Introduction
Prostate and breast carcinomas are clinically common
malignancies and often progress to bone metastasis (1–4). Bone
scintigraphy is a sensitive and efficient method for the detection
of bone metastases of malignant tumors, although it is considered
to be a nonspecific method. Bone scintigraphy has value in
determining the stage (1),
selecting therapeutic schedule, evaluating prognosis (2) and performing follow-up (3) for tumor patients. A number of studies
concerning bone scintigraphy of these tumors have been reported in
the literature, but a comparative study of the distribution of
metastatic bone lesions in prostate and breast carcinomas has not
been performed. In several previous studies (4–6), Tofe
et al(5) compared the
distribution of metastatic skeletal involvements of different
tumors by patient-based analyses. However, the total incidences of
bone metastasis in the tumor patients have significant differences
(breast carcinoma, 28 vs. 67%; prostate carcinoma, 35 vs. 62%) as
demonstrated in previous studies (5,6). If
the total incidence of bone metastasis of a certain tumor is very
high, the metastasis incidence of each category of bones (such as
the ribs and vertebrae) of the tumor is correspondingly high.
Accordingly, when the metastases of bones within the same bone
category are compared in different tumors, the total incidences of
bone metastasis may influence the results. Furthermore, the
incidence of bone metastasis cannot represent the constituent ratio
and distribution of certain metastatic bone lesions in the entire
metastatic bone lesion. The incidence of bone metastasis was
determined by patient-based analysis and was equal to the ratio of
the number of patients who had bone metastasis to the number of
total patients. Hence, it is not reasonable to evaluate the
distribution of the metastatic bone lesions by the incidence. The
results of other studies have shown that predilection sites and
total distribution characteristics of bone metastases were similar
in prostate (7,8) and breast (5,9,10)
carcinomas; the ribs, thoracic vertebrae, lumbar vertebrae and
ilium were reported to be the main predilection sites for the two
diseases. However, the results of the study by Conti et
al(2) indicated that the femur
of prostate carcinoma patients was the most frequent bone
metastatic site, which is different from the result of Huang et
al(7). It is thus clear that
there are controversies surrounding the distribution of bone
metastases.
We studied the distribution of bone metastases of
breast and prostate carcinomas using the lesion-based analysis
method. We classified the patients with metastatic bone diseases
according to the total number of metastatic bone lesions, and
studied the changes in distribution of metastatic bone lesions in
cases with different numbers of lesions. We also compared the
distributions between the two types of carcinoma. We found that the
distribution of metastatic bone lesions in breast and prostate
carcinomas was correlated with the lesion number and also had
different characteristics.
Patients and methods
Patients
In this study, 504 patients in whom bone
scintigraphies were performed were enrolled, including 360 patients
with breast carcinoma (4 males; 356 females; ages, 22–82 years;
median age, 50.0 years) and 144 male patients with prostate
carcinoma (ages, 38–92 years; median age, 72.5 years). All patients
received a definitive diagnosis using a pathological method. Only
one bone scintigraphy was registered for study. If necessary, the
other bone scintigraphies, performed before and after the
registered bone scintigraphy, were regarded as references for
diagnosis and were not registered. The clinical study was not
limited to a specific stage of disease. This study was approved by
the local Ethics Committees of Zhongnan Hospital of Wuhan
University, Wuhan, China, and informed consent was obtained from
all participants.
Imaging
SPECT with low-energy and high-resolution collimator
(Model #, E.CAM; Siemens Company, Hoffman Estates, IL, USA),
99Mo-99mTc generators and the methylene
diphosphonate (Beijing Institute of Atomic Energy in China,
Beijing, China) were used in this study. All patients were
instructed to drink ∼1,000 ml water within 2 h of the intravenous
injection of 740 MBq of 99mTc-methylene diphosphonate
and to urinate prior to bone scintigraphy. All planar bone scans,
including anterior and posterior projections, were performed ∼3 h
after the injection of imaging reagents, according to the following
conditions: supine posture of patients; matrix, 256 x 1024; zoom,
1.0; movement velocity of examination bed, 15–25 cm/min. If
necessary, additional local planar and SPECT bone imaging were
performed.
Diagnostic criteria of bone
metastasis
The interpretations of the 99mTc-MDP
planar bone scan and SPECT bone imaging were made as a consensus
reading of two nuclear medicine physicians, and that of the X-ray,
CT and MRI as a consensus reading of a nuclear medicine physician
and a radiological physician. According to the diagnostic method
described by Even-Sapir et al(11), the results of the bone scans were
interpreted as metastatic bone lesions under these circumstances:
i) Vertebral lesions of increased uptake involved the posterior
aspect of the vertebral body and pedicle, or involved the vertebrae
extensively (12,13); ii) rib lesions of increased uptake
exhibited the strip form (14);
iii) the lesions of increased uptake exhibited the lamellar form
with or without corroding multiple adjacent bones (14); iv) the lesions of decreased uptake
were confirmed to not be bone cysts and ischemic bone necrosis, or
accompanied progressive osteodynia symptoms; v) the lesions of
markedly increased uptake were confirmed to not be benign bone
diseases, or exhibited multiple sites and scrambled arrangement;
vi) the bone lesions, of increased or decreased uptake, were
confirmed to be bone metastases by X-ray, CT or MRI; vii) by
comparing the result of bone scans that were performed at different
times, the new bone lesions could not be interpreted as benign
diseases, or the lesions presented ‘flare phenomenon’ (15). The results of bone scans were
considered negative under the following circumstances: i) no
abnormal radiotracer uptake was detected; ii) there was
indeterminate decreased radioactivity in local bones; iii) the bone
lesions of increased or decreased radiotracer uptake were
characterized as benign disease.
