Introduction
Colorectal cancer (CRC) was the third most common
type of malignancy and the third leading cause of cancer-related
mortality (for both genders) worldwide in 2011 (1). At present, the pathogenesis of
colorectal cancer remains unclear, and early detection remains the
most promising approach to improving long-term survival of patients
with CRC (2–4). Numerous molecular markers, including
the carcinoembryonic antigen (CEA), have been used for detecting
CRC (5,6). However, these biomarkers do not
provide sufficient sensitivity and reliability for the detection of
CRC (7,8). Thus, there is an urgent demand for the
detection of new biomarkers that are capable of serving as
diagnostic and prognostic markers for CRC.
With the invention and development of mass
spectrometry (MS), proteomics analysis is currently considered to
be a strong tool for global evaluation of protein expression and
has been widely applied in analysis of diseases, particularly in
cancer research (9–12). In our previous study, we compared
the secretome of fresh-cultured colorectal tissues and paired
normal colorectal tissues. By adopting the proteomics strategy of
one-dimensional gel electrophoresis coupled with liquid
chromatography-tandem mass spectrometry and quantification with
label-free spectral counting, 123 differentially expressed secreted
proteins (DESPs) were identified. One of the top 10 upregulated
DESPs, EFEMP2, was validated as a serum biomarker in the early
stage of CRC (13).
In the present study, another protein,
matrix-remodeling associated (MXRA) protein, was selected for
investigation into tumorigenesis in CRC, as few previous studies
have included this protein.
Materials and methods
Tissue samples
In our study, 176 tissue samples were used,
including 156 CRC tissues and paired normal tissues from CRC
patients who had not received pre-operative chemotherapy or
radiotherapy, and 20 adenoma tissues from the control subjects. For
the immunohistochemistry (IHC) experiment, one set of these tissues
was cut into formalin-fixed, paraffin-embedded tissue blocks. For
the quantitative real-time PCR (qRT-PCR) experiment, the other set
of these tissues was immediately frozen in liquid nitrogen and then
stored at −80°C until use. Tumor staging was classified according
to the TNM classification system (UICC). The clinical features of
these tissue samples are described in Table I. All tissue samples were obtained
between September 2009 and October 2010 in the Xinhua Hospital
Affiliated to Shanghai Jiaotong University School of Medicine. The
present study was approved by the Xinhua Hospital Ethics Committee
and conducted with the consent of all patients.
 | Table I.Correlation of MXRA5 protein
expression with CRC patients’ pathological features. |
Table I.
Correlation of MXRA5 protein
expression with CRC patients’ pathological features.
| Clinical
features | No. of cases | MXRA5 positive | P-value |
|---|
| Gender | 156 | | 0.791 |
| Male | 88 | 60 (68.2%) | |
| Female | 68 | 45 (66.2%) | |
| Age (years) | 156 | | 0.400 |
| ≤60 | 54 | 34 (63.0%) | |
| >60 | 102 | 71 (69.6%) | |
| Lesion sites | 156 | | 0.026 |
| Colon | 75 | 57 (76.0%) | |
| Rectum | 81 | 48 (59.3%) | |
| Gross pathology | 156 | | 0.471 |
| Exophytic | 43 | 29 (67.4%) | |
| Exophytic and
ulceration | 6 | 3 (50.0%) | |
| Ulceration | 97 | 68 (70.1%) | |
| Infiltrative | 10 | 5 (50.0%) | |
| Tumor diameter | 156 | | 0.470 |
| ≤5 cm | 89 | 62 (69.7%) | |
| >5 cm | 67 | 43 (64.2%) | |
| Differentiation | 156 | | 0.818 |
| Well | 14 | 10 (71.4%) | |
| Moderate | 132 | 91 (68.9%) | |
| Poor | 10 | 6 (60.0%) | |
