Introduction
Ovarian cancer (OVCA) remains the leading cause of
mortality for patients with gynecologic malignancies, despite
recent advances in post-surgical chemotherapy (1). Numerous patients with OVCA are
diagnosed at an advanced stage of the disease, but may be treated
with surgery followed by chemotherapy. Initially, OVCA may be
chemotherapy-sensitive and the majority of patients achieve
clinical remission following primary surgical debulking and
adjuvant platinum-based therapy. However, the majority of patients
who respond to such therapy ultimately succumb due to relapse from
recurrent and drug-resistant disease. Following initial treatment,
70–90% of patients relapse. With additional second-line
chemotherapy, some patients return to partial or complete
remission. However, further relapse is likely to occur (2).
Novel therapies that reduce the risk of relapse are
therefore urgently required. A variety of systemic and regional
consolidation approaches with standard chemotherapy are being
investigated. In this context, targeted immunotherapy may be a
useful anti-OVCA strategy since such therapy may be effective
against chemotherapy-resistant disease with minimal toxicity. This
observation has also led to the recent development of various
immunotherapeutic treatment strategies (3).
One of the requirements for this approach is the
identification of antigens capable of mediating tumor rejection.
Certain antigen targets for immunotherapy of ovarian cancer such as
MUC1 (4,5), Her-2/neu (6,7) and
CA125 (8,9) are already known. However, other
antigens remain to be identified. The majority of tumor antigens
are non-mutated self-antigens to which the immune system is
tolerant. It is well documented that tumor cells do not express
co-stimulatory molecules and seldom express MHC class II molecules,
which are both essential for the induction of cell immunity. As a
result, tumor antigens may not be effectively presented to the
immune system (10,11), or worse, T cells responding to tumor
antigens may be anergic (12–14).
Therefore, new approaches are required to overcome these barriers
that prevent the induction of effective anti-tumor immunity against
antigens selective for, or over-expressed in, OVCA.
A strategy that has been developed is the
sensitization of dendritic cells (DCs) with tumor cells or tumor
antigens. DCs are bone marrow-derived leukocytes that are critical
in the initiation of T cell-mediated immunity (15,16).
These cells derive their potency from the constitutive and
inducible expression of essential co-stimulatory ligands on the
cell surface, including CD80, CD86, CD56 and CD40 (17,18).
DCs fused with patient-derived OVCA cells (19,20)
were found to induce cytotoxic T cells against autologous OVCA
cells.
In the present study, we described the use of DCs
sensitized with a liposomal construct of autologous and allogeneic
tumor antigens (DC-OVCA) in a patient with metastatic OVCA who had
residual metastatic lesions following chemotherapy and surgery.
Materials and methods
Consent for DC-OVCA injections
Informed consent was obtained from the patient prior
to the collection of DCs and OVCA cells, and prior to injections.
The consent form and immune cell procedures were reviewed and
approved by the Ethics Committee and the Institutional Review
Committee on Molecular and Cellular Therapeutics at the National
Kidney and Transplant Institute, Philippines.
Generation of DCs from peripheral blood
monocytes
Leukapheresis was performed for 4 h using a Cobe
leukapheresis machine. The peripheral blood monocytes (PBMC) were
separated through Ficoll density-gradient centrifugation, washed
twice with RPMI-1640, and resuspended in RPMI-1640 with 1%
autologous serum. Cells were cultured in a CO2 incubator
overnight in sterile culture flasks. Following the initial culture,
the non-adherent cells were decanted and the remaining adherent
cells were cultured in the presence of 5% autologous serum/RPMI
with 1000 U/ml GM-CSF and 500 U/ml IL-4 for 10 days. The cells were
then trypsinized and resuspended in RPMI-1640, 40% autologous serum
and 10% DMSO. The cells were transferred to freezing vials,
progressively cooled to lower temperatures, and then frozen in
liquid nitrogen.
Isolation and culture of OVCA cells
OVCA cells were isolated from the resected specimen
at the time of surgery. Tumor samples were transferred to the
laboratory in a gentamycin-containing RPMI-1640. The tumor tissue
(1 mg/ml) was minced finely with a sterile scalpel, transferred
into a sterile petri dish containing RPMI-1640 with L-glutamine,
gentamycin and 10% autologous plasma at a concentration of
5×106 tumor cells/ml, and cultured in a 5%
CO2 incubator at 37°C. After three days, the adherent
cells were plated in sterile flasks containing RPMI-1640 with
L-glutamine, gentamycin and 10% autologous plasma, and cultured
further in a 5% CO2 incubator at 37°C. After seven days,
approximately half of the cultured cells were trypsinized and
frozen in a medium containing 50% autologous serum, 40% RPMI-1640
and 10% DMSO.
Characterization of DCs and OVCA
cells
After 10 days in culture, a portion of DCs were
trypsinized and stained by indirect immunofluorescence with a CD86
antibody (Pharmingen, San Diego, CA, USA), which is reactive with
DCs. The autologous and allogeneic OVCA cells were tested by
indirect immunofluorescence with antibodies against intracellular
keratin and Her2/neu (Sigma, St. Louis, MO, USA), CA125
(Novocastra, Newcastle, UK) and MUC1 (Pharmingen) after seven
days.
Fusion of DCs with liposomal construct of
autologous and allogeneic OVCA antigens
The OVCA cells isolated above were cultured for
seven days and irradiated at 50 Gy. The autologous OVCA cells
(2×106) were mixed with MUC-positive allogeneic OVCA
cells (1×106) at a ratio of 2:1, respectively. This
mixture was washed twice with serum-free RPMI-1640. The cell
mixture was centrifuged at 2000 rpm and resuspended in serum-free
RPMI-1640. The cell pellet was sonicated for 5 min and resuspended
in 0.50 ml of a liposomal mixture of phosphatidylcholine and
phospho-ethanolamine containing 5% polyethylene glycol (PEG)
solution without Ca++ and Mg++, and
maintained at 37°C for 5 min. The liposomal construct of OVCA
antigens was mixed with 1×107 autologous DCs,
centrifuged and resuspended in 1.5 ml of RPMI-1640 with 10%
autologous plasma. PEG-induced fusion was confirmed by microscopy.
For preparation of the DC-OVCA injection, the DCs fused with
liposomal OVCA were mixed with 500 U/ml GM-CSF placed in two
sterile syringes containing 0.75 ml of the mixture per syringe for
intradermal injection.
In vitro tests of immune activity and
T-cell proliferation
PBMC of the patient was isolated by Ficoll
density-gradient centrifugation. PBMC was cultured in RPMI-1640
containing 1% autologous serum for 1 h. The non-adherent cells were
removed, and the T cells were purified by nylon wool separation.
DCs (isolated from the patient prior to in vivo
immunization) were treated with mitomycin C at 50 μg/ml for 45 min
and washed 3 times with PBS. The DCs were resuspended in RPMI-1640
with 20% fetal calf serum. The T cells were co-cultured with DCs at
a 10:1 ratio of T cells to DCs in medium containing 10% human serum
for five days. T-cell proliferation was measured using standard
[3H]-thymidine incorporation. The cells were pulsed with
1 uCi [3H]-thymidine (New England Nuclear, Boston, MA,
USA) per well for 12 h and then collected on filters with a
semi-automatic cell harvester. Tritium incorporation was quantified
by liquid scintillation. Determinations were conducted in
triplicate and expressed as the mean ± SD.
Cytolytic (CTL) activity directed against
OVCA cells
PBMC (10×106) from the patient was
cultured in RPMI-1640 containing 1% autologous serum for 1 h. The T
cells were purified by passage using nylon wool. DCs (isolated from
the patient prior to in vivo immunization) sensitized with
various antigen constructs were added at a 10:1 ratio of T cells to
DCs in medium containing 10% human serum in the presence of 1000
U/ml GM-CSF and 500 U/ml IL-4 for 10 days. The sensitized T cells
were then co-cultured with 51Cr-labeled targets for 5 h
at 37°C. The cell targets included normal fibroblasts, autologous
OVCA cells, allogeneic OVCA cells and the HL60 leukemia cell line.