Relevant data were collected by direct interviews or
from medical files on the trauma and surgical information in order
to exclude the possibility that the benign lesions were caused by
the surgery or trauma, and if necessary, the diagnosis was decided
by follow-up after more than six months. For patients with fewer
lesions or with vertebral lesions, especially those with only
lumbar lesions, the results of the bone X-ray, CT, MRI, local
planar bone imaging, SPECT bone imaging and previous bone
scintigraphies were comprehensively analyzed. The aim was to
exclude the common benign diseases of bones and joints, including
hyperosteogeny, osteophytes, bone-bridge, degenerative
osteoarthropathy and inflammatory disease, as much as possible.
Grouping
To study the correlation between the distribution
and the number of metastatic bone lesions and to compare the
distribution of the metastatic bone lesions between breast and
prostate carcinomas, we divided patients with bone metastasis into
three groups according to the total number of metastatic bone
lesions: few bone metastases, with the total number being 1–3;
moderate bone metastases, with the total number being 4–10;
extensive bone metastases, with the total number being >10.
Statistical analyses
Data were analyzed using the SPSS statistical
software (version 13.0; SPSS, Inc., Chicago, IL, USA). The
Chi-square test was performed to compare the difference between the
proportions. P<0.05 was considered to indicate a statistically
significant result.
Results
Incidence of bone metastasis
Of a total of 504 patients with malignant tumors,
252 developed bone metastases and a total of 3,324 metastatic bone
lesions were detected. The incidence of bone metastasis of prostate
carcinoma (70.8%; 102/144) was higher than that of breast carcinoma
(41.7%; 150/360; χ2=35.8, P=0.000).
Comparison of bone metastasis
distribution between breast and prostate carcinomas
The proportions of metastatic bone lesions of breast
and prostate carcinomas are listed in Tables I–IV. In cases with few bone metastases
(Table I), the proportions of
metastatic lesions of the lumbar vertebrae, ischium, pubis and
femur in prostate carcinoma patients were higher than those in
breast carcinoma patients; the proportions of metastatic lesions of
the ribs, sternum and skull in breast carcinoma patients were
higher than those in prostate carcinoma patients. In cases of
prostate carcinoma, 81.0% (47/58) of the metastatic bone lesions
were located in the thoracic vertebrae, lumbar vertebrae and
pelvis, whereas in breast carcinoma, 65.6% (99/151) of lesions were
located in the thoracic skeleton (Table
II). In cases with moderate bone metastases (Table III), the proportions of metastatic
lesions of the ribs and sternum in breast carcinoma patients were
higher than those in prostate carcinoma patients. In cases with
extensive bone metastases (Table
IV), the proportions of metastatic lesions of the ilium,
ischium, pubis and ribs in prostate carcinoma patients were higher
than those in breast carcinoma patients; the proportion of
metastatic lesions of the skull in breast carcinoma patients was
higher than that in prostate carcinoma patients; however, the
proportions of metastatic lesions of the lumbar vertebrae, sternum
and femur were not significantly different between breast and
prostate carcinomas.
 | Table IComparison of bone metastases (n=209)
in cases with few bone metastases in breast and prostate
carcinomas. |
Table I
Comparison of bone metastases (n=209)
in cases with few bone metastases in breast and prostate
carcinomas.
| Prostate carcinoma
(n=58)
| Breast carcinoma
(n=151)
| | |
|---|
| Skeleton | n | % | n | % | χ2 | P-value |
|---|
| Cervical
vertebrae | 2 | 3.45 | 3 | 1.99 | 0.357 | 0.550 |
| Thoracic
vertebrae | 10 | 17.24 | 24 | 15.89 | 0.055 | 0.814 |
| Lumbar vertebrae | 23 | 39.66 | 21 | 13.91 | 15.431 | 0.000 |
| Sacrococcyx | 2 | 3.45 | 6 | 3.97 | 0.032 | 0.858 |
| Ilium | 6 | 10.34 | 11 | 7.29 | 0.502 | 0.478 |
| Ischium | 2 | 3.45 | 0 | 0.00 | 5.178 | 0.023 |
| Pubis | 4 | 6.90 | 1 | 0.66 | 6.070 | 0.014 |
| Ribs | 5 | 8.62 | 41 | 27.15 | 9.632 | 0.002 |
| Sternum | 1 | 1.72 | 27 | 17.88 | 12.719 | 0.000 |
| Skull | 0 | 0.00 | 6 | 3.97 | 3.968 | 0.046 |
| Scapula | 0 | 0.00 | 4 | 2.65 | 2.630 | 0.105 |
| Collar bone | 0 | 0.00 | 3 | 1.99 | 1.967 | 0.161 |
| Humerus | 0 | 0.00 | 3 | 1.99 | 1.967 | 0.161 |
| Femur | 3 | 5.17 | 1 | 0.66 | 3.930 | 0.047 |
| Radioulnar and
tibiofibular | 0 | 0.00 | 0 | 0.00 | - | - |
| Bones of hands and
feet | 0 | 0.00 | 0 | 0.00 | - | - |
| Table IVComparison of bone metastases
(n=2770) in cases with extensive bone metastases in breast and
prostate carcinomas. |
Table IV
Comparison of bone metastases
(n=2770) in cases with extensive bone metastases in breast and
prostate carcinomas.
