Introduction
Carcinosarcoma, also termed sarcomatoid carcinoma,
pseudosarcoma or spindle cell carcinoma, is an unusual biphasic
malignant neoplasm consisting of both carcinomatous and sarcomatous
components. It is mainly characterized by a large, bulky and
polypoid mass. Carcinosarcoma usually occurs in such diverse
locations as the uterus, breast, thyroid, lung and upper
gastrointestinal system. In this study, we describe a rare case of
multiple carcinosarcomas (MCS) that occurred in the esophagus and
stomach. To the best of our knowledge, this is the first report of
MCS arising from both these regions. The study was approved by the
Ethics Committee of Changhai Hospital, Shanghai, China. The patient
provided written informed consent and accepted the therapy.
Case report
In April 2010, an 84-year-old male presented with
recurrent epigastric pain for 9 months and melena for 5 months. The
initial admission (4 months ago) revealed that the patient had
severe anemia [hemoglobin, 5.5 g/dl; mean capuscular volume (MCV),
82.1 fl) with marked pallor. The patient had a long history of
smoking exceeding 50 pack years (1000 cigarette years). The first
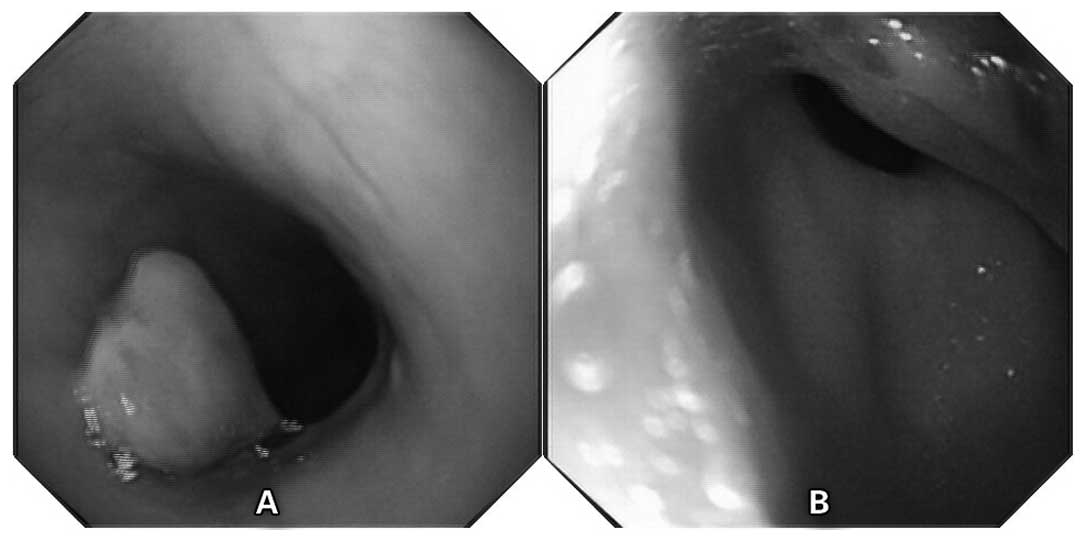
esophagogastroduodenoscopy (EGD) revealed a pedunculated polypoid
lesion in the esophagus and an elevated huge mass in the lesser
curvature (Fig. 1). Both biopsies
of the esophageal and gastric lesions revealed poorly
differentiated squamous cell carcinoma, and the patient was
negative for Helicobacter pylori. Without surgical
indications, the patient received 4 cycles of chemotherapy using
folinic acid, fluorouracil and oxaliplatin (FOLFOX). One week ago,
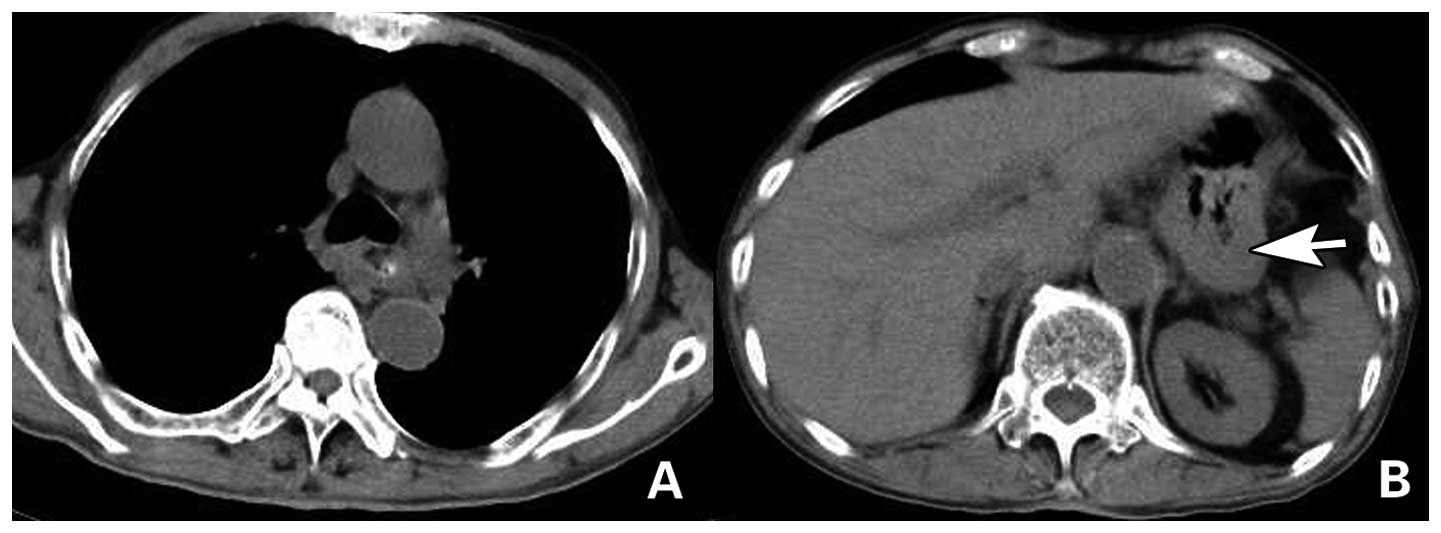
the patient was re-admitted due to dysphagia. A computed tomography
(CT) examination demonstrated a heterogenous tumorous formation
