Introduction
Regenerating islet-derived family, member 4
(REG4, which encodes Reg IV) is a member of the REG
gene family, which constitutes a multi-gene family belonging to the
calcium-dependent lectin superfamily. REG4 was originally
identified by high-throughput sequence analysis of a large
inflammatory bowel disease cDNA library (1). Previously a serial analysis of gene
expression in four primary gastric cancer tissues was performed and
a number of gastric cancer-specific genes were identified (2,3). Of
these genes, REG4 is a candidate gene for cancer-specific
expression in patients with gastric cancer. Our previous
immunohistochemical analysis showed that Reg IV was expressed in
30% of gastric cancers and was associated with intestinal mucin
phenotype and neuroendocrine differentiation (4). A number of immunohistochemical
analyses of Reg IV have been reported in human cancers, including
lung, breast, pancreas, colorectal, prostate, salivary gland,
kidney, urinary bladder and gallbladder cancer (4–11).
These analyses indicate that Reg IV is expressed in adenocarcinoma
cells showing intestinal mucin differentiation. Reg IV staining
also aids in the diagnosis of gastrointestinal signet ring cell
carcinoma, a unique subtype of adenocarcinoma (12). By contrast, little is known about
Reg IV expression in other histological types of cancer, such as
squamous cell carcinoma (SCC).
In addition to adenocarcinoma, Reg IV expression has
been reported in neuroendocrine neoplasms, including
gastrointestinal and renal carcinoids (4,10,13).
Reg IV expression is also found in small cell carcinoma of the lung
(14). However, Reg IV expression
in small cell carcinoma of the esophagus has yet to be
investigated.
Reg IV is a secreted protein and a novel biomarker
for gastric cancer (15). The
diagnostic sensitivity of serum Reg IV was superior to that of
serum carcinoembryonic antigen or carbohydrate antigen 19-9. Serum
Reg IV serves as a tumor marker for colorectal, pancreatic and
prostate cancer (5,7,10). The
data support the hypothesis that Reg IV protein is a potentially
novel serum tumor marker for a wide range of malignancies. However,
the serum concentration of Reg IV in esophageal cancer has yet to
be measured.
In the present study, the expression and
distribution of Reg IV in human esophageal cancers, including SCC,
adenocarcinoma and small cell carcinoma, was examined by
immunohistochemistry. Previously two Reg IV staining patterns,
i.e., mucin-like and strong perinuclear staining were reported
(4). Mucin-like staining is
observed in goblet cells and goblet cell-like vesicles of cancer
cells. These cells are positive for MUC2 (a marker of goblet
cells). By contrast, strong perinuclear staining is detected in
neuroendocrine cells. These cells are positive for chromogranin A
(a marker of neuroendocrine cells). Therefore, the coexpression of
Reg IV and MUC2 or chromogranin A was examined. Additionally, the
Reg IV levels in sera from patients with esophageal cancer were
measured using an enzyme-linked immunosorbent assay (ELISA) to
investigate the potential diagnostic utility of Reg IV
measurement.
Materials and methods
Tissue samples
Primary tumor samples from 279 patients with
esophageal cancer (35 females and 244 males; age range 36–84 years,
mean 65) and serum samples from 65 patients with esophageal cancer
(8 females and 57 males; age range 49–82 years, mean 65) were
collected. The patients had undergone curative resection between
1990 and 2002 at Oita University Hospital, Oita, Japan. Only
patients without pre-operative radio- or chemotherapy and without
clinical evidence of distant metastasis were enrolled in the study.
The histologic classification was based on the World Health
Organization system. Tumor staging was performed according to the
TNM stage grouping system. For strict privacy protection,
identifying information for the samples was removed prior to being
analyzed in accordance with the Ethical Guidelines for Human
Genome/Gene Research enacted by the Japanese Government.
For quantitative reverse transcription-polymerase
chain reaction (RT-PCR), 10 primary esophageal cancer tissue
samples and their corresponding non-neoplastic mucosa samples were
used. The 10 esophageal cancer samples were all SCC. The samples
were obtained at the time of resection, immediately frozen in
liquid nitrogen and stored at −80°C until use. It was
microscopically confirmed that the tumor specimens consisted mainly
(>50%) of carcinoma tissue.