| TNM staging | 156 | | 0.032 |
| I and II | 55 | 31 (56.4%) | |
| III and IV | 101 | 74 (73.3%) | |
| Invasion | 156 | | 0.999 |
| T1 | 3 | 2 (66.7%) | |
| T2 | 42 | 28 (66.7%) | |
| T3 | 21 | 14 (66.7%) | |
| T4 | 90 | 61 (67.8%) | |
| Lymph metastasis | 156 | | 0.082 |
| N0 | 55 | 31 (56.4%) | |
| N1 | 47 | 33 (70.2%) | |
| N2 | 54 | 41 (75.9%) | |
| Metastasis | 156 | | 0.043 |
| Present | 70 | 53 (75.7%) | |
| Liver
metastasis | 31 | 21 (67.7%) | |
| Omental
metastasis | 34 | 28 (82.4%) | |
| Pelvic cavity
metastasis | 24 | 17 (70.8%) | |
| Lung
metastasis | 5 | 1 (20.0%) | |
| Not present | 86 | 52 (60.5%) | |
IHC and tissue microarray
All tissues mentioned previously were made into
sections and two tissue microarrays. The sections were stained with
hematoxylin and eosin (H&E) to ensure that the sectioned block
contained either normal or tumor cells. Other sections were then
stained immunohisto-chemically. First, sections were deparaffinized
in xylene and then rehydrated in a series of ethanol solutions of
increasing strength. In order to increase specificity and
sensitivity, sections were pretreated by microwaving for 5 min on
high mode and then 10 min on middle mode in citrate buffer, pH 6.5.
Peroxidase activity was blocked with 3%
H2O2-methanol for 30 min and sections were
incubated with normal goat serum for 30 min to eliminate
non-specific staining. Sections were incubated with anti-human
MXRA5 polyclonal antibodies diluted at 1:10 (SAB1402656, Sigma, St.
Louis, MO, USA) overnight at 4°C. Then, sections were washed 3
times with phosphate-buffered saline (PBS) and incubated with
secondary antibody (GK500705; Gene Company Ltd., Shanghai, China)
for another 30 min at room temperature. Following three 5-min
rinses in PBS, staining was completed with 10 min incubation with
3,3′-diaminobenzidine (DAB) solution. Finally, sections were
counterstained with 0.1% hematoxylin and coverslipped.
For the assessment, five representative fields were
assessed per section at ×200 magnification with a light microscope
(Carl Zeiss, Göttingen, Germany). The immunostaining was evaluated
according to the following standards; staining intensity was
classified as 0 (lack of staining), 1 (mild staining), 2 (moderate
staining) or 3 (strong staining), and the percentage of staining
was designated 1 (<25%), 2 (25–50%), 3 (51–75%) or 4 (>75%).
For each section, the semi-quantitative score was calculated by
multiplying these two values (which ranged from 0–12) and the
result was defined as either negative (0), weakly positive (1–3),
positive (4–7) or strongly positive (8–12). Two histopathologists
blindly reviewed the slides and evaluated the data.
RNA extraction and qRT-PCR
Among the 156 CRC tissues, 70 CRC tissues and their
matched normal tissues were randomly selected for RQ value
detection of MXRA5 mRNA expression. Total RNA was extracted from
frozen tissues with the RNAiso Plus kit (Takara Bio Inc., Shiga,
Japan) according to the manufacturer’s instructions. Reverse
transcription of extracted RNA (500 ng) was performed using RNase
H-deficient reverse transcriptase (Superscript II; Life
Technologies, Carlsbad, CA, USA). The reverse transcription
reaction mixture (2 μl) was used for quantification of MXRA5 gene
expression by RT-PCR assay. Gene specific primers used in qRT-PCR
were as follows: MXRA5 forward primer, 5′-CAT TGC TAG ACA CGT GGA
AAG A-3′; reverse primer, 5′-TCT CAT TGC CGT GAA TCA TAA G-3′.
qRT-PCR was conducted in an Applied Biosystems 7500 Real-Time PCR
system (Applied Biosystems, Foster City, CA, USA) using SYBR Premix
Ex Taq™ kit (Takara) according to the manufacturer’s instructions.
