Introduction
Globally, colorectal cancer (CRC) is the third most
commonly diagnosed cancer in males and the second in females
(1). A number of studies have
demonstrated the critical involvement of cyclooxygenase (COX) in
the development and progression of CRC (2,3). COX
is a rate-limiting enzyme in the synthesis of bioactive
prostaglandins or thromboxanes from arachidonic acid (AA), which is
mainly released from membrane-bound glycerophospholipids.
Phospholipase A2 (PLA2) is a key esterase that cleaves the
glycerophospholipids at the sn-2 ester bond to release a fatty acid
and lysophospholipid (4).
Therefore, the tissue expression of PLA2 is thought to have
important roles in the development of CRC.
PLA2 proteins are broadly defined into three
different classes: secretory PLA2 (sPLA2), cytosolic PLA2 (cPLA2)
and Ca2+-independent PLA2 (iPLA2). Approximately
one-third of the PLA2s belong to the sPLA2 family, which contains
typically disulfide-rich, low molecular weight enzymes with strict
Ca2+ dependence and a His-Asp catalytic dyad (5). To date, 11 sPLA2s (IB, IIA, IIC, IID,
IIE, IIF, III, V, X, XIIA and XIIB) have been identified in
mammals. After being secreted to the extracellular space, sPLA2s
act on cellular membrane-bound phospholipids in an autocrine or
paracrine manner, leading to the production of various inflammatory
mediators, including prostaglandins, leukotrienes and thromboxane.
The other cleavage products, namely lysophospholipids, such as
lysophosphatidylcholine (LPC) and lysophosphatidic acid (LPA), also
have various bioactivities. Moreover, sPLA2s also act on
non-cellular phospholipids, including those in microvesicles,
pulmonary surfactant, lipoproteins, microbial membranes and food
substances (4).
The physiological functions of the different sPLA2s
have been gradually elucidated. They have been implicated in lipid
digestion and obesity, activation of immune cells, asthma,
atherosclerosis, acute respiratory distress syndrome and host
defense against bacteria, viruses and parasites (5–8).
However, differences in pathophysiological roles as well as the
expression profile of each enzyme remain largely unknown. Of the
sPLA2 family, sPLA2 group X (PLA2GX) has the most powerful
AA-releasing activity from cell membrane-bound phospholipids,
leading to eicosanoid formation (9,10).
Morioka et al have shown that PLA2GX also releases AA from
cultured human colon carcinoma cell lines, leading to
COX-2-dependent PGE2 formation (11). The authors also showed enhanced
expression of PLA2GX in adenocarcinoma cells in comparison with the
normal colonic epithelia, by immunohistochemistry. PLA2GX has also
been shown to stimulate the proliferation of colon cancer cells
(12). From these data, the
positive role of PLA2GX on colorectal carcinogenesis is speculated.
In fact, previous studies have also described the expression of
PLA2GX in human colon cancer tissue at the mRNA (13) and protein (14) levels. However, the precise
expression and distribution patterns of PLA2GX in colonic cancer
tissues remain to be characterized. In the present study, we aimed
to examine the expression of PLA2GX in human CRC tissue and its
possible correlation with clinical and pathological variables as
well as with patient outcome.
Patients and methods
Patients and samples
A total of 158 consecutive patients with colorectal
adenocarcinoma who underwent curative resection with lymph node
dissection at the University of Tokyo Hospital (Tokyo, Japan), in
the period between January 1991 and March 1994, were enrolled.
There were 96 males and 62 females (mean age, 62 years; range,
38–90 years). Cases of ulcerative colitis and familial adenomatous
polyposis were excluded from this study. None of the patients had
received preoperative chemotherapy or radiation therapy. All
pertinent clinical and histopathological data of the patients and
their tumors were collected from the patients’ case records.
Clinicopathological features were analyzed based on the TNM
classification of malignant tumors of the Union for International
Cancer Control (UICC; 7th edition). All patients had been
subsequently followed up at regular clinical visits until mortality
or when last seen alive, for a mean observation period of 108
months. Informed consent was obtained from all patients and the
study was approved by the Ethics Committee of the Hospital of the
University of Tokyo, Tokyo, Japan.
