Introduction
Bladder cancer (BC), the incidence and mortality of
which increases directly with age, is a heterogeneous disease that
affects approximately 68,000 people in the United States annually
(1). In Korea, BC is the second
most common urological malignancy and is about five times more
common in male as compared to female individuals (2). Patients diagnosed with non-muscle
invasive bladder cancers (NMIBC) may have indolent, albeit
recurrent, disease. However, NMIBC patients are required to receive
frequent cystourethroscopy, which is inconvenient for patients.
Additionally, they may experience progression to muscle invasive
bladder cancer (MIBC), which potentially has a narrow
window-of-cure and requires aggressive treatment (3). Therefore, predicting the course of the
disease is of great value to both patients and urologists, in order
for adequate management of NMIBC to occur. For example, early
radical cystectomy has a superior 5-year survival rate compared to
bladder-sparing surgery (4). The
development of accurate and reliable biological markers would be
useful for assessing aggressiveness and for predicting the
prognosis of NMIBC.
Previously, we undertook a microarray analysis of
specimens derived from 103 primary NMIBC patients and identified an
eight-gene progression-related gene classifier (5). Although there have been numerous
attempts to establish prognostic markers for NMIBC (3,6–8), the
limited value of current markers means that new predictive
indicators of BC outcome are urgently required. Due to the
molecular and cellular heterogeneity of most cancers, and the
subsequent variability in biological behavior, a single pathway or
gene marker, may have inherent limitations in terms of predicting
cancer outcome.
In this study, three genes were selected to yield a
signature not previously described for BC: the cadherin EGF LAG
seven-pass G-type receptor 3 (CELSR3), kinesin family member
1A (KIF1A) and coagulation factor C homolog (COCH).
Using quantitative real-time PCR (qPCR), the up-regulated
expression of the mRNA for these genes was shown to be associated
with disease progression. The relationship between this three-gene
signature and NMIBC outcomes was investigated using data obtained
from a previous study population and from new cases, all with an
extended follow-up period.
Materials and methods
Patients
A total of 193 primary NMIBC patients with
transitional cell carcinoma of the urinary bladder treated with
transurethral resection (TUR) between 1995 and 2008 were eligible
for inclusion in the present study. A minimum follow-up period of 6
months was required (unless recurrence and/or progression occurred
prior to this 6-month period). To make the study population more
homogeneous, patients with concomitant carcinoma in situ
(CIS) and those who had undergone radical cystectomy were excluded.
All tumors were macrodissected, typically within 15 min of surgical
resection. Each BC specimen was confirmed by a pathological
analysis of fresh frozen sections obtained from part of the TUR
tissue samples. Samples were then frozen in liquid nitrogen and
stored at −80°C until required. The collection and analysis of all
samples was approved by the local institutional review board and
informed consent was obtained from each subject.
A second TUR was performed 2–4 weeks after the
initial resection if a BC specimen did not include proper muscle
tissue, or when a high-grade tumor was detected (9). Patients with a T1 tumor, multiple
tumors, large tumors (≥3 cm in diameter), or a high-grade Ta tumor
received one cycle of intravesical treatment (BCG or mitomycin-C)
(9,10). If a patient refused intravesical
therapy, it was not administered after TUR. Response to treatment
was assessed by cystoscopy and urinary cytology. Patients who were
disease-free within 3 months after treatment were assessed every 3
months for the first 2 years and every 6 months thereafter
(9,10). Tumors were staged and graded
according to the 2002 TNM classification and the 1973 WHO grading
system, respectively (9,11). Recurrence was defined as relapse of
the primary NMIBC with a lower, or the same, pathological stage,
and progression was defined as disease with a higher TNM stage upon
relapse.
RNA extraction and construction of
cDNA
RNA was isolated from tissue using 1 ml of TRIzol
reagent (Invitrogen, Carlsbad, CA, USA) and homogenized in a 5 ml
glass tube. The homogenate was transferred to a 1.5 ml tube and
mixed with 200 μl of chloroform. After incubation for 5 min at 4°C,
the homogenate was centrifuged for 13 min at 13,000 × g at 4°C. The
upper aqueous phase was transferred to a clean tube and then 500 μl
of isopropanol was added. The mixture was incubated for 60 min at
4°C, and the tube was centrifuged for 8 min at 13,000 × g at 4°C.