The 269 primary esophageal cancer tissue samples
were used for immunohistochemical analysis. The samples were
archival formalin-fixed, paraffin-embedded tissues. These 269
esophageal cancer samples were classified histologically as SCC
(n=255), adenocarcinoma (n=10) or small cell carcinoma (n=4).
Serum samples were used to measure Reg IV levels
using ELISA. All 65 serum samples were obtained from patients with
esophageal SCC prior to surgery and before initiation of therapy.
Primary esophageal SCC tissue samples from all 65 patients with
esophageal cancer were available for immunohistochemical analysis.
The control serum samples were obtained from 133 healthy
individuals (92 females and 41 males; age range 21–80 years, mean
51). Control subjects were randomly selected from individuals
visiting hospitals for regular health checks or due to certain
symptoms, such as appetite loss or epigastralgia. The control
subjects were confirmed to be free of malignancy by
gastrointestinal endoscopy and biopsy. The serum samples were
stored at −80°C until analysis.
Quantitative RT-PCR
Total RNA was extracted with an RNeasy mini kit
(Qiagen, Valencia, CA, USA) and 1 μg of total RNA was converted to
cDNA with a First Strand cDNA synthesis kit (Amersham Biosciences,
Piscataway, NJ, USA). Quantitation of REG4 mRNA levels was
performed by real-time fluorescence detection as previously
described (2). In brief, PCR was
performed with a SYBR-Green PCR Core Reagents kit (Applied
Biosystems, Foster City, CA, USA). Real-time detection of the
emission intensity of SYBR-Green bound to double-stranded DNA was
performed with an ABI PRISM 7700 Sequence Detection System (Applied
Biosystems) as previously described (16). ACTB-specific PCR products were
amplified from the same RNA samples and served as an internal
control.
Immunohistochemistry
Formalin-fixed, paraffin-embedded samples were
sectioned, deparaffinized and stained with hematoxylin and eosin to
ensure that the sectioned block contained tumor cells. Adjacent
sections were then stained immunohistochemically. The sections were
pre-treated by microwaving in citrate buffer for 30 min to retrieve
antigenicity. After peroxidase activity was blocked with 3%
H2O2-methanol for 10 min, the sections were
incubated with normal goat serum (Dako, Carpinteria, CA, USA) for
20 min to block non-specific antibody binding. The sections were
incubated with a primary antibody against Reg IV (rabbit polyclonal
antibody, diluted 1:50; anti-Reg IV antibody was raised and
characterized in our laboratory) (4), MUC2 (1:50; Novocastra, Newcastle, UK)
or chromogranin A (1:50; Novocastra) for 1 h at room temperature,
followed by incubation with peroxidase-labeled anti-rabbit or
anti-mouse IgG for 1 h. Staining was completed with a 10-min
incubation in a substrate-chromogen solution. The sections were
counterstained with 0.1% hematoxylin. The specificity of the Reg IV
antibody was previously characterized (4). Staining of each antibody was
considered positive if any tumor cells were stained.
Enzyme-linked immunosorbent assay
For the measurement of serum Reg IV concentration, a
sandwich ELISA method was developed as previously described
(15). First, polystyrene
microtiter plates were coated with mouse monoclonal anti-Reg IV
antibody (R&D Systems, Abingdon, UK) by overnight incubation of
50 μl/125 ng/well antibody diluted in Tris buffer (pH 7.4). The
plates were then washed three times with wash buffer. After the
plates were blocked with 1% milk in phosphate-buffered saline, 50
μl of recombinant Reg IV standard or sample was added to each well
and incubated overnight at 4°C. After three washes, 50 μl of
biotinylated goat polyclonal anti-Reg IV antibody (R&D Systems)
in assay buffer [1% bovine serum albumin (BSA), Tris buffer (pH
7.4) and 0.05% normal goat serum] was added to each well (75 ng
antibody/well). The mixture was then incubated for 1 h with
agitation at 37°C and washed three times with wash buffer. The
plates were incubated with 50 μl/well alkaline
phosphatase-conjugated streptavidin (Dako) diluted 1:2,000 in
diluent containing 1% BSA and Tris buffer (pH 7.4) for 1 h at 37°C
and washed three times. Color development was performed with the
addition of pNPP chromogenic substrate (Sigma-Aldrich, St. Louis,
MO, USA) followed by incubation at 37°C for 1 h. Absorbance at 405
nm was measured with an ELISA plate reader. As a reference
standard, known concentrations of human recombinant Reg IV from 0
to 30 ng/ml were tested in triplicate.