The surgically resected specimens were immediately
fixed in 10% buffered formalin and the cross-sections of the entire
cancerous lesion were embedded in paraffin. Conventional
pathological diagnosis of the primary lesion and the dissected
lymph nodes was performed on hematoxylin and eosin
(H&E)-stained sections. PLA2GX expression in the cancerous
lesion was examined by immunohistochemical staining, as described
below.
Immunohistochemical study
Rabbit anti-sPLA2GX polyclonal antibody was
generated by the immunization of rabbit with a polypeptide at The
Tokyo Metropolitan Institute of Medical Science (Tokyo, Japan). The
specificity and immunoreactivity of the antibody was verified by
immunoblotting with sPLA2-transfected cells (15). Consecutive formalin-fixed
paraffin-embedded sections (4 μm thick) were immunohistochemically
stained by the streptavidin-biotin (SAB) immunoperoxidase method.
For immunohistochemical staining, the sections were deparaffinized
with xylene and dehydrated with 98% ethanol, placed in 0.01 M
sodium citrate buffer (pH 6.0) and heated in an autoclave oven for
15 min. After washing twice in PBS, endogenous peroxidase activity
was inhibited by incubation with 0.3% hydrogen peroxide in methanol
for 20 min. After three washes in PBS, non-specific reactions were
blocked by incubation with 10% goat serum for 30 min at room
temperature. Biotinylated goat anti-rabbit immunoglobulin and SAB
complex, supplied commercially [Histfine SAB-PO(R) kit, Nichirei,
Tokyo, Japan] were used as the reagents in the subsequent steps.
The sections were incubated with the anti-PLA2GX antibody overnight
at 4°C. The color was then developed with diaminobenzidine
solution. The sections were then lightly counterstained with a
cocktail of Mayer’s/Lillie-Mayer’s hematoxylin and mounted.
Spermatozoa were used as a positive control (16). For the negative control, the
antibody was replaced with PBS.
Evaluation of immunostaining
The expression of PLA2GX in the cancerous lesion and
in the surrounding normal mucosa was assessed by two observers
(S.K. and M.H.) without knowledge of the corresponding clinical
data. All tissue samples were assessed in a consecutive analysis to
ensure maximal internal consistency. For the objective assessment
of the PLA2GX expression level, it was stratified into three
groups, as follows: −, not detected; +, focally positive in cancer
cells; ++, diffusely positive in carcinoma cells. The consistency
between the observers was 80.1% (κ test), and in the discrepant
cases, a consensus was reached after a joint review. In the
statistical analysis, − and + were considered to be the low
expression group, and ++ was considered to be the high expression
group.
Statistical analysis
The statistical significance of the differences was
evaluated by χ2 test, Fisher’s exact test or a
non-paired Student’s t-test, as appropriate. The disease-specific
survival (DSS) rate was analyzed by the Kaplan-Meier method and the
log-rank comparison test. To assess the value of PLA2GX as an
independent predictor, a multivariate survival analysis was
performed, using the Cox proportional hazards regression model. All
statistical analyses were performed with JMP 9.0 (SAS Institute,
Cary, NJ, USA). P<0.05 was considered to indicate a
statistically significant result.