The upper aqueous phase was discarded and mixed with 500 μl of 75%
ethanol, and centrifuged for 5 min at 13,000 × g at 4°C. After
discarding the upper aqueous layer, the pellet was dried at room
temperature, dissolved in diethylpyrocarbonate (DEPC)-treated
water, and then stored at −80°C. The quality and integrity of the
RNA were confirmed by agarose gel electrophoresis and ethidium
bromide staining followed by visual inspection under ultraviolet
light. cDNA was prepared from 1 μg of total-RNA using a
First-Strand cDNA Synthesis kit (Amersham Biosciences Europe GmbH,
Freiburg, Germany) according to the manufacturer's
instructions.
Quantitative real-time PCR
qPCR amplification was performed using a Rotor-Gene
6000 instrument (Corbett Research, Mortlake, Australia) to quantify
the expression of CELSR3, KIF1A and COCH. qPCR
assays were carried out in micro-reaction tubes (Corbett Research)
using SYBR-Premix Ex Taq (Takara, Otsu, Japan). The primers used in
the amplification were: CELSR3 (129 bp), sense 5′-CTC CAT
GTT GGT GAC TGT CAC-3′ and antisense 5′-TCC TGC CAC ATG TTC TCA
AG-3′; KIF1A (157 bp), sense 5′-AAG AAC CAA GGG CAA CCT
TCG-3′ and antisense 5′-CTC CAT TCA TGT TGG TGG CC-3′; COCH
(134 bp), sense 5′-AGA AAG CAG ATG TCC TCT GC-3′ and antisense
5′-TCC CCC TGA GTT GCT GAT TA-3′. The PCR reaction was performed in
a final volume of 10 μl consisting of 5 μl of 2X SYBR-Premix Ex Taq
buffer, 0.5 μl each of 5′- and 3′-primer (10 pmol/μl), and 1 μl of
the cDNA sample. The product was purified with a QIAquick
Extraction kit (Qiagen, Hilden, Germany), quantified with a
spectrophotometer (Perkin Elmer MBA2000, Fremont, CA, USA), and
then sequenced with an automated laser fluorescence sequencer (ABI
PRISM 3100 Genetic Analyzer, Foster City, WI, USA). Ten-fold serial
dilutions of a known concentration of the product (from 100 to 0.1
pg/μl) were used to establish the standard curve for qPCR. The qPCR
conditions were: 1 cycle for 20 sec at 96°C, followed by 40 cycles
of 2 sec at 96°C for denaturation, 15 sec at 60°C for annealing,
and 15 sec at 72°C for extension. The melting program was performed
at 72–95°C with a heating rate of 1°C per 45 sec. Spectral data
were captured and analyzed using Rotor-Gene Real-Time Analysis
Software 6.0 Build 14 (Corbett Research). All of the samples were
run in triplicate. Glyceraldehyde-3-phosphate dehydrogenase
(GAPDH) was analyzed as an endogenous RNA reference gene and
gene expression was normalized to the expression of
GAPDH.
Statistical analysis
Data from the three genes were natural
log-transformed to normalize the highly skewed distribution of mRNA
expression levels (12), and a risk
score for recurrence and progression was calculated for each
patient (the sum of the levels of expression of each gene
multiplied by the corresponding regression coefficients) (5,13–18).
Receiver operating characteristic (ROC) curves were used to
determine the optimal cut-off point for each risk score that
yielded the highest combined sensitivity and specificity for
recurrence and progression, respectively. Using these values,
patients were classified into high- or low-risk signature groups.
The Kaplan-Meier method was used to estimate time-to-recurrence and
progression, and differences were assessed using log-rank
statistics. The prognostic value of the three-gene risk signature,
in terms of recurrence and progression, was analyzed using
multivariate Cox proportional hazard regression models. Statistical
analysis was performed using SPSS 12.0 software (SPSS, Chicago, IL,
USA). P<0.05 was considered to be statistically significant.