| Prostate carcinoma
(n=1781)
| Breast carcinoma
(n=989)
| | |
|---|
| Skeleton | n | % | n | % | χ2 | P-value |
|---|
| Cervical
vertebrae | 53 | 2.98 | 37 | 3.74 | 1.162 | 0.281 |
| Thoracic
vertebrae | 247 | 13.87 | 135 | 13.65 | 0.026 | 0.873 |
| Lumbar
vertebrae | 115 | 6.46 | 71 | 7.18 | 0.524 | 0.469 |
| Sacrococcyx | 80 | 4.49 | 37 | 3.74 | 0.902 | 0.342 |
| Ilium | 248 | 13.92 | 97 | 9.81 | 10.206 | 0.001 |
| Ischium | 96 | 5.39 | 36 | 3.64 | 4.467 | 0.035 |
| Pubis | 80 | 4.49 | 29 | 2.93 | 4.277 | 0.039 |
| Ribs | 551 | 30.94 | 269 | 27.20 | 4.297 | 0.038 |
| Sternum | 56 | 3.14 | 43 | 4.35 | 2.604 | 0.107 |
| Skull | 60 | 3.37 | 97 | 9.81 | 46.771 | 0.000 |
| Scapula | 44 | 2.47 | 37 | 3.74 | 3.502 | 0.061 |
| Collar bone | 21 | 1.18 | 14 | 1.42 | 0.280 | 0.596 |
| Humerus | 36 | 2.02 | 33 | 3.34 | 4.363 | 0.037 |
| Femur | 90 | 5.05 | 52 | 5.26 | 0.054 | 0.815 |
| Radioulnar and
tibiofibular | 4 | 0.22 | 2 | 0.20 | 0.015 | 0.903 |
| Bones of hands and
feet | 0 | 0.00 | 0 | 0.00 | - | - |
| Table IIComparison of bone metastasis
distribution between breast and prostate carcinomas. |
Table II
Comparison of bone metastasis
distribution between breast and prostate carcinomas.
| Few bone metastases
| Extensive bone
metastases
|
|---|
Bca (n=151)
| Pca (n=58)
| | | Bca (n=989)
| Pca (n=1781)
| | |
|---|
| Metastatic
position | n | % | n | % | χ2 | P-value | n | % | n | % | χ2 | P-value |
|---|
| Vertebrae and
pelvis | 63 | 41.7 | 47 | 81.0 | 27.6 | 0.000 | 405 | 41.0 | 866 | 48.6 | 15.1 | 0.000 |
| Thoracic
skeleton | 99 | 65.6 | 16 | 27.6 | 24.8 | 0.000 | 498 | 50.4 | 919 | 51.6 | 0.4 | 0.530 |
| Table IIIComparison of bone metastases (n=345)
in cases with moderate bone metastases in breast and prostate
carcinomas. |
Table III
Comparison of bone metastases (n=345)
in cases with moderate bone metastases in breast and prostate
carcinomas.
| Prostate carcinoma
(n=161)
| Breast carcinoma
(n=184)
| | |
|---|
| Skeleton | n | % | n | % | χ2 | P-value |
|---|
| Cervical
vertebrae | 5 | 3.11 | 0 | 0.00 | 7.705 | 0.006 |
| Thoracic
vertebrae | 39 | 24.22 | 34 | 18.48 | 1.696 | 0.193 |
| Lumbar
vertebrae | 22 | 13.66 | 24 | 13.04 | 0.029 | 0.866 |
| Sacrococcyx | 14 | 8.70 | 8 | 4.35 | 2.730 | 0.098 |
| Ilium | 22 | 13.66 | 23 | 12.50 | 0.103 | 0.749 |
| Ischium | 11 | 6.83 | 10 | 5.43 | 0.293 | 0.589 |
| Pubis | 7 | 4.35 | 4 | 2.17 | 1.320 | 0.251 |
| Ribs | 22 | 13.66 | 53 | 28.80 | 11.908 | 0.001 |
| Sternum | 1 | 0.62 | 14 | 7.61 | 12.215 | 0.000 |
| Skull | 5 | 3.11 | 2 | 1.09 | 1.796 | 0.180 |
| Scapula | 0 | 0.00 | 4 | 2.17 | 5.070 | 0.024 |
| Collar bone | 1 | 0.62 | 2 | 1.09 | 0.222 | 0.638 |
| Humerus | 5 | 3.11 | 3 | 1.63 | 0.827 | 0.363 |
| Femur | 7 | 4.35 | 3 | 1.63 | 2.290 | 0.130 |
| Radioulnar and
tibiofibular | 0 | 0.00 | 0 | 0.00 | - | - |
| Bones of hands and
feet | 0 | 0.00 | 0 | 0.00 | - | - |
Change of predilection sites in cases
with different numbers of lesions
The results showed that the ribs, thoracic
vertebrae, lumbar vertebrae and ilium were predilection sites of
bone metastases, but on the basis of the proportions, the sequences
of these predilection sites were different in cases with different
numbers of lesions and in different tumors. For prostate carcinoma,
in decreasing order, the predilection sites of bone metastasis were
the lumbar vertebrae, thoracic vertebrae, ilium and ribs in cases
with few bone metastases (Table I);
the thoracic vertebrae, lumbar vertebrae, ilium and ribs in cases
with moderate bone metastases (Table
III); and the ribs, ilium, thoracic vertebrae and lumbar
vertebrae in cases with extensive bone metastases (Table IV). For breast carcinoma, in
decreasing order, the predilection sites of bone metastasis were
the ribs, sternum, thoracic vertebrae, lumbar vertebrae and ilium
in cases with few bone metastases (Table II). The ribs, thoracic vertebrae,
lumbar vertebrae, ilium and sternum in cases with moderate bone
metastases (Table III); and the
ribs, thoracic vertebrae, ilium, skull and lumbar vertebrae in
cases with extensive bone metastases (Table IV).