The reaction was repeated three times and threshold cycle numbers
were averaged. The expression intensity of MXRA5 in CRC samples was
expressed as fold changes over the average of normal tissue
samples. GAPDH was amplified from the same RNA samples and served
as an internal control.
Statistical analysis
Statistical calculations were performed using SPSS
17.0 software (SPSS Inc., Chicago, IL, USA). Comparisons of data
between two groups were analyzed using a Student’s t-test and a
two-tailed P<0.05 was considered to indicate a statistically
significant difference.
Results
IHC staining
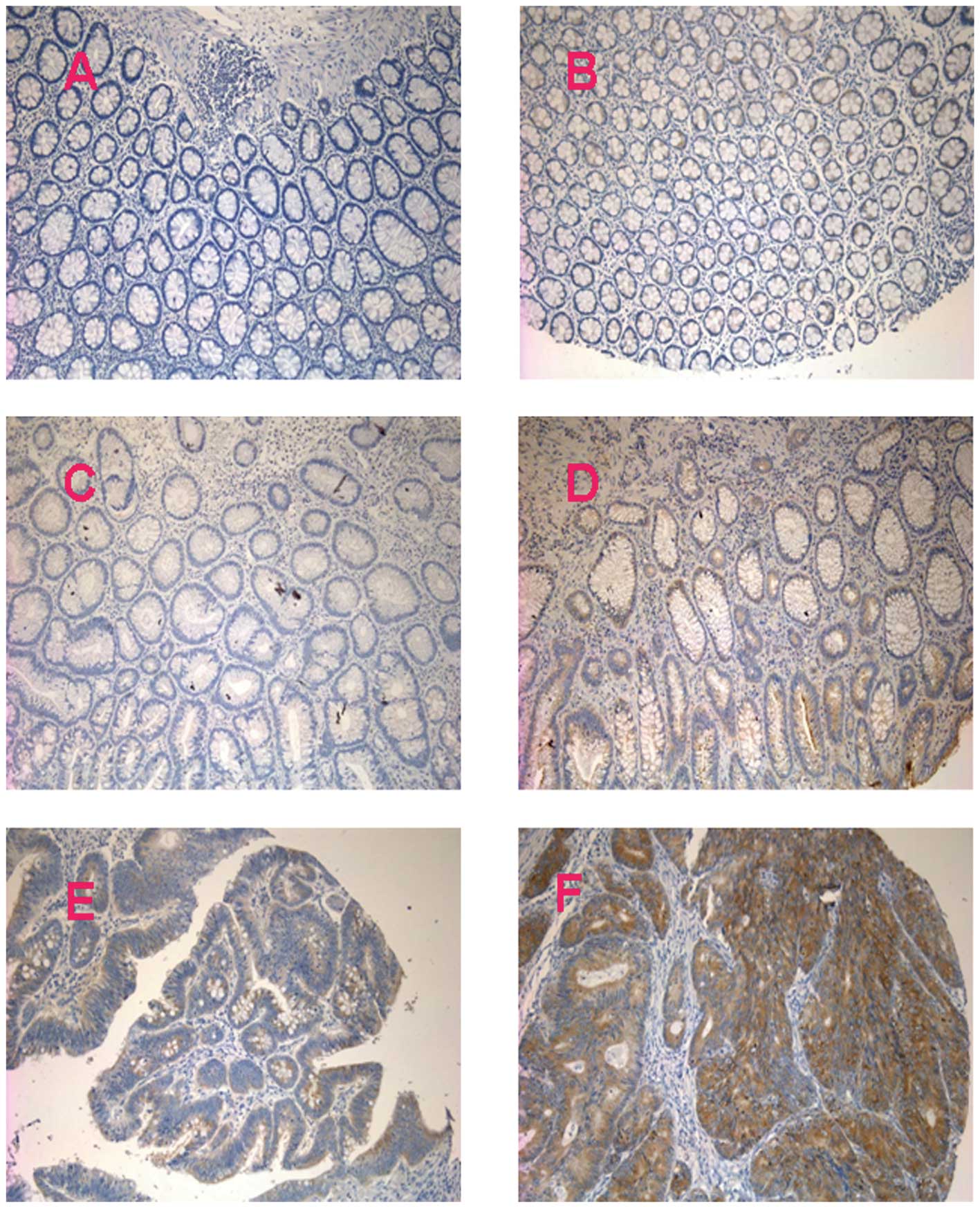
To investigate the oncogenic properties of MXRA5 in
CRC, paraffin-embedded tissues were stained aganinst MXRA5
antibody. As shown in Fig. 1,
staining for MXRA5 was mainly located in the cytoplasm of CRC
cells, suggesting that the CRC cells were responsible for the
overexpression of MXRA5.
