental
niches orchestrate the metastatic process, their clinical
manifestation often presents as an ambiguous diagnostic landscape.
Consequently, the management of metastatic cancer at the
lung-urological interface is frequently complicated by notable
diagnostic uncertainty. Accurately distinguishing a metastasis from
a second primary tumor is not only an academic exercise but
important in determining therapeutic strategies and prognosis. This
section explores the clinical challenges and evolving role of
advanced diagnostic modalities in identifying metastatic disease
status, as well as the integrated approach required for precision
medicine along the pulmonary-urological axis (Table III) (5,47–54).
| Table III.Diagnostic approach to metastatic
tumors of uncertain origin at the lung-urological interface. |
Table III.
Diagnostic approach to metastatic
tumors of uncertain origin at the lung-urological interface.
| Clinical
scenario | Recommended
diagnostic algorithm | Key
immunohistochemical markers | Value of molecular
profiling or liquid biopsy | (Refs.) |
|---|
| Solitary pulmonary
nodule in a patient with a history of RCC or prostate cancer |
Clinical-radiological correlation followed
by IHC, in turn followed by NGS if results are inconclusive. | For RCC metastasis
vs. lung primary tumors: PAX8 positive and TTF-1 negative. For
prostate metastasis vs. lung primary tumors: PSA/P501S positive and
TTF-1 negative. | Confirms clonal
origin; distinguishes metastasis from second primary. | (5,47,48) |
| Solitary renal
lesion in a patient with a history of primary lung cancer |
Clinical-radiological correlation followed
by IHC, in turn followed by NGS if results are inconclusive. | For lung primary
metastasis: TTF-1 positive and PAX8 negative. For challenging
cases, including those with urothelial-like features or
tumor-to-tumor metastasis, an extended panel incor-porating CK7,
CK20 or GATA3 may be required to resolve diagnostic ambiguity. | Identifies
lineage-specific drivers; guides targeted therapy selection. | (47,49,50) |
| Poorly
differentiated or rare tumor types, such as RCC with TFE3 gene
fusions and urothelial-like prostate cancer | Comprehensive IHC
followed by confirmatory genetic testing via FISH or NGS. | For RCC with TFE3
gene fusions: TFE3 shows strong nuclear positivity. Challenging
cases may require extended panels, for example using IHC to detect
CK7, CK20 or GATA3, to resolve ambiguity. | Definitive
diagnosis via pathognomonic alterations. | (5,49,50) |
| Monitoring disease
evolution and assessing tumor heterogeneity | Integration of
radiological surveillance (e.g., computed tomography) and serial
liquid biopsy via ctDNA analysis, as discussed in Section 5. | IHC is not the
primary tool for dynamic monitoring | Tracks clonal
evolution in real-time; assesses metastatic heterogeneity. | (52–54) |
Clinician's challenge: Distinguishing
a metastasis from a second primary tumor
The initial clinical dilemma involved in
distinguishing second primary tumors from metastases often arises
from non-specific radiological findings. Solitary pulmonary nodules
in a patient with a history of RCC or prostate cancer can represent
either a metastatic deposit or a new primary lung adenocarcinoma.
Conventional imaging modalities, such as computed tomography (CT),
frequently lack the specificity required to differentiate between
these entities, leading to diagnostic inertia and potential delays
in initiating appropriate therapy. This challenge has been
underscored by the results of clinicopathological analyses, which
have revealed that a notable number of tumors at the pulmonary
interface have been initially misclassified. For instance, a study
has shown that solitary renal lesions in the context of a known
lung primary tumor can be mistakenly diagnosed as second primaries,
complicating cancer stage classification and treatment planning
(47). The issue of tumor
misclassification is further compounded by rare phenomena, such as
tumor-to-tumor metastasis, and the existence of aggressive
morphological variants, such as prostatic adenocarcinomas with
urothelial-like features, which can blur histological boundaries
and confound initial diagnostic efforts (49). Consequently, diagnostic reliance on
patient clinical history and standard imaging alone is
insufficient, necessitating the development of more sophisticated
diagnostic algorithms.
Evolving role of pathology and
molecular profiling
To resolve this diagnostic impasse, pathology has
moved beyond traditional histology to incorporate sophisticated
immunohistochemical panels and next-generation sequencing (NGS).
IHC serves as the primary method for determining the tumoral tissue
of origin (48). A panel including
markers such as: i) PAX8 for detecting RCC; ii) TTF-1 for detecting
lung adenocarcinoma; iii) GATA binding protein 3 to detect
urothelial carcinoma; and iv) puromycin-sensitive
aminopeptidase/P501S (prostein, a prostate-specific marker encoded
by the SLC45A3 gene) for prostate cancer can provide decisive
evidence in a number of cases (48). However, IHC has its limitations,
particularly in poorly differentiated or rare tumor types. For
example, RCCs exhibiting Xp11.2 translocation and transcription
factor E3 gene fusions exhibit a unique diagnostic profile that
requires specific genetic or immunohistochemical confirmation
beyond standard IHC markers (51).
Similarly, the expression of cytokeratin (CK)7 and CK20 in some
prostate cancers can mimic urothelial carcinoma, which highlights
the potential for diagnostic misinterpretations using IHC and the
need for a comprehensive marker panel (49).
In cases where IHC yields ambiguous or contradictory
results, molecular profiling has emerged as a powerful adjunct. NGS
can identify the lineage of a tumor by revealing pathognomonic
genetic alterations (5). The
analysis of metastatic patterns using ctDNA has proven particularly
insightful. In a landmark study reported by Shiota et al
(5), analysis of ctDNA from
patients with castration-resistant prostate cancer demonstrated
that the same AR-ligand binding-domain alteration present in the
primary tumor was detectable in the majority of concurrent
pulmonary metastases, whereas this modification was absent in
synchronous primary lung cancers identified within the same cohort.
This finding underscores the high specificity of clonal relatedness
for confirming metastatic spread. Furthermore, NGS has revealed the
genomic heterogeneity of metastases; for example, visceral
metastases derived from prostate cancer often exhibit a distinct
genomic landscape compared with bone metastases, with an enrichment
of alterations in genes such as tumor protein p53 (TP53) and
retinoblastoma-associated protein (RB1), as well as AR
amplifications (52). This
heterogeneity not only aids diagnosis, but also has profound
implications for selecting targeted therapies; for example, the
identification of specific MET mutations in papillary RCC may
predict therapeutic responses to cabozantinib (50). The convergence of IHC and NGS thus
provides a multi-modal diagnostic pathway, in which IHC offers a
rapid, cost-effective method of initial tumor classification and
NGS delivers definitive genomic evidence for challenging cases to
guide therapeutic decision-making.