obturating the esophageal lumen without enlarged lymph nodes in the
thoracic region, while nodular thickening of the gastric antral
wall and narrowing of the gastric cavity in the upper abdomen were
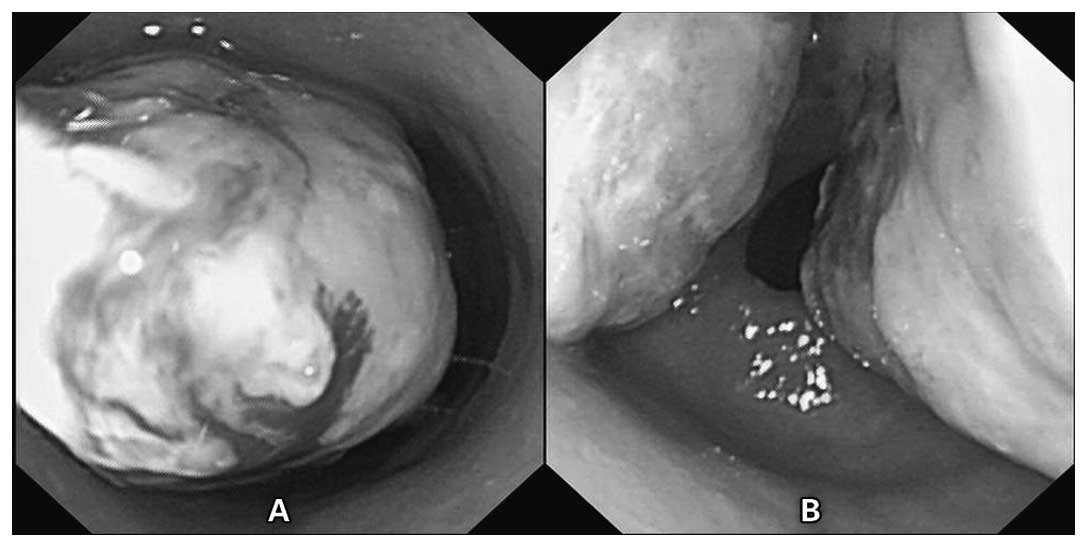
observed (Fig. 2). Compared with
the first EGD, the second revealed that the two lesions in the
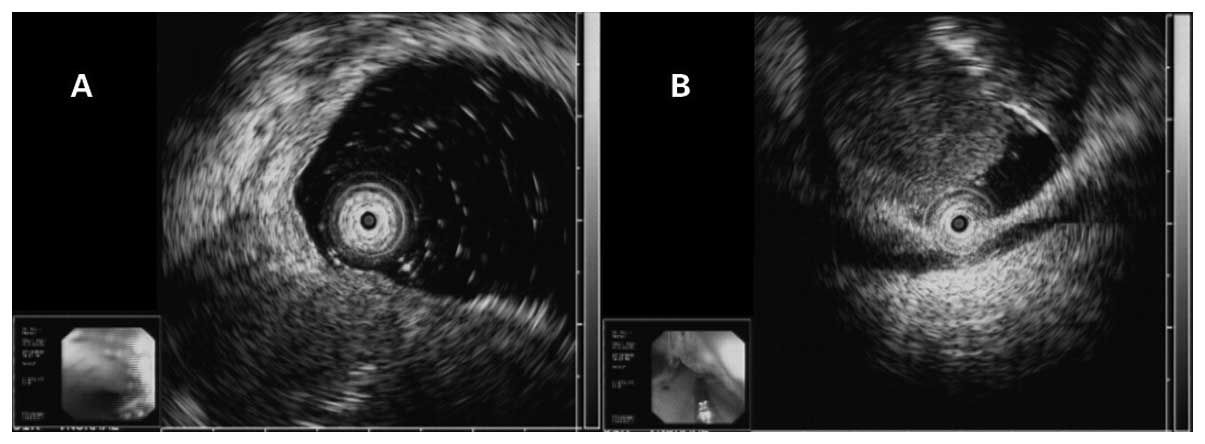
esophagus and stomach had evidently increased in size (Fig. 3). Endoscopic ultrasound (EUS)
independently demonstrated a hypoechoic mass both in the esophagus
and the gastric corpus (Fig. 4). To
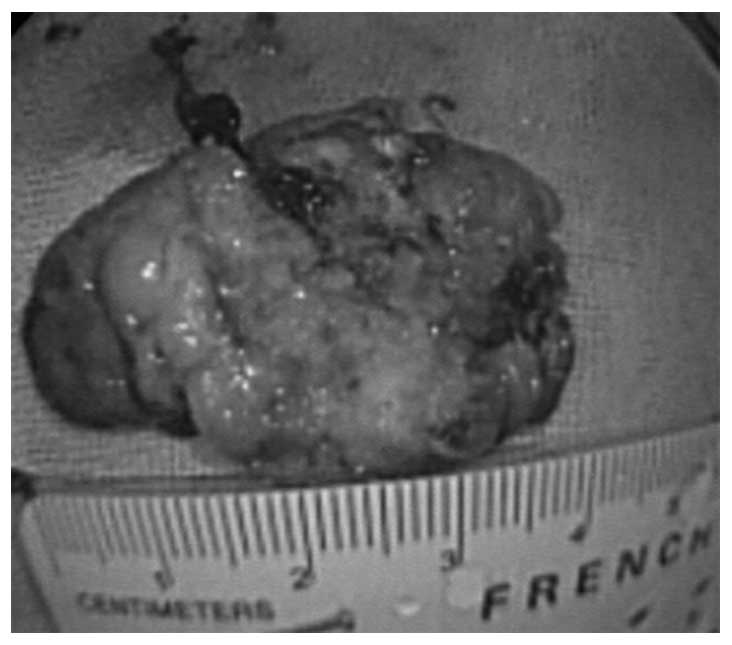
relieve the symptom of regurgitation, we performed a palliative
esophageal endoscopic polypoid tumor resection (specimen size,
4×2.5×1.5 cm; Fig. 5) without
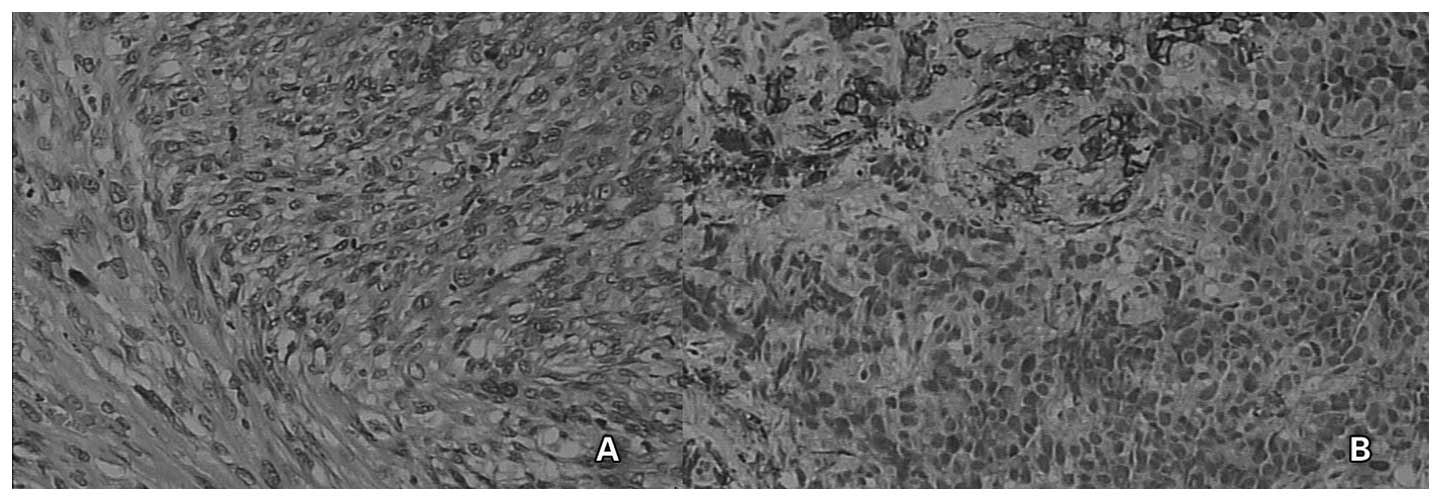
bleeding and perforation. Microscopically, the resected tumor