Results
PLA2GX expression in human CRC
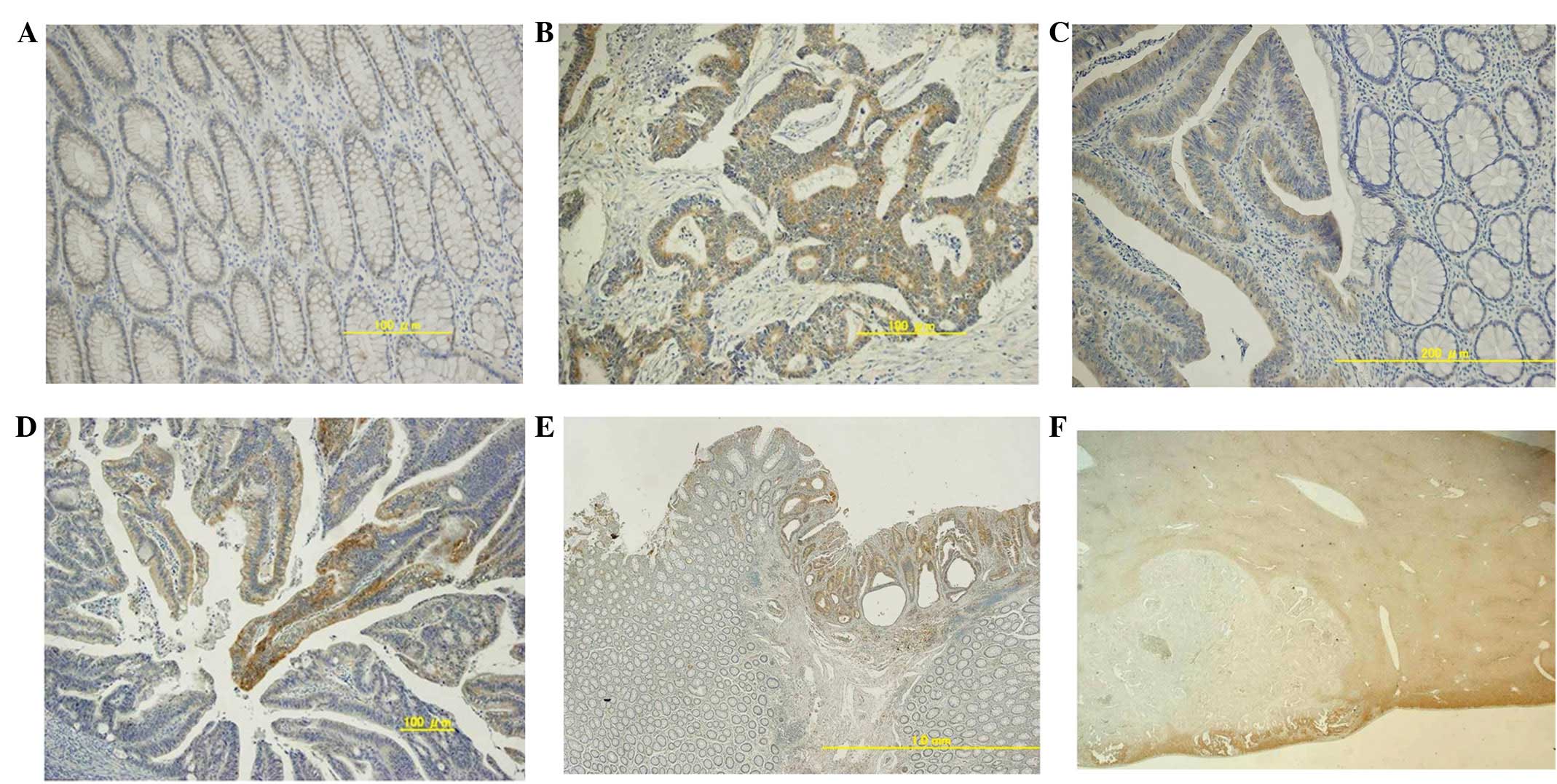
The staining patterns of PLA2GX in CRC specimens are
shown in Fig. 1. In the normal
colonic mucosa adjacent to the CRC, most of the colonic epithelial
cells showed a weak expression of PLA2GX (Fig. 1A), although there was a variation of
immunoreactivity among the cases. In the majority of the 158
tumors, PLA2GX expression was found predominantly in the cytoplasm
of carcinoma cells and, compared with the normal epithelium, the
staining signal was generally enhanced (Fig. 1B). The stromal tissue was not
stained in any analyzed specimen. In 101 cases, PLA2GX expression
was diffusely and almost equally detected in most of the cancer
cells, as shown in Fig. 1B, whereas
in 54 cases, the expression was observed only in focal cancer cells
(Fig. 1D). In 3 cases, however,
negligible staining of cancer cells was found. In addition, PLA2GX
was hardly detected in the hepatic metastatic lesions, although the
expression was diffuse in the primary lesion. (Fig. 1E and F). For further analyses, the
tumors were divided into high expression (101 cases) and low
expression (57 cases) groups.