Results
Baseline characteristics
The median follow-up period after surgery was 44.9
months (range 6.1–194.5) and the median age was 67.0 years (range
24.0–91.0). Of the 193 patients, 71 (36.8%) experienced recurrence
and 20 (10.4%) experienced progression. The mean intervals for
recurrence and progression were 41.2 months (median 22.1; range
1.4–164.4) and 55.3 months (median 44.9; range 6.1–194.5),
respectively. Other clinical and pathological characteristics of
the patients are shown in Table
I.
 | Table IBaseline characteristics of primary
non-muscle invasive bladder cancer patients. |
Table I
Baseline characteristics of primary
non-muscle invasive bladder cancer patients.
| Variables | No. of patients
(%) |
|---|
| Age (years), median
(range) | 67.0
(24.0–91.0) |
| Median follow-up in
months (range) | 44.9
(6.1–194.5) |
| Gender |
| Male | 157 (81.3) |
| Female | 36 (18.7) |
| Grade |
| G1 | 67 (34.7) |
| G2 | 101 (52.3) |
| G3 | 25 (13.0) |
| Stage |
| Ta | 71 (36.8) |
| T1 | 122 (63.2) |
| Size |
| <3 cm | 109 (56.5) |
| ≥3 cm | 84 (43.5) |
| Number |
| Single | 111 (57.5) |
| Multiple | 82 (43.5) |
| Intravesical
therapy |
| No | 80 (41.5) |
| Yes | 113 (58.5) |
Prognostic value of three-gene risk
signature for recurrence and progression
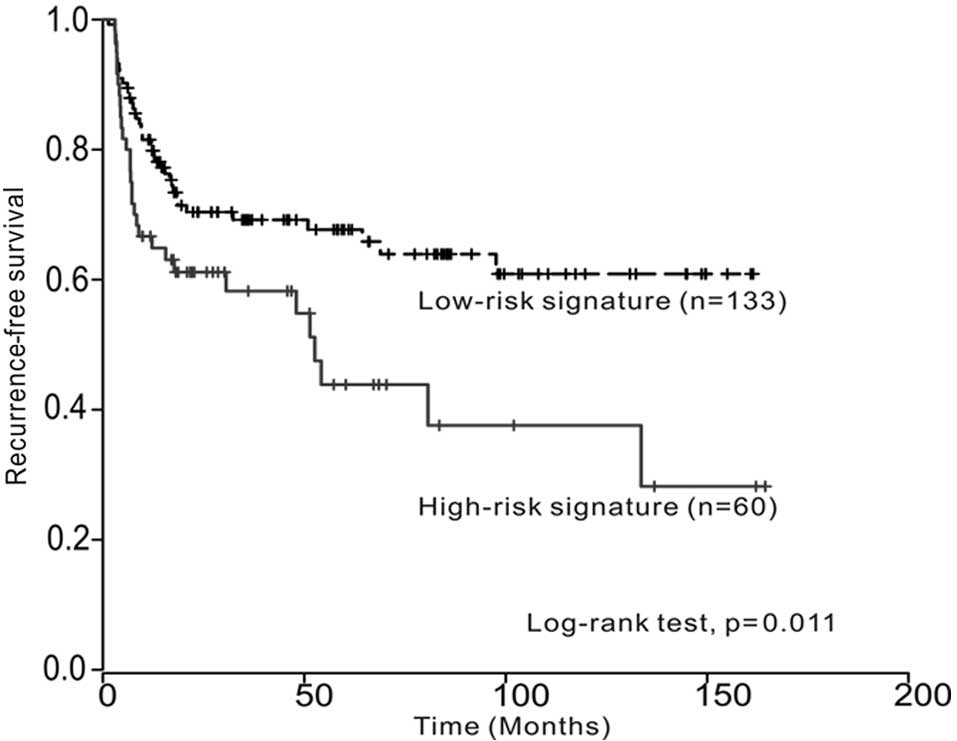
Kaplan-Meier estimates revealed significant
differences in time-to-recurrence and progression between low- and
high-risk signatures (log-rank test, p=0.011 and p<0.001,
respectively) (Fig. 1A and B). The
multivariate Cox regression analysis revealed that the three-gene
signature was an independent predictor of bladder tumor progression
(hazard ratio, 4.268; 95% CI, 1.542–11.814; p=0.005) (Table II). However, the multivariate
survival analysis showed that the three-gene signature was not an
independent predictor of tumor recurrence.
| Table IIMultivariate Cox regression analysis
for the prediction of recurrence and progression in
non-muscle-invasive bladder cancer. |
Table II
Multivariate Cox regression analysis
for the prediction of recurrence and progression in
non-muscle-invasive bladder cancer.
| Variables | Recurrence | Progression |
|---|
|
|
|
|---|
| HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (<67 vs. ≥67
years) | 1.018
(0.617–1.680) | 0.943 | 1.075
(0.410–2.819) | 0.883 |
| Gender (male vs.