Promise of liquid biopsy and
integrated diagnostic pathways
The advent of liquid biopsy represents a paradigm
shift towards non-invasive, dynamic disease monitoring. Liquid
biopsy is a non-invasive diagnostic modality that comprises the
analysis of non-solid biological tissues, primarily blood, to
detect tumor-derived genetic material, primarily through the
analysis of ctDNA (55). A study
reported by Esposito et al (55) demonstrated that monitoring
tumor-derived cell-free DNA enables the non-invasive detection of
genetic alterations in metastatic disease, offering clinical
utility in early assessment of treatment response, real-time
tracking of clonal evolution, and identification of resistance
mechanisms without the need for repeat tissue biopsies. This
promise has been cause for investigation, as ctDNA analysis allows
for the genomic characterization of metastatic disease without the
need for invasive tissue biopsy, which is particularly valuable in
cases involving lesions that are difficult to access (53). For example, genomic amplifications
identified in ctDNA, such as AR amplifications in metastatic
castration-resistant prostate cancer (mCRPC), have provided both
diagnostic confirmation of metastatic spread and important
prognostic information (54).
Despite its promise as a diagnostic modality, the
detection and molecular characterization of both CTCs and ctDNA has
presented technical challenges in the clinical setting, including
issues related to sensitivity and standardization (53). Notably, the clinical utility of
liquid biopsy is severely constrained in low tumor-burden settings.
In scenarios involving solitary pulmonary nodules or early
oligometastatic renal recurrences, the shedding of tumor DNA into
the circulation is often insufficient to surpass the limit of
detection of standard NGS assays. Consequently, a negative liquid
biopsy result does not definitively exclude metastatic disease due
to the risk of false negatives, necessitating a return to tissue
sampling or close radiological surveillance in these indeterminate
cases (53).
However, when successfully implemented, liquid
biopsies can identify actionable alterations in tumor genomes and
track clonal evolution in real time. This is especially relevant
for predicting sites of metastasis; specific genomic signatures
detected in ctDNA have been investigated as biomarkers for
predicting the propensity of prostate cancer to metastasize to
specific sites, such as bone or viscera (56). The integration of these biomarkers
with traditional tissue-based diagnostics creates a powerful,
complementary framework for accurate cancer diagnosis. This
multi-step strategy aligns with contemporary diagnostic paradigms
that advocate for the systematic integration of clinical,
histopathological and molecular data to resolve diagnostic
uncertainty in tumors of uncertain origin (48). This multi-step process ensures that
patients receive a precise pathological assignment, following the
recommended diagnostic algorithm outlined in Table III. As shown in Table III, this algorithm prioritizes
the hierarchical application of IHC panels, for example PAX8 vs.
TTF-1, to resolve common diagnostic ambiguities, whereas advanced
molecular profiling is reserved for complex scenarios, such as
solitary lesions with atypical morphology.
Therapeutic implications and the era of
agnostic oncology
Building upon the aforementioned findings regarding
the precise diagnostic stratification and elucidation of shared
molecular drivers and immune contextures, the therapeutic landscape
has been undergoing a notable transformation. The traditional
paradigm of organ-specific therapy has been increasingly challenged
by molecular evidence demonstrating that metastatic tumors derived
from different primary tumors may share actionable genomic
alterations (27,56,57).
This convergence has catalyzed the emergence of agnostic oncology,
which is also known as tissue-agnostic or tumor-agnostic therapy
(27,57). This paradigm involves a shift in
clinical decision-making, so that treatment is administered based
on the presence of specific genomic alterations or molecular
signatures, for example microsatellite instability-high (MSI-H)
signatures, regardless of the histological origin or anatomical
location of the tumor. In the specific context of lung-urological
metastatic overlap, three therapeutic strategies exemplify this
shift: i) Tissue-agnostic approval of ICIs for MSI-H or
mismatch-repair deficient (dMMR) tumors; ii) targeted inhibition of
shared oncogenic drivers, such as neurotrophic receptor tyrosine
kinase fusions, MET exon 14 skipping or DNA-repair
defects; and iii) targeting organ-specific differential responses
to the same agent. These three strategies are outlined in Table IV (6,57–66),
providing a structured framework for selecting the most appropriate
mechanism-centric intervention based on the specific molecular
profile of tumors.
| Table IV.Therapeutic paradigms in the
lung-urological metastatic axis. |
Table IV.
Therapeutic paradigms in the
lung-urological metastatic axis.
| Therapeutic
domain | Molecular target or
biomarker | Key agents | Evidence in the
lung-urological axis | (Refs.) |
|---|
| Tissue-agnostic
therapy | MSI-H or dMMR; NTRK
fusions | Pembrolizumab and
larotrectinib | Comparable MSI-H
prevalence in lung and urothelial cancer metastases; efficacy of
larotrectinib in prostate cancer pulmonary metastasis. | (58,59) |
| Shared oncogenic
drivers | MET exon 14
skipping | Savolitinib | Similar response
rates in papillary RCC with lung metastases and primary NSCLC
harboring MET alterations. | (60) |
| Shared DNA-repair
defects | HRD, for example
BRCA or ATM | Talazoparib;
talazoparib + avelumab | High response in
lung lesions of mCRPC; activity in MSI-H- or ATM-deficient
urothelial carcinoma with lung metastases. | (61,62) |
| Organ-specific
efficacy of ICIs (combination) | PD-1/PD-L1 | Nivolumab +
ipilimumab | Cases of pulmonary
remission with concurrent bone progression in RCC. | (63) |
| Organ-specific
efficacy of ICIs (combination) | PD-1/PD-L1 | Pembrolizumab;
nivolumab | Higher ORR in lung
vs. renal parenchymal metastases from UC. | (6,64) |
| Complex predictive
biomarkers | TMB; tryptophan
catabolism | N/A | Differential
predictive power of TMB cut-offs in lung vs. urothelial cancers;
association of elevated IDO activity with lung-targeted
immunotherapy resistance. | (57,65,66) |
From organ-centric to
mechanism-centric therapy
Pembrolizumab was the first drug to receive
tumor-agnostic approval by the Food and Drug Administration for use
in targeting MSI-H or dMMR tumors (58). A 2023 real-world study of 3,112
ctDNA profiles revealed that MSI-H prevalence is comparable across
pulmonary metastases of urothelial carcinoma and primary lung
adenocarcinoma, which display prevalence rates of 6.8 and 5.9%
respectively, supporting the cross-organ applicability of
pembrolizumab in this molecular subset of tumors (58). Similarly, neurotrophic receptor
tyrosine kinase (NTRK) fusion basket trials demonstrated an ORR
>75% for larotrectinib regardless of primary tumor site; one of
the 55 patients included in the study had a pulmonary metastasis
from prostate cancer that achieved complete remission lasting 18
months (59). These findings
validate the biological principle that a single type of genomic
alteration can dominate metastatic behavior irrespective of organ
ancestry.
Shared drivers in the lung-urological
axis: MET, poly (ADP-ribose) polymerase (PARP) and beyond
MET exon 14 skipping occurs in 3–4% of
patients with NSCLC and in ≤2% of papillary RCC. Savolitinib, a
selective MET inhibitor, produced a 42% partial-response rate among
26 patients with papillary RCC and lung-dominant metastatic disease
(60), mirroring the 44% ORR
reported in patients with NSCLC harboring the same alteration. This
comparable efficacy across distinct tumor types harboring the same
molecular alteration supports true clonal sensitivity rather than
organ-specific pharmacokinetic activity.
PARP inhibition represents another mechanism-centric
therapeutic strategy. In the TALAPRO-1 trial (ClinicalTrials.gov
identifier: NCT03148795), talazoparib monotherapy yielded a 46% ORR
in mCRPC that exhibited DNA-repair defects; notably, targeted lung
lesions shrank in 9 of 11 cases, whereas bone lesions responded in
only 18%, suggesting organ-specific modulation of drug efficacy
(61). The subsequent JAVELIN PARP
Medley trial (ClinicalTrials.gov identifier: NCT03330405) extended
this concept to solid non-prostate tumors: Administration of
avelumab combined with talazoparib achieved a 30% ORR in MSI-H or
ataxia telangiectasia mutated (ATM)-deficient tumors, including in
2 patients with urothelial carcinoma that exhibited lung metastases
that had progressed after platinum-based chemotherapy (62). Collectively, these observations
indicated that homologous recombination deficiency (HRD), including
deficiency in ATM and other DNA repair genes, is a trans-organ
predictive biomarker of therapeutic efficacy, but that the
metastatic-site microenvironment may still influence the depth and
durability of therapeutic responses.
ICIs: Organ-specific efficacy within
an agnostic frame
Despite the agnostic approval of pembrolizumab for
MSI-H tumors, organ-specific response patterns have been
increasingly reported. A study by Furubayashi et al
(6) retrospectively compared
pulmonary vs. renal-parenchymal lesions in 92 patients with
urothelial carcinoma receiving pembrolizumab after platinum failure
who were not preselected based on microsatellite instability-high
(MSI-H) status (i.e., an all-comer population); the ORR of lung
metastases was 38%, which was identical to lymph-node disease,
whereas the ORR of renal parenchymal metastases was only 14%.
Multiplex immunofluorescence revealed that responding lung lesions
were enriched in TLSs and Ki-67+ PD-1+
CD8+ T cells, whereas non-responding renal lesions
harbored an IL-30+ macrophage signature, implying that
myeloid exclusion networks may counteract T-cell reinvigoration in
specific metastatic niches (6).
These findings are consistent with case-level
observations in RCC; two independent reports have documented
complete pulmonary remission following nivolumab monotherapy or
combination treatments with nivolumab and ipilimumab, whereas
concurrent bone lesions progressed (6,63).
Conversely, hyperprogression in pulmonary metastases has also been
described following treatment with ICIs. A 2021 case report
highlighted the notable growth of lung lesions in a patient with
metastatic RCC receiving radiotherapy and anti-PD-1 therapy;
however, extra-pulmonary metastatic sites remained stable,
underscoring the dual capacity of the pulmonary microenvironment to
either amplify or attenuate ICI activity (64). However, caution is warranted in
attributing these response patterns solely to microenvironmental
distinctiveness. Confounding variables, including the
immunosuppressive sequelae of prior systemic therapies and the
inherent genomic heterogeneity of metastatic subclones, may also
contribute to these site-dependent discrepancies in treatment
efficacy, as evidenced by the distinct mutational landscapes
observed between visceral and bone metastases (52).
Biomarker complexity: Tumor mutational
burden (TMB), PD-L1 and beyond
TMB has gained traction as a pan-cancer biomarker,
yet threshold validity values differ between pulmonary and
urological metastases. A study reported by Passaro et al
(65) noted that a TMB≥10
mutations/Mb predicted therapeutic benefits of ICI treatment in
NSCLC with a positive predictive value (PPV) of 68%, whereas the
same cutoff in urothelial carcinoma yielded a PPV of only 45%.
ctDNA analyses have further revealed that sub-clonal TMB, rather
than bulk TMB, associates with pulmonary metastatic relapse after
ICI discontinuation, suggesting that spatial heterogeneity may
obscure binary TMB cutoffs (66).
Tryptophan catabolism, which is measured by determining the plasma
kynurenine/tryptophan ratio, has also emerged as an orthogonal
resistance mechanism. A study reported by Botticelli et al
(57) demonstrated that the level
of indoleamine 2,3-dioxygenase 1 activity in patients with
progressive disease involving lung metastases was three-fold higher
than that observed in patients with progressive disease involving
lymph nodes during pembrolizumab therapy, indicating that metabolic
immune escape may be particularly active in pulmonary niches.
Future perspectives
The increasing recognition of the lung-urological
metastatic overlap has necessitated a shift from reactive tumor
management to proactive, mechanism-based strategies (20,27,57).
Although the integration of multidisciplinary teams (MDTs), defined
as collaborative groups of healthcare professionals from diverse
specialties such as urology, thoracic surgery, medical oncology,
radiology and pathology, and advanced sequencing platforms
constitutes the immediate next step for advancing treatments
targeting tumors along this axis, the long-term goal remains the
translation of molecular discoveries into tangible clinical
benefits. Specifically, translational efforts should prioritize the
pharmacological disruption of the CXCR4/CXCL12 axis, for example by
using repurposed antagonists such as plerixafor, to block
metastatic seeding, as well as the standardization of detecting
exosomal miR-210-3p as a non-invasive biomarker for early
intervention. Ultimately, future management of the lung-urological
metastatic overlap necessitates a dual approach aimed at
simultaneously refining diagnostic precision through agnostic
oncology frameworks and enhancing therapeutic specificity by
translating molecular insights into targeted interventions for
investigation in prospective clinical trials.
Liquid biopsy-mediated analysis of ctDNA in
particular represents a cornerstone diagnostic modality for the
dynamic monitoring of pulmonary and urological tumors in the
future. A prospective study has provided evidence that rising ctDNA
levels can predict radiographic progression in pulmonary metastases
from prostate cancer or RCC weeks in advance (67). However, the analytical sensitivity
of ctDNA assays does not remain uniform across metastatic sites.
Recent high-impact research reported by Afridi et al
(68) highlighted a notable
limitation of ctDNA analysis: Standard mutant allele fraction
thresholds that are sensitive for lung-target lesions often fail to
detect bone metastases. This finding underscores the necessity of
adaptive, organ-specific ctDNA thresholds that integrate both tumor
burden and metastatic location to avoid false-negative
stratification. While technological refinements, such as duplex
sequencing, can enhance ctDNA sensitivity across anatomical sites,
these often increase costs and may still fail in cases involving
exceedingly low CTC counts (67).
Therefore, the future clinical utility of ctDNA analysis will
depend on standardized, cost-effective assays validated in
large-scale intervention trials to confirm that pre-emptive
treatment modification guided by molecular relapse (defined as a
sustained increase in ctDNA levels indicating impending
radiographic progression before overt clinical or imaging evidence
of disease) improves survival outcomes.
Concurrently, the integration of artificial
intelligence (AI) with medical imaging has unlocked novel
diagnostic and predictive capabilities. Radiomic signatures
extracted from CT scans based on AI algorithms can non-invasively
predict molecular features, such as EGFR mutation status in brain
metastases of lung adenocarcinoma (69). Furthermore, a study reported by
Leivaditis et al (70)
emphasized that AI surpassed its use in simple diagnostics to
become an integral part of thoracic surgical planning. The analysis
in the aforementioned study demonstrated that AI-driven models can
now predict perioperative risks and long-term survival in complex
metastatic resections, advocating for the inclusion of AI metrics
in MDT decision-making processes. Despite this promise, vendor
dependency and a lack of standardization in AI model training
across different cohorts and imaging platforms remain major
obstacles to the widespread clinical deployment of AI; external
validation studies often report diminished performance levels when
AI algorithms are applied to images acquired from different CT
scanner models from those they are trained on (71,72).
Federated learning platforms, which enable the pooling of imaging,
genomic and clinical data across institutions without compromising
patient privacy and are currently piloted by international
consortia, represent a promising next step for overcoming cohort
heterogeneity and building robust, generalizable models (73).
Regarding tissue diagnostics, spatial
transcriptomics and multiplex immunoprofiling have revealed the
profound impact of the spatial architecture of the TME on
therapeutic responses. These technologies have consistently shown
that TLSs are enriched in pulmonary metastases and associate with
promising responses to immune-checkpoint blockade independently of
traditional biomarkers, such as tumor mutational burden (74). Conversely, TLS are virtually absent
in paired renal parenchymal metastases, highlighting the
fundamental, organ-specific differences in immune topography that
influence treatment efficacy (74,75).
The translation of these insights will involve developing spatial
theranostics, which are diagnostic tests that can guide targeted
therapies based on the spatial context of the TME. For example,
FAP-targeted PET tracers have achieved high tumor-to-background
signal ratios in both primary lung tumors and pulmonary metastases
derived from urological primaries, providing pan-cancer read-outs
of the metastatic niche (76).
However, dosimetry modeling has revealed high renal cortex uptake
of these tracers, raising nephrotoxicity concerns for subsequent
FAP-directed radionuclide therapies and necessitating thorough
risk-benefit assessments (76).
Similarly, CXCR4-directed PET has demonstrated heterogeneous
intra-pulmonary tracer distribution, with hotspots co-localizing
with immune-suppressive, CD163+ macrophage-rich regions,
suggesting that future radiotherapeutic strategies may require
‘dose painting’ to effectively target these immune-excluded
sub-niches (77,78).
Therapeutic innovation has become increasingly
focused on targeting the metastatic organ itself, leading to the
development of designer nanotherapies and cell-based products. A
breakthrough study in Molecular Cancer has advanced this
therapeutic innovation by developing nanoparticle-formulated
chimeric antigen receptor T-cell (CAR-T) therapies. The study
demonstrated that these nanocarriers markedly enhanced the
accumulation of therapeutic agents within pulmonary metastases when
compared with normal drug administration and concurrently reduced
systemic toxicity (79). Notably,
the enhancement of drug accumulation observed in lung tumors was
equivalent for metastases originating from both prostate and renal
primary tumors. This implied that organ-specific vascular
permeability, rather than cancer histology, is a key determinant of
pharmacokinetics (79). In terms
of cellular therapy, CAR-Ts engineered to secrete anti-PD-L1
nanobodies have been shown to proliferate robustly within pulmonary
lesions but exhibit poor persistence in renal parenchymal tumors.
This disparity reflects the underlying site-specific immune
landscapes, wherein pulmonary metastases are characterized by an
immune-excluded phenotype with CD8+ T cells confined to the
invasive margins, as detailed in section 4 of this review (80). The robust proliferation of
engineered CAR-T cells within these pulmonary lesions highlights a
therapeutic strategy designed to overcome, rather than contradict,
this native immune barrier. These findings collectively support the
utility of advanced therapies in which the homing moieties, payload
release kinetics and co-stimulatory domains (e.g., CD28 or 4-1BB
signaling modules that enhance T-cell activation and persistence)
are tailored to the unique biology of the metastatic organ.
Deciphering the lung-urological metastatic axis
requires the evolution of anticancer therapeutic strategies from
systemic therapies to precision medicine. The integration of
AI-driven predictive modeling and organotropic nanotherapies
remains a priority for translational cancer research. Future
efforts should focus on validating these modalities in clinical
trials to address microenvironmental heterogeneity. Ultimately,
disruption of the molecular crosstalk within the lung-urological
metastatic axis holds the potential to redefine standards of care
and improve survival outcomes for patients exhibiting this complex
metastatic disease.
Conclusions
Elucidation of the metastatic overlap between
pulmonary and urological malignancies requires a fundamental
paradigm shift. Notably, the synthesis of previous data highlights
two major breakthroughs. Primarily, the identification of common
targets of cross-organ metastasis offers a biological rationale for
deploying tissue-agnostic therapies. Furthermore, tumor-mediated
regulation of the organ microenvironment acts as a decisive
determinant of clinical outcomes and therapeutic responses. As
such, integrating these shared molecular vulnerabilities with
niche-specific observations remains important for improving patient
survival in this complex patient cohort.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
YW conducted the literature search, drafted the
original manuscript and prepared the figures and tables. JG
conceived the focus of the review, supervised the overall project
and critically revised and edited the manuscript for intellectual
content. All authors read and approved the final manuscript. Data
authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CAFs
|
cancer-associated fibroblasts
|
|
CAR-T
|
chimeric antigen receptor T-cell
|
|
ctDNA
|
circulating tumor DNA
|
|
dMMR
|
mismatch-repair deficient
|
|
EMT
|
epithelial-mesenchymal transition
|
|
FAP
|
fibroblast activation protein
|
|
ICIs
|
immune-checkpoint inhibitors
|
|
MDT
|
multidisciplinary team
|
|
MET
|
mesenchymal-epithelial transition
|
|
MSI-H
|
microsatellite instability-high
|
|
NSCLC
|
non-small cell lung cancer
|
|
PARP
|
poly(ADP-ribose) polymerase
|
|
PD-L1
|
programmed death-ligand 1
|
|
RCC
|
renal cell carcinoma
|
|
TAMs
|
tumor-associated macrophages
|
|
TLS
|
tertiary lymphoid structure
|
|
TMB
|
tumor mutational burden
|
|
TME
|
tumor microenvironment
|
References
|
1
|
Deng Y, Bi R, Zhu Z, Li S, Xu B, Rather WA
and Wang C: A surveillance, epidemiology and end results database
analysis of the prognostic value of organ-specific metastases in
patients with advanced prostatic adenocarcinoma. Oncol Lett.
18:1057–1070. 2019.PubMed/NCBI
|
|
2
|
Surveillance Epidemiology, End Results
(SEER) Program, . SEER*Stat Database: Incidence-SEER Research Data,
8 Registries, Nov 2024 Sub (1975–2022). National Cancer Institute,
Division of Cancer Control and Population Sciences, Surveillance
Research Program. Released. April. 2025, Available from:.
www.seer.cancer.gov
|
|
3
|
Epstein JI, Egevad L, Amin MB, Delahunt B,
Srigley JR and Humphrey PA; Grading Committee, : The 2014
International society of urological pathology (ISUP) consensus
conference on Gleason grading of prostatic carcinoma: Definition of
grading patterns and proposal for a new grading system. Am J Surg
Pathol. 40:244–252. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wei H, Miao J, Cui J, Zheng W, Chen X,
Zhang Q, Liu F, Mao Z, Qiu S and Zhang D: The prognosis and
clinicopathological features of different distant metastases
patterns in renal cell carcinoma: Analysis based on the SEER
database. Sci Rep. 11:178222021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shiota M, Matsubara N, Kato T, Eto M,
Osawa T, Abe T, Shinohara N, Nishimoto K, Yasumizu Y, Tanaka N, et
al: Genomic characterization of metastatic patterns in prostate
cancer using circulating tumor DNA data from the SCRUM-Japan
MONSTAR SCREEN project. J Liq Biopsy. 7:1002822024. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Furubayashi N, Negishi T, Sakamoto N,
Shimokawa H, Morokuma F, Song Y, Hori Y, Tomoda T, Tokuda N, Seki
N, et al: Organ-specific tumor response to pembrolizumab in
advanced urothelial carcinoma after Platinum-based chemotherapy.
Onco Targets Ther. 14:1981–1988. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhuang W, Li Y, Chen P, Wang J, Liu W and
Chen J: Do renal cell carcinoma patients with brain metastases
still need nephrectomy? Int Urol Nephrol. 51:941–949. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hamadi R, Karam I, Khan S, Homsy S and
Luhrs C: Tumour-To-Tumour metastasis: A rare case of prostate
cancer metastasising to primary lung adenocarcinoma. Eur J Case Rep
Intern Med. 11:0045792024.PubMed/NCBI
|
|
9
|
Steindl A, Alpar D, Heller G, Mair MJ,
Gatterbauer B, Dieckmann K, Widhalm G, Hainfellner JA, Schmidinger
M, Bock C, et al: Tumor mutational burden and immune infiltrates in
renal cell carcinoma and matched brain metastases. ESMO Open.
6:1000572021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sorrentino C, Yin Z, Ciummo S, Lanuti P,
Lu LF, Marchisio M, Bellone M and Di Carlo E: Targeting
Interleukin(IL)-30/IL-27p28 signaling in cancer stem-like cells and
host environment synergistically inhibits prostate cancer growth
and improves survival. J Immunother Cancer. 7:2012019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hakozaki K, Tanaka N, Takamatsu K,
Takahashi R, Yasumizu Y, Mikami S, Shinojima T, Kakimi K, Kamatani
T, Miya F, et al: Landscape of prognostic signatures and
immunogenomics of the AXL/GAS6 axis in renal cell carcinoma. Br J
Cancer. 125:1533–1543. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen J, Cao N, Li S and Wang Y:
Identification of a risk stratification model to predict overall
survival and surgical benefit in clear cell renal cell carcinoma
with distant metastasis. Front Oncol. 11:6308422021. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang L, Yang G, Zhao D, Wang J, Bai Y,
Peng Q, Wang H, Fang R, Chen G, Wang Z, et al: CD103-positive CSC
exosome promotes EMT of clear cell renal cell carcinoma: Role of
remote MiR-19b-3p. Mol Cancer. 18:862019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Petrozza V, Costantini M, Tito C,
Giammusso LM, Sorrentino V, Cacciotti J, Porta N, Iaiza A, Pastore
AL, Di Carlo A, et al: Emerging role of secreted miR-210-3p as
potential biomarker for clear cell renal cell carcinoma metastasis.
Cancer Biomark. 27:181–188. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cai Q, Chen Y, Zhang D, Pan J, Xie Z, Ma
S, Liu C, Zuo J, Zhou X, Quan C, et al: Loss of epithelial AR
increase castration resistant stem-like prostate cancer cells and
promotes cancer metastasis via TGF-β1/EMT pathway. Transl Androl
Urol. 9:1013–1027. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li W, Yang FQ, Sun CM, Huang JH, Zhang HM,
Li X, Wang GC, Zhang N, Che JP, Zhang WT, et al: circPRRC2A
promotes angiogenesis and metastasis through epithelial-mesenchymal
transition and upregulates TRPM3 in renal cell carcinoma.
Theranostics. 10:4395–4409. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wu N, Wang Y, Wang K, Zhong B, Liao Y,
Liang J and Jiang N: Cathepsin K regulates the tumor growth and
metastasis by IL-17/CTSK/EMT axis and mediates M2 macrophage
polarization in castration-resistant prostate cancer. Cell Death
Dis. 13:8132022. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chen X, Jia Y, Zhang Y, Zhou D, Sun H and
Ma X: α5-nAChR contributes to epithelial-mesenchymal transition and
metastasis by regulating Jab1/Csn5 signalling in lung cancer. J
Cell Mol Med. 24:2497–2506. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cao Q, Liu Y, Wu Y, Hu C, Sun L, Wang J,
Li C, Guo M, Liu X, Lv J, et al: Profilin 2 promotes growth,
metastasis, and angiogenesis of small cell lung cancer through
cancer-derived exosomes. Aging (Albany NY). 12:25981–25999. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Davoodvandi A, Darvish M, Borran S, Nejati
M, Mazaheri S, Reza Tamtaji O, Hamblin MR, Masoudian N and Mirzaei
H: The therapeutic potential of resveratrol in a mouse model of
melanoma lung metastasis. Int Immunopharmacol. 88:1069052020.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Masuda C, Sugimoto M, Wakita D, Monnai M,
Ishimaru C, Nakamura R, Kinoshita M, Yorozu K, Kurasawa M, Kondoh O
and Yamamoto K: Bevacizumab suppresses the growth of established
non-small-cell lung cancer brain metastases in a hematogenous brain
metastasis model. Clin Exp Metastasis. 37:199–207. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Berta J, Török S, Tárnoki-Zách J,
Drozdovszky O, Tóvári J, Paku S, Kovács I, Czirók A, Masri B,
Megyesfalvi Z, et al: Apelin promotes blood and lymph vessel
formation and the growth of melanoma lung metastasis. Sci Rep.
11:57982021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang B, Pan LY, Kang N and Shen XY: PP4R1
interacts with HMGA2 to promote non-small-cell lung cancer
migration and metastasis via activating MAPK/ERK-induced
epithelial-mesenchymal transition. Mol Carcinog. 59:467–477. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang B, Li Y, Wu Q, Xie L, Barwick B, Fu
C, Li X, Wu D, Xia S, Chen J, et al: Acetylation of KLF5 maintains
EMT and tumorigenicity to cause chemoresistant bone metastasis in
prostate cancer. Nat Commun. 12:17142021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shin SB, Jang HR, Xu R, Won JY and Yim H:
Active PLK1-driven metastasis is amplified by TGF-β signaling that
forms a positive feedback loop in non-small cell lung cancer.
Oncogene. 39:767–785. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gallazzi M, Baci D, Mortara L, Bosi A,
Buono G, Naselli A, Guarneri A, Dehò F, Capogrosso P, Albini A, et
al: Prostate cancer peripheral blood NK cells show enhanced CD9,
CD49a, CXCR4, CXCL8, MMP-9 production and secrete
monocyte-recruiting and polarizing factors. Front Immunol.
11:5861262020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Li L, Zhao L, Yang J and Zhou L:
Multifaceted effects of LRP6 in cancer: Exploring tumor
development, immune modulation and targeted therapies. Med Oncol.
41:1802024. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ruan T, Jiang L, Xu J and Zhou J:
Abiraterone suppresses irradiated lung cancer cells-induced
angiogenic capacities of endothelial cells. J Bioenerg Biomembr.
53:343–349. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chang YC, Liu CT, Yu CY and Sung WW:
NPS-1034 exerts therapeutic efficacy in renal cell carcinoma
through multiple targets of MET, AXL, and TNFRSF1A signaling in a
metastatic model. Cells. 13:17132024. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Greifenstein L, Kramer CS, Moon ES, Rösch
F, Klega A, Landvogt C, Müller C and Baum RP: From automated
synthesis to in vivo application in multiple types of
Cancer-clinical results with [68Ga]Ga-DATA5m.SA.FAPi.
Pharmaceuticals (Basel). 15:10002022. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kraxner A, Braun F, Cheng WY, Yang TO,
Pipaliya S, Canamero M, Andersson E, Harring SV, Dziadek S, Bröske
AE, et al: Investigating the complex interplay between fibroblast
activation protein α-positive cancer associated fibroblasts and the
tumor microenvironment in the context of cancer immunotherapy.
Front Immunol. 15:13526322024. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yu W, Zhang X, Zhang W, Xiong M, Lin Y,
Chang M, Xu L, Lu Y, Liu Y and Zhang J: 19-Hydroxybufalin inhibits
non-small cell lung cancer cell proliferation and promotes cell
apoptosis via the Wnt/β-catenin pathway. Exp Hematol Oncol.
10:482021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Watts A, Singh B, Singh H, Kaur H, Bal A,
Vohra M, Arora SK and Behera D: 68Ga-pentixafor PET/CT
demonstrating in vivo CXCR4 receptor overexpression in rare lung
malignancies: Correlation with histologic and histochemical
findings. J Nucl Med Technol. 50:278–281. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Slania SL, Das D, Lisok A, Du Y, Jiang Z,
Mease RC, Rowe SP, Nimmagadda S, Yang X, Pomper MG, et al: Imaging
of fibroblast activation protein in cancer xenografts using novel
(4-Quinolinoyl)-glycyl-2-cyanopyrrolidine-Based small molecules. J
Med Chem. 64:4059–4070. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Manawy SM, Faruk EM, Hindawy RF, Hassan
MM, Farrag DMG, Bashar MAE, Fouad H, Bagabir RA, Hassan DAA, Zaazaa
AM, et al: Modulation of the Sirtuin-1 signaling pathway in
doxorubicin-induced nephrotoxicity (synergistic amelioration by
resveratrol and pirfenidone). Tissue Cell. 87:1023302024.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zheng Y, Yang S, Si J, Zhao Y, Zhao M and
Ji E: Shashen-maidong decoction inhibited cancer growth under
intermittent hypoxia conditions by suppressing oxidative stress and
inflammation. J Ethnopharmacol. 299:1156542022. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Liu X, Tang J, Peng L, Nie H, Zhang Y and
Liu P: Cancer-associated fibroblasts promote malignant phenotypes
of prostate cancer cells via autophagy: Cancer-associated
fibroblasts promote prostate cancer developmentt. Apoptosis.
28:881–891. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gao F, Chen X, Li X, Deng C and Luo P: The
Pro-migratory and Pro-invasive roles of cancer-associated
fibroblasts secreted IL-17A in prostate cancer. J Biochem Mol
Toxicol. 39:e700472025. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Li H, Ding J, Lu M, Liu H, Miao Y, Li L,
Wang G, Zheng J, Pei D and Zhang Q: CAIX-specific CAR-T cells and
sunitinib show synergistic effects against metastatic renal cancer
models. J Immunother. 43:16–28. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Maolake A, Izumi K, Shigehara K,
Natsagdorj A, Iwamoto H, Kadomoto S, Takezawa Y, Machioka K,
Narimoto K, Namiki M, et al: Tumor-associated macrophages promote
prostate cancer migration through activation of the CCL22-CCR4
axis. Oncotarget. 8:9739–9751. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shi F, Sun MH, Zhou Z, Wu L, Zhu Z, Xia
SJ, Han BM, Zhao YY, Jing YF and Cui D: Tumor-associated
macrophages in direct contact with prostate cancer cells promote
malignant proliferation and metastasis through NOTCH1 pathway. Int
J Biol Sci. 18:5994–6007. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wang C, Wang Y, Hong T, Ye J, Chu C, Zuo
L, Zhang J and Cui X: Targeting a positive regulatory loop in the
tumor-macrophage interaction impairs the progression of clear cell
renal cell carcinoma. Cell Death Differ. 28:932–951. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
O'Shaughnessy MJ, Murray KS, La Rosa SP,
Budhu S, Merghoub T, Somma A, Monette S, Kim K, Corradi RB, Scherz
A and Coleman JA: Systemic antitumor immunity by PD-1/PD-L1
Inhibition is potentiated by Vascular-targeted photodynamic therapy
of primary tumors. Clin Cancer Res. 24:592–599. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhao Y, Peng X, Baldwin H, Zhang C, Liu Z
and Lu X: Anti-androgen therapy induces transcriptomic
reprogramming in metastatic castration-resistant prostate cancer in
a murine model. Biochim Biophys Acta Mol Basis Dis.
1867:1661512021. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lv Z, Cui B, Huang X, Feng HY, Wang T,
Wang HF, Xuan YD, Li HZ, Ma X, Huang Y and Zhang X: FGL1 as a novel
mediator and biomarker of malignant progression in clear cell renal
cell carcinoma. Front Oncol. 11:7568432021. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Zhang Y, Wang X, Gu Y, Liu T, Zhao X,
Cheng S, Duan L, Huang C, Wu S and Gao S: Complement C3 of
tumor-derived extracellular vesicles promotes metastasis of RCC via
recruitment of immunosuppressive myeloid cells. Proc Natl Acad Sci
USA. 122:e24200051222025. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zhu Y, Han CH, Yang YL, Xu JJ and Yu YW:
Metastatic renal cell carcinoma: A clinicopathological analysis of
196 cases. Zhonghua Bing Li Xue Za Zhi. 49:1255–1260. 2020.(In
Chinese). PubMed/NCBI
|
|
48
|
Herrington CS, Poulsom R and Coates PJ:
Recent advances in pathology: The 2019 annual review issue of the
journal of pathology. J Pathol. 247:535–538. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Nguyen NJ, Sherman C, van der Kwast TH and
Downes MR: Aggressive prostatic adenocarcinoma with urothelial-like
morphology, with frequent CK7/CK20/HMWK expression and occasional
diffuse neuroendocrine features: A clinicopathologic study of 12
cases. Pathol Res Pract. 254:1551052024. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zhao H, Nolley R, Chan AMW, Rankin EB and
Peehl DM: Cabozantinib inhibits tumor growth and metastasis of a
patient-derived xenograft model of papillary renal cell carcinoma
with MET mutation. Cancer Biol Ther. 18:863–871. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Yu W, Wang Y, Rao Q, Jiang Y, Zhang W and
Li Y: Xp11.2 translocation renal neoplasm with features of TFE3
rearrangement associated renal cell carcinoma and Xp11
translocation renal mesenchymal tumor with melanocytic
differentiation harboring NONO-TFE3 fusion gene. Pathol Res Pract.
215:1525212019. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Gong Y, Fan L, Fei X, Zhu Y, Du X, He Y,
Pan J, Dong B and Xue W: Targeted Next-generation sequencing
reveals heterogenous genomic features in viscerally metastatic
prostate cancer. J Urol. 206:279–288. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Strati A, Markou A, Kyriakopoulou E and
Lianidou E: Detection and molecular characterization of circulating
tumour cells: Challenges for the clinical setting. Cancers (Basel).
15:21852023. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Dincman TA, Karam JAQ, Giordano A, Li H,
Drusbosky LM, Gourdin TS, Howe PH and Lilly MB: Genomic
amplifications identified by circulating tumor DNA analysis guide
prognosis in metastatic castration-resistant prostate cancer. Front
Oncol. 13:12022772023. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Esposito A, Bardelli A, Criscitiello C,
Colombo N, Gelao L, Fumagalli L, Minchella I, Locatelli M,
Goldhirsch A and Curigliano G: Monitoring tumor-derived cell-free
DNA in patients with solid tumors: Clinical perspectives and
research opportunities. Cancer Treat Rev. 40:648–655. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Ying M, Mao J, Sheng L, Wu H, Bai G, Zhong
Z and Pan Z: Biomarkers for prostate cancer bone metastasis
detection and prediction. J Pers Med. 13:7052023. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Botticelli A, Mezi S, Pomati G, Cerbelli
B, Cerbelli E, Roberto M, Giusti R, Cortellini A, Lionetto L,
Scagnoli S, et al: Tryptophan catabolism as immune mechanism of
primary resistance to Anti-PD-1. Front Immunol. 11:12432020.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Kasi PM, Bucheit LA, Liao J, Starr J,
Barata P, Klempner SJ, Gandara D, Shergill A, Madeira da Silva L,
Weipert C, et al: Pan-cancer prevalence of microsatellite
Instability-High (MSI-H) identified by circulating tumor DNA and
Associated Real-world clinical outcomes. JCO Precis Oncol.
7:e23001182023. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Pollack M, Keating K, Wissinger E, Jackson
L, Sarnes E and Cuffel B: Transforming approaches to treating TRK
fusion cancer: Historical comparison of larotrectinib and
histology-specific therapies. Curr Med Res Opin. 37:59–70. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Markham A: Savolitinib: First approval.
Drugs. 81:1665–1670. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
de Bono JS, Mehra N, Scagliotti GV, Castro
E, Dorff T, Stirling A, Stenzl A, Fleming MT, Higano CS, Saad F, et
al: Talazoparib monotherapy in metastatic Castration-resistant
prostate cancer with DNA repair alterations (TALAPRO-1): An
open-label, phase 2 trial. Lancet Oncol. 22:1250–1264. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Yap TA, Bardia A, Dvorkin M, Galsky MD,
Beck JT, Wise DR, Karyakin O, Rubovszky G, Kislov N, Rohrberg K, et
al: Avelumab plus talazoparib in patients with advanced solid
tumors: The JAVELIN PARP medley nonrandomized controlled trial.
JAMA Oncol. 9:40–50. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Danno T, Iwata S, Niimi F, Honda S, Okada
H and Azuma T: Nivolumab and ipilimumab combination immunotherapy
for patients with metastatic collecting duct carcinoma. Case Rep
Urol. 2021:99363302021.PubMed/NCBI
|
|
64
|
Liu C, Piao J and Shang Z:
Hyperprogressive disease after radiotherapy combined with anti-PD-1
therapy in renal cell carcinoma: A case report and review of the
literature. BMC Urol. 21:422021. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Passaro A, Stenzinger A and Peters S:
Tumor mutational burden as a Pan-cancer biomarker for
immunotherapy: The limits and potential for convergence. Cancer
Cell. 38:624–625. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Chen A, Zhang S, Xiong L, Xi S, Tao R,
Chen C, Li J, Chen J and Li C: Investigation of an Alternative
marker for hypermutability evaluation in different tumors. Genes
(Basel). 12:1972021. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zhang C, Liu Y, Chen Z, Liu YI, Mao Q,
Zhang GE, Lin H, Zheng J and Li H: Current status, hotspots, and
trends in cancer prevention, screening, diagnosis, treatment, and
rehabilitation: A bibliometric analysis. Oncol Res. 33:1437–1458.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Afridi WA, Picos SH, Bark JM, Stamoudis
DAF, Vasani S, Irwin D, Fielding D and Punyadeera C: Minimally
invasive biomarkers for triaging lung nodules-challenges and future
perspectives. Cancer Metastasis Rev. 44:292025. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Tabnak P, Kargar Z, Ebrahimnezhad M and
HajiEsmailPoor Z: A Bayesian meta-analysis on MRI-based radiomics
for predicting EGFR mutation in brain metastasis of lung cancer.
BMC Med Imaging. 25:442025. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Leivaditis V, Maniatopoulos AA, Lausberg
H, Mulita F, Papatriantafyllou A, Liolis E, Beltsios E, Adamou A,
Kontodimopoulos N and Dahm M: Artificial intelligence in thoracic
surgery: A review bridging innovation and clinical practice for the
next generation of surgical care. J Clin Med. 14:27292025.
View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Tang F, Zha XK, Ye W, Wang YM, Wu YF, Wang
LN, Lyu LP and Lyu XM: Artificial intelligence-assisted
endobronchial ultrasound for differentiating between benign and
malignant thoracic lymph nodes: A meta-analysis. BMC Pulm Med.
25:3032025. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Zhang L, Yang D, Ye X and Bai C:
Successful application of artificial Intelligence-assisted analysis
of invasive pulmonary adenocarcinoma less than 6 mm in size: A case
report and literature review. Clin Respir J. 19:e700732025.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Talebi F, Gregucci F, Ahmed J, Ben Chetrit
N, D Brown B, Chan TA, Chand D, Constanzo J, Demaria S, I
Gabrilovich D, et al: Updates on radiotherapy-immunotherapy
combinations: Proceedings of 8th Annual ImmunoRad Conference.
Oncoimmunology. 14:25078562025. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Suzuki H, Maruya Y, Inomata S, Yamaguchi
H, Ozaki Y, Watanabe M, Fukuhara M, Muto S and Okabe N: Clinical
significance and future prospects of tertiary lymphoid structure in
lung cancer. Gan To Kagaku Ryoho. 52:628–632. 2025.(In Japanese).
PubMed/NCBI
|
|
75
|
Jahangir CA, Page DB, Broeckx G, Gonzalez
CA, Burke C, Murphy C, Reis-Filho JS, Ly A, Harms PW, Gupta RR, et
al: Image-based multiplex immune profiling of cancer tissues:
Translational implications. A report of the International
Immuno-oncology Biomarker Working Group on Breast Cancer. J Pathol.
262:271–288. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Lee EJ, Chung HW, So Y, Kim IA, Kim HJ and
Lee KY: Recent advances in PET and radioligand therapy for lung
cancer: FDG and FAP. Cancers (Basel). 17:25492025. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Hajikarimloo B, Mohammadzadeh I, Tos SM,
Habibi MA, Hashemi R, Hezaveh EB, Najari D, Hasanzade A, Hooshmand
M and Bana S: Machine learning in prediction of epidermal growth
factor receptor status in non-small cell lung cancer brain
metastases: A systematic review and meta-analysis. BMC Cancer.
25:8182025. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Yu J, Kong X and Feng Y: Tumor
microenvironment-driven resistance to immunotherapy in non-small
cell lung cancer: Strategies for Cold-to-Hot tumor transformation.
Cancer Drug Resist. 8:212025.PubMed/NCBI
|
|
79
|
Shang D, Zhou Z, Shi R, Wang Z, Zhang P,
Peng F, Li H, Cheng G, Qin H, Xie Z, et al: Nanoparticle-based
strategy in CAR-T cell immunotherapy: Challenges, implications, and
perspectives. Mol Cancer. 24:2812025. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Rafii S, Mukherji D, Komaranchath AS,
Khalil C, Iqbal F, Abdelwahab SI, Abyad A, Abuhelwa AY, Gandikota L
and Al-Shamsi HO: Advancing CAR T-Cell therapy in solid tumors:
Current landscape and future directions. Cancers (Basel).
17:28982025. View Article : Google Scholar : PubMed/NCBI
|