consisted of polymorphic spindle cells mixed with a number of
squamous cells, while the gastric biopsies revealed carcinomatous
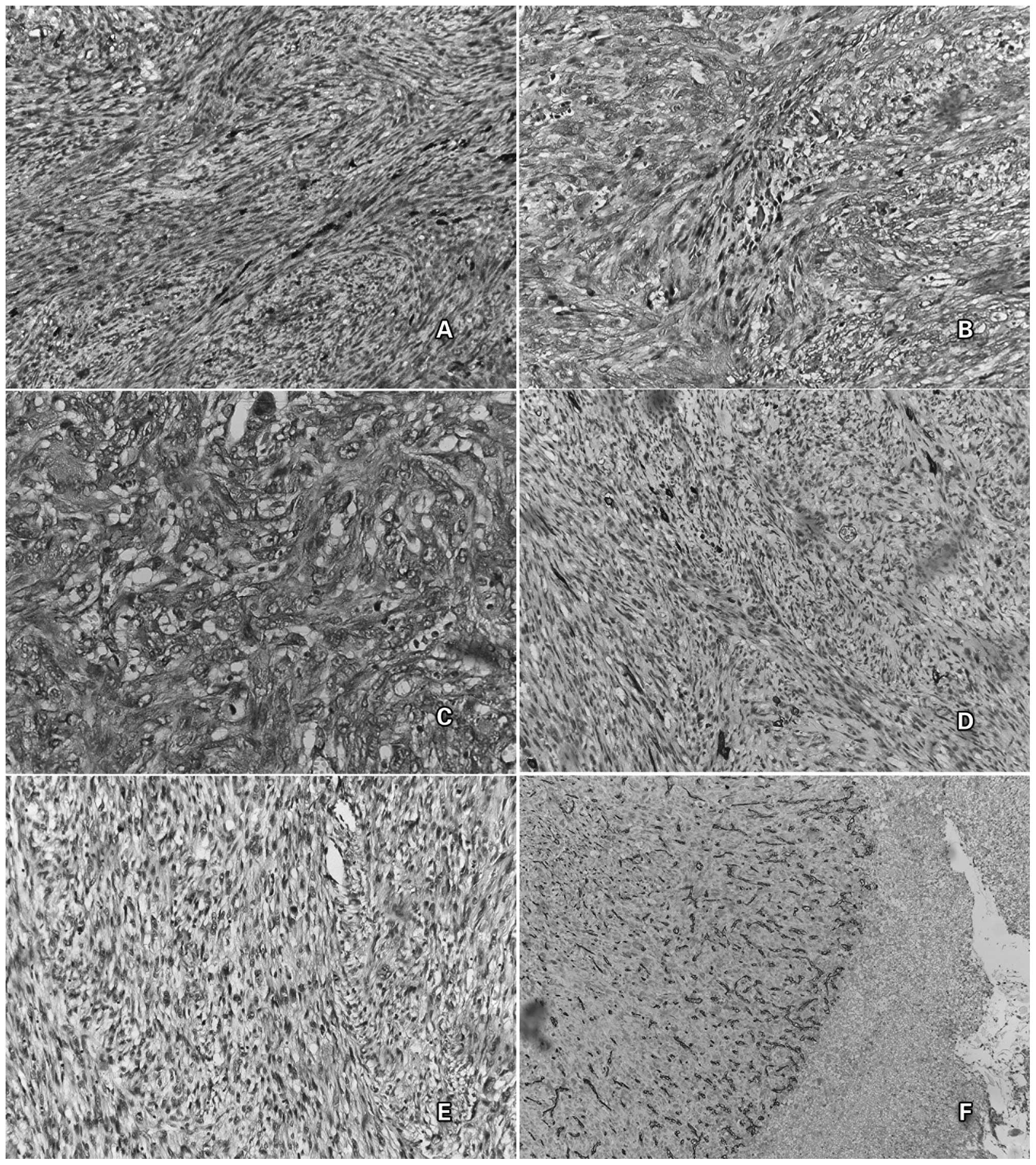
cells with polymorphous spindle cells (Fig. 6). Immunohistochemically, the
resected tumor stained positively for epithelial markers of
epithelial membrane antigen (EMA) and cytokeratin 19 (CK 19), and
mesenchymal markers of smooth muscle actin (SMA) and vimentin
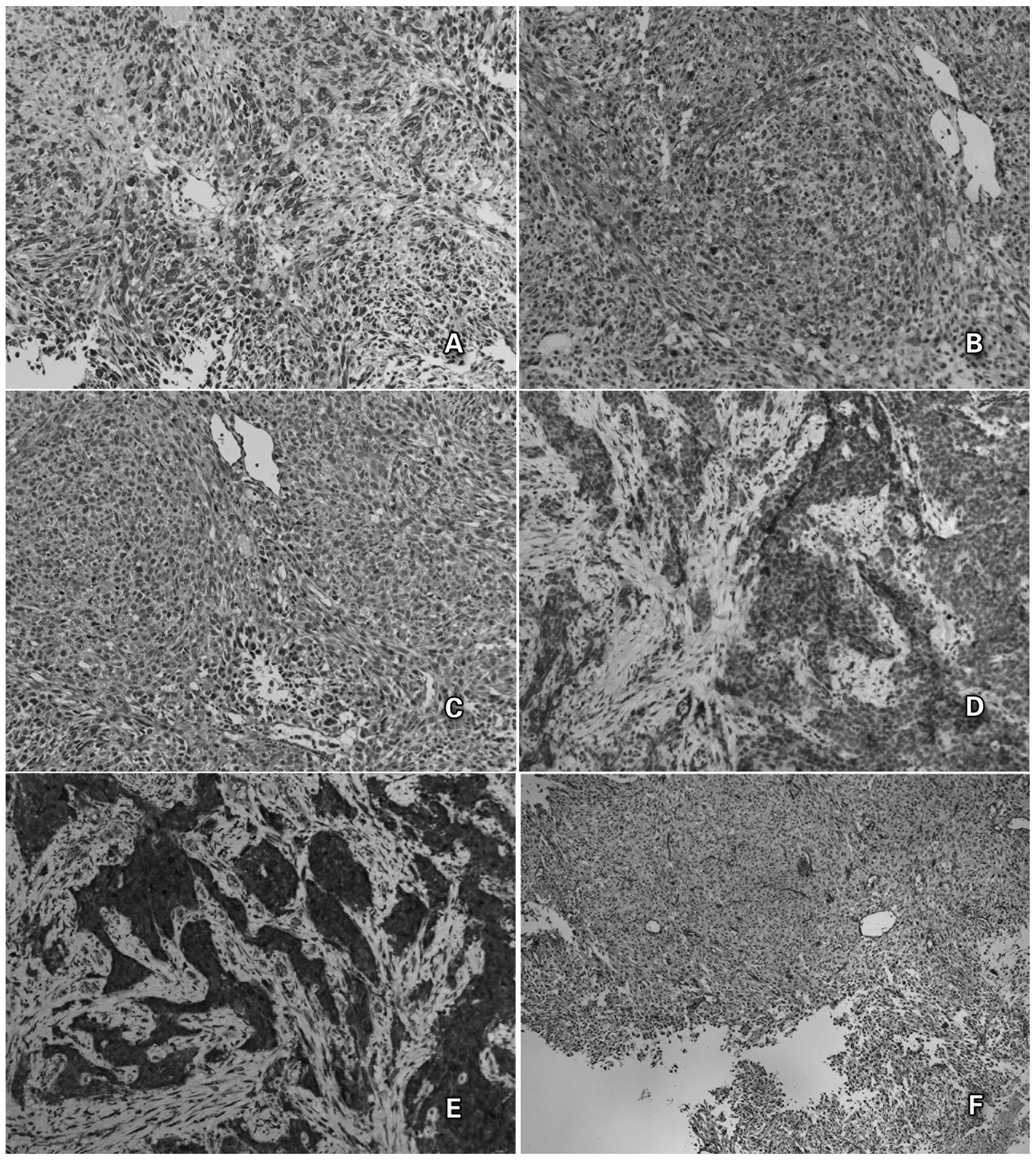
(Fig. 7). In the gastric lesion,
staining was positive for CK AE1/AE3, actin and vimentin, but
negative for EMA (Fig. 8). The
aforementioned findings confirmed the diagnosis of multiple
carcinosarcomas. Notably, both lesions stained positively for
neuron specific enolase (NSE), demonstrating neuroendocrine
differentiation (Fig. 7E and
Fig. 8E), and positively for CD 34
in the vascular endothelial cells (Fig.
7F and Fig. 8F). The patient
