Introduction
Multiple myeloma (MM) is a malignant neoplasm of
plasma cells that accumulate in the bone marrow. MM accounts for
approximately 10% of all hematologic malignancies (1,2). It is
characterized by skeletal destruction, renal failure,
hypercalcaemia and monoclonal immunoglobulin (M protein)
accumulation in serum or urine. The IgG and IgA type M proteins are
most commonly observed. The IgM type is extremely rare, accounting
for 0.5% of patients with myeloma (3,4).
The distinction between IgM MM and Waldenstrom’s
macroglobulinemia (WM) is usually straightforward. The presence of
an IgM monoclonal gammopathy with lymphadenopathy,
hepatosplenomegaly, hyperviscosity syndrome and lymphoplasmacytoid
cell infiltration is characteristic of WM. The possibility of IgM
myeloma arises when a patient presents with monoclonal IgM protein,
multiple lytic bone lesions and renal insufficiency, particularly
in the absence of lymphadenopathy and hepatomegaly. However, it has
been noted that typical clinical features, such as lytic bone
lesions in IgM MM or organomegaly in WM, are not always present.
Therefore, additional diagnostic tools are required for a
definitive diagnosis of IgM MM. We present a case of IgM myeloma
without multiple lytic bone lesions and renal insufficiency. The
diagnosis was confirmed by immuno-phenotype analysis.
Case report
A 57-year-old male complained of repeated epistaxis
for one week prior to admission. No organomegaly or lymphadenopathy
was documented upon physical and abdominal ultrasound examination.
Laboratory findings at diagnosis were: erythrocyte sedimentation
rate 147 mm/h, white blood cells 5.07×109/l, hemoglobin
72 g/l, platelets 219×1012/l, activated partial
thromboplastin time 68.3 sec (reference range, 25.5–45.5 sec),
creatinine 77.4 μmol/l (reference range, 52–102 μmol/l), blood urea
nitrogen 7.48 μmol/l (reference range, 2.86–8.20 μmol/l) and
calcium 2.46 μmol/l (reference range, 2.03–2.54 μmol/l). Other
routine laboratory parameters were normal. Serum electrophoresis
revealed a homogeneous spike in the gamma region identified as an
IgM by immunofixation with the presence of IgL-λ in the serum.
Nephelometry showed a higher IgM level of 106 g/l (reference range,
0.40–3.00 g/l), a higher IgL-λ level of 11.6 g/l (reference range,
0.9–2.1 g/l), a lower level of IgG 6.13 g/l (reference range,
7.0–16.0 g/l), and a normal level of IgA of 0.64 g/l (reference
range, 0.5–4.00 g/l). The ß2-microglobulin level was 3.76 mg/l
(reference range, 0.7–1.8 mg/l). Whole body bone scan and an X-ray
of the skull and pelvis showed no evidence of osteolytic lesions.
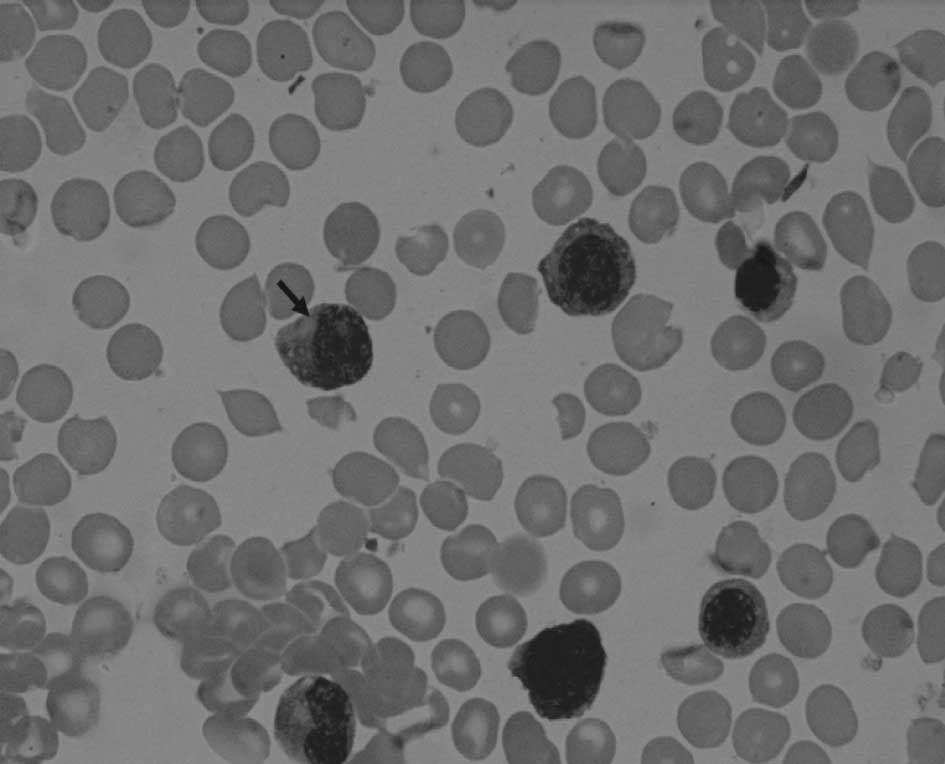
Bone marrow aspirate morphology showed a diffuse infiltration of
35% atypical plasma cells. The cells showed eccentrically placed
nuclei, intracytoplasmic vacuoles, clumped chromatin and a
prominent nucleolus (Fig. 1).