As demonstrated in Table
I, of 156 normal tissues, 84% (131/156) were negative (IRS, 0),
while 16% (25/156) were weakly positive/positive (IRS, 1–4).
Percentages of tissues exhibiting an IRS of 2, 3 and 4 were 0.6%
(1/156), 6.4% (10/156) and 9% (14/156), respectively. In 20 adenoma
specimens, scores of 0, 2, 3, 4 and 6 were detected in 35% (7/20),
20% (4/20), 15% (3/20), 15% (3/20) and 15% (3/20), respectively,
while no strong staining (IRS, 9–12) was observed. Of the 156 CRC
specimens, IRS of 2, 3, 4, 6, 8, 9 and 12 were detected in 8.3%
(13/156), 10.9% (17/156), 13.5% (21/156), 30.8% (48/156), 16.0%
(25/156), 3.8% (6/156) and 16.7% (26/156), respectively. There was
a significant difference in MXRA5 expression in CRC tissues and
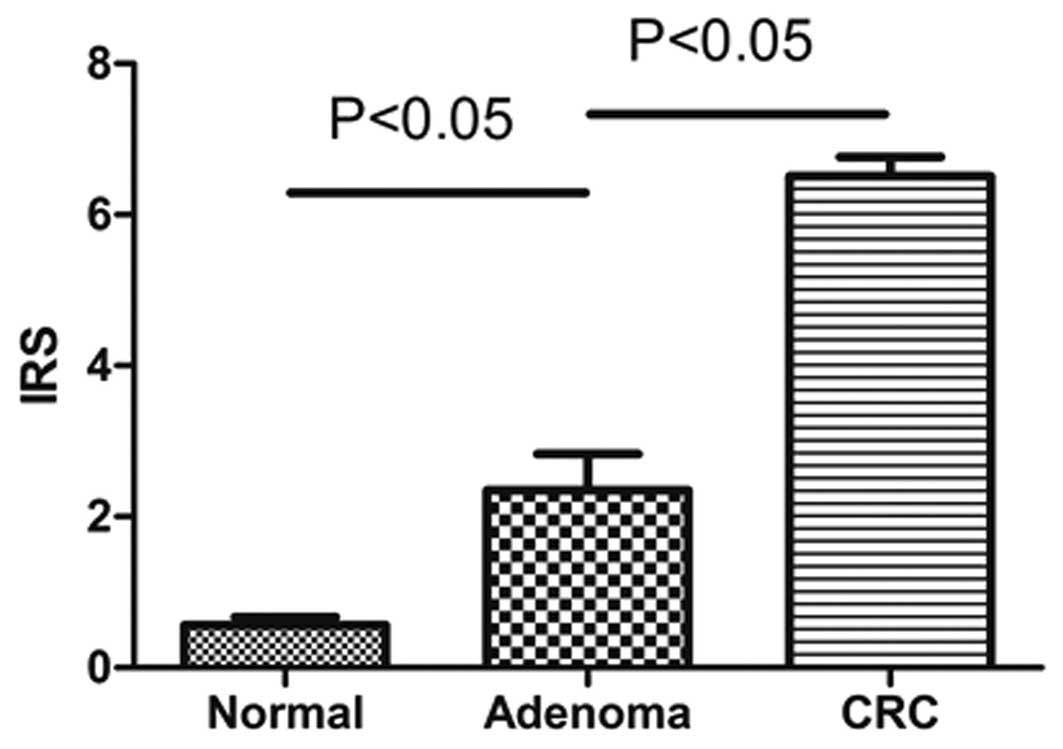
adenoma tissues compared with normal tissues. Furthermore, as
demonstrated in Fig. 2, the IRS of
normal, adenoma and CRC tissue specimens were 0.56±1.31, 2.25±2.159
and 6.55±3.072, respectively. The IRS gradually increased from
normal to adenoma to CRC tissue with significantly different
expression between the different groups.