female) | 0.954
(0.481–1.895) | 0.894 | 0.763
(0.170–3.433) | 0.724 |
| Grade |
| G1 | 1 | - | 1 | - |
| G2 | 1.038
(0.527–2.044) | 0.915 | 1.152
(0.280–4.740) | 0.844 |
| G3 | 1.110
(0.449–2.746) | 0.821 | 3.240
(0.504–20.834) | 0.216 |
| Number of tumors
(single vs. multiple) | 1.115
(0.680–1.830) | 0.666 | 1.108
(0.454–2.700) | 0.822 |
| Tumor size (<3
vs. ≥3 cm) | 1.152
(0.709–1.873) | 0.567 | 2.428
(0.904–6.526) | 0.079 |
| Stage (Ta vs.
T1) | 0.961
(0.481–1.895) | 0.905 | 0.644
(0.174–2.390) | 0.511 |
| Intravesical
therapy (No vs. Yes) | 2.646
(1.397–5.014) | 0.003 | 2.195
(0.574–8.397) | 0.251 |
| Three-gene risk
signature (low vs. high) | 1.519
(0.926–2.493) | 0.098 | 4.268
(1.542–11.814) | 0.005 |
Discussion
Our experimental approach was based on an initial
microarray gene expression analysis of 103 randomly selected
primary NMIBC specimens (5). The
number of NMIBC samples was progressively increased and three genes
not previously described in BC were selected. Specifically,
patients designated as high-risk by the three-gene signature were
more likely to show progression of NMIBC, had a strong hazard ratio
(4.268) following multivariate analysis, and had various known
clinical risk factors, including age, tumor size, number of tumors,
T-category, tumor grade and intravesical therapy. This result
provided evidence that a gene signature was able to provide
additional risk stratification beyond pathology, which is
particularly useful due to the inter-observer variability inherent
in tumor staging and grading (19,20).
CELSR3 is a member of the flamingo protein
subfamily, which is part of the cadherin superfamily. The flamingo
cadherins comprise nine cadherin domains, seven epidermal growth
factor-like repeats and two laminin AG-type repeats within the
ectodomain (21). Using microarray
analysis, Erkan et al reported that CELSR3 was
up-regulated in tumor-associated stellate cells compared with
inflammation-associated ones. These data were confirmed by mRNA
expression, immunoblot analysis, and tissue immunohistochemistry
(22). The authors suggested that
the up-regulation of CELSR3 in tumors provides a potential
drug target, since the protein encoded by this gene is located at
the plasma membrane and has noteworthy signaling capabilities
(23). It is postulated that these
proteins are receptors involved in contact-mediated communication,
with the cadherin domains acting as homophilic binding regions and
the EGF-like domains involved in cell adhesion and receptor-ligand
interactions. Taken together, these data suggest a significant role
for CELSR3 in BC that warrants further investigation.
KIF1A, located on chromosome 2q37, is a member of the
kinesin superfamily of motor proteins. This protein is an
anterograde motor protein that transports membranous organelles
along the axonal microtubules and is extremely similar to the mouse
heavy chain kinesin member 1A (KHC) protein (24,25).
In the mouse colon, KHC transports the APC protein along
microtubules. The suppression of KHC expression eliminates the
peripheral translocation of APC and induces the cellular
accumulation of β-catenin, leading to malignant transformation
(26). The altered expression of
KIF1A and other kinesin superfamily genes has been reported
in a variety of human cancers including breast, glioblastoma, and
prostate cancer (27–29). A recent study reported that
KIF1A showed significant differences in plasma DNA
methylation between control and patient samples in lung cancer and
suggested a significant potential of molecular detection approaches
(30). COCH is a cell
adhesion molecule (31) that maps
to human chromosome 14q11.2–13 (32), and is linked with non-syndromic,
autosomal dominant hearing loss due to vestibular malfunction with
variable penetrance. However, the cancer-related functions of
COCH have yet to be demonstrated. Only one report links
COCH to cancer, and suggests that it is regulated by
leukemia inhibitory factor in the uterus at the time of embryo
implantation (33).