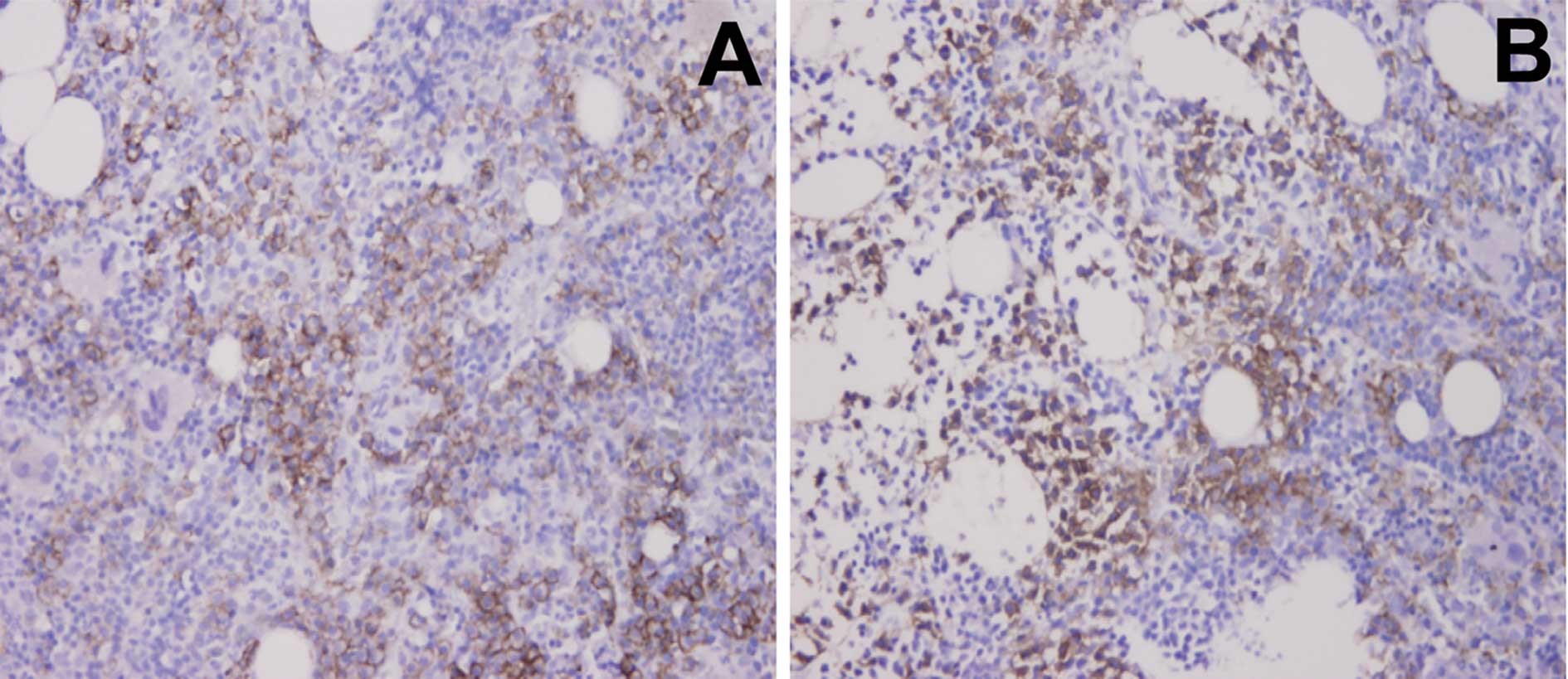
Immunohistochemical staining of a bone marrow trephine biopsy
specimen revealed CD38- and CD138-positive cell infiltration
(Fig. 2). The cells were CD19-,
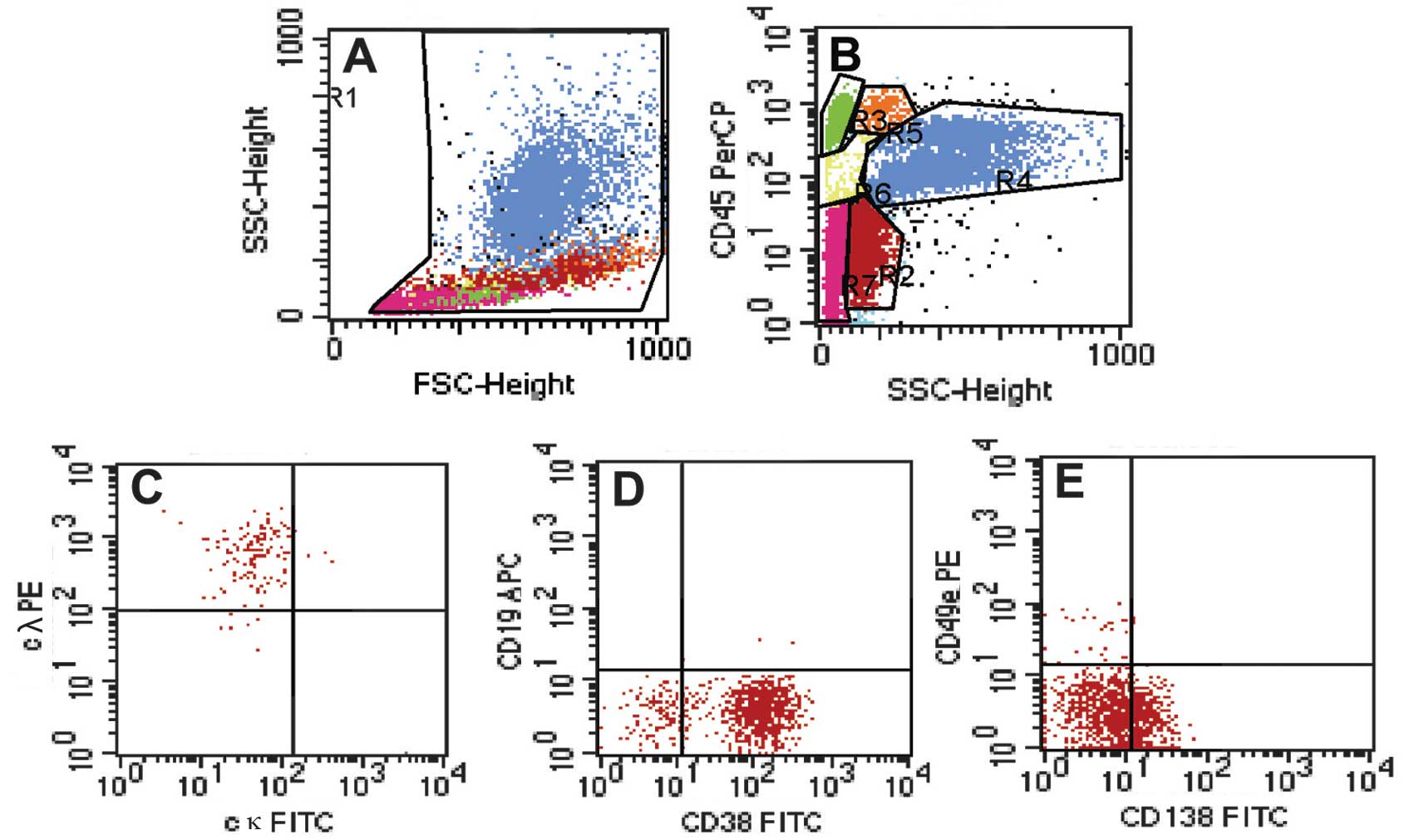
CD20-, CD56- and CD117-negative. As shown in Fig. 3, the flow cytometric analysis of
bone marrow cells revealed monoclonal cytoplasmatic IgL-λ. Abnormal
cells were positive for CD38, CD138 and CD23. These cells did not
express B-cell markers, such as CD19, CD20, CD22, nor other
markers, such as CD5, CD10, CD25, CD27, CD49e, CD56 and CD117.
The diagnosis of IgM myeloma was made, and the
patient was treated with a combination chemotherapy of
cyclophosphamide, methylprednisolone and thalidomide. Currently,
the patient is free of epistaxis and has shown signs of improvement
during the eight months following initial diagnosis.