Proportion of non-predilection sites in
different lesions
The results in Tables
I, III and IV show that the cervical vertebrae,
scapula, collar bone and humerus did not have a higher proportion
of bone metastasis in breast and prostate carcinomas compared to
the predilection sites in the ribs, thoracic vertebrae, lumbar
vertebrae and ilium. For prostate carcinoma, no metastatic bone
lesion was detected in these bones, with the exception of the
cervical vertebrae in the few bone metastases group (Table I). The metastatic lesion proportions
of the radioulnar, tibiofibular and bones of the hands and feet
were lowest in breast and prostate carcinomas, and no metastatic
lesion was detected in these bones in either the few or moderate
bone metastases groups, whereas only a small number of metastatic
bone lesions was detected in the extensive bone metastases group.
Therefore, the radioulnar, tibiofibular and bones of the hands and
feet were non-predilection site of bone metastasis.
Comparison of bone metastasis
distribution in cases with different numbers of lesions
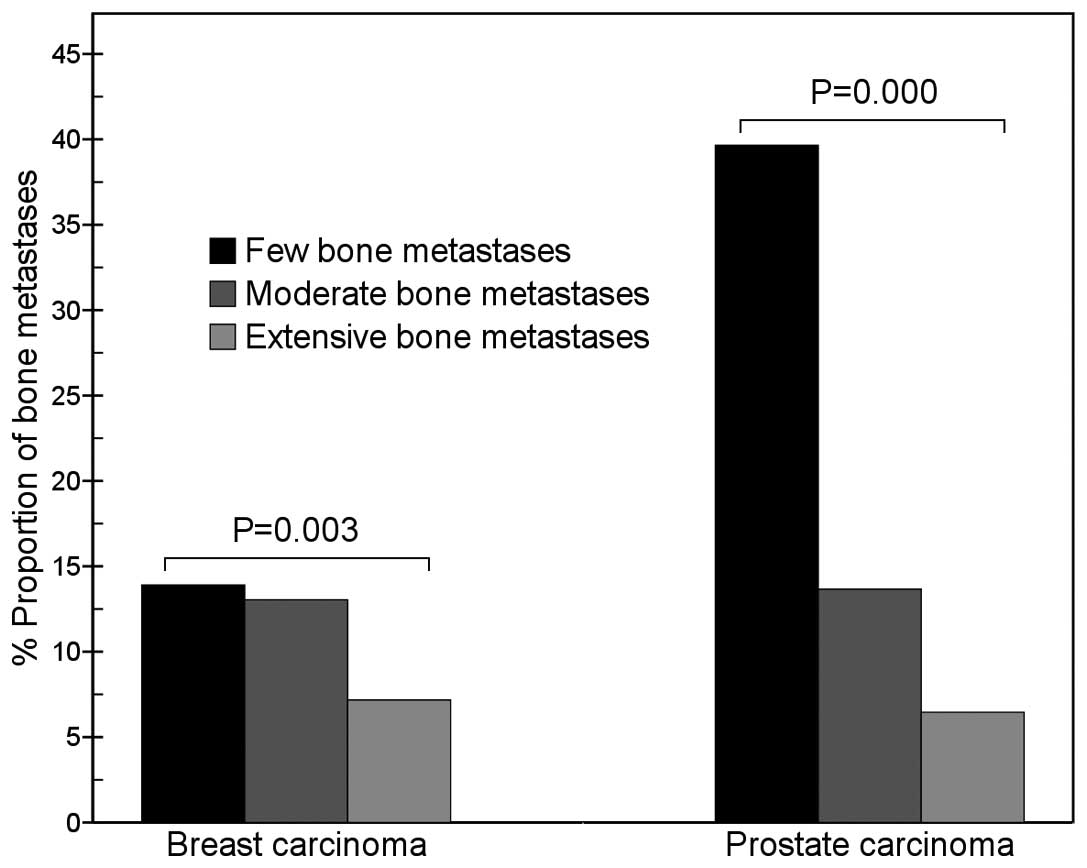
For prostate carcinoma, between the three groups
with different numbers of lesions, the differences in the
proportion of lesions in the thoracic vertebrae
(χ2=11.3, P=0.003), lumbar vertebrae
(χ2=56.1, P=0.000), ribs (χ2=39.1, P=0.000)
and scapula (χ2=10.3, P=0.006) were significant. The
proportion of metastatic lumbar vertebrae lesions in the few bone
metastases group (39.7%; 23/58) was significantly higher than that
in the moderate bone metastases group (13.7%; 22/161;
χ2=16.1, P=0.000); and that in the moderate bone
metastases group (13.7%) was significantly higher than that in the
extensive bone metastases group (6.5%; 115/1781; χ2=9.6,
P=0.002; Fig. 1). The proportion of
metastatic rib lesions in the extensive bone metastases group
(30.9%; 551/1781) was significantly higher than that in the
moderate bone metastases group (13.7%; 22/161; χ2=24.2,
P=0.000) and that in the few bone metastases group (8.6%; 5/58;
χ2=16.5, P=0.000; Fig.
2).