Correlation between PLA2GX expression and
clinicopathological features
Descriptive characteristics of the study subjects
are presented in Table I. The
expression of PLA2GX showed no correlation with age, gender, tumor
size, tumor location, histological appearance, lymphatic invasion
or venous involvement. However, the rate of hematogenous metastasis
was significantly higher in the low PLA2GX expression group (10.5%)
than in the high PLA2GX expression group (1.0%; P= 0.005).
Similarly, there was a tendency for higher incidence of lymph node
metastasis in the low PLA2GX expression group (50.9%) than in the
high expression group (36.6%; P=0.081) (Table II). When the study sample was
restricted to left-sided tumors (112 cases), nodal metastasis was
observed in 52.4% (22/42) of the low PLA2GX expression group, which
was significantly higher than that in the high expression group
(30.0%; 21/70; P= 0.018). By contrast, when samples were restricted
to right-sided tumors, no difference in the incidence of nodal
metastasis was observed. Additionally, only border-line
significance (P=0.051) was observed in the association between the
PLA2GX expression and the UICC stage.
 | Table I.Association of PLA2GX expression with
clinical variables. |
Table I.
Association of PLA2GX expression with
clinical variables.
| | PLA2GX
| |
|---|
| Factor | n | High expression
(n=101) | Low expression
(n=57) | P-value |
|---|
| Age (years), mean ±
SD | 158 | 62.4±11.1 | 63.6±10.3 | 0.481 |
| Gender, n (%) | | | | |
| Male | 96 | 41 (40.6) | 21 (36.8) | 0.642 |
| Female | 62 | 60 (59.4) | 36 (63.2) | |
| Size of tumor (mm),
mean ± SD | 158 | 46.5±24.1 | 47.3±17.7 | 0.824 |
| T stagea, n (%) | | | | |
| T1/T2 | 36 | 27 (26.7) | 9 (15.8) | 0.108 |
| T3/T4 | 122 | 74 (73.3) | 48 (84.2) | |
| Histological type,
n (%) | | | | |
| Well, mod
differentiated | 152 | 96 (95.0) | 56 (98.2) | 0.285 |
| Muc, por
differentiated | 6 | 5 (5.0) | 1 (1.8) | |
| Lymphatic invasion,
n (%) | | | | |
| Absent | 118 | 76 (75.2) | 42 (73.7) | 0.829 |
| Present | 40 | 25 (24.8) | 15 (26.3) | |
| Lymph node
metastasis, n (%) | | | | |
| Absent | 92 | 64 (63.4) | 28 (49.1) | 0.081 |
| Present | 66 | 37 (36.6) | 29 (50.9) | |
| Venous involvement,
n (%) | | | | |
| Absent | 75 | 50 (49.5) | 25 (43.9) | 0.495 |
| Present | 83 | 51 (50.5) | 32 (56.1) | |
| Location of the
tumor, n (%) | | | | |
| Colon | 117 | 78 (77.2) | 39 (68.4) | 0.229 |
| Rectum | 41 | 23 (22.8) | 18 (31.6) | |
| Right side | 46 | 31 (30.7) | 15 (26.3) | 0.559 |
| Left side | 112 | 70 (69.3) | 42 (73.7) | |
| UICC stage, n
(%) | | | | |
| I/II | 91 | 64 (63.4) | 27 (47.4) | 0.051 |
| III/IV | 67 | 37 (36.6) | 30 (52.6) | |
| Hematogenous
metastasis, n (%) | | | | |
| Absent | 151 | 100 (99.0) | 51 (89.5) | 0.005 |
| Present | 7 | 1 (1.0) | 6 (10.5) | |
| Table II.Association of PLA2GX expression in
the left side of the colon with clinical variables. |
Table II.