Frequent recurrence and progression are devastating
events for both urologists and BC patients. As a result, there have
been various efforts to develop methods for detecting and
predicting the biological behavior of BC. The methods used for
evaluation should be convenient and adequate for patients as well
as urologists. Economic problems also have to be considered with
respect to BC patients, as the high incidence of recurrence results
in considerable costs, which render NMIBC one of the most expensive
diseases to treat (34).
Progression from NMIBC to MIBC, or metastasis, is not uncommon and
is often life-threatening. Efforts geared towards preventing these
events are ongoing. Conventional methods include a second TUR,
intravesical drug instillation treatment, and early cystectomy
(35,36). However, the compliance of patients
treated with intravesical drug instillation is poor and cystectomy
may lead to severe complications or morbidity (37). On the other hand, the use of the
three-gene signature in a clinical setting is beneficial in that
management of numerous NMIBC patients is feasible. Therefore,
obtaining information regarding disease aggressiveness at the time
of initial diagnosis is possible. Assessment of the true malignant
potential of NMIBC at the time of diagnosis may change the current
schedule of treatment. For instance, it may prioritize high-risk
patients for early cystectomy, or urgent cystoscopy, and may delay
or prolong the interval between examinations for low-risk patients,
thereby improving patient quality of life and outcome.
Additionally, this method may be cost-effective for BC patients as
compared to microarray analysis or a panel of markers,
simultaneously overcoming the limitations of single marker analysis
and the current stage-grading system.
The exact mechanism underlying the progression of
NMIBC driven by the three genes remains to be elucidated.
Investigation of these mechanisms may be the subject of future
studies. The three-gene signature we identified can be applied
clinically. Predictive models, including or excluding any new
putative biomarkers, need to show clinically significant
improvements in performance to claim any real benefit.
Consequently, we are currently recruiting a larger cohort of BC
patients and using long-term follow-up periods in an independent
cohort.
In conclusion, this study shows that our three-gene
signature is capable of predicting the prognosis of NMIBC and is
closely associated with disease progression. Utilization of this
technique in clinical practice is likely to improve the follow-up
schedule of NMIBC patients. However, introducing this prognostic
test for NMIBC into routine clinical practice requires further
external validation in a prospective manner using a large number of
samples.
Acknowledgements
The present study was supported by the Basic Science
Research Program through the National Research Foundation of Korea
(NRF) funded by the Ministry of Education, Science and Technology
(2010-0001730).
Abbreviations:
|
BC
|
bladder cancer
|
|
NMIBC
|
non-muscle invasive bladder cancer
|
|
MIBC
|
muscle invasive bladder cancer
|
|
CELSR3
|
cadherin EGF LAG seven-pass G-type
receptor 3
|
|
KIF1A
|
kinesin family member 1A
|
|
COCH
|
coagulation factor C homolog
|
|
qPCR
|
quantitative real-time PCR
|
|
TUR
|
transurethral resection
|
|
CIS
|
carcinoma in situ
|
|
GAPDH
|
glyceraldehyde-3-phosphate
dehydrogenase
|
References
|
1
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J,
Murray T and Thun MJ: Cancer statistics. CA Cancer J Clin.
58:71–96. 2008.
|
|
2
|
Ha YS, Kim MJ, Yoon HY, Kang HW, Kim YJ,
Yun SJ, Lee SC and Kim WJ: mRNA expression of S100A8 as a
prognostic marker for progression of non-muscle-invasive bladder
cancer. Korean J Urol. 51:15–20. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sylvester RJ, van der Meijden AP,
Oosterlinck W, Witjes JA, Bouffioux C, Denis L, Newling DW and
Kurth K: Predicting recurrence and progression in individual
patients with stage Ta T1 bladder cancer using EORTC risk tables: a
combined analysis of 2596 patients from seven EORTC trials. Eur
Urol. 49:S466–S477. 2006. View Article : Google Scholar
|
|
4
|
Borden LS Jr, Clark PE and Hall MC:
Bladder cancer. Curr Opin Oncol. 15:227–233. 2003. View Article : Google Scholar
|
|
5
|
Kim WJ, Kim EJ, Kim SK, Kim YJ, Ha YS,
Jeong P, Kim MJ, Yun SJ, Lee KM, Moon SK, Lee SC, Cha EJ and Bae
SC: Predictive value of progression-related gene classifier in
primary non-muscle invasive bladder cancer. Mol Cancer. 9:32010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shariat SF, Zippe C, Ludecke G, et al:
Nomograms including nuclear matrix protein 22 for prediction of
disease recurrence and progression in patients with Ta, T1 or CIS
transitional cell carcinoma of the bladder. J Urol. 173:1518–1525.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hong SJ, Cho KS, Han M, Rhew HY, Kim CS,
Ryu SB, Sul CK, Chung MK, Park TC and Kim HJ: Nomograms for
prediction of disease recurrence in patients with primary Ta, T1
transitional cell carcinoma of the bladder. J Korean Med Sci.