The T cells and various cell targets were resuspended in culture
medium at a 10:1 ratio of T cells to target cells in 96-well,
V-bottom plates. The plates were centrifuged at 1400 rpm for 5 min
to initiate cell contact and incubated for 5 h at 37°C with 5%
CO2. Following incubation, supernatant was collected and
radioactivity was quantified in a gamma counter. The spontaneous
release of 51Cr was determined by incubation of targets
in the absence of effectors, while maximum or total release of
51Cr was determined by the incubation of targets in 0.1%
Triton X-100. The percentage of specific release of 51Cr
was determined using the equation: percentage-specific release =
[(experimental - spontaneous) / (maximum - spontaneous)] × 100.
Immunoblotting of patient serum on OVCA
antigens
Membrane extracts of primary foreskin fibroblasts,
autologous OVCA cells isolated from the patients, the OVCAR cell
line (ATCC) and the MCF7 breast carcinoma cell line (ATCC) were
standardized to a protein concentration of 10 μg/ml and applied to
SDS-PAGE samples, and were then separated on SDS-PAGE and
transferred onto a Hybond-C nitrocellulose membrane (Amersham, UK).
The membrane was blocked with 5% non-fat milk in TBST (10 mM Tris
HCl, pH 7.5, 100 mM NaCl and 0.1% Tween-20) and incubated with the
patient's serum overnight at 4°C. After the membrane was exposed to
goat anti-human secondary antibodies for 1 h, the blots were
detected using an enhanced chemiluminescence method (Pierce,
Rockford, IL, USA).
Results
Patient data
DCs generated from a patient with metastatic OVCA
were sensitized with different antigenic constructs in vitro
and analyzed for immune reactivity. DCs isolated from the patient
prior to and following immunization with DC-OVCA were analyzed for
cytotoxicity against OVCA and other cell targets in vitro.
The immune reactivity of the patient prior to and following DC-OVCA
administration was analyzed by the immunoblot recognition of OVCA
antigens. The clinical response of the patient was then followed by
serial CAT scans.
The patient was a 35-year-old physician with a
gynecological history of G2P2Ab0. The patient was generally
asymptomatic with the exception of occasional pelvic pains that
started in mid 2002. The patient took oral contraceptives for a few
weeks in 2002, which decreased the frequency of her pelvic pains.
In February 2004, she developed increasing cramping pain in the
pelvic area associated with loose stools. An abdominal ultrasound
performed on March 17, 2004, showed suspicious liver lesions. A CT
scan on March 18, 2004, showed multiple pelvic masses, the largest
measuring 5.6×4.8 cm. Multiple lesions were observed in the liver,
the largest measuring 4.7 cm in the left lobe of the liver. In
addition, there were numerous pulmonary masses involving the lungs.
Lower GI endoscopy on March 27, 2004, was normal with the exception
of hemorrhoids. Upper GI endoscopy on March 28, 2004, was normal
and the stomach biopsy was negative. The mammogram and thyroid
ultrasound were also normal. Serum tumor markers obtained on March
29, 2004, included a CA125 of 41 U/ml (normal, <35 U/ml), CA
19-9 of 46 U/ml (normal, <27 u/ml), CEA of 6.3 ng/ml (normal,
<5.5 ng/ml), AFP was 4 IU/ml (normal, <5.8 IU/ml) and HCG was
negative. On April 4, 2004, the patient underwent a CT-guided liver
biopsy which revealed metastatic and poorly differentiated
adenocarcinoma. Immunohistochemical stains were positive for CK7,
but negative for CK20, TTF-1, S-100, ER, chromogranin, placental
alkaline phosphatase, hepar-1 and inhibin. The diagnostic
impression at this time was metastatic adenocarcinoma of unknown
primary origin.
Treatments
In April 2004, the patient started chemotherapy
consisting of carboplatin with AUC 7, paclitaxel 175
mg/m2, and etoposide 50 mg alternating with 100 mg days
1–10, administered every 3–4 weeks. Following the sixth course of
chemotherapy, the patient developed persistent thrombocytopenia.
The etoposide dose was reduced in subsequent courses and eventually
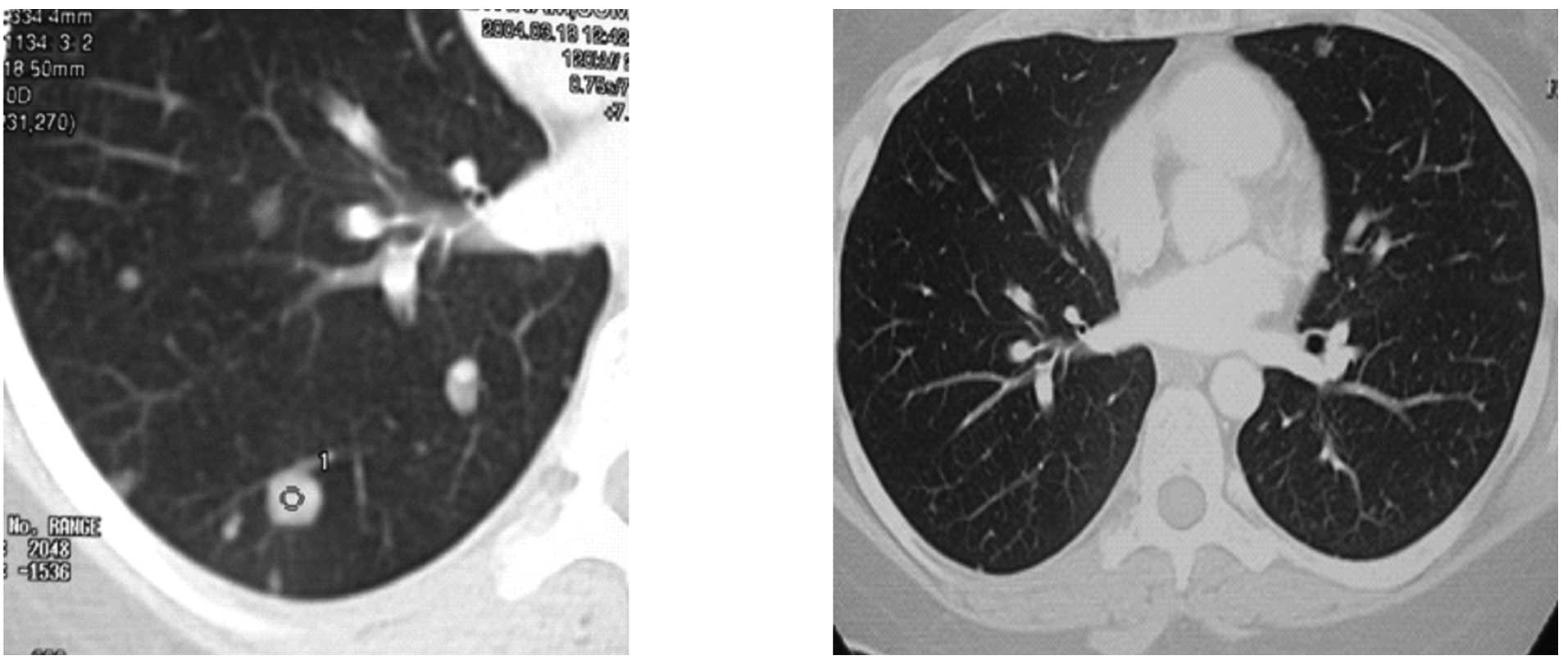
discontinued. After six courses of chemotherapy, CT scans on
September 29, 2004, showed numerous residual masses, with the
largest liver lesion measuring 3.6×2.0 cm and the largest pelvic
masses measuring 3.7×3.0 cm in diameter. Chemotherapy was continued
with carboplatin and paclitaxel for four additional courses. A CT
scan on December 28, 2004, showed multiple liver lesions with the
largest still measuring 3.6×2.0 cm, and bilateral multiple masses
in the lungs with each measuring approximately 1 cm in diameter.
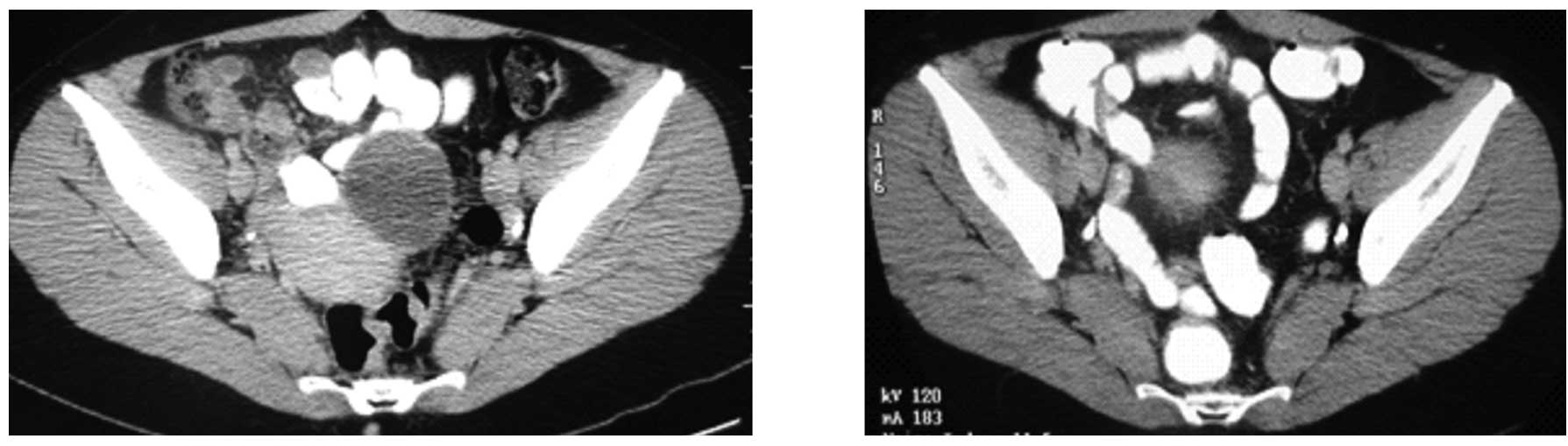
However, certain lesions increased in size despite continued
chemotherapy. A right adnexal mass increased in size to 5.7×4.4 cm,
almost double in size compared to that of three months prior to the
measurement.
In January of 2005, the patient complained of
increasing right pelvic pain requiring narcotics. An MRI performed
on January 20, 2005, showed a further enlargement of the largest
adnexal mass, now measuring 7.2×4.9×4.2 cm. Multiple metastatic
tumors were also observed in the liver and lungs. Due to
intractable pelvic pain, the patient underwent palliative surgery,
with total hysterectomy with bilateral salpingo-oophorectomy on
January 5, 2005. At the time of surgery, a large cystic mass was
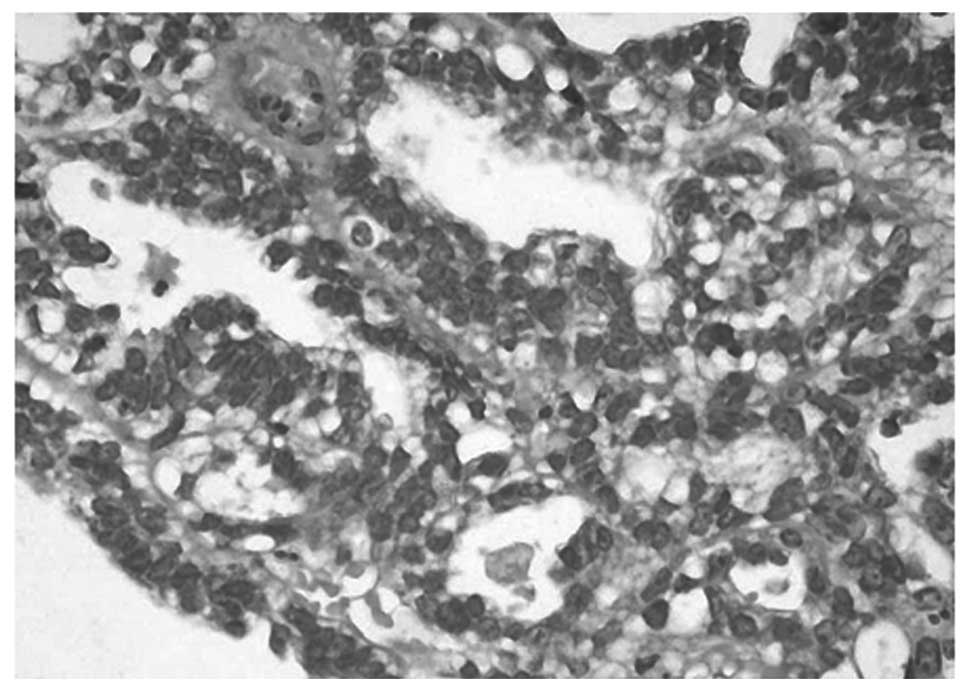
found in the right ovary. The histological diagnosis was
endometrioid adenocarcinoma with a tubulo-papillary pattern arising
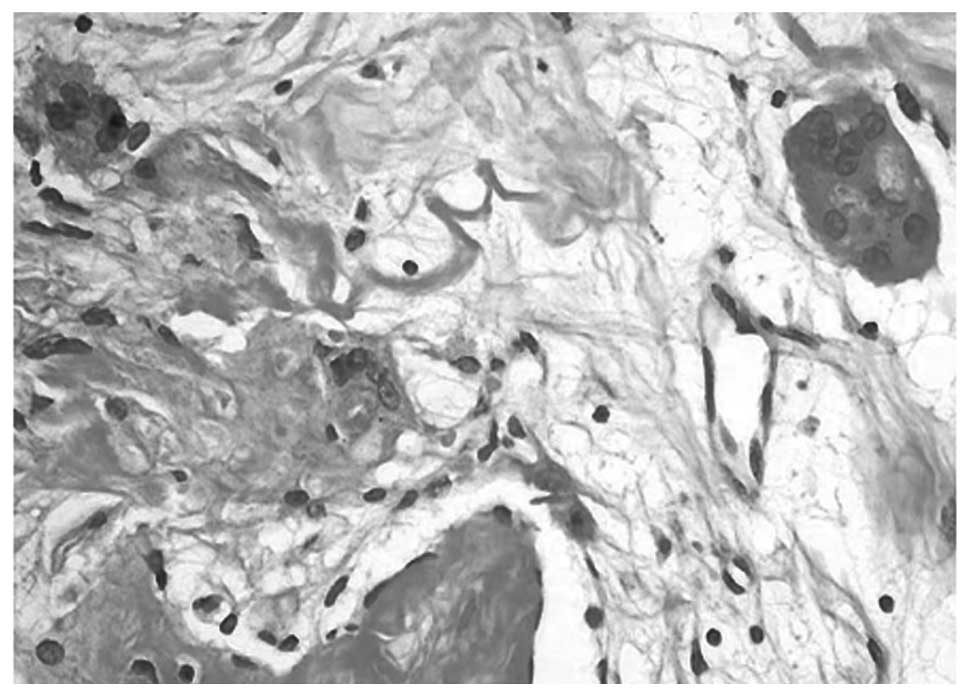
from an ovarian cyst (Fig. 1).
Numerous multinucleated giant cells were also found in the tissue
specimen (Fig. 2). Part of the OVCA
was minced, frozen, and used as intact cells or as cell lysate
incorporated into a liposomal construct.
From the resected ovarian mass, viable OVCA cells
were isolated and cultured for two weeks until processing for
antigen. Aliquots of the cultured cells were allowed to adhere to
sterile coverslips and were tested for antigen reactivity.
Permeabilized cells were reactive with anti-cytokeratin in the
cytoplasm. There was strong membrane staining with MUC1, weak
staining for CA125 and negative staining for the Her2/neu antigen.
Following 2 weeks in culture, the adherent cells were trypsinized
and irradiated at 50 Gy prior to use as antigen either as intact
cells or as a tumor lysate.
The patient underwent a 4-h leukapheresis without
any complications. The leukapheresis sample, following Ficoll
density-gradient centrifugation, yielded a total of
5×107 mononuclear cells. Following the initial culture,
the non-adherent cells were decanted and the adherent population
was incubated further in the presence of 5% autologous serum and
RPMI premixed with 1000 U/ml GM-CSF and 500 U/ml IL-4. By five
days, the cells flattened and became markedly adherent to the
culture flask. By seven days, the majority of the cells exhibited
long dendrite-like projections that came into contact with other
cells. Approximately 80% of the cells were reactive with anti-CD86
antibody by indirect immunofluorescence microscopy. Following 10
days of culture, the cells were scraped gently and aliquoted into
vials with RPMI containing 10% DMSO. After the serial temperature
dropped, the vials were stored in a liquid nitrogen tank. Two vials
were thawed after five days in the frozen state and found to have
70% viability by trypan blue compared to 95% viability prior to
freezing.
T-cell proliferation induced by the
fusion of DC
In vitro tests of immune reactivity were
performed on DCs developed from the mononuclear cells collected by
leukapheresis. Various concentrations of control liposome,
autologous OVCA cells, liposomal construct of autologous OVCA, and
liposomal construct of allogeneic OVCA were fused with the DCs and
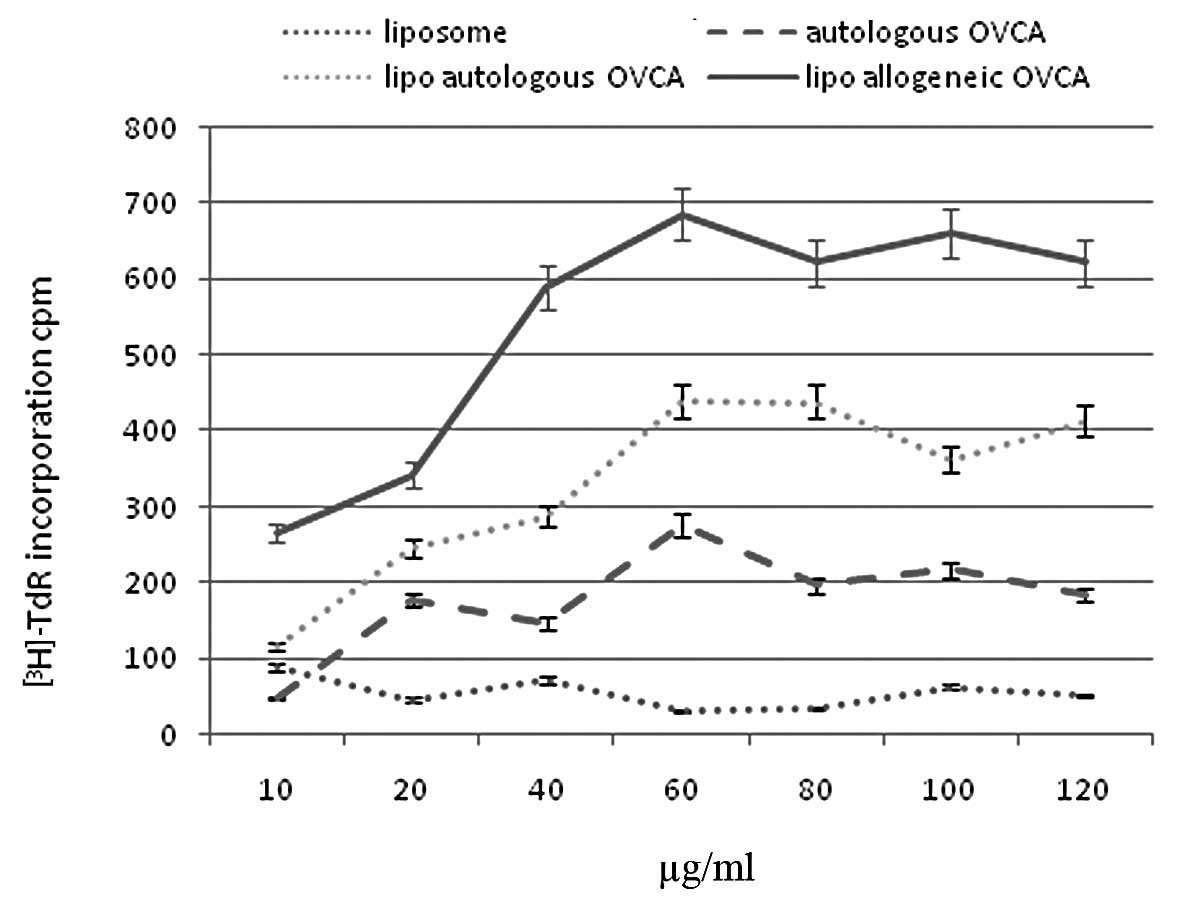
tested for their ability to stimulate T-cell proliferation. As
shown in Fig. 3, liposomes in the
absence of antigens did not significantly induce T-cell
proliferation. DCs fused with autologous whole OVCA cells showed
increasing T-cell proliferation, up to 60 μg/ml of the construct,
but reached a plateau. Higher concentrations of the antigen
preparations did not induce greater T-cell proliferation. A
liposomal construct of autologous OVCA antigens showed a higher
T-cell proliferation, almost 2-fold compared to intact autologous
OVCA cells. A liposomal construct of allogeneic OVCA cells showed
an even higher T-cell proliferation, almost 3-fold compared to the
intact autologous OVCA cells.
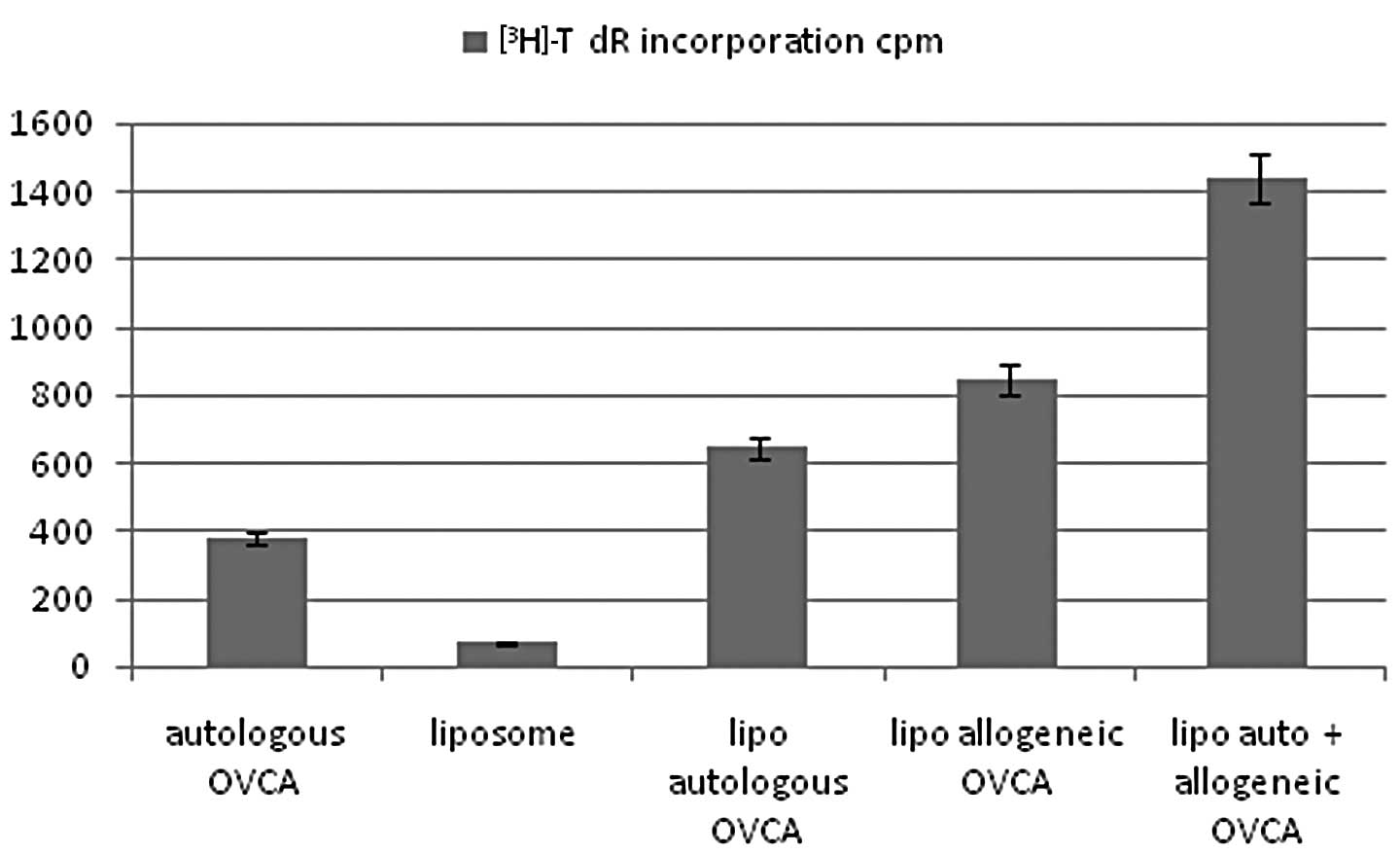
Using the peak concentration (60 μg/ml) of each
construct, T-cell proliferation induced after fusion with DCs was
determined using the combination of liposomal autologous and
liposomal allogeneic OVCA. The results, shown in Fig. 4, demonstrated that further
stimulation of T-cell proliferation was induced by the liposomal
construct combining autologous and allogeneic OVCA antigens with a
higher activity compared with autologous OVCA, control liposomes,
or single constructs of liposomal autologous OVCA, or liposomal
allogeneic OVCA alone.
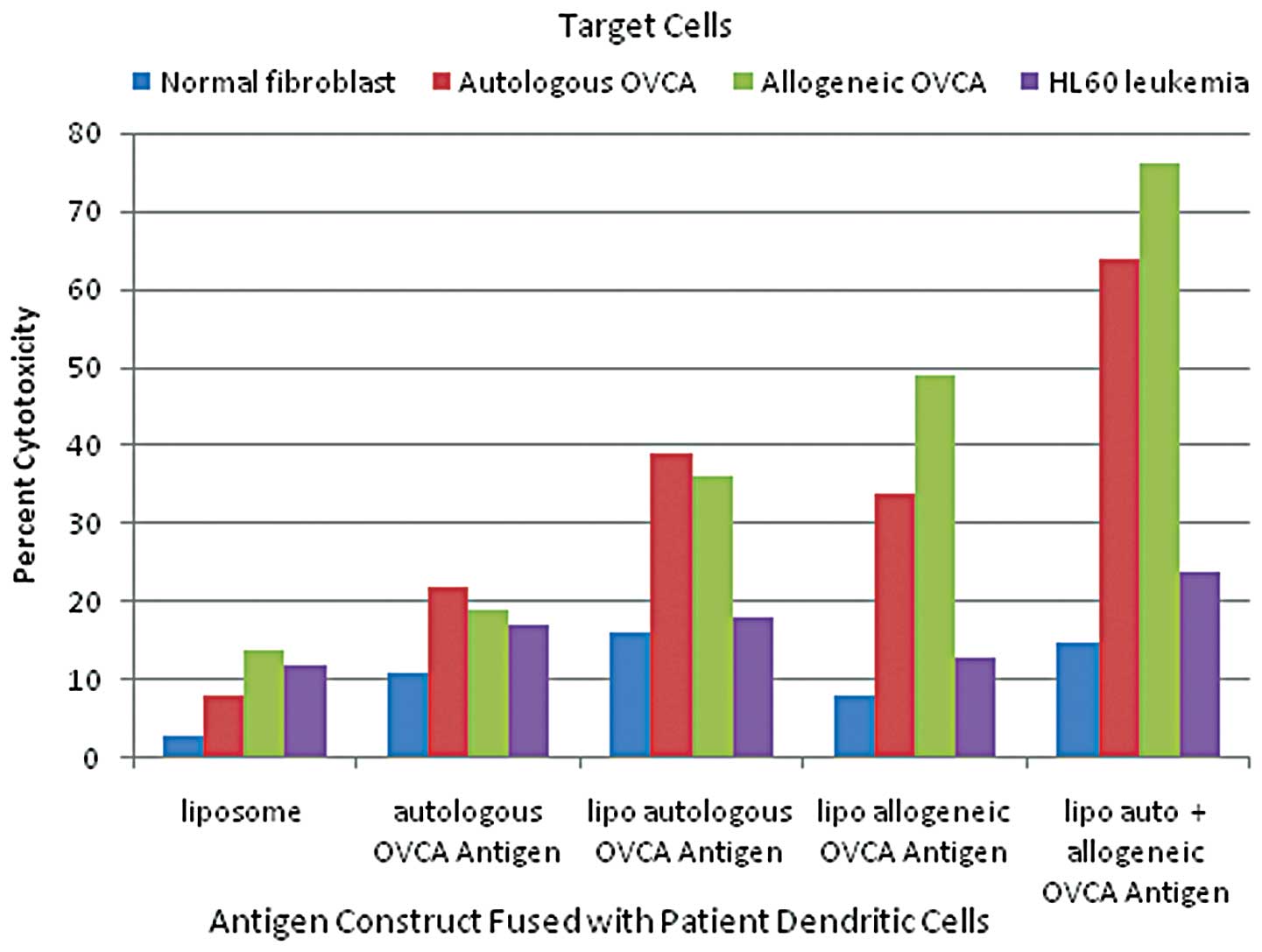
In vitro cytotoxicity induced by fusion
of DC
The effect of fusion of DCs with different antigen
preparations on the cytotoxicity of T cells in vitro was
determined. As shown in Fig. 5, the
greatest OVCA cell cytotoxicity was induced by fusion of DCs with a
liposomal construct combining autologous and allogeneic OVCA
antigens compared with autologous intact OVCA cells, or single
liposomal constructs of autologous OVCA or allogeneic OVCA alone.
Control liposomes without OVCA antigens had minimal effect on
T-cell induction of cytotoxicity.
The immunogen administered to the patient consisted
of DCs fused with a liposomal construct of autologous and
allogeneic OVCA antigens. The patient received six monthly
intradermal injections (January to June, 2005) of DC-OVCA, in each
arm. With the exception of mild local skin reactions of swelling
and slight redness that lasted for two days, the patient tolerated
the injections well without fever, rash, muscle aches or joint
pains. Following the six monthly injections, the patient's CT scans
showed progressive reductions in the size and number of the
metastatic lesions in the liver, lungs and pelvis. Since the
patient still had residual masses, she received two additional
chemotherapy courses with carboplatinum and taxol but was unable to
continue due to severe thrombocytopenia, neutropenia, nausea and
neuropathy. The patient's last chemotherapy cycle was administered
in July 2005.
The patient was subsequently treated with DC-OVCA
every month for an additional four treatments, without any
chemotherapy. The patient showed continued improvement in her
strength and peripheral nerve symptoms. Moroever, she gained weight
and her overall function improved. A follow-up CT scan of the
abdomen and pelvis in September 2005, showed a marked decrease in
the number and size of metastatic lesions in the liver. The pelvis
showed no masses. Lung CT showed a decreased size and number of
lung nodules.
Patient outcome
By January 2006, a CT scan of the patient's lungs,
liver and pelvis showed no metastatic lesions (Fig. 6-8).
The patient was asymptomatic, maintaining normal activities with
normal blood tests two years following the diagnosis of metastatic
ovarian cancer. In 2006, the patient's only treatment consisted of
one OVCA immune injection. On recent follow-up, the CT scans
performed in March and November of 2006, and January 2007, showed
no tumor masses. Serum tumor markers, including CA125, and liver
functions tests were all normal. On further clinical follow-up and
scans in 2010 and 2011, seven years following diagnosis, the
patient remained tumor-free, asymptomatic and with a normal
lifestyle.
After the patient completed DC-OVCA immunization,
mononuclear cells were isolated to prepare DCs and were compared
with pre-immunization DCs. As shown in Fig. 9, the post-immunization DCs showed 2-
to 3-fold greater toxicity against autologous and allogeneic OVCA
cells compared to pre-immunization DCs. The post-immunization and
pre-immunization DCs did not show any significant cytotoxicity
against normal fibroblasts or HL60 leukemia cells.
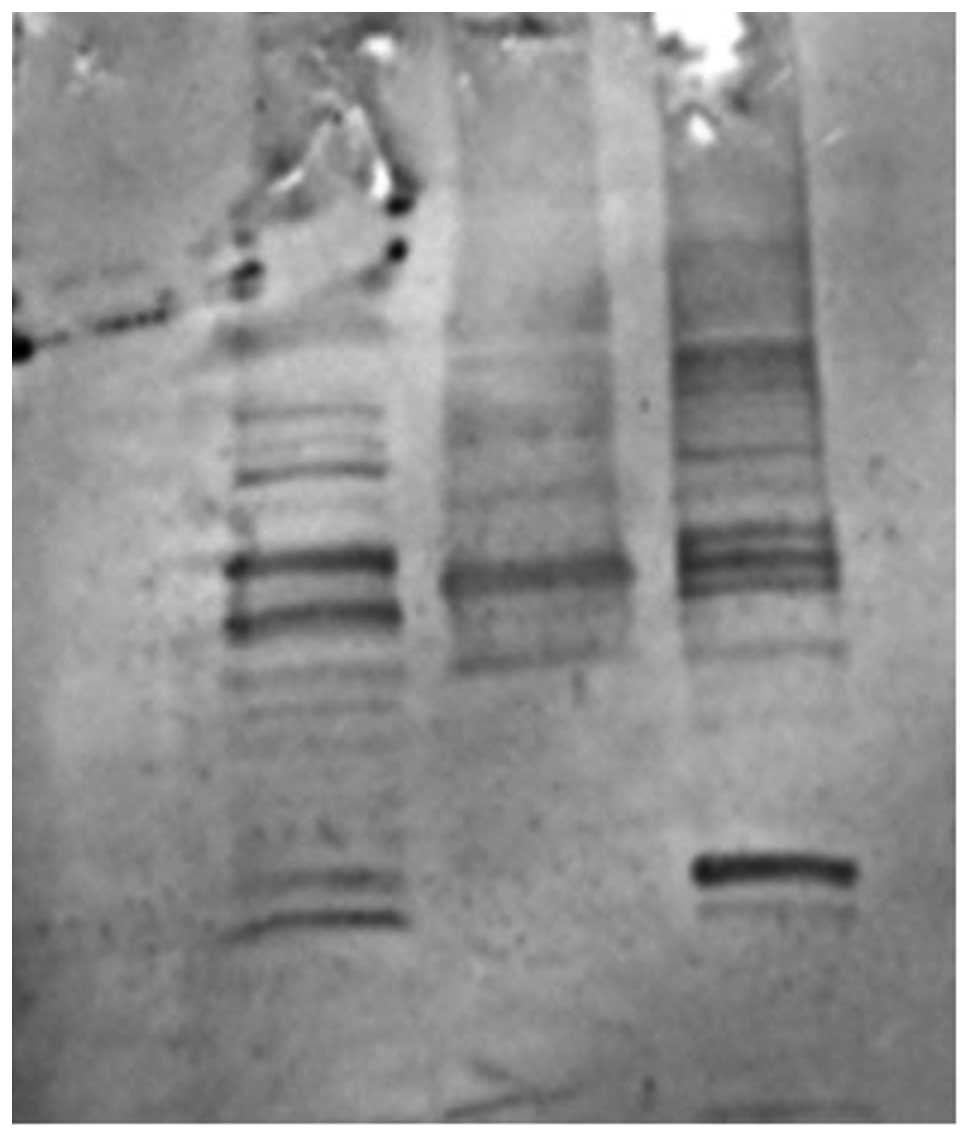
The patient's serum collected in January 2006,
following completion of the DC-OVCA treatment was examined by
immunoblot analysis, which showed that the serum antibodies were
reactive antigens of 60, 65, 110 and 120 kDa present in autologous
OVCA (Fig. 10B) and allogeneic
OVCA cells (Fig. 10D). The serum
collected prior to DC-OVCA did not show reactivity with these
antigens (data not shown). The serum antibodies upon completion of
DC-OVCA treatment did not react with similar sized antigens in
extracts from normal fibroblasts (Fig.
10A) and MCF 7 breast cancer cells (Fig. 10C).
Discussion
Present treatments of OVCA
Epithelial OVCA is the sixth most common cause of
mortality due to cancer worldwide. The overall prognosis is poor as
most patients present with advanced disease and efforts for early
detection and screening have not been effective. The patient
reported in this study is a young physician who only had a few
months of mild pelvic discomfort, but at initial diagnosis already
had large pelvic masses and numerous metastatic lesions in the
lungs and the liver. The current ‘standard treatment’ for advanced
ovarian cancer is a combination of a platinum compound and a
taxane, usually in the form of carboplatin and paclitaxel (21). Although this platinum/taxane-based
chemotherapy produces a high regression rate, the large majority of
patients (70–90%) relapse within 18 months, often with
chemotherapy-resistant diseases. Overall survival is relatively
poor with only 10–15% of advanced-disease patients surviving at 10
years. Therefore, new treatment approaches are required to improve
response rates, to prevent relapse following chemotherapy and to
prolong progression-free survival.
Rationale for immunotherapy in OVCA
Evidence exists that tumor antigens and anti-tumor
immunity exist in patients with OVCA and affect the course of the
cancer (22–25). A number of known tumor-associated
antigens, including MUC-1, Her2/neu, p53, CA125, MAGE antigens and
testis cancer antigens, were found to be overexpressed in OVCA
(26). Tumor antigen-specific T
cells occur naturally in OVCA patients. Naturally occurring T cells
that recognize tumor-associated antigens were found in 50% of OVCA
patients (27). The presence of
intratumoral T cells correlates with improved clinical outcome in
advanced OVCA (24). These
tumor-infiltrating T cells are capable of identifying autologous
ovarian tumor or peptides derived from OVCA tumor antigens
(22,23). The tumor antigen-specific T cells
may be expanded from OVCA patients in vitro (27) and may recognize similar epitopes in
HER2/neu antigens of breast cancer (7). The adoptive transfer of these
tumor-infiltrating lymphocytes has been found to prolong
disease-free survival in patients with advanced OVCA (25).
The presence of tumor-infiltrating T cells was found
to have a significant impact on the outcome of OVCA following
chemotherapy (24). The five-year
survival rate of patients whose tumor contained tumor-infiltrating
T cells was 38%, whereas the survival rate of patients without
tumor-infiltrating T cells was only 4.5%. This survival difference
was highly statistically significant, with p<0.001. The presence
of T-cell infiltration was found by multivariate analysis to be a
statistically independent prognostic variable that correlated with
progression-free and overall survival, and was independent of the
clinical response to chemotherapy.
Thus, there is strong justification, for exploring
immunotherapy in the treatment of advanced OVCA using tumor
antigen-specific cytotoxic immune cells for killing cancer cells by
a mechanism distinct from chemotherapy (28,29).
Immunotherapy has the potential to enhance the body's own ability
to attack the cancer with greater specificity and less toxicity.
However, the appearance and growth of the tumor itself indicates a
failure of the immune surveillance of the body at the control
mechanisms for immune induction and action, and possibly indicates
defects at the level of antigen presentation, the action of
co-stimulatory molecules and immune tolerance, and T cell
unresponsiveness to tumor-associated antigens.
The use of DCs is one way to enhance the tumor
antigen presentation. In OVCA, the approaches for antigen
presentation included DC-OVCA fusion and antigen pulsing (30,31).
DCs fused with OVCA cells have the potential of delivering the
mature immune cells with the appropriate co-stimulatory and MHC
molecules, and with the whole complement of tumor antigens to
facilitate endogenous and exogenous pathways of antigen
presentation, leading to the induction of CD4 and CD8 T cells.
DCs/OVCA cells were found to stimulate the interferon expression of
CD4 and CD8 T cells, and to induce CTL activity against autologous
OVCA cells [A]. DC/OVCA fusion cells stimulated T cells and
reversed the unresponsiveness of T cells to autologous OVCA cells.
The DCs of the patient are capable of being fused with autologous
or allogeneic tumor cells, or both these types of cells.
In the current patient, viable autologous OVCA cells
were collected at the time of surgery. The injections administered
consisted of a liposomal construct including autologous and
allogeneic OVCA cells. A significant advantage of using autologous
tumor cells in the DC-OVCA fusion is that these cells contain the
relevant OVCA antigens required to control the patient's tumor.
Disadvantages include the need for arranging the collection of
viable tumor at the time of surgery and the difficulties in
culturing tumor cells. The culture of tumor cells requires advance
planning, but since debulking surgery is often part of the
treatment of OVCA, the opportunity for collecting and growing OVCA
cells should not be missed.
When this patient underwent bilateral
salpingo-oophorectomy and hysterectomy, she was found to have a
large cystic mass in the right ovary with a histological diagnosis
of endometrioid adenocarcinoma with a tubulo-papillary pattern
arising from an ovarian cyst. The tumor cells were reactive with
anti-cytokeratin in the cytoplasm, and had strong membrane staining
for MUC1, weak staining for CA125 and negative staining for
Her2/neu antigens. Although, histologically, the patient was found
to have carcinoma arising from the ovary, there were no ovarian
markers in the tissue and serum, such as CA125, that were useful in
the identification of this patient's tumor. For this patient, tumor
cells were kept viable at the time of surgery and were the source
of autologous tumor cells used for DC sensitization. However,
numerous patients with progressive ovarian cancer do not have
viable tumor cells saved at the time of biopsy or surgery.
Moreover, using only the patient's tumor cells may not effectively
present antigens to the immune system (10,11),
and the patient's T cells may be anergic to the autologous tumor
antigens (12–14). Therefore, for this patient, we also
used allogeneic OCVA cells to supplement the autologous tumor
cells.
Optimal immune reactivity in vitro and in
vivo induced by the liposomal construct of autologous and
allogeneic tumor antigens
To determine the best immunogen for DC
sensitization, in vitro tests of immune activity were
performed on the DCs and T cells collected at the time of initial
leukapheresis. The peak concentrations of each preparation of
intact OVCA cells, the liposomal construct of autologous OVCA
antigens, and the liposomal construct of allogeneic OVCA antigens
on T-cell proliferation were determined, showing higher immune
activity using liposomal constructs compared to intact tumor cells.
The T-cell proliferative activity using higher concentrations of
each construct reached a plateau. However, the plateau was 2-fold
higher with the liposomal construct of autologous OVCA antigens and
approximately 3-fold higher using the liposomal construct of
allogeneic OVCA antigens compared to intact autologous OVCA cells.
This observation emphasizes that simply fusing intact autologous
tumor cells with DCs may not be sufficient to induce optimal immune
reactivity against the tumor.
The highest T-cell proliferation was observed using
a liposomal construct combining autologous and allogeneic OVCA
cells. The highest OVCA target cell cytotoxicity was also observed
with the liposomal construct with combined autologous and
allogeneic OVCA antigens compared with intact autologous OVCA cells
or liposomal constructs of autologous or allogeneic antigens alone.
The cytotoxicity induced by the liposomal construct with combined
autologous and allogeneic OVCA antigens induced much greater
cytotoxicity on OVCA cells compared with normal fibroblasts and
HL60 leukemic cells.
Based on the in vitro studies, the patient
was injected with DCs fused with a liposomal construct with
autologous and allogeneic OVCA antigens. The OVCA cells, both
autologous and allogeneic, were irradiated at 50 Gy prior to being
used in antigen extraction and incorporated into liposomes.
Following completion of the DC-OVCA injections, DCs isolated from
the patient post-immunization were compared to pre-immunization
DCs. DCs prepared from mononuclear cells collected
post-immunization showed 2- to 3-fold greater cytotoxicity against
autologous and allogeneic OVCA cells compared to DCs
pre-immunization. Serum antibodies collected post-immunization also
showed reactivity with specific antigens present in OVCA cells, but
were not present in normal fibroblasts and MCF-7 breast cancer
cells. Thus, the immunization of this patient with a liposomal
construct combining autologous and allogeneic OVCA cells induced
specific immune reactivity against OVCA antigens in
vivo.
Treatment with chemotherapy combined with
DC-OVCA immunotherapy
The current patient was initially treated with
chemotherapy prior to the DC-OVCA injections. At initial
presentation, this patient was considered to have carcinoma of
unknown primary origin. The initial CT scan showed numerous
pulmonary masses involving the lungs, multiple pelvic masses and a
number of large lesions in the liver. Lower GI and upper GI
endoscopy were normal and the gastric biopsy was negative. The
serum tumor markers at initial presentation, including CA125, CA
19-9 and CEA, were mildly elevated, whereas AFP and HCG were
normal. A CT-guided liver biopsy revealed as a metastatic and
poorly differentiated adenocarcinoma with no clear indication of
primary origin. Immunohistochemical stains of the liver biopsy
specimen were positive for CK7, but negative for CK20, TTF-1,
S-100, ER, chromogranin, placental alkaline phosphatase, hepar-1
and inhibin. Thus, there were no germ cell markers present that
would have predicted responsiveness to chemotherapy. The tumor was
of epithelial origin but the formal interpretation of the initial
biopsy was metastatic adenocarcinoma of unknown primary origin.
The patient's initial treatment regimen, based upon
a diagnosis of carcinoma of unknown primary origin, consisting of
carboplatinum, taxol and etoposide, caused considerable side
effects, including abdominal discomfort, neuropathy, severe
thrombocytopenia and neutropenia, requiring multiple dose
adjustments, cytokine support and, eventually, discontinuation of
the chemotherapy. Although the patient had a partial response to
chemotherapy, she had multiple residual masses and progressive
enlargement of pelvic masses. This mixed response to treatment was
indicative of the heterogeneity of the tumor. Thus, chemotherapy by
itself was not sufficient in controlling the tumor. The patient
eventually underwent surgery to resect an enlarging pelvic mass,
which caused increasing pelvic pain requiring narcotic
administration.
The conventional view of chemotherapy is an
immuno-suppressive treatment that has the potential to reduce
myelocytes and lymphocytes (32).
However, patients with advanced OVCA were found to have enhanced
T-cell function with increased CD8+ T-cell responses to a pool of
MHC class I-restricted recall antigens in that following
administration of carboplatinum-paclitaxel combination
chemotherapy, patients with advanced OVCA were found to have
enhanced T-cell function (31).
Synergies between chemotherapy and immunotherapy have also been
found in experimental tumor systems (33). Chemotherapy may act to decrease
tumor load and tumor-induced immunosuppression, supporting the idea
that the ideal time to induce anti-tumor immunity is following
chemotherapy/radiation or debulking surgery.
In other types of gynecologic cancer, immune
enhancement was found to be significant in the effects of
chemotherapy. Patients who received platinum-based adjuvant
chemotherapy and chemo-radiation for cervical cancer were also
found to have an increased proportion of CD4+ and CD8+ T cells and
natural killer cells in draining pelvic lymph nodes biopsied
following surgery (34). The
enhancement of immune cell activity was not limited to
carboplatinum and paclitaxel. In an animal model, gemcitabine was
found to increase antigen cross-presentation, T-cell expansion and
infiltration of tumors, resulting in the eradication of the tumor.
The effect of chemotherapy with gemcitabine did not appear to be
due solely to decreased tumor bulk, as surgical resection of the
tumor by itself did not lead to an enhanced immunotherapeutic
effect (33).
By itself, immunotherapy alone is unlikely to be
effective in cancer with bulky masses, such as ovarian cancer, even
following surgery. Since chemotherapy enhances rather than impedes
immune cell function, the best effect of immunotherapy may be
following chemotherapy. Moreover, immunotherapy may act better in
minimal residual disease and may then be integrated in adjuvant
treatment programs following surgery and/or radiation.
In conclusion, a combination of DC-OVCA treatment
following chemotherapy was successful in treating a patient with
metastatic OVCA who presented with large pelvic masses and large
metastatic lesions in the liver and lungs. The patient had a
partial response following chemotherapy but had persistent large
masses in the pelvis and residual lesions in the liver and lungs.
Following DC treatment, the patient's metastatic lesions markedly
decreased in size. Seven years following the initial diagnosis, the
patient has shown no residual disease. Thus, further investigations
should be conducted on the use of immunotherapy in combination with
chemotherapy in the treatment of OVCA.
References
|
1
|
Jemal A, Murray T, Samuels A, Ghafoor A,
Ward E and Thun MJ: Cancer statistics. CA Cancer J Clin. 53:5–26.
2003.
|
|
2
|
McGuire WP, Hoskins WJ, Brady MF, Kucera
PR, Partridge EE, Look KY, Clarke-Pearson DL and Davidson M:
Cyclophosphamide and cisplatin compared with paclitaxel and
cisplatin in patients with stage III and stage IV ovarian cancer. N
Engl J Med. 334:1–6. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kirby TO, Huh W and Alvarez R:
Immunotherapy of ovarian cancer. Exp Opin Biol Ther. 2:409–417.
2002. View Article : Google Scholar
|
|
4
|
Ichige K, Perey L, Vogel CA, Buchegger F
and Kufe D: Expression of the DF3-P epitope in human ovarian
carcinomas. Clin Cancer Res. 1:565–571. 1995.PubMed/NCBI
|
|
5
|
Lu KH, Patterson AP, Wang L, et al:
Selection of potential markers for epithelial ovarian cancer with
gene expression arrays and recursive descent partition analysis.
Clin Cancer Res. 10:3291–3300. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
McKenzie SJ, DeSombre KA, Bast BS, et al:
Serum levels of HER-2 neu (C-erbB-2) correlate with overexpression
of p185neu in human ovarian cancer. Cancer. 71:3942–3946. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Peoples GE, Goedegebuure PS, Smith R,
Linehan DC, Yoshino I and Eberlein TJ: Breast and ovarian
cancer-specific cytotoxic T lymphocytes recognize the same
HER2/neu-derived peptide. Proc Nat Acad Sci USA. 92:432–436. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wagner U, Schlebusch H, Kohler S,
Schmolling J, Grunn U and Krebs D: Immunological responses to the
tumor-associated antigen CA125 in patients with advanced ovarian
cancer induced by the murine monoclonal anti-idiotype vaccine
ACA125. Hybridoma. 16:33–40. 1997. View Article : Google Scholar
|
|
9
|
Jacobs I and Bast RC Jr: The CA 125
tumour-associated antigen: a review of the literature. Hum Reprod.
4:1–12. 1989.PubMed/NCBI
|
|
10
|
Gusdon JP Jr, Homesley HD, Jobson VW and
Muss HB: Treatment of advanced ovarian malignancy with
chemo-immunotherapy using autologous tumor and Corynebacterium
parvum. Obstet Gynecol. 62:728–735. 1983.PubMed/NCBI
|
|
11
|
Dillman RO, Nayak SK, Brown JV, Mahdavi K
and Beutel LD: The feasibility of using short-term cultures of
ovarian cancer cells for use as autologous tumor cell vaccines as
adjuvant treatment of advanced ovarian cancer. Cancer Biother
Radiopharm. 14:443–449. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bachmann MF, Speiser DE, Mak TW and Ohashi
PS: Absence of costimulation and not the intensity of TCR signaling
is critical for the induction of T cell unresponsiveness in vivo.
Eur J Immunol. 29:2156–2166. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen L, Ashe S, Brady WA, et al:
Costimulation of antitumor immunity by the B7 counterreceptor for
the T lymphocyte molecules CD28 and CTLA-4. Cell. 71:1093–1102.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zheng P, Sarma S, Guo Y and Liu Y: Two
mechanisms for tumor evasion of preexisting cytotoxic T-cell
responses: lessons from recurrent tumors. Cancer Res. 59:3461–3467.
1999.PubMed/NCBI
|
|
15
|
Steinman RM: The dendritic cell system and
its role in immunogenicity. Annu Rev Immunol. 9:271–296. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Steinman RM: Dendritic cells and the
control of immunity: enhancing the efficiency of antigen
presentation. Mt Sinai J Med. 68:106–166. 2001.PubMed/NCBI
|
|
17
|
Young JW, Koulova L, Soergel SA, Clark EA,
Steinman RM and Dupont B: The B7/BB1 antigen provides one of
several costimulatory signals for the activation of CD4+ T
lymphocytes by human blood dendritic cells in vitro. J Clin Invest.
90:229–237. 1992.PubMed/NCBI
|
|
18
|
Inaba K, Witmer-Pack M, Inaba M, et al:
The tissue distribution of the B7-2 costimulator in mice: abundant
expression on dendritic cells in situ and during maturation in
vitro. J Exp Med. 180:1849–1860. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gong J, Nikrui N, Chen D, et al: Fusions
of human ovarian carcinoma cells with autologous or allogeneic
dendritic cells induce antitumor immunity. J Immunol.
165:1705–1711. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Koido S, Ohana M, Liu C, et al: Dendritic
cells fused with human cancer cells: morphology, antigen expression
and T cell stimulation. Clin Immunol. 113:261–269. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kaye S: Chemotherapy for ovarian cancer:
yesterday, today and tomorrow. Br J Cancer. 89:S1–S2. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dadmarz RD, Ordoubadi A, Mixon A, et al:
Tumor-infiltrating lymphocytes from human ovarian cancer patients
recognize autologous tumor in an MHC Class II-restricted fashion.
Cancer J Sci Am. 2:2631996.
|
|
23
|
Hayashi K, Yonamine K, Masuko-Hongo K, et
al: Clonal expansion of T cells that are specific for autologous
ovarian tumor among tumorinfiltrating T cells in humans. Gynecol
Oncol. 74:86–92. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang L, Conejo-Garcia JR, Katsaros D, et
al: Intratumoral T cells, recurrence, and survival in epithelial
ovarian cancer. N Engl J Med. 348:203–213. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fujita K, Ikarashi H, Takakuwa K, et al:
Prolonged disease-free period in patients with advanced epithelial
ovarian cancer after adoptive transfer of tumor-infiltrating
lymphocytes. Clin Cancer Res. 1:501–507. 1995.
|
|
26
|
Nijman H, van Diest P, Poort-Keesom R, et
al: T cell infiltration and MHC I and II expression in the presence
of tumor antigens: an immunohistochemical study in patients with
serous epithelial ovarian cancer. Eur J Obstet Gynecol Reprod Biol.
94:114–120. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Freedman R and Platsoucas C: Immunotherapy
for peritoneal ovarian carcinoma metastasis using ex vivo expanded
tumor infiltrating lymphocytes. Cancer Treat Res. 82:115–146. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schlienger K, Chu C, Woo E, et al: TRANCE-
and CD40 ligand matured dendritic cells reveal MHC class
I-restricted T cells specific for autologous tumor in late-stage
ovarian cancer patients. Clin Cancer Res. 9:1517–1527. 2003.
|
|
29
|
Pardoll D: Spinning molecular immunology
into successful immunotherapy. Nat Rev Immunol. 2:227–238. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Koidoa S, Nikruib N, Ohanac M, Xiac J,
Tanaka Y, Liuc C, Durfeec J, Lernerc A and Gong J: Assessment of
fusion cells from patient-derived ovarian carcinoma cells and
dendritic cells as a vaccine for clinical use. Gynecologic
Oncology. 99:462–471. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Adams M, Navabi H, Croston D, Coleman S,
Tabi Z, Clayton A, Jasani B and Mason MD: The rationale for
combined chemo/immunotherapy using a Toll-like receptor 3 (TLR3)
agonist and tumour-derived exosomes in advanced ovarian cancer.
Vaccine. 23:2374–2378. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Rosenberg S, Yang J and Restifo N: Cancer
immunotherapy: moving beyond current vaccines. Nat Med. 10:909–915.
2004. View
Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nowak A, Robinson B and Lake R: Synergy
between chemotherapy and immunotherapy in the treatment of
established murine solid tumors. Cancer Res. 63:4490–4496.
2003.PubMed/NCBI
|
|
34
|
Fattorossi A, Battaglia A, Ferrandina G,
et al: Neoadjuvant therapy changes the lymphocyte composition of
tumor-draining lymph nodes in cervical carcinoma. Cancer.
100:1418–1428. 2004. View Article : Google Scholar : PubMed/NCBI
|