Association of PLA2GX expression in
the left side of the colon with clinical variables.
| | PLA2GX, n (%)
| |
|---|
| Factor | n | High expression
(n=70) | Low expression
(n=42) | P-value |
|---|
| Lymphatic
invasion | | | | |
| Absent | 85 | 54 (77.1) | 31 (73.8) | 0.691 |
| Present | 27 | 16 (22.9) | 11 (26.2) | |
| Lymph node
metastasis | | | | |
| Absent | 69 | 49 (70.0) | 20 (47.6) | 0.018 |
| Present | 43 | 21 (30.0) | 22 (52.4) | |
| Venous
involvement | | | | |
| Absent | 54 | 35 (50.0) | 19 (45.2) | 0.625 |
| Present | 58 | 35 (50.0) | 23 (54.8) | |
| Hematogenous
metastasis | | | | |
| Absent | 105 | 69 (98.6) | 36 (85.7) | 0.017 |
| Present | 7 | 1 (1.4) | 6 (14.3) | |
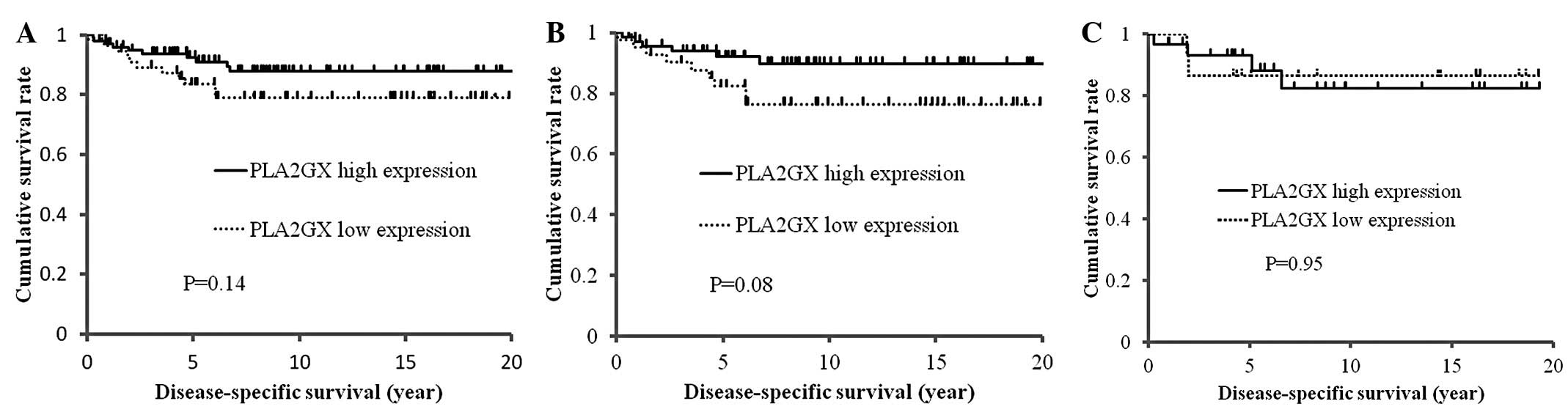
Overall survival and DSS analysis of CRC
with regard to PLA2GX expression
Next, we examined the correlation between PLA2GX
expression and the outcome of patients, by the Kaplan-Meier
analysis and the log-rank test. As shown in Fig. 2A, the high PLA2GX expression group
tended to have a longer DSS, although the difference did not reach
statistical significance (P=0.14). This trend was pronounced in
left-sided CRC (P=0.08) and was observed in right-sided CRC
(Fig. 2B).
Discussion
Due to their functional diversity, PLA2 enzymes have
been implicated in various biological processes, including
arthritis, asthma, defense against microbes, digestion,
atherosclerosis and cancer (17).
PLA2GX is known as the most potent sPLA2 capable of hydrolyzing
phosphatidylcholine and acting extra-cellularly on cellular
membranes and noncellular phospholipid substrates (5,9–11). It
has been confirmed that PLA2GX, as well as other sPLA2s, including
GIIA, GIII and GXIIA, are highly expressed in CRC tissue (13,14,18).
However, no information is available concerning the correlation
between PLA2GX expression in cancer and clinicopathological
features. Thus, in the present study, we aimed to investigate the
expression of PLA2GX in patients with CRC at various stages.