Statistical methods
Differences in the serum Reg IV concentration
between two groups were tested using the non-parametric
Mann-Whitney U test. Correlations between the serum Reg IV
concentration and age or gender were assessed using Spearman’s rank
correlation test. P<0.05 was considered to be statistically
significant.
Results
Expression of Reg IV in esophageal
cancer
An immunohistochemical analysis of Reg IV was
performed in 269 human esophageal cancer tissue samples. Although
esophageal SCC is the most frequent subtype of esophageal cancer in
Asian countries, no Reg IV staining was detected in any of the 255
esophageal SCC samples. Quantitative RT-PCR of REG4 was
performed in 10 esophageal SCC samples; however, no REG4
expression was found. By contrast, Reg IV was stained in 4 of 10
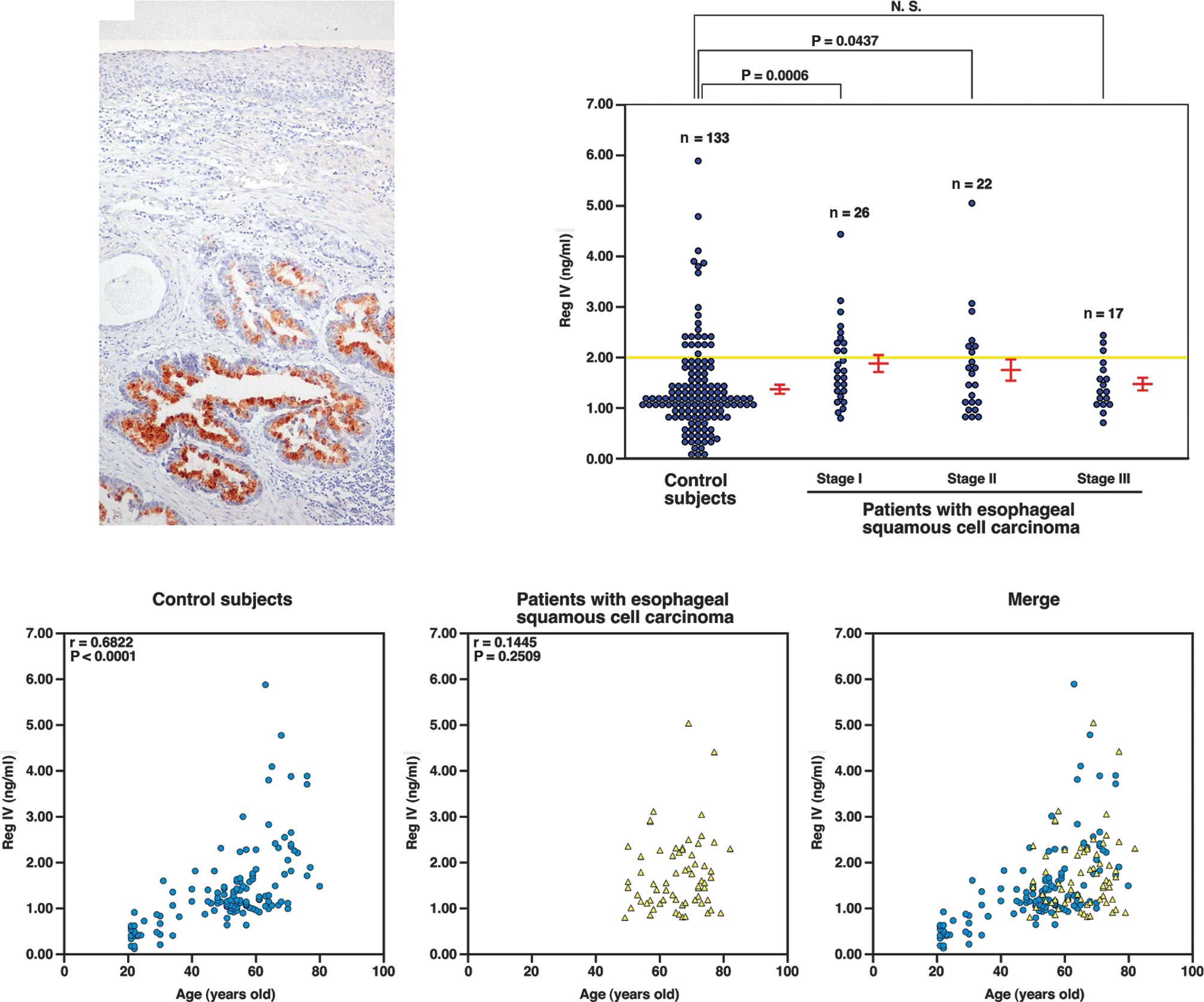
(40%) adenocarcinoma samples (Fig.
1A). The Reg IV staining was mucin-like; no perinuclear
staining was noted. It was confirmed that tumor cells showing
mucin-like staining of Reg IV were positive for MUC2 and negative
for chromogranin A (data not shown). Although extensive
chromogranin A staining was observed in the 4 samples of small cell
carcinoma, no Reg IV staining was found (data not shown). Reg IV
staining was also not found in corresponding non-neoplastic
squamous cells (Fig. 1A).
Serum Reg IV concentration in patients
with esophageal squamous cell carcinoma and control subjects
Serum Reg IV levels in 133 control subjects and 65
patients with esophageal SCC measured by ELISA are shown in
Fig. 1B. The serum Reg IV
concentration of control subjects measured in the present study
(mean ± SE, 1.38±0.08 ng/ml) was higher than that measured in our
previous study (0.52±0.05 ng/ml) (15). The correlation between the serum
concentration of Reg IV and age or gender was investigated.
Although the serum concentration of Reg IV did not correlate with
age in our previous study (15),
serum concentration was higher in elderly compared to that in young
control subjects. Spearman’s rank correlation test showed a
significant correlation between serum Reg IV and age (r=0.4362,
P<0.0001) (Fig. 1C). In our
previous study, the cut-off level for Reg IV was set at 2 ng/ml
(15). A high level of Reg IV
concentration was found in 13 of 23 (57%) control subjects who were
more than 65 years old.
Serum Reg IV concentration in esophageal SCC
patients at stage I (n=26, 1.88±0.16 ng/ml, P=0.0006, Mann-Whitney
U test) and stage II (n=22, 1.76±0.21 ng/ml, P=0.0437, Mann-Whitney
U test) was significantly higher than that of the control subjects
(Fig. 1B). By contrast, the serum
Reg IV concentration in esophageal SCC patients at stage III was
not significantly elevated (n=17, 1.48±0.11 ng/ml, P=0.1329,
Mann-Whitney U test). In total, serum Reg IV concentration in
esophageal SCC patients (n=65, 1.74±0.10 ng/ml) was significantly
higher compared to that of the control subjects (P=0.0003,
Mann-Whitney U test).
In the present study, no Reg IV expression was
detected in esophageal SCC by quantitative RT-PCR and
immunohistochemistry. However, serum Reg IV concentration in
esophageal SCC patients was significantly higher compared to that
of the control subjects. Discrepancy between immunostaining and
ELISA results is not likely due only to methodological differences.
Spearman’s rank correlation test showed that there was no
significant correlation between serum Reg IV concentration in
esophageal SCC patients and age (r=0.1445, P=0.2509) (Fig. 1D). Additionally, when the
distribution of serum Reg IV concentration in esophageal SCC
patients was compared to that of the control subjects, it was not
significantly different (Fig.
1E).
Discussion
This study aimed to investigate the expression of
Reg IV in esophageal cancer. Although Reg IV staining was not
detected in esophageal SCC and small cell carcinoma samples, it was
present in 40% of adenocarcinoma samples. We confirmed that the
adenocarcinoma cells were also positive for MUC2. In our previous
study, Reg IV expression was not found in renal cell carcinoma and
was noted in only 1% of urothelial carcinoma, neither of which are
adenocarcinomas (10). Taken
together, these results indicate that the expression of Reg IV is
highly specific for adenocarcinoma.
Although Reg IV expression was not found in
esophageal SCC at the mRNA and protein levels, serum Reg IV
concentrations in esophageal SCC patients at stages I and II were
significantly higher compared to those of the control subjects.
Spearman’s rank correlation test showed a significant correlation
between serum Reg IV and age in control subjects. In the ELISA
analysis, the mean age of the control subjects (51 years) was
younger than that of patients with esophageal SCC (65 years),
suggesting that the elevation of the serum concentration of Reg IV
in esophageal SCC is age-related and not due to esophageal SCC.
Notably, the distribution of serum Reg IV concentration in
esophageal SCC patients did not show a significant difference from
that noted in the control subjects.
We are unable to thoroughly explain this age-related
elevation of serum Reg IV concentration. A number of lines of
evidence have suggested that Reg IV protein detected in serum
samples is derived from cancer cells. In pancreatic adenocarcinoma
patients, postoperative serum Reg IV levels were reduced to within
normal range 3 or 4 weeks following tumor resection (5). The Reg IV concentration in serum
samples from patients with gastric cancer showing Reg IV-positive
immunostaining was significantly higher compared to that with
gastric cancer showing Reg IV-negative immunostaining (15). Although the control subjects were
confirmed to be free of malignancy by gastrointestinal endoscopy
and biopsy, the possibility that the control subjects had cancer
cannot be excluded. To address these issues, serum samples from
cancer-free subjects confirmed by autopsy should be analyzed.
Another possible explanation for the age-related
elevation of serum Reg IV concentration is Reg IV expression in
intestinal metaplasia of the stomach. In our previous study, normal
stomach cells were not stained by Reg IV, however, extensive
staining of Reg IV was observed in intestinal metaplasia of the
stomach (4). Since the incidence
and prevalence of intestinal metaplasia of the stomach increase
with age, age-related elevation of serum Reg IV concentration may
be due to Reg IV expression in intestinal metaplasia of the
stomach.
In conclusion, we showed that the expression of Reg
IV is highly specific for adenocarcinoma, but is not specific for
SCC or small cell carcinoma. Although serum Reg IV concentration in
esophageal SCC patients was significantly higher than that in
control subjects, we hypothesize that serum Reg IV is not suitable
as a tumor marker for esophageal SCC detection. The reason for the
apparent age-related elevation of serum Reg IV concentration in
esophageal SCC patients has yet to be elucidated and further
investigation is required to clarify the potential utility of serum
Reg IV measurement.
Acknowledgements
We thank Mr. Shinichi Norimura for the excellent
technical assistance and advice. This study was carried out with
the kind cooperation of the Research Center for Molecular Medicine,
Faculty of Medicine, Hiroshima University. We thank the Analysis
Center of Life Science, Hiroshima University, for the use of their
facilities. This study was supported in part by Grants-in-Aid for
Cancer Research from the Ministry of Education, Culture, Science,
Sports and Technology of Japan, and from the Ministry of Health,
Labor and Welfare of Japan.
References
|
1
|
Hartupee JC, Zhang H, Bonaldo MF, Soares
MB and Dieckgraefe BK: Isolation and characterization of a cDNA
encoding a novel member of the human regenerating protein family:
Reg IV. Biochim Biophys Acta. 1518:287–293. 2001. View Article : Google Scholar
|
|
2
|
Oue N, Hamai Y, Mitani Y, Matsumura S,
Oshimo Y, Aung PP, Kuraoka K, Nakayama H and Yasui W: Gene
expression profile of gastric carcinoma: identification of genes
and tags potentially involved in invasion, metastasis, and
carcinogenesis by serial analysis of gene expression. Cancer Res.
64:2397–2405. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aung PP, Oue N, Mitani Y, Nakayama H,
Yoshida K, Noguchi T, Bosserhoff AK and Yasui W: Systematic search
for gastric cancer-specific genes based on SAGE data: melanoma
inhibitory activity and matrix metalloproteinase-10 are novel
prognostic factors in patients with gastric cancer. Oncogene.
25:2546–2557. 2006. View Article : Google Scholar
|
|
4
|
Oue N, Mitani Y, Aung PP, Sakakura C,
Takeshima Y, Kaneko M, Noguchi T, Nakayama H and Yasui W:
Expression and localization of Reg IV in human neoplastic and
non-neoplastic tissues: Reg IV expression is associated with
intestinal and neuroendocrine differentiation in gastric
adenocarcinoma. J Pathol. 207:185–198. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Takehara A, Eguchi H, Ohigashi H, Ishikawa
O, Kasugai T, Hosokawa M, Katagiri T, Nakamura Y and Nakagawa H:
Novel tumor marker REG4 detected in serum of patients with
resectable pancreatic cancer and feasibility for antibody therapy
targeting REG4. Cancer Sci. 97:1191–1197. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Nakata K, Nagai E, Ohuchida K, Aishima S,
Hayashi A, Miyasaka Y, Yu J, Mizumoto K, Tanaka M and Tsuneyoshi M:
REG4 is associated with carcinogenesis in the ‘intestinal’ pathway
of intraductal papillary mucinous neoplasms. Mod Pathol.
22:460–468. 2009.
|
|
7
|
Oue N, Kuniyasu H, Noguchi T, Sentani K,
Ito M, Tanaka S, Setoyama T, Sakakura C, Natsugoe S and Yasui W:
Serum concentration of Reg IV in patients with colorectal cancer:
overexpression and high serum levels of Reg IV are associated with
liver metastasis. Oncology. 72:371–380. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ohara S, Oue N, Matsubara A, Mita K,
Hasegawa Y, Hayashi T, Usui T, Amatya VJ, Takeshima Y, Kuniyasu H
and Yasui W: Reg IV is an independent prognostic factor for relapse
in patients with clinically localized prostate cancer. Cancer Sci.
99:1570–1577. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sasahira T, Oue N, Kirita T, Luo Y, Bhawal
UK, Fujii K, Yasui W and Kuniyasu H: Reg IV expression is
associated with cell growth and prognosis of adenoid cystic
carcinoma in the salivary gland. Histopathology. 53:667–675. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hayashi T, Matsubara A, Ohara S, Mita K,
Hasegawa Y, Usui T, Arihiro K, Norimura S, Sentani K, Oue N and
Yasui W: Immunohistochemical analysis of Reg IV in urogenital
organs: Frequent expression of Reg IV in prostate cancer and
potential utility as serum tumor marker. Oncol Rep. 21:95–100.
2009.
|
|
11
|
Tamura H, Ohtsuka M, Washiro M, Kimura F,
Shimizu H, Yoshidome H, Kato A, Seki N and Miyazaki M: Reg IV
expression and clinicopathologic features of gallbladder carcinoma.
Hum Pathol. 40:1686–1692. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sentani K, Oue N, Tashiro T, Sakamoto N,
Nishisaka T, Fukuhara T, Taniyama K, Matsuura H, Arihiro K, Ochiai
A and Yasui W: Immunohistochemical staining of Reg IV and
claudin-18 is useful in the diagnosis of gastrointestinal signet
ring cell carcinoma. Am J Surg Pathol. 32:1182–1189. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sentani K, Oue N, Noguchi T, Sakamoto N,
Matsusaki K and Yasui W: Immunostaining of gastric cancer with
neuroendocrine differentiation: Reg IV-positive neuroendocrine
cells are associated with gastrin, serotonin, pancreatic
polypeptide and somatostatin. Pathol Int. 60:291–297. 2010.
View Article : Google Scholar
|
|
14
|
Heiskala K, Arola J, Heiskala M and
Andersson LC: Expression of Reg IV and Hath1 in neuroendocrine
neoplasms. Histol Histopathol. 25:63–72. 2010.PubMed/NCBI
|
|
15
|
Mitani Y, Oue N, Matsumura S, Yoshida K,
Noguchi T, Ito M, Tanaka S, Kuniyasu H, Kamata N and Yasui W: Reg
IV is a serum biomarker for gastric cancer patients and predicts
response to 5-fluorouracil-based chemotherapy. Oncogene.
26:4383–4393. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kondo T, Oue N, Yoshida K, Mitani Y, Naka
K, Nakayama H and Yasui W: Expression of POT1 is associated with
tumor stage and telomere length in gastric carcinoma. Cancer Res.
64:523–529. 2004. View Article : Google Scholar : PubMed/NCBI
|