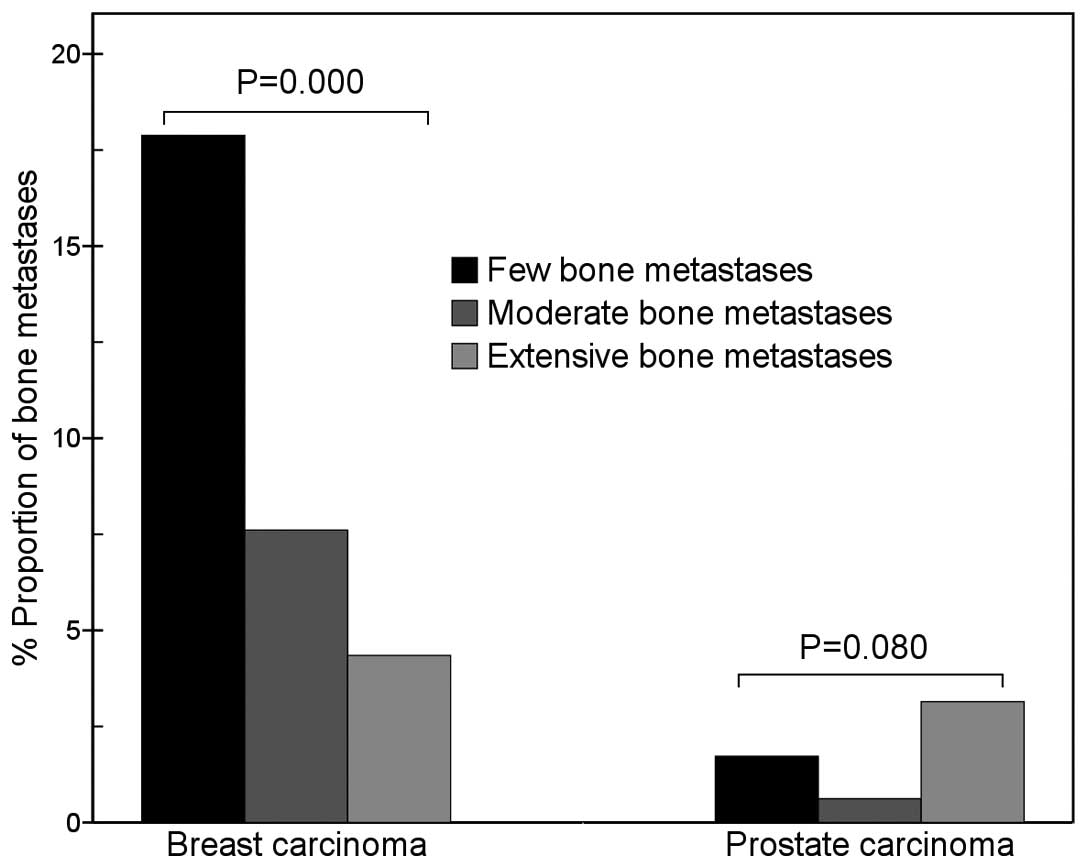
 | Figure 2Comparison of rib metastases between
breast and prostate carcinomas. The results show that with an
increase in the number of metastatic bone lesions, the proportion
of metastatic rib lesions of prostate carcinoma gradually increased
(χ2=39.1, P=0.000), but that of breast carcinoma did not
change (χ2=0.2, P=0.903). In the few bone metastases
group, the proportion of metastatic rib lesions of prostate
carcinoma was markedly lower than that of breast carcinoma (8.6 vs.
27.2%, χ2=9.6, P=0.002), but in the extensive bone
metastases group, it was similar to that of breast carcinoma (30.9
vs. 27.2%, χ2=4.3, P=0.038). |
For breast carcinoma, metastases in the cervical
vertebrae (χ2=13.5, P=0.001), lumbar vertebrae
(χ2=11.3, P=0.003), ischium (χ2=12.6,
P=0.002), sternum (χ2=31.2, P=0.000), skull
(χ2=26.5, P=0.000) and femur (χ2=13.6,
P=0.001) were present in significantly different proportions in
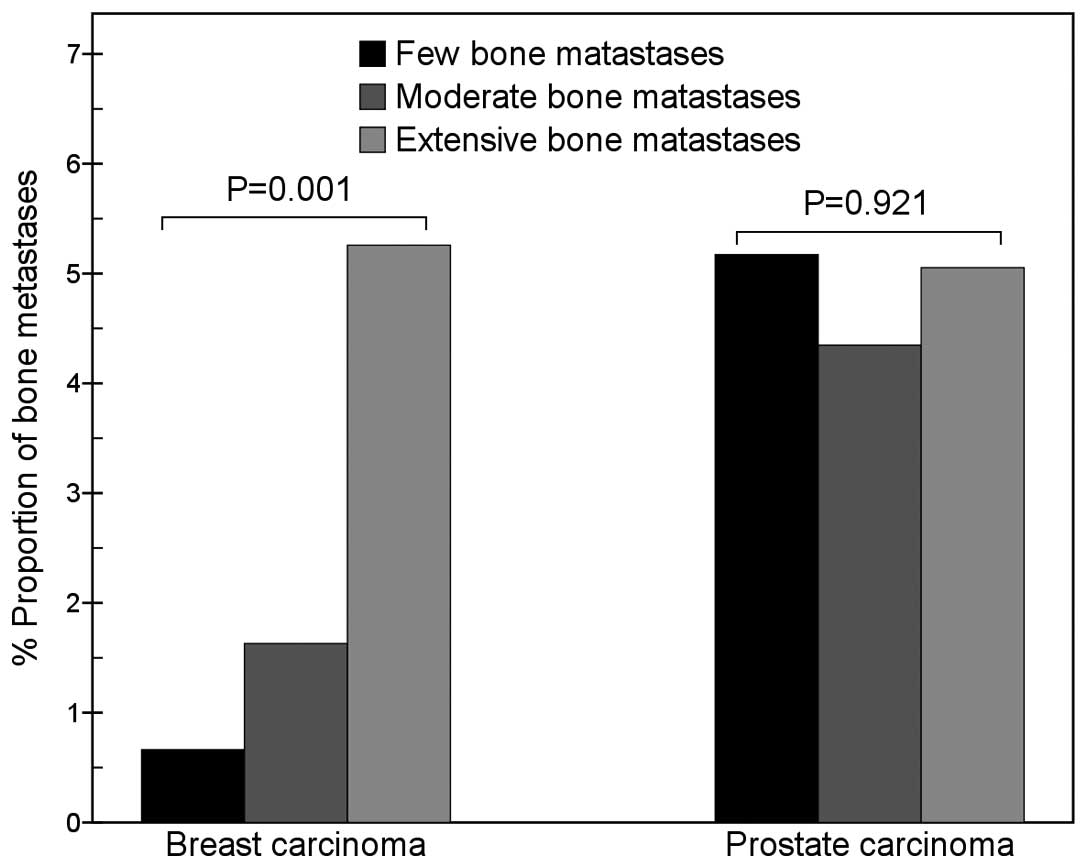
cases with different numbers of bone metastases. The proportion of
metastatic sternum lesions in the few bone metastases group (17.9%;
27/151) was significantly higher than that in the moderate bone
metastases group (7.6%; 14/184; χ2=8.2, P=0.004) and
that in the extensive bone metastases group (4.3%; 43/989;
χ2=30.7, P=0.000; Fig.