In our series, the majority of the carcinoma cells
in primary CRC showed enhanced cytoplasmic expression of PLA2GX as
compared with normal colonic epithelia, which is consistent with
previous results (11,13,14).
However, in 64% of the 158 cases, PLA2GX expression was diffusely
detected, while in certain cases PLA2GX was only partially
expressed and in a few cases, its expression was negative. In these
cases, a significant inverse correlation was found between PLA2GX
expression and hematogenous metastasis and, although without
significance, also with nodal metastasis. As a consequence,
patients with tumors with high PLA2GX expression had a better
outcome than those with low expression. To the best of our
knowledge, this is the first study to show the inverse correlation
of the expression of PLA2GX with the outcome of CRC patients, and
the possibility that this enzyme has suppressive effects on tumor
metastasis in CRC is suggested.
Increased expression of sPLA2 has been demonstrated
in numerous types of cancer, including breast (19,20),
pancreatic (21), prostate
(22,23), liver (24), gastric (25,26)
and colorectal (14,27) cancer. Of these, group IIA PLA2
(PLA2GIIA) is one of the isoforms most commonly investigated in
cancer tissue. Kashiwagi et al reported that the high
expression of PLA2GIIA was correlated with longer survival in
pancreatic cancer (28). More
recently, Xing et al have shown the same tendency in gastric
cancer, and suggested that PLA2GIIA may negatively affect the
meta-static potential of gastric cancer cells (26). In fact, Ganesan et al have
demonstrated that the silencing of the PLA2GIIA gene enhances the
invasive activity of tumor cells, whereas enforced expression
inhibited invasion (29). These
results are consistent with our finding on PLA2GX, suggesting a
possibility that PLA2GX, as well as PLA2GIIA, may play negative
roles in the metastatic potential of gastrointestinal cancer.
However, Buhmeida et al have shown a negative association of
the expression of PLA2GIIA with the prognosis of stage II CRC
(27). Also, Graff et al
have shown that PLA2GIIA expression increases with the progression
of prostate cancer in an androgen-independent manner (30). These controversial results suggest
that the role of PLA2GIIA is dependent on the interaction of cancer
cells with the microenvironment in different tissues.
Surrel et al have reported that, in
vitro, the addition of PLA2GX stimulates the proliferative
ability of colon cancer cells by producing various lipid mediators
(12). However, in their study, the
proliferation of the cells was examined in serum-free media, and
the effect was not completely abrogated by COX and lipooxygenase
inhibitors, suggesting the involvement of other lipid mediators.
The released AA itself induces the apoptosis of diverse cells,
including human colon cancer cells, via an intracellular
ceramide-mediated pathway (31).
Ceramide acts as a second messenger in the activation process of
the cellular apoptotic machinery (31). Diets rich in unsatu-rated fatty
acids such as AA are associated with a decreased incidence of colon
cancer (32). On the bases of these
facts, the negative effect of PLA2GX may be attributed to the
increased levels of AA produced and the subsequent increased
susceptibility to apoptosis.
Although there is no significant difference between
PLA2GX expression and the tumor location, the rate of lymph node
metastasis was found to be significantly lower and the DSS better
in left-sided CRC than in right-sided. This finding suggests the
possibility that CRCs developing in the two different colonic sites
may have different biological behaviors. It is known that right-
and left-sided colonic tumors have different molecular profiles,
with microsatellite instability and methylator phenotypes being
prevalent in right-sided tumors and chromosomal instability being
predominant in left-sided tumors, resulting in different biological
features (33,34). It is possible that these molecular
profiles are intimately associated with the different lymphatic
metastatic potentials. Indeed, the PLA2GX gene expression level was
reported to be significantly higher in the normal mucosa of the
left side of the colon than in that of the right side (13).
In conclusion, our study showed an inverse
association between the reduced expression of PLA2GX and the
increased metastatic potential of human CRC, especially in the
left-sided tumors. Our data suggest that PLA2GX may have a
protective role against the invasive ability of CRC, and the
reduced ability to produce PLA2GX may result in the acquisition of
a clinically more malignant phenotype. Thus, PLA2GX expression may
be a potential clinical biomarker for the prediction of the
invasive ability of human CRC. To date, several inhibitors of PLA2s
have been developed as anticancer drugs (35). However, since PLA2s, in certain
situations, may also have a suppressive effect on tumor
progression, they may be two-edged swords, and thus their
indication should be carefully considered.