was discharged from hospital with normal food intake, and succumbed
7 months later.
Discussion
In 1865, Virchow named the rare malignant neoplasm
consisting of carcinomatous and sarcomatous components as
‘carcinosarcoma’ (1). Since then,
it has also been referred to as sarcomatoid carcinoma,
pseudosarcoma or spindle cell carcinoma. In 1992, Ro et al
proposed the histological criteria of carcinosarcoma (2): (i) the concurrent presence of
malignant epithelial and spindle cell components, between which
there are transitional areas, and (ii) the sarcomatoid component
expresses an epithelial phenotype. In this study, no transitional
area was observed between the sarcomatous and carcinomatous
components, but irregular intermingling was identified.
Carcinosarcoma most commonly occurs in middle-aged and elderly men
with a history of smoking or drinking. In the present case, the
patient had a long history of smoking. Carcinosarcoma has been
found in such diverse locations as the uterus, breast, thyroid,
lung and upper gastrointestinal system (3). It is most frequently observed in the
esophagus, while localization in the stomach has been less
frequently identified (4,5). More than 80% of carcinosarcomas are
located in the middle and/or lower esophagus. Macroscopically, the
majority of carcinosarcomas are of the polypoid type and others are
of the ulcerative type (6,7). Gastric carcinosarcoma typically
presents with an elevated lesion or increased thickness of the
gastric wall (8,9), and rarely presents with an ulcerated
lesion (10). In the current case,
a bulky pedunculated polypoid lesion in the middle of the esophagus
and a huge discoid lesion in the lesser curvature with increased
thickness of the gastric wall were observed. MCS of the esophagus
and stomach has not been previously reported.