Correlations with CRC
characteristics
The correlation between MXRA5 staining and
clinicopathological characteristics was investigated. As
demonstrated in Table II, MXRA5
protein expression was significantly correlated with certain
pathological features of CRC, including the lesion site of the
right colon, advanced stage (III and IV) and distant metastasis,
while no significant correlation was observed with gender, age,
gross pathology, tumor diameter, differentiation, invasion or lymph
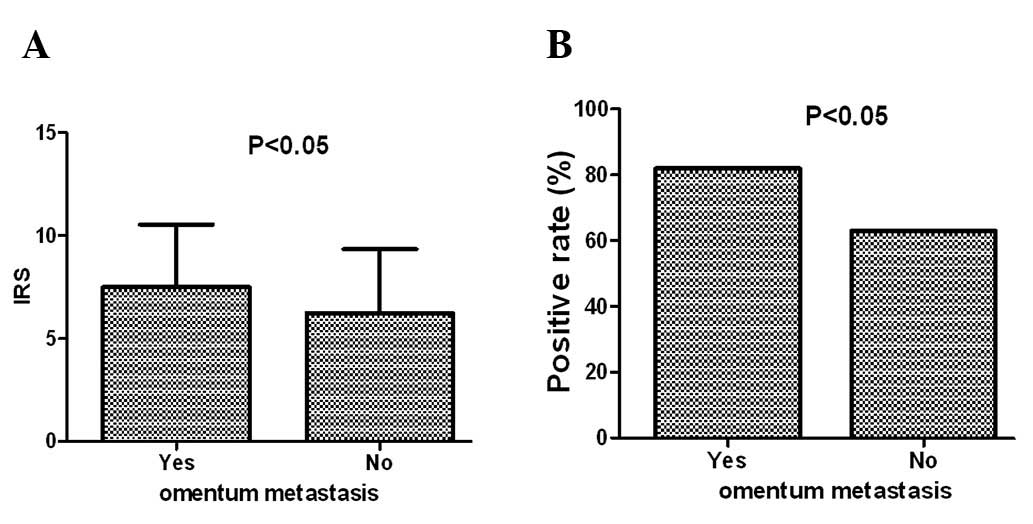
metastasis. Furthermore, as sites of distant metastasis included
the liver, pelvic cavity, omentum and other sites, the correlations
of MXRA5 protein expression with the different types of distant
metastasis were investigated in detail. As shown in Fig. 3, both the positive expression rate
and IRS of MXRA5 expression were significantly higher in the
omental metastasis group compared with the group without omental
metastasis. No significant change was observed in the liver, pelvic
cavity or any of the other sites of distant metastasis
investigated.
| Table II.Classification of MXRA5 protein
immunoreactivity in the CRC tissues, their corresponding normal
tissue and the adenoma tissues. |
Table II.
Classification of MXRA5 protein
immunoreactivity in the CRC tissues, their corresponding normal
tissue and the adenoma tissues.
| | IRS (%)
| P-value
|
|---|
| Group | N | 0 | 1–4 | 5–8 | 9–12 | All positive | vs. N | vs. Ad |
|---|
| N | 156 | 131 (84%) | 25 (16%) | 0 (0%) | 0 (0%) | 25 (16%) | | |
| A | 20 | 7 (35%) | 10 (50%) | 3 (15%) | 0 (0%) | 13 (65%) | <0.001 | |
| CRC | 156 | 0 (0%) | 51 (33%) | 73 (47%) | 32 (20%) | 156 (100%) | <0.001 | <0.001 |
qRT-PCR analysis
Additionally, the differential expression of the
MXRA5 gene in normal and CRC samples was detected by qRT-PCR
analysis at the mRNA level. However, no significant differences in
MXRA5 expression were found between tumor samples and
patient-matched normal tissues. Furthermore, no significant
correlation between the IRS of protein expression and its
corresponding RQ value of mRNA expression was observed (data not
shown).
Discussion
MXRA5, also known as Adlican, is a 312-kDa protein
and belongs to the MXRA gene family that participates in cell
adhesion and matrix remodeling. MXRA2 is an α-parvin, a cell-matrix
adhesion protein that co-localizes with actin filaments at membrane
ruffles and focal contacts in fibroblasts (14). MXRA4 is a C1q complement component
receptor. C1q has several functions, including stimulating
endothelial expression of cell adhesion molecules and promoting
cell attachment (15). MXRA5 is an
adhesion proteoglycan with VEGF receptor activity that shows
elevated expression in the cartilage of patients with
osteoarthritis, and is involved in adhesion and matrix remodeling
(16). Cell adhesion and matrix
remodeling play a key role in many disease processes, including
cancer, arthritis, angiogenesis, ulceration and fibrosis.
Therefore, we hypothesized that MXRA genes may play an important
role in tumor development.
Previous studies have revealed that the MXRA5 gene
was upregulated in individuals exposed to fractionated radiation,
by cDNA array (17,18). The gene has also been observed to be
overexpressed in skin fibroblasts from centenarians compared with
younger controls (19). Regarding
its role in tumorigenesis, Buckanovich et al(20) found that MXRA5 was overexpressed in
ovarian cancer compared with normal ovaries (by qRT-PCR) and it was
involved in tumor angiogenesis. The authors simultaneously
demonstrated that MXRA5 was absent in almost all normal colon
tissues, with few exceptions. This is consistent with our results.
The only study concerning MXRA5 in relation to CRC tumorigenesis
was a study by Zou et al(21), which demonstrated using qRT-PCR that
the MXRA5 gene was over-expressed in CRC tissues compared with
their corresponding normal tissue, and that the gene may be
involved in the development and progression of CRC (21). However, our data suggests that the
protein expression of MXRA5 was aberrantly high in CRC tissues
while the mRNA expression was not, which is inconsistent with the
study by Zou et al. The reasons for this are mainly due to
sample size; Zou et al only experimented with 13 CRC
tissues, compared with our 156 CRC tissues for protein expression
and 70 CRC tissues for mRNA expression.
Notably, MXRA5 protein expression was also detected
in human adenoma tissues in our study, and the protein expression
level of MXRA5 from normal colorectal to adenoma and then to
carcinoma tissue markedly increased, paralleling the increasing
severity of colorectal tissue injury. This result indicated that
the aberrant protein expression of MXRA5 was an early event in CRC
tumorigenesis.
Additionally, it was demonstrated that aberrant
protein expression of MXRA5 was significantly correlated with the
lesion site of CRC, advanced TNM stage and distant metastasis
(omental metastasis in particular). The omentum is an important
intraperitoneal structure with unique anatomic and pathologic
features, mainly comprising of fat, while the numerous other
components include blood vessels, lymphatics and cellular tissues
of the immune system (22).
Histologically, the omentum is composed of a double layer of
peritoneum that extends inferiorly from the greater curvature of
the stomach. Following extension for a distance that typically
ranges from 14–36 cm, the greater omentum turns superiorly on
itself to drape over the transverse colon and extend to the
retroperitoneal pancreas. Metastatic disease involving the omentum
is far more common than primary tumors. Although any tumor may
secondarily involve the omentum, the most frequent malignant
lesions that metastasize to the omentum include ovarian carcinoma
and tumors of the colon and pancreas. Metastases from the stomach,
appendix, kidney, uterus and biliary tract may also metastasize to
the omentum (22–26). Omental metastasis may be involved in
several pathways, including direct extension along the various
contiguous ligaments and hematogenous or peritoneal seeding
(22). Therefore, this explains our
result that aberrant protein expression of MXRA5 was significantly
correlated with the lesion site of colon and omental metastases. In
addition, omental metastasis was a significant, poor prognostic
factor for endometrioid adenocarcinoma, suggesting the need for
intra-operative examination of the omentum by close inspection and
palpation as well as pathologic examination (27). The significance of the correlation
between MXRA5 protein expression and greater omental metastases of
CRC requires further investigation.
In this study, our results indicate that MXRA5
protein expression is aberrantly detected in CRC tissues, and has
potential value as a biomarker for the early detection of CRC and
omental metastasis. However, the reasons for the inconsistency
between protein expression and mRNA expression require further
study.
References
|
1.
|
Siegel R, Ward E, Brawley O and Jemal A:
Cancer statistics, 2011: the impact of eliminating socioeconomic
and racial disparities on premature cancer deaths. CA Cancer J
Clin. 61:212–236. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Ross JS: Biomarker update for breast,
colorectal and non-small cell lung cancer. Drug News Perspect.
23:82–88. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Bast RC Jr, Ravdin P, Hayes DF, et al:
2000 update of recommendations for the use of tumor markers in
breast and colorectal cancer: clinical practice guidelines of the
American Society of Clinical Oncology. J Clin Oncol. 19:1865–1878.
2001.PubMed/NCBI
|
|
4.
|
Duffy M, Van Dalen A, Haglund C, et al:
Tumour markers in colorectal cancer: European Group on Tumour
Markers (EGTM) guidelines for clinical use. Eur J Cancer.
43:1348–1360. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Wang Q, Zhang YN, Lin GL, et al: S100P, a
potential novel prognostic marker in colorectal cancer. Oncol Rep.
28:303–310. 2012.
|
|
6.
|
Higashijima J, Kurita N, Miyatani T, et
al: Expression of histone deacetylase 1 and metastasis-associated
protein 1 as prognostic factors in colon cancer. Oncol Rep.
26:343–348. 2011.PubMed/NCBI
|
|
7.
|
Walther A, Johnstone E, Swanton C, Midgley
R, Tomlinson I and Kerr D: Genetic prognostic and predictive
markers in colorectal cancer. Nat Rev Cancer. 9:489–499. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Siena S, Sartore-Bianchi A, Di
Nicolantonio F, Balfour J and Bardelli A: Biomarkers predicting
clinical outcome of epidermal growth factor receptor-targeted
therapy in metastatic colorectal cancer. J Natl Cancer Inst.
101:1308–1324. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Helgason HH, Engwegen JY, Zapatka M, et
al: Identification of serum proteins as prognostic and predictive
markers of colorectal cancer using surface enhanced laser
desorption ionization-time of flight mass spectrometry. Oncol Rep.
24:57–64. 2010. View Article : Google Scholar
|
|
10.
|
Chung CH, Seeley EH, Roder H, et al:
Detection of tumor epidermal growth factor receptor pathway
dependence by serum mass spectrometry in cancer patients. Cancer
Epidemiol Biomarkers Prev. 19:358–365. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Sun W, Xing B, Sun Y, et al: Proteome
analysis of hepatocellular carcinoma by two-dimensional difference
gel electrophoresis: novel protein markers in hepatocellular
carcinoma tissues. Mol Cell Proteomics. 6:1798–1808. 2007.
View Article : Google Scholar
|
|
12.
|
Phizicky E, Bastiaens PI, Zhu H, Snyder M
and Fields S: Protein analysis on a proteomic scale. Nature.
422:208–215. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Yao L, Lao W, Zhang Y, et al:
Identification of EFEMP2 as a serum biomarker for the early
detection of colorectal cancer with lectin affinity capture
assisted secretome analysis of cultured fresh tissues. J Proteome
Res. Apr 30–2012.(Epub ahead of print).
|
|
14.
|
Olski TM, Noegel AA and Korenbaum E:
Parvin, a 42 kDa focal adhesion protein, related to the
alpha-actinin superfamily. J Cell Sci. 114:525–538. 2001.PubMed/NCBI
|
|
15.
|
Lozada C, Levin RI, Huie M, et al:
Identification of C1q as the heat-labile serum cofactor required
for immune complexes to stimulate endothelial expression of the
adhesion molecules E-selectin and intercellular and vascular cell
adhesion molecules 1. Proc Natl Acad Sci USA. 92:8378–8382. 1995.
View Article : Google Scholar
|
|
16.
|
Walker MG and Volkmuth W: Cell adhesion
and matrix remodeling genes identified by co-expression analysis.
Gene Function & Disease. 3:109–112. 2002.
|
|
17.
|
Alsner J, Rødningen OK and Overgaard J:
Differential gene expression before and after ionizing radiation of
subcutaneous fibroblasts identifies breast cancer patients
resistant to radiation-induced fibrosis. Radiother Oncol.
83:261–266. 2007. View Article : Google Scholar
|
|
18.
|
Rødningen OK, Børresen-Dale AL, Alsner J,
Hastie T and Overgaard J: Radiation-induced gene expression in
human subcutaneous fibroblasts is predictive of radiation-induced
fibrosis. Radiother Oncol. 86:314–320. 2008.PubMed/NCBI
|
|
19.
|
Chondrogianni N, de C M Simoes D,
Franceschi C and Gonos ES: Cloning of differentially expressed
genes in skin fibroblasts from centenarians. Biogerontology.
5:401–409. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Buckanovich RJ, Sasaroli D,
O’Brien-Jenkins A, et al: Tumor vascular proteins as biomarkers in
ovarian cancer. J Clin Oncol. 25:852–861. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Zou TT, Selaru FM, Xu Y, et al:
Application of cDNA microarrays to generate a molecular taxonomy
capable of distinguishing between colon cancer and normal colon.
Oncogene. 21:4855–4862. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Sompayrac SW, Mindelzun RE, Silverman PM
and Sze R: The greater omentum. AJR Am J Roentgenol. 168:683–687.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Kehinde E, Abdeen S, Al-Hunayan A and Ali
Y: Prostate cancer metastatic to the omentum. Scand J Urol Nephrol.
36:225–227. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Chou CK, Liu GC, Su JH, Chen LT, Sheu RS
and Jaw TS: MRI demonstration of peritoneal implants. Abdom
Imaging. 19:95–101. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Levitt RG, Koehler RE, Sagel SS and Lee
JK: Metastatic disease of the mesentery and omentum. Radiol Clin
North Am. 20:501–510. 1982.PubMed/NCBI
|
|
26.
|
Silverman P and Cooper C: Mesenteric and
omental lesions. Textbook of Gastrointestinal Radiology. 1st
edition. WB Saunders; Philadelphia, PA: 1994
|
|
27.
|
Fujiwara H, Saga Y, Takahashi K, et al:
Omental metastases in clinical stage I endometrioid adenocarcinoma.
Int J Gynecol Cancer. 18:165–167. 2008. View Article : Google Scholar : PubMed/NCBI
|