References
|
1.
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar
|
|
2.
|
Williams CS, Tsujii M, Reese J, Dey SK and
DuBois RN: Host cyclooxygenase-2 modulates carcinoma growth. J Clin
Invest. 105:1589–1594. 2000. View
Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Rodrigues S, Bruyneel E, Rodrigue CM,
Shahin E and Gespach C: Cyclooxygenase 2 and carcinogenesis. Bull
Cancer. 91(Suppl 2): S61–S76. 2004.(In French).
|
|
4.
|
Murakami M, Taketomi Y, Sato H and
Yamamoto K: Secreted phospholipase A2 revisited. J Biochem.
150:233–255. 2011. View Article : Google Scholar
|
|
5.
|
Lambeau G and Gelb MH: Biochemistry and
physiology of mammalian secreted phospholipases A2. Annu Rev
Biochem. 77:495–520. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Touqui L and Wu YZ: Interaction of
secreted phospholipase A2 and pulmonary surfactant and its
pathophysiological relevance in acute respiratory distress
syndrome. Acta Pharmacol Sin. 24:1292–1296. 2003.PubMed/NCBI
|
|
7.
|
Triggiani M, Granata F, Frattini A and
Marone G: Activation of human inflammatory cells by secreted
phospholipases A2. Biochim Biophys Acta. 1761:1289–1300. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Nevalainen TJ, Graham GG and Scott KF:
Antibacterial actions of secreted phospholipases A2. Review.
Biochim Biophys Acta. 1781:1–9. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Hanasaki K, Ono T, Saiga A, et al:
Purified group X secretory phospholipase A(2) induced prominent
release of arachidonic acid from human myeloid leukemia cells. J
Biol Chem. 274:34203–34211. 1999. View Article : Google Scholar
|
|
10.
|
Murakami M, Kambe T, Shimbara S, et al:
Different functional aspects of the group II subfamily (Types IIA
and V) and type X secretory phospholipase A(2)s in regulating
arachidonic acid release and prostaglandin generation. Implications
of cyclooxygenase-2 induction and phospholipid scramblase-mediated
cellular membrane perturbation. J Biol Chem. 274:31435–31444.
1999.
|
|
11.
|
Morioka Y, Ikeda M, Saiga A, et al:
Potential role of group X secretory phospholipase A(2) in
cyclooxygenase-2-dependent PGE(2) formation during colon
tumorigenesis. FEBS Lett. 487:262–266. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Surrel F, Jemel I, Boilard E, et al: Group
X phospholipase A2 stimulates the proliferation of colon cancer
cells by producing various lipid mediators. Mol Pharmacol.
76:778–790. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Mounier CM, Wendum D, Greenspan E, Fléjou
JF, Rosenberg DW and Lambeau G: Distinct expression pattern of the
full set of secreted phospholipases A2 in human colorectal
adenocarcinomas: sPLA2-III as a biomarker candidate. Br J Cancer.
98:587–595. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Tribler L, Jensen LT, Jørgensen K, et al:
Increased expression and activity of group IIA and X secretory
phospholipase A2 in peritumoral versus central colon carcinoma
tissue. Anticancer Res. 27:3179–3185. 2007.PubMed/NCBI
|
|
15.
|
Degousee N, Ghomashchi F, Stefanski E, et
al: Groups IV, V, and X phospholipases A2s in human neutrophils:
role in eicosanoid production and gram-negative bacterial
phospholipid hydrolysis. J Biol Chem. 277:5061–5073. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Masuda S, Murakami M, Matsumoto S, et al:
Localization of various secretory phospholipase A2 enzymes in male
reproductive organs. Biochim Biophys Acta. 1686:61–76. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Murakami M, Taketomi Y, Miki Y, Sato H,
Hirabayashi T and Yamamoto K: Recent progress in phospholipase
A2 research: from cells to animals to humans. Prog Lipid
Res. 50:152–192. 2011.
|
|
18.
|
Murakami M, Masuda S, Shimbara S, Ishikawa
Y, Ishii T and Kudo I: Cellular distribution, post-translational
modification, and tumorigenic potential of human group III secreted
phospholipase A(2). J Biol Chem. 280:24987–24998. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Yamashita S, Yamashita J, Sakamoto K, et
al: Increased expression of membrane-associated phospholipase A2
shows malignant potential of human breast cancer cells. Cancer.