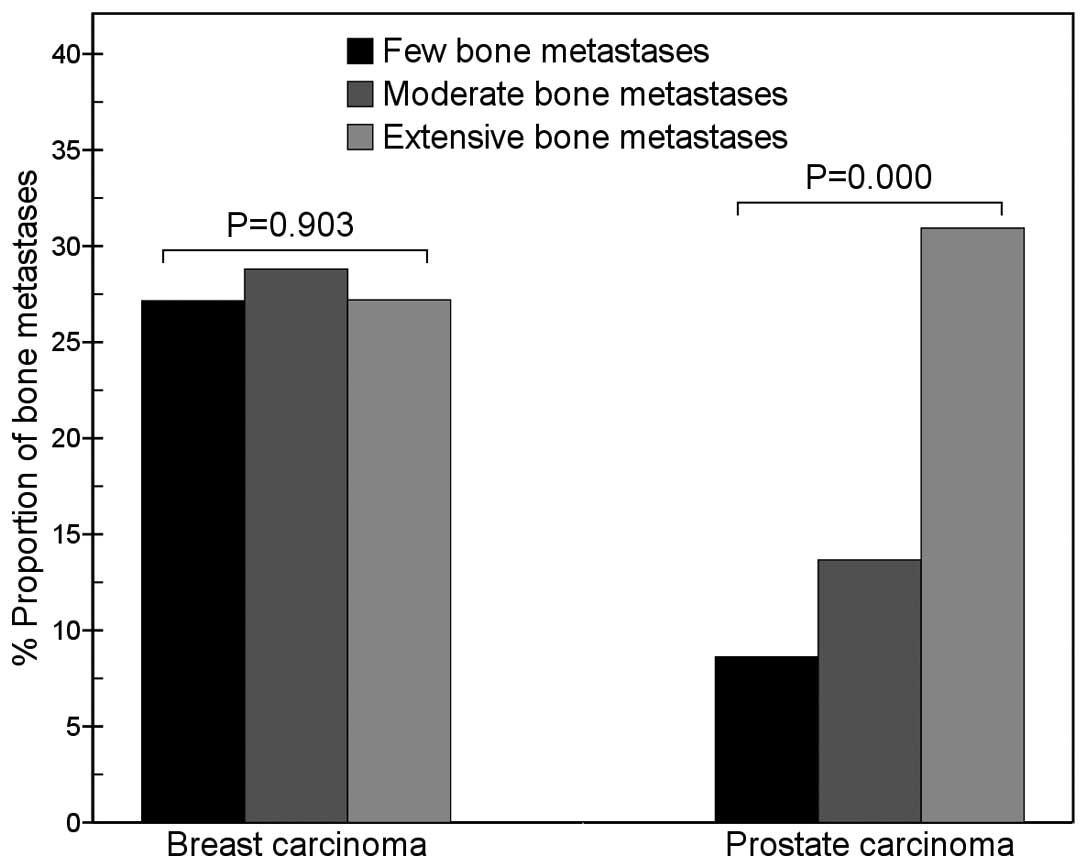
3). The proportion of metastatic femur lesions gradually
increased with an increase in the total number of metastatic bone
lesions (Fig. 4).
Discussion
Predilection and non-predilection sites
of bone metastases
The most common human carcinomas (breast and
prostate) have a great avidity for bone, frequently leading to
painful and untreatable consequences. Patients with advanced breast
and prostate carcinomas frequently develop bone metastases, and the
risks are extremely high (16).
There is a wide range in the reported incidence of bone metastasis.
In the present study, the incidence of bone metastasis of prostate
carcinoma (70.8%) was higher than that of breast carcinoma (41.7%).
The study by Wilson and Calhoun (6)
reported that the difference in bone metastasis incidence between
breast and prostate carcinomas was not significant (28 vs. 35%,
χ2=0.4, P=0.529). In the study by Tofe et
al(5), the incidences of bone
metastasis of breast and prostate carcinomas were higher than that
reported by Wilson and Calhoun and were similar in the two types of
carcinoma (67 vs. 62%, χ2=1.3, P=0.258). Therefore, our
result is different from the outcomes reported by Wilson and
Calhoun (6) and by Tofe et
al(5), which may be due to the
different study populations.
Our results show that the ribs, thoracic vertebrae,
lumbar vertebrae and ilium are the main predilection sites of
breast and prostate carcinomas and that the middle-distal bones of
the extremities are non-predilection sites, which are the common
features of the distribution of metastatic bone lesions. The
features are similar to the results reported in previous studies
(5–10). Metastatic bone lesions are commonly
distributed in these predilection sites and are rarely observed in
the middle-distal bones of the extremities.