23:428–433. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Habuchi T, Marberger M, Droller MJ,
Hemstreet GP III, Grossman HB, Schalken JA, Schmitz-Drager BJ,
Murphy WM, Bono AV, Goebell P, Getzenberg RH, Hautmann SH, Messing
E, Fradet Y and Lokeshwar VB: Prognostic markers for bladder
cancer: International Consensus Panel on bladder tumor markers.
Urology. 66:64–74. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Babjuk M, Oosterlinck W, Sylvester R,
Kaasinen E, Bohle A and Palou-Redorta J: EAU guidelines on
non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol.
54:303–314. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hall MC, Chang SS, Dalbagni G, Pruthi RS,
Seigne JD, Skinner EC, Wolf JS Jr and Schellhammer PF: Guideline
for the management of nonmuscle invasive bladder cancer (stages Ta,
T1, and Tis): 2007 update. J Urol. 178:2314–2330. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Greene FL: The american joint committee on
cancer: updating the strategies in cancer staging. Bull Am Coll
Surg. 87:13–15. 2002.PubMed/NCBI
|
|
12
|
Bland JM and Altman DG: Transformations,
means, and confidence intervals. BMJ. 312:10791996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kim YJ, Ha YS, Kim SK, Yoon HY, Lym MS,
Kim MJ, Moon SK, Choi YH and Kim WJ: Gene signatures for the
prediction of response to Bacillus Calmette-Guerin immunotherapy in
primary pT1 bladder cancers. Clin Cancer Res. 16:2131–2137. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen HY, Yu SL, Chen CH, Chang GC, Chen
CY, Yuan A, Cheng CL, Wang CH, Terng HJ, Kao SF, Chan WK, Li HN,
Liu CC, Singh S, Chen WJ, Chen JJ and Yang PC: A five-gene
signature and clinical outcome in non-small-cell lung cancer. N
Engl J Med. 356:11–20. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lossos IS, Czerwinski DK, Alizadeh AA,
Wechser MA, Tibshirani R, Botstein D and Levy R: Prediction of
survival in diffuse large-B-cell lymphoma based on the expression
of six genes. N Engl J Med. 350:1828–1837. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Beer DG, Kardia SL, Huang CC, Giordano TJ,
Levin AM, Misek DE, Lin L, Chen G, Gharib TG, Thomas DG, Lizyness
ML, Kuick R, Hayasaka S, Taylor JM, Iannettoni MD, Orringer MB and
Hanash S: Gene-expression profiles predict survival of patients
with lung adenocarcinoma. Nat Med. 8:816–824. 2002.PubMed/NCBI
|
|
17
|
Skrzypski M, Jassem E, Taron M, Sanchez
JJ, Mendez P, Rzyman W, Gulida G, Raz D, Jablons D, Provencio M,
Massuti B, Chaib I, Perez-Roca L, Jassem J and Rosell R: Three-gene
expression signature predicts survival in early-stage squamous cell
carcinoma of the lung. Clin Cancer Res. 14:4794–4799. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Paik S, Shak S, Tang G, Kim C, Baker J,
Cronin M, Baehner FL, Walker MG, Watson D, Park T, Hiller W, Fisher
ER, Wickerham DL, Bryant J and Wolmark N: A multigene assay to
predict recurrence of tamoxifen-treated, node-negative breast
cancer. N Engl J Med. 351:2817–2826. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bol MG, Baak JP, Buhr-Wildhagen S, Kruse
AJ, Kjellevold KH, Janssen EA, Mestad O and Ogreid P:
Reproducibility and prognostic variability of grade and lamina
propria invasion in stages Ta, T1 urothelial carcinoma of the
bladder. J Urol. 169:1291–1294. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Murphy WM, Takezawa K and Maruniak NA:
Interobserver discrepancy using the 1998 World Health
Organization/International Society of Urologic Pathology
classification of urothelial neoplasms: practical choices for
patient care. J Urol. 168:968–972. 2002. View Article : Google Scholar
|
|
21
|
Wu Q and Maniatis T: Large exons encoding
multiple ectodomains are a characteristic feature of protocadherin
genes. Proc Natl Acad Sci USA. 97:3124–3129. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Erkan M, Weis N, Pan Z, Schwager C,
Samkharadze T, Jiang X, Wirkner U, Giese NA, Ansorge W, Debus J,
Huber PE, Friess H, Abdollahi A and Kleeff J: Organ-, inflammation-
and cancer specific transcriptional fingerprints of pancreatic and
hepatic stellate cells. Mol Cancer. 9:882010. View Article : Google Scholar
|
|
23
|
Katoh M: WNT/PCP signaling pathway and
human cancer (Review). Oncol Rep. 14:1583–1588. 2005.PubMed/NCBI
|
|
24
|
Hirokawa N: Kinesin and dynein superfamily
proteins and the mechanism of organelle transport. Science.