71:3058–3064. 1993. View Article : Google Scholar
|
|
20.
|
Yamashita S, Yamashita J and Ogawa M:
Overexpression of group II phospholipase A2 in human breast cancer
tissues is closely associated with their malignant potency. Br J
Cancer. 69:1166–1170. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Kiyohara H, Egami H, Kako H, et al:
Immunohistochemical localization of group II phospholipase A2 in
human pancreatic carcinomas. Int J Pancreatol. 13:49–57.
1993.PubMed/NCBI
|
|
22.
|
Jiang J, Neubauer BL, Graff JR, et al:
Expression of group IIA secretory phospholipase A2 is elevated in
prostatic intraepithelial neoplasia and adenocarcinoma. Am J
Pathol. 160:667–671. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Dong Q, Patel M, Scott KF, Graham GG,
Russell PJ and Sved P: Oncogenic action of phospholipase A2 in
prostate cancer. Cancer Lett. 240:9–16. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Ying Z, Tojo H, Komatsubara T, et al:
Enhanced expression of group II phospholipase A2 in human
hepatocellular carcinoma. Biochim Biophys Acta. 1226:201–205. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Leung SY, Chen X, Chu KM, et al:
Phospholipase A2 group IIA expression in gastric adenocarcinoma is
associated with prolonged survival and less frequent metastasis.
Proc Natl Acad Sci USA. 99:16203–16208. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Xing XF, Li H, Zhong XY, et al:
Phospholipase A2 group IIA expression correlates with prolonged
survival in gastric cancer. Histopathology. 59:198–206.
2011.PubMed/NCBI
|
|
27.
|
Buhmeida A, Bendardaf R, Hilska M, et al:
PLA2 (group IIA phospholipase A2) as a prognostic determinant in
stage II colorectal carcinoma. Ann Oncol. 20:1230–1235. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Kashiwagi M, Friess H, Uhl W, et al: Group
II and IV phospholipase A(2) are produced in human pancreatic
cancer cells and influence prognosis. Gut. 45:605–612. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Ganesan K, Ivanova T, Wu Y, et al:
Inhibition of gastric cancer invasion and metastasis by PLA2G2A, a
novel beta-catenin/TCF target gene. Cancer Res. 68:4277–4286. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Graff JR, Konicek BW, Deddens JA, et al:
Expression of group IIa secretory phospholipase A2 increases with
prostate tumor grade. Clin Cancer Res. 7:3857–3861. 2001.PubMed/NCBI
|
|
31.
|
Chan TA, Morin PJ, Vogelstein B and
Kinzler KW: Mechanisms underlying nonsteroidal antiinflammatory
drug-mediated apoptosis. Proc Natl Acad Sci USA. 95:681–686. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
32.
|
Reddy BS: Chemoprevention of colon cancer
by dietary fatty acids. Cancer Metastasis Rev. 13:285–302. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Bendardaf R, Lamlum H, Ristämaki R,
Korkeila E, Syrjänen K and Pyrhönen S: Mismatch repair status is a
predictive factor of tumour response to 5-fluorouracil and
irinotecan chemotherapy in patients with advanced colorectal
cancer. Tumour Biol. 28:212–220. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Bendardaf R, Lamlum H, Ristamäki R,
Korkeila E, Syrjänen K and Pyrhönen S: Thymidylate synthase and
microsatellite instability in colorectal cancer: implications for
disease free survival, treatment response and survival with
metastases. Acta Oncol. 47:1046–1053. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Cummings BS: Phospholipase A2 as targets
for anti-cancer drugs. Biochem Pharmacol. 74:949–959. 2007.
View Article : Google Scholar : PubMed/NCBI
|