Immunocytochemistry is the gold standard for the
diagnosis of carcinosarcoma, as upper gastrointestinal series
(barium swallow), CT and even endoscopy are observed to be less
efficient and accurate. It has been demonstrated that CEA, EMA,
pancreatin, chromogranin A, CD56 and synaptophysin staining are
highly specific markers for the carcinomatous components, while
desmin, vimentin and smooth muscle/sarcomeric actin show affinity
for the sarcomatous elements (11,12).
In the present case, the immunohistochemical staining findings in
both the esophageal and gastric lesions were consistent with the
diagnosis of carcinosarcoma.
The histological origin of carcinosarcoma is
debated, and two main hypotheses have been proposed. The first
hypothesis is a stem cell theory of origin, with tumor stem cells
differentiating toward epithelial neoplasm and mesenchymal
metaplasia (13). The second
hypothesis is a tumor collision theory, with neoplasm derived from
the collision of two distinct neoplasms that are epithelial and
mesenchymal in origin (14,15). Molecular analysis has revealed that
the two components of carcinosarcoma have different genetic
mutations, mainly involving the P53, cyclin D1, P16, MDM2 and CDK4
genes (16–21). P53 gene mutations exist in both the
sarcomatous and carcinomatous components, but the type of mutation
differs (16). Cyclin D1 gene
amplification is frequently amplified in carcinosarcoma,
particularly in the sarcomatous component (17). It has been demonstrated in the
esophagus that the two components exhibited cyclin D1 gene
amplification and p16 homozygous deletion, by differential
polymerase chain reaction and fluorescence in situ
hybridization (19). Certain
studies have demonstrated that MDM2 and CDK4 were strongly
implicated in the pathogenesis of carcinoma and sarcoma (14,20,21).
CDK4 overexpression was observed in laryngeal squamous cell
carcinoma, which was significantly correlated with tumor size and
an advanced stage (21). Nikitakis
et al(14) compared the
expression of MDM2 and CDK4 in two cases of esophageal
carcinosarcoma, and selected cases of esophageal squamous cell
carcinoma with a prominent stromal reaction. The results supported
the common epithelial origin of carcinosarcoma.
We assumed that carcinosarcoma is a type of
malignant disease that is different from cancer or sarcoma, with
its own unique pathological features. The diversity, complexity and
mixed type of the two components reveal the possibility of
origination from the same original proto-stem cells of
carcinosarcomas. Under certain carcinogens, these proto-stem cells
may commence pathological differentiation in different ways and
present the traits of mutagenized malignant cells. In this case,
the patient exhibited MCS of the esophagus and stomach. We suggest
that it is possible that the tumor originated from the same
original proto-stem cells. Further genetic analyses of the lesions
of the two locations may assist in determining the cell source of
carcinosarcoma.
With respect to the treatment of upper
gastrointestinal carcinosarcoma, there is no recommended clinical
management at present. The treatment modalities for esophageal
carcinosarcoma include esophagectomy, endoscopic resection and
chemo-radiotherapy (22,23). Esophagectomy has been traditionally
considered as the first option for esophageal carcinosarcoma
(24), but endoscopic therapy may
represent an alternative to surgery for superficial carcinosarcoma.
In gastric carcinosarcoma, the main therapy conducted is radical
and comprises partial or total gastrectomy (10,25).
At present, surgery is regarded to be the only curative treatment
for gastric carcinosarcoma. Endoscopic polypectomy is a novel
alternative to surgery for patients with polypoid carcinosarcoma
confined to the mucosal layer with no involvement of the lymph
nodes. Pesenti et al(23)
conducted the first EMR for esophageal carcinosarcoma with good
tolerance and a favorable prognosis. In the present case, with two
lesions in both the esophagus and stomach, the patient was unable
to tolerate radical esophagectomy or gastrectomy at the same time
due to his poor condition. To improve the symptoms of esophageal
obstruction and guarantee normal eating, esophageal EMR (palliative
surgery) was performed and a series of treatments, including acid
suppression, anti-inflammatory and hemostasis, followed. The
patient demonstrated a good postoperative recovery without bleeding
or perforation; however, the patient succumbed after seven months.