279:519–526. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Aizawa H, Sekine Y, Takemura R, Zhang Z,
Nangaku M and Hirokawa N: Kinesin family in murine central nervous
system. J Cell Biol. 119:1287–1296. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cui H, Dong M, Sadhu DN and Rosenberg DW:
Suppression of kinesin expression disrupts adenomatous polyposis
coli (APC) localization and affects beta-catenin turnover in young
adult mouse colon (YAMC) epithelial cells. Exp Cell Res. 280:12–23.
2002. View Article : Google Scholar
|
|
27
|
Ostrow KL, Park HL, Hoque MO, Kim MS, Liu
J, Argani P, Westra W, Van Criekinge W and Sidransky D:
Pharmacologic unmasking of epigenetically silenced genes in breast
cancer. Clin Cancer Res. 15:1184–1191. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Uchiyama CM, Zhu J, Carroll RS, Leon SP
and Black PM: Differential display of messenger ribonucleic acid: a
useful technique for analyzing differential gene expression in
human brain tumors. Neurosurgery. 37(Suppl): S464–S470. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Stearns ME and Wang M: Regulation of
kinesin expression and type IV collagenase secretion in invasive
human prostate PC-3 tumor sublines. Cancer Res. 51:5866–5875.
1991.PubMed/NCBI
|
|
30
|
Ostrow KL, Hoque MO, Loyo M, Brait M,
Greenberg A, Siegfried JM, Grandis JR, Gaither Davis A, Bigbee WL,
Rom W and Sidransky D: Molecular analysis of plasma DNA for the
early detection of lung cancer by quantitative methylation-specific
PCR. Clin Cancer Res. 16:3463–3472. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tuckwell D: Evolution of von Willebrand
factor A (VWA) domains. Biochem Soc Trans. 27:835–840.
1999.PubMed/NCBI
|
|
32
|
Robertson NG, Skvorak AB, Yin Y,
Weremowicz S, Johnson KR, Kovatch KA, Battey JF, Bieber FR and
Morton CC: Mapping and characterization of a novel cochlear gene in
human and in mouse: a positional candidate gene for a deafness
disorder, DFNA9. Genomics. 46:345–354. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Rodriguez CI, Cheng JG, Liu L and Stewart
CL: Cochlin, a secreted von Willebrand factor type a
domain-containing factor, is regulated by leukemia inhibitory
factor in the uterus at the time of embryo implantation.
Endocrinology. 145:1410–1418. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Botteman MF, Pashos CL, Redaelli A, Laskin
B and Hauser R: The health economics of bladder cancer: a
comprehensive review of the published literature.
Pharmacoeconomics. 21:1315–1330. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Divrik RT, Yildirim U, Zorlu F and Ozen H:
The effect of repeat transurethral resection on recurrence and
progression rates in patients with T1 tumors of the bladder who
received intravesical mitomycin: a prospective, randomized clinical
trial. J Urol. 175:1641–1644. 2006. View Article : Google Scholar
|
|
36
|
Thalmann GN, Markwalder R, Shahin O,
Burkhard FC, Hochreiter WW and Studer UE: Primary T1G3 bladder
cancer: organ preserving approach or immediate cystectomy? J Urol.
172:70–75. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ramani VA, Bromage SJ and Clarke NW: A
contemporary standard for morbidity and outcome after radical
cystectomy. BJU Int. 104:628–632. 2009. View Article : Google Scholar : PubMed/NCBI
|