Correlation between distribution and
number of metastatic bone lesions
In the present study, the proportion of metastatic
lesions in certain bones was significantly different in cases with
different numbers of metastatic bone lesions. With an increase in
the number of metastatic bone lesions, the proportion of rib
lesions in prostate carcinoma patients and that of femur lesions in
breast carcinoma patients gradually increased; by contrast, those
of lumbar vertebrae lesions in prostate carcinoma patients and
sternum lesions in breast carcinoma patients gradually decreased.
Accordingly, with regards to the proportion of metastatic bone
lesions, the tendency of different bones to change varied. These
outcomes demonstrate that the distribution of metastatic bone
lesions is not always fixed, but is changed with an increase in the
number of metastatic bone lesions. Therefore, the distribution of
metastatic bone lesions is correlated with the number of bone
lesions, and differs in cases with different numbers of metastatic
bone lesions. This may be due to the non-random spreading of breast
or prostate carcinoma cells, which do not spread to different bones
proportionately, but prefer to metastasize to certain bones first
and then to other bones via a different pathway.
Correlation between predilection site and
number of metastatic bone lesions
As the distribution of metastatic bone lesions
changes with the total number of lesions, the predilection sites of
bone metastases may also be different in cases with different
numbers of metastatic bone lesions. In the present study, the
predilection sites of bone metastases or the sequence of the
predilection sites were often different in cases with different
numbers of lesions, which indicates that the predilection sites of
bone metastases are correlated with the total number of metastatic
bone lesions.
Patients with few bone metastases are considered to
be in the early stage of bone metastases; patients with extensive
bone metastases have a great number of metastases, so they are
considered to have developed advanced stage bone metastases. Our
results show that the lumbar vertebrae are the main predilection
site of prostate carcinoma in the early stage, rather than the
ribs. The hypothesis that tumor cells invade the lumbar vertebrae
early in the disease and later metastasize to the ribs may be
explained by spreading through the Batson venous plexus (17). Tumor cells usually spread to the
lumbar vertebrae at an early stage via the Batson venous plexus,
and then metastasize to the ribs and other bones; therefore, the
ribs are the main predilection site of prostate carcinoma in
advanced stages. However, the ribs of breast carcinoma patients are
the most important predilection site in early and advanced stages,
which is different from the distribution of rib lesions in prostate
carcinoma patients. In the early stage, patients with breast
carcinoma progress to rib metastasis more frequently than patients
with prostate carcinoma. The reason for the difference may be
different spreading mechanisms. Breast carcinoma cells may directly
invade the neighboring ribs at an early stage and may also spread
to the ribs via the aorta following metastasis to lung. However,
the anatomical features of the prostate-Batson venous plexus path
mean that prostate carcinoma cells are unable to reach the ribs at
an early stage, but are able to at an advanced stage. These
different mechanisms influence the early distribution of metastatic
bone lesions, and so the early distribution of rib lesions is
different in breast and prostate carcinoma. For breast carcinoma,
after the ribs the sternum is the main predilection site of bone
metastasis at early stages. Ohtake et al(18) suggested that breast carcinoma cells
spread to the sternum via the parasternal lymph nodes, which is the
reason that the sternum is invaded earlier by carcinoma cells than
a number of other bones, except the ribs.
Different distributions of metastatic
bone lesions in breast and prostate carcinoma
In the present study, most bone lesions of prostate
carcinoma patients were distributed in the vertebrae and pelvis in
the early stage, but those of breast carcinoma patients were
located in the thoracic skeleton; therefore, the early
distributions were different. Our results demonstrate that
differences in the distribution of metastatic lesions of certain
bones were present between breast and prostate carcinomas and also
in cases with different numbers of lesions. In cases with few bone
metastases, the proportion of metastatic lumbar lesions of prostate
carcinoma (39.7%) was approximately three times higher than that of
breast carcinoma (13.9%); by contrast, the proportion of metastatic
rib lesions of breast carcinoma (27.2%) was three to four times
higher than that of prostate carcinoma (8.6%). The results show
that the distribution of early stage bone metastases in the lumbar
vertebrae and ribs is markedly different in breast and prostate
carcinomas. Furthermore, the distribution of early stage metastatic
bone lesions in breast carcinoma is characterized by a markedly
higher proportion of sternum metastases and a lower proportion of
femur metastases than that of prostate carcinoma. These features
are useful in the early and differential diagnosis of bone
metastases in breast and prostate carcinomas. In cases with
extensive bone metastases, a marked difference was observed in the
proportion of breast carcinoma metastases to the skull, which was
approximately three times higher than that in prostate carcinoma.
The reason that the skull of breast carcinoma patients is more
frequently invaded in the advanced stage of bone metastases may be
that breast carcinoma cells spread to the skull by the lung-aorta
route and also via the Batson venous plexus. The spreading to the
skull of breast carcinoma cells may be easier than that of prostate
carcinoma cells, via both the Batson venous plexus and lung-aorta
paths. Therefore, the difference of predilection sites of bone
metastases between breast and prostate carcinomas is most marked in
cases with few bone metastases, but not in cases with extensive
bone metastases.
Conclusion
The distributions of metastatic bone lesions in
breast and prostate carcinomas not only have common features, but
also have different characteristics. In the early stage, metastatic
bone lesions of breast carcinoma are distributed mainly in the
thoracic skeleton, but those of prostate carcinoma are mainly
observed in the vertebrae and pelvis. The most noteworthy finding
of the present study is that the distribution of bone metastases is
correlated with the total number of metastatic bone lesions of
patients. With an increase in the metastatic bone lesion number,
the distribution of metastatic lesions of certain bones markedly
changes, and the trend of the metastatic lesion distributions
differs in certain bones or in two types of tumor. The bones which
change most prominently are the ribs and lumbar vertebrae in
prostate carcinoma and the sternum and femur in breast carcinoma.
The proportion of metastatic bone lesions in the lumbar vertebrae
in prostate carcinoma and the sternum in breast carcinoma markedly
decreases with an increase in the total number of metastatic bone
lesions; however, the proportions of lesions in the ribs in
prostate carcinoma and the femur in breast carcinoma gradually
increase with an increase in the number of lesions, which is
different from many other bones. Our results indicate that the
lumbar vertebrae in prostate carcinoma and the ribs and sternum in
breast carcinoma are frequently invaded in the early stage of bone
metastasis; however, the ribs in prostate carcinoma are seldom
invaded in the early stage, but are invaded in the advanced stage.
The difference of predilection sites between breast and prostate
carcinomas is marked in cases with few bone metastases, but not in
cases with extensive bone metastases. Understanding these different
features of metastatic bone lesions in breast and prostate
carcinomas is useful for an early and differential diagnosis of the
diseases.
Acknowledgements
The authors thank Dr Xiang-yuan Zhang
and Dr Ling-long Jiang for their technical assistance, and Dr
Chenling Xiong from the Gene Diagnosis Center of Zhongnan Hospital
for the assistance in the language editing.
References
|
1
|
Lin K, Szabo Z, Chin BB and Civelek AC:
The value of a baseline bone scan in patients with newly diagnosed
prostate cancer. Clin Nucl Med. 24:579–582. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Conti G, La Torre G, Cicalese V, et al:
Prostate cancer metastases to bone: Observational study for the
evaluation of clinical presentation, course and treatment patterns.
Presentation of the METAURO protocol and of patient baseline
features. Arch Ital Urol Androl. 80:59–64. 2008.
|
|
3
|
Maffioli L, Florimonte L, Pagani L, Butti
I and Roca I: Current role of bone scan with phosphonates in the
follow-up of breast cancer. Eur J Nucl Med Mol Imaging. 31(Suppl
1): S143–S148. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Osmond JD III, Pendergrass HP and Potsaid
MS: Accuracy of 99mTc-diphosphonate bone scans and
roentgenograms in the detection of prostate, breast and lung
carcinoma metastases. Am J Roentgenol Radium Ther Nucl Med.
125:972–977. 1975.
|
|
5
|
Tofe AJ, Francis MD and Harvey WJ:
Correlation of neoplasms with incidence and localization of
skeletal metastases: An analysis of 1355 diphosphonate bone scans.
J Nucl Med. 16:986–989. 1975.PubMed/NCBI
|
|
6
|
Wilson MA and Calhoun FW: The distribution
of skeletal metastases in breast and pulmonary cancer: concise
communication. J Nucl Med. 22:594–597. 1981.PubMed/NCBI
|
|
7
|
Huang CY, Hsu HC, Chang CH, Tseng KF and
Fong YC: Prostate cancer with bone metastases: a clinical pofile.
Mid Taiwan J Med. 11:82–89. 2006.
|
|
8
|
Picchio M, Spinapolice EG, Fallanca F,
Crivellaro C, Giovacchini G, Gianolli L and Messa C: [11C] Choline
PET/CT detection of bone metastases in patients with PSA
progression after primary treatment for prostate cancer: comparison
with bone scintigraphy. Eur J Nucl Med Mol Imaging. 39:13–26.
2012.
|
|
9
|
Jacobson AF, Stomper PC, Jochelson MS,
Ascoli DM, Henderson IC and Kaplan WD: Association between number
and sites of new bone scan abnormalities and presence of skeletal
metastases in patients with breast cancer. J Nucl Med. 31:387–392.
1990.PubMed/NCBI
|
|
10
|
Mohammadzadeh M, Alikhah H and Zareh AG:
Comparison of bone scan with carbohydrate antigen 15-3 for
evaluation of bone metastasis of breast cancer. Pak J Biol Sci.
13:175–179. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Even-Sapir E, Metser U, Mishani E,
Lievshitz G, Lerman H and Leibovitch I: The detection of bone
metastases in patients with high-risk prostate cancer:
99mTc-MDP Planar bone scintigraphy, single-and
multi-field-of-view SPECT, 18F-fluoride PET, and
18F-fluoride PET/CT. J Nucl Med. 47:287–297.
2006.PubMed/NCBI
|
|
12
|
Gate GF: SPECT bone scanning of the spine.
Semin Nucl Med. 28:78–94. 1998. View Article : Google Scholar
|
|
13
|
Even-Sapir E, Martin RH, Barnes DC,
Pringle CR, Iles SE and Mitchell MJ: Role of SPECT in
differentiating malignant from benign lesions in the lower thoracic
and lumbar vertebrae. Radiology. 187:193–198. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang CY and Zhang XY: Evaluation of
eikonic characteristic of skeletal metastasis of primary pulmonary
carcinoma with 99Tcm methylene diphosphonate
whole-body bone scans. Chinese-German J Clin Oncol. 9:435–440.
2010. View Article : Google Scholar
|
|
15
|
Cook GJ, Venkitaraman R, Sohaib AS, et al:
The diagnostic utility of the flare phenomenon on bone scintigraphy
in staging prostate cancer. Eur J Nucl Med Mol Imaging. 38:7–13.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mundy GR: Metastasis to bone: causes,
consequences and therapeutic opportunities. Nat Rev Cancer.
2:584–593. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bubendorf L, Schöpfer A, Wagner U, et al:
Metastatic patterns of prostate cancer: an autopsy study of 1,589
patients. Hum Pathol. 31:578–583. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ohtake E, Murata H and Maruno H: Bone
scintigraphy in patients with breast cancer: malignant involvement
of the sternum. Radiat Med. 12:25–28. 1994.PubMed/NCBI
|