We propose that if the patient had received laparoscopic gastric
partial gastrectomy at the same time, he may have had a longer
survival time and an improved prognosis. However, for age reasons,
the patient refused to undergo further laparoscopic surgery.
In conclusion, carcinosarcoma is a rare tumor with
limited clinical recognition and an extremely high rate of mis
diagnosis. There are no reports regarding the occurrence of MCS in
both the esophagus and stomach. Therefore, due to the polypoid
non-invasive lesions in the esophagus, and the discoid non-invasive
mass with an off-white surface in the stomach, extensive samples
should be obtained for immunohistochemistry or genetic analysis to
achieve a definite diagnosis. Immunocytochemistry has been the gold
standard for the diagnosis of carcinosarcoma. Chemotherapy for
carcinosarcoma was demonstrated to be ineffective. Compared with
traditional surgery, therapeutic endoscopy has been proven to be
less invasive; notably, it enables the esophagus to be preserved.
Therefore, therapeutic endoscopy may provide an alternative method
of treating carcinosarcoma, particularly MCS.
Abbreviations:
|
CDK4
|
cyclin-dependent kinase 4
|
|
CK
|
cytokeratin
|
|
CT
|
computed tomography
|
|
EGD
|
esophagogastroduodenoscopy
|
|
EMA
|
epithelial membrane antigen
|
|
EMR
|
endoscopic mucosal resection
|
|
MCS
|
multiple carcinosarcomas
|
|
MDM2
|
murine double minute
|
|
NSE
|
neuron specific enolase
|
|
P53
|
protein 53
|
|
SMA
|
smooth muscle actin
|
References
|
1
|
Virchow RLK: Vorlesungen uber Pathologie
die krankhaften Geschwulste. A Hirschwald, Berlin. 1865.(In
German).
|
|
2
|
Ro JY, Chen JL, Lee JS, et al: Sarcomatoid
carcinoma of the lung: Immunohistochemaical and ultrastructural
studies of 14 cases. Cancer. 69:376–386. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Robey-Cafferty SS, Gringon DJ, Ro JY, et
al: Sarcomatoid carcinoma of the stomach: A report of three cases
with immunohistochemical and ultrastructural observations. Cancer.
65:1601–1606. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kanamoto A, Nakanishi Y, Ochiai A, et al:
A case of small polypoid esophageal carcinoma with multidirectional
differentiation, including neuroendocrine, squamous, ciliated
glandular, and sarcomatous components. Arch Pathol Lab Med.
124:1685–1687. 2000.
|
|
5
|
Yamazaki K: A gastric carcinosarcoma with
neuroendocrine cell differentiation and undifferentiated
spindle-shaped sarcoma component possibly progressing from the
conventional tubular adenocarcinoma; an immunohistochemical and
ultrastructural study. Virchows Arch. 442:77–81. 2003.
|
|
6
|
Iyomasa S, Kato H, Tachimori Y, et al:
Carcinosarcoma of the esophagus: a twenty-case study. Jpn J Clin
Oncol. 20:99–106. 1990.PubMed/NCBI
|
|
7
|
Kuo CJ, Lin TN, Lin CJ, et al: Clinical
manifestation of esophageal carcinosarcoma: a Taiwan experience.
Dis Esophagus. 23:122–127. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ashida K, Wamata T, Sugesawa A, et al: A
case of so-called carcinosarcoma of the stomach. J Jpn Surg Assoc.
59:702–706. 1998. View Article : Google Scholar
|
|
9
|
Tanimura H and Furuta M: Carcinosarcoma of
the stomach. Am J Surg. 113:702–709. 1967. View Article : Google Scholar
|
|
10
|
Kikuyama R, Tanaka K, Tano S, et al: A
case of gastric carcinosarcoma. Endoscopy. 41:E220–221. 2009.
View Article : Google Scholar
|
|
11
|
Teramachi K, Kanomata N, Hasebe T, et al:
Carcinosarcoma (pