Introduction
Primary gallbladder carcinoma shows a variety of
growth patterns, some of which spread expansively to form a mass
while others infiltrate diffusely and deeply into the gallbladder
wall or the surrounding organs. Numerous studies have been
conducted on gallbladder carcinoma with cystic formation, such as
cystadenocarcinoma of the gallbladder (1–4) and
Rokitansky-Aschoff sinus (RAS)-associated gallbladder carcinoma
(5–7). In these tumors, it is normal that the
cancerous cystic component is multilocular or not large in size.
This study evaluated the clinicopathological findings and analyzed
the morphogenesis of a gallbladder carcinoma showing a large
malignant cystic growth.
Case report
A 79-year-old Japanese female suffering from upper
abdominal pain and distention was admitted to our hospital. The
patient had previous illness of note nor a family history of
disease. A large mass was palpable in the right upper quadrant of
the abdomen. The patient’s lactate dehydrogenase was elevated to
413 IU/l (normal range <230), and two serum tumor markers,
carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9
(CA19-9), were both elevated at 3.4 ng/ml (normal range <2.5)
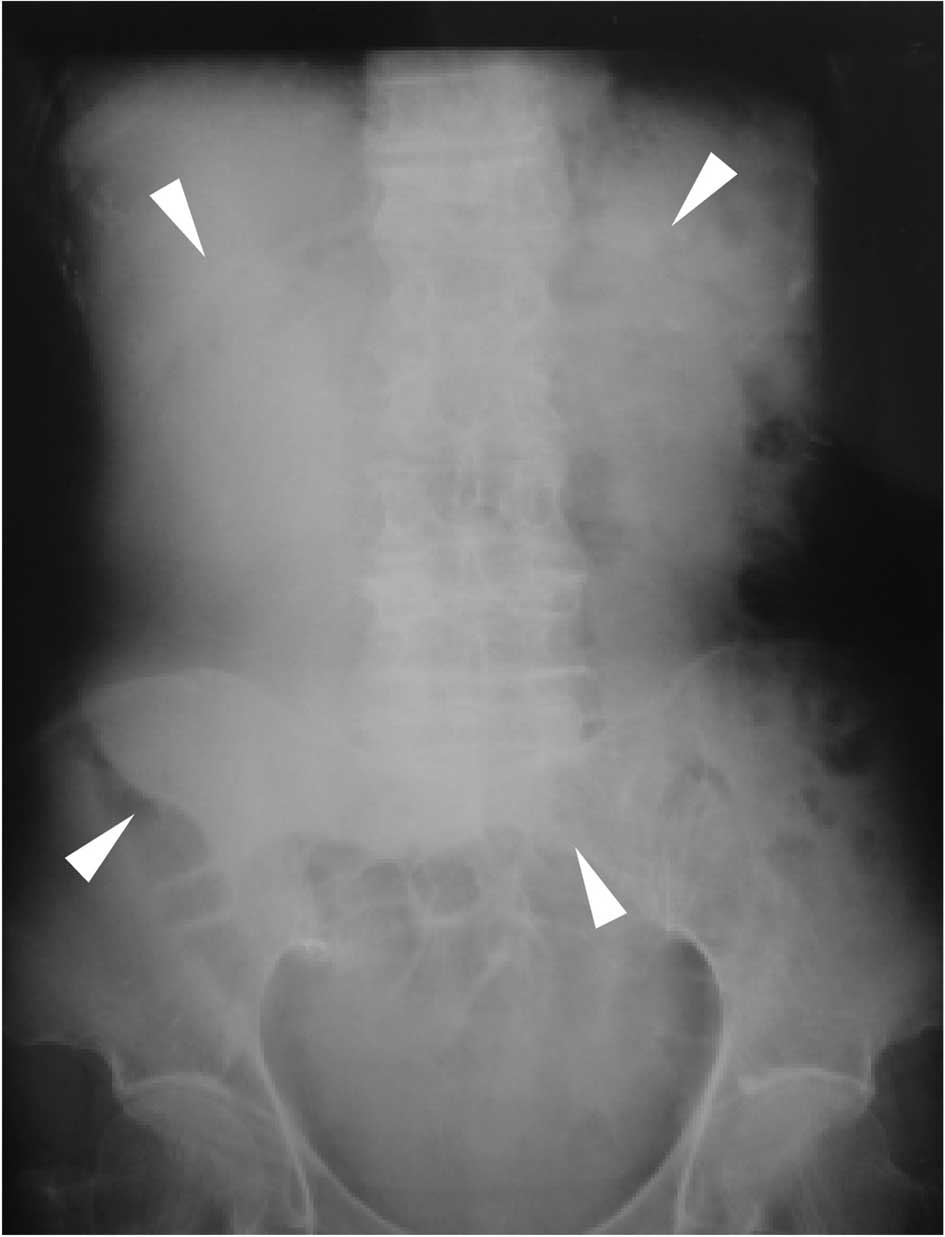
and 1465.3 U/ml (normal range <37), respectively. Abdominal
radiography showed an oval radio-opaque shape of 15 cm in diameter
in the right upper abdomen (Fig.
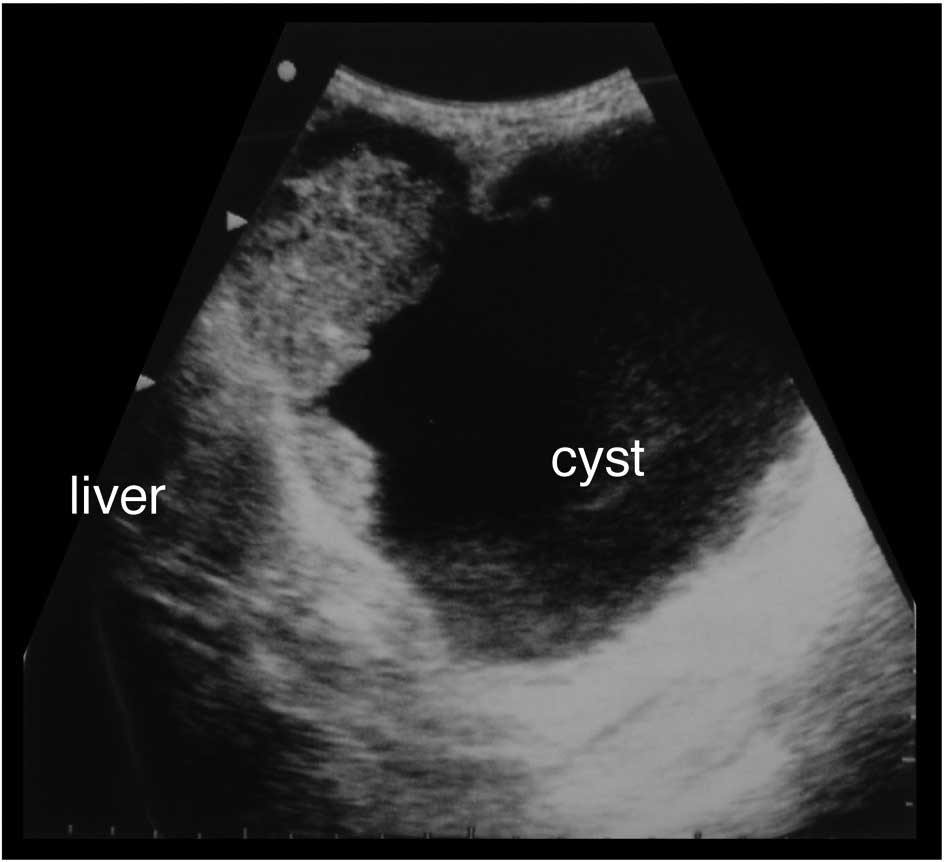
1). Ultrasonography (Fig. 2)
and computed tomography (CT) (Fig.
3) revealed the tumor to be a monolocular cyst with an
irregular wall thickness of 15 cm in diameter concomitant with a
solid mass of 8 cm in diameter around the gallbladder bed,
suspected to be a tumor originating from the gallbladder.
Endoscopic examinations of the alimentary tract showed no
abnormalities. During celiotomy, the tumor with a large pale gray
cystic component was identified at the fundus of the gallbladder.
The tumor fibrously adhered to the liver, duodenum, and greater
omentum, but it appeared to have only partially infiltrated into
the transverse colon. A number of small nodules suspected to be
tumor dissemination were scattered on the peritoneum. Gallbladder
cancer with peritoneal dissemination was diagnosed. Although
curative resection for the tumor was impossible, a simple
cholecystectomy was performed that included the tumor without
systematic lymphadenectomy, and a partial resection of the
transverse colon was added due to its tight adhesion by the tumor
cyst.
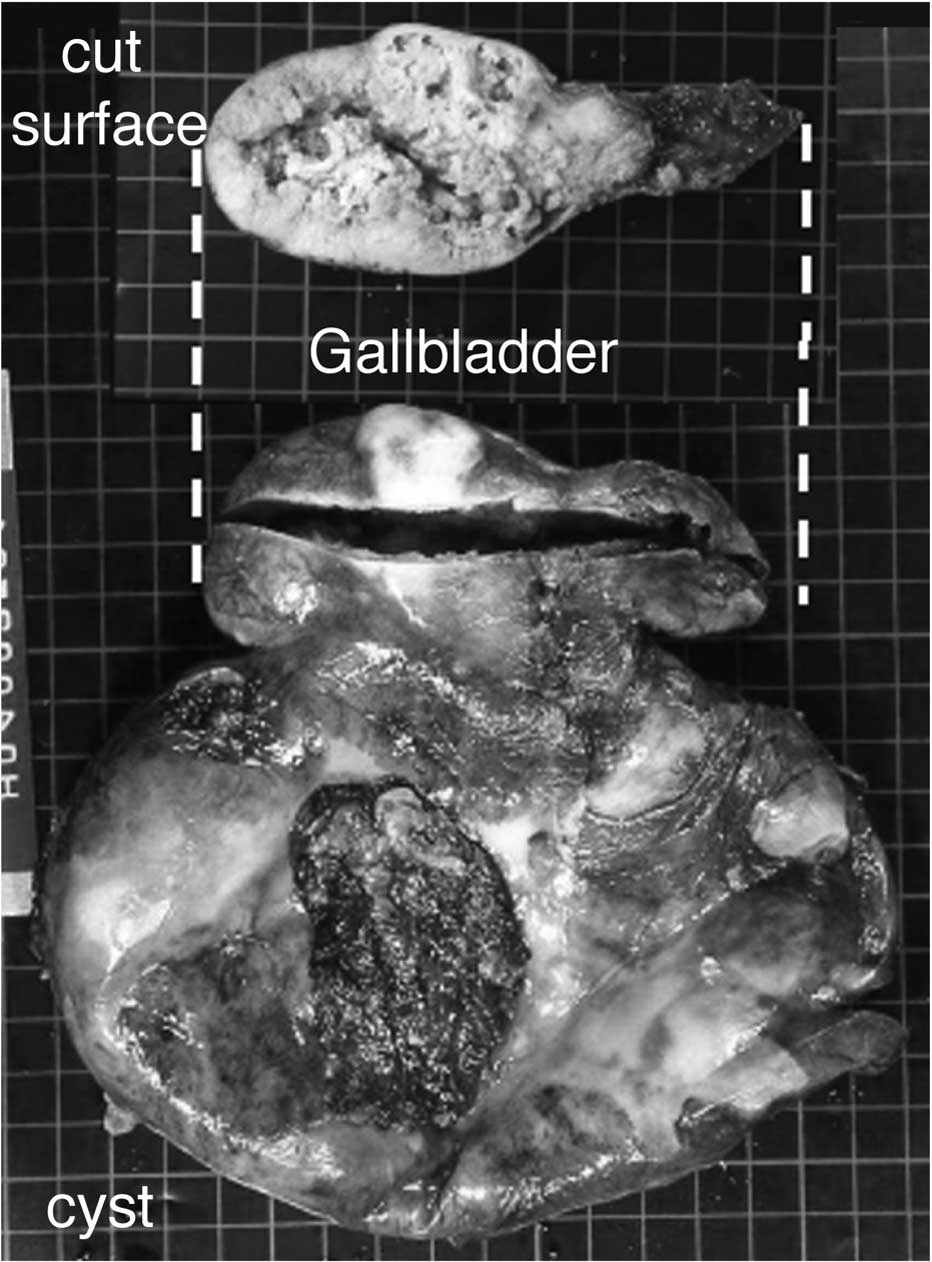
The gross appearance of the excised gallbladder with
the monolocular large cyst is shown in Fig. 4. On the cut face of the gallbladder,
the lumen was occupied by a solid neoplasm. The cyst included a
large amount of serous fluid and protruded continuously from the
body of the gallbladder, but was not part of the gallbladder lumen.
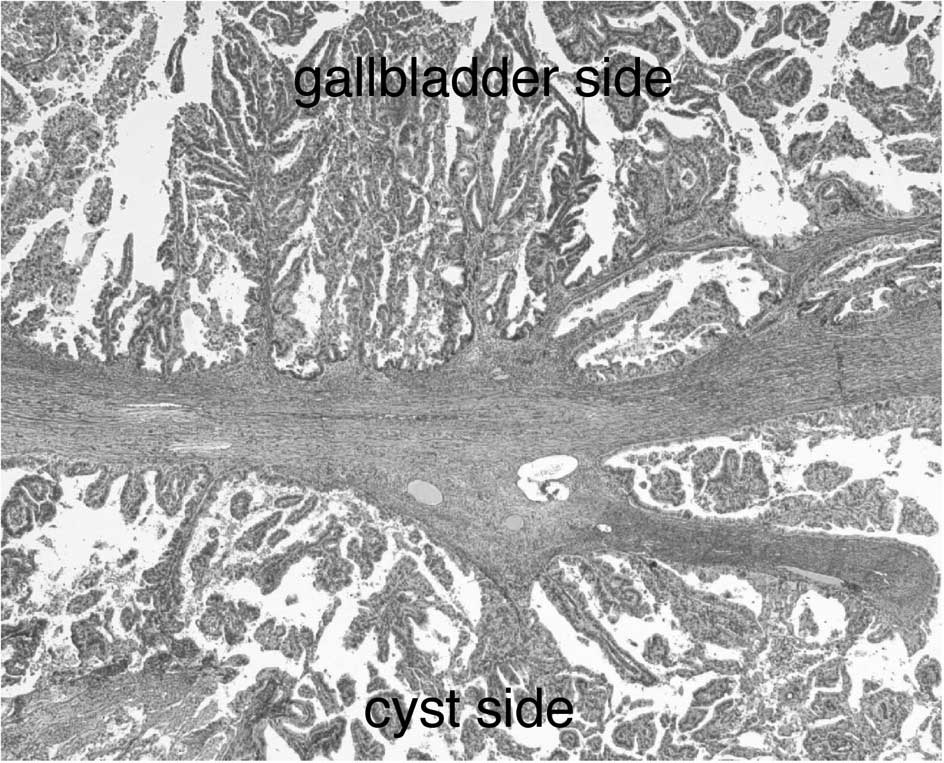
Microscopic examination suggested that the internal wall of the
cyst was covered with non-neoplastic low papillary columnar
epithelium and papillary adenocarcinoma. However, the remainder of
the cyst was composed of papillary carcinoma (Figs. 4B and 5A). A macroscopic solid mass observed in
the gallbladder lumen also consisted microscopically of
various-sized cystic components composed of papillary
adenocarcinoma (Fig. 5B).
Immunohistochemical examinations showed that the
cancer cells of the gallbladder and the large cyst were positive
for cytokeratin 7 and CEA, and were negative for mesothelin and
calretinin. The immunohistochemical findings proved that the
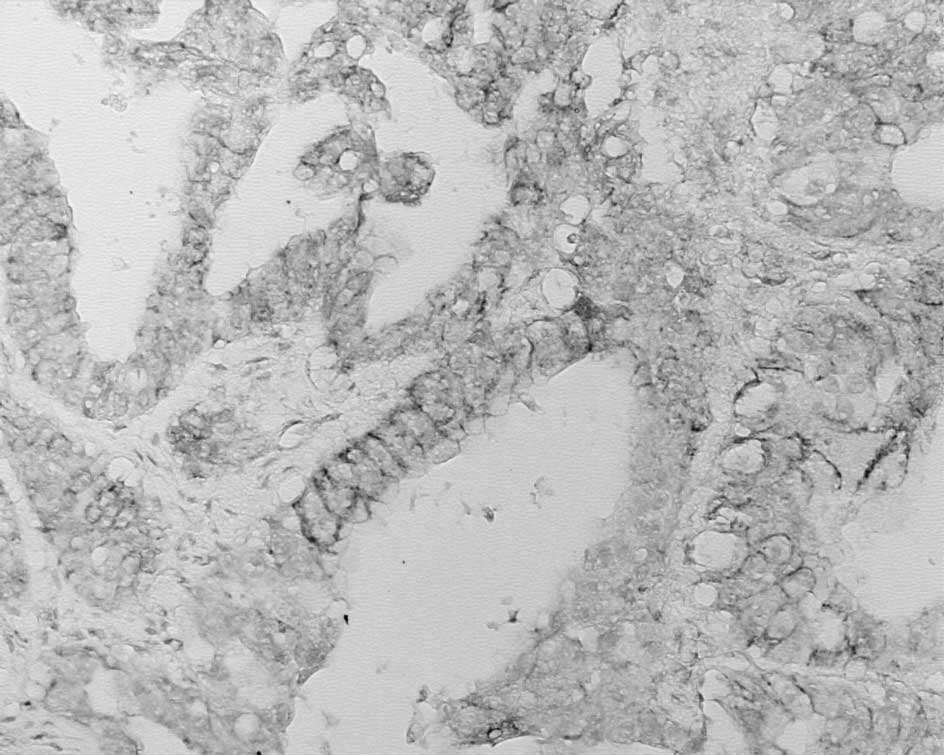
carcinoma was derived from gallbladder epithelium. Further
immunohistochemical studies [E-cadherin, epidermal growth factor
(EGF) and hepatocyte growth factor (HGF)] were performed to
determine the morphogenesis of this tumor. The cancer cells of the
gallbladder and large cystic lesion showed positive staining for
E-cadherin (Fig. 6A), EGF (Fig. 6B) and HGF (Fig. 6C).
The postoperative clinical course of the patient was
uneventful. Some anti-cancer chemotherapy was recommended, but the
patient refused to undergo this treatment. The patient succumbed to
the disease at 185 days post-surgery.
Discussion
The key interest of this case involved cystic
formation, which was associated with gallbladder carcinoma cells.
Various hypotheses have been documented regarding the genesis of
the cystic structure in gallbladder mucosal tissues. Essentially,
there are two types of cysts: acquired and congenital. Acquired
cysts develop as a result of RAS, pericholecystic adhesion,
parasites (8) or closed
communication between the diverticulum and the gallbladder caused
by inflammation or a tumor (9).
With regard to gallbladder carcinoma, the cysts are presumed to
originate in the RAS, diverticulum or to be associated with
congenital cysts (5–7,9).
However, gallbladder carcinoma with a large monolocular cystic
cancerous component is an extremely rare condition. To the best of
our knowledge, there has been only one case report of gallbladder
carcinoma accompanied by a large malignant epithelium-covered cyst
of more than 10 cm in diameter (9).
Sworn and Gay (9) reported an
epithelium-covered cyst of 16 cm in diameter associated with
gallbladder carcinoma. The cyst was lined by papillary gallbladder
epithelium with carcinoma in situ in various parts. Similar
to the present case, no communication between the cyst and the
gallbladder lumen was found, and the cyst contained serous fluid.
The authors hypothesized that the cyst was acquired by the
occlusion of the communication of a fundal diverticulum and the
gallbladder. The tumor epithelium-covered cysts can probably be
regarded as a special subtype of papillary carcinoma, and are
different from cystadenocarcinoma of the gallbladder in which
malignant cyst formation is likely the dominant type of growth.
One of the possible mechanisms underlying the
formation of these cysts is the occlusion of the communication
between RAS or a blockage in the communication between the
diverticulum and gallbladder due to inflammation or cancer growth.
The present case showed large and small cancerous lesions forming
various cystic structures, suggesting that the large cysts may have
arisen following the transition from one of the small cysts in the
solid gallbladder carcinoma (Fig.
5B). Therefore, we speculate that this characteristic papillary
adenocarcinoma results in the formation of cysts.
We previously reported the acquisition of cysts from
gallbladder epithelial and gallbladder cancer cells in
vitro, and confirmed that the expression of EGF, HGF and
E-cadherin were essential to the cystogenesis of these gallbladder
cancer cells (10–13). We confirmed that EGF, HGF and
E-cadherin were expressed in the cancer cells of both the
gallbladder and large cyst in vivo. Although the results of
immunohistochemical analyses are not sufficient to clarify the
mechanism underlying the cyst-forming growth in our case, it is
compatible with the previous hypothesis.
In conclusion, this study reports a rare case of
gallbladder carcinoma with a large monolocular cystic carcinoma
component. Although the mechanism responsible for the development
of cyst-forming papillary carcinoma of the gallbladder remains
unknown, the present case is crucial for understanding the
mechanism of cystogenesis in gallbladder carcinoma. We anticipate
that as additional case reports accumulate, it is likely that the
nature of cyst-forming papillary carcinoma may be proven and the
entity established as a unique carcinoma.
References
|
1
|
Matsumoto M, Murata M, Maeda K, Utsumi T,
Sugioka A and Kuroda M: Epithelial cyst of the gallbladder
associated with adenocarcinoma. J Hepatobiliary Pancreat Surg.
9:389–392. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Terada T, Takeuchi T and Taniguchi M:
Hepatobiliary cystadenocarcinoma with cystadenoma elements of the
gallbladder in an old man. Pathol Int. 53:790–795. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Terada T: Gallbladder adenocarcinoma
arising in Rokitansky-Aschoff sinus. Pathol Int. 58:806–809. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Waldmann J, Zielke A, Moll R, Schweinsberg
TS, Rothmund M and Langer P: Cystadenocarcinoma of the gallbladder.
J Hepatobiliary Pancreat Surg. 13:594–599. 2006. View Article : Google Scholar
|
|
5
|
Kawarada Y, Sanda M, Mizumoto R and Yatani
R: Early carcinoma of the gallbladder, noninvasive carcinoma
originating in the Rokitansky-Aschoff Sinus: a case report. Am J
Gastroenterol. 81:61–66. 1986.PubMed/NCBI
|
|
6
|
Funabiki T, Matsumoto S, Tsukada N, Kimura
T, Yoshizaki S and Horibe Y: A patient with early gallbladder
cancer derived from a Rokitansky-Aschoff sinus. Surg Today.
23:350–355. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Albores-Saavedra J, Shukla D, Carrick K
and Henson DE: In situ and invasive adenocarcinoma of the
gallbladder extending into or arising from Rokitansky-Aschoff
sinus. Am J Surg Pathol. 28:621–628. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jacobs E, Ardichvili D, D’avanzo E,
Penneman R and Van Gansbeke D: Cyst of the gallbladder. Dig Dis
Sci. 36:1796–1802. 1991. View Article : Google Scholar
|
|
9
|
Sworn MJ and Gay P: A fundal cyst of the
gallbladder - an unusual abdominal mass. Med J Aust. 2:307–308.
1975.PubMed/NCBI
|
|
10
|
Mori M and Miyazaki K: Factors affecting
morphogenesis of rabbit gallbladder epithelial cells cultured in
collagen gels. Cell Tissue Res. 300:331–344. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mukai S, Miyazaki K and Yakushiji H: The
role of E-cadherin in the differentiation of gallbladder cancer
cells. Cell Tissue Res. 306:117–128. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kohya N, Kitajima Y, Jiao W and Miyazaki
K: Effects of E-cadherin transfection on gene expression of a
gallbladder carcinoma cell line: repression of MTS1/S100A4 gene
expression. Int J Cancer. 104:44–53. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jiao W, Miyazaki K and Kitajima Y:
Exogenous expression of E-cadherin in gallbladder carcinoma cell
line G-415 restores its cellular polarity and differentiation. Int
J Oncol. 19:1099–1107. 2001.PubMed/NCBI
|