Discussion
IgM MM is a rare lymphoproliferative disease
accounting for approximately 0.5% of MM cases (3,4). Few
cases of IgM MM have been reported in the medical literature thus
far (5). In 2006, Annibali et
al (6) reported 4 cases of IgM
MM and reviewed another 9 cases published as case reports since
1998. Among these 13 patients only 1 patient survived more than 36
months, suggesting that IgM MM is more aggressive than WM which is
associated with a median survival of 60 months (7). Therefore, accurate differentiation of
these conditions is vital as they run different courses and require
different therapeutic approaches.
Regarding the differential diagnosis between IgM MM
and WM, the presence of multiple lytic bone lesions with bone
marrow plasma cell infiltration supports a diagnosis of myeloma
while lymphadenopathy or hepatosplenomegaly with lymphoplasmacytoid
bone marrow proliferation favors WM (8). Therefore, certain authors consider
lytic bone lesions to be an indicator for differentiating IgM MM
from WM (7,9). However, clinical features are not
always helpful in differentiating IgM MM from WM. Notably, lytic
bone lesions may not be present in IgM MM patients (6), limiting the diagnostic potential.
Therefore, the correct diagnosis of IgM MM should be based on
plasma cells with >15% nucleated bone marrow cells. Berman
(10) recommended morphologic
criteria as an ideal way to distinguish between IgM MM and WM. When
infiltrated cells do not exhibit typical plasma cell morphology, an
accurate immunophenotype characterization is required. However,
limited data are available in the literature relating specifically
to the phenotype of IgM MM (9,11).
The clinical manifestation of our patient was
atypical. He presented with bleeding tendency rather than bone pain
or renal failure. No lymphadenopathy or hepatomegaly was
documented. The distinction between lymphoid cells with
plasmacytoid features and atypical plasma cells was difficult under
light microscopy. However, the immunophenotype was suggestive of MM
as these cells were uniformly positive for cytoplasmatic IgL-λ and
expressed CD38 and CD138, both of which are typical for plasma
cells, but absent in WM. Pan-B-cell surface markers, CD19, CD20 and
CD22, which are characteristic of the typical immunophenotype of
WM, were negative. In addition, the expression of CD5, CD10, CD25,
CD27, CD56 and CD117 was negative, disproving the diagnosis of WM
(7). The pattern of
immunohistochemical staining for the bone marrow trephine biopsy
specimen also supported a diagnosis of IgM MM.
In conclusion, our case of IgM MM confirmed the
existence of this rare subtype of MM. Given the more aggressive
clinical course of patients with IgM MM, detailed immunophenotype
evaluation is critical when clinical and morphological features are
atypical.
References
|
1
|
Kyle RA and Rajkumar SV: Multiple myeloma.
Blood. 111:2962–2972. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rao PH, Cigudosa JC, Ning Y, et al:
Multicolor spectral karyotyping identifies new recurring
breakpoints and translocations in multiple myeloma. Blood.
92:1743–1748. 1998.PubMed/NCBI
|
|
3
|
De Gramont A, Grosbois B, Michaux JL, et
al: IgM myeloma: 6 cases and a review of the literature. Rev Med
Interne. 11:13–18. 1990.PubMed/NCBI
|
|
4
|
Dierlamm T, Laack E, Dierlamm J, Fiedler W
and Hossfeld DK: IgM myeloma: a report of four cases. Ann Hematol.
81:136–139. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tahan I, Seale J and Edwards D: IgM
multiple myeloma presenting with spinal cord compression caused by
a plasmacytoma: A case report. Cases J. 1:2072008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Annibali O, Petrucci MT, Del Bianco P, et
al: IgM multiple myeloma: report of four cases and review of the
literature. Leuk Lymphoma. 47:1565–1569. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vijay A and Gertz MA: Waldenstrom
macroglobulinemia. Blood. 109:5096–5103. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hewamana S, Pepper C, Couzens S, Thomas A
and Knapper S: IgM multiple myeloma: a diagnostic challenge in a
patient with coexisting chronic lymphocytic leukaemia. Int J
Hematol. 88:424–427. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Haghighi B, Yanagihara R and Cornbleet PJ:
IgM myeloma: case report with immunophenotypic profile. Am J
Hematol. 59:302–308. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Berman HH: Waldenstrom’s macroglobulinemia
with lytic osseous lesions and plasma-cell morphology. Report of a
case. Am J Clin Pathol. 63:397–402. 1975.
|
|
11
|
Feyler S, O’Connor SJ, Rawstron AC, et al:
IgM myeloma: a rare entity characterized by a CD20-CD56-CD117-
immuno-phenotype and the t(11;14). Br J Haematol. 140:547–551.
2008. View Article : Google Scholar : PubMed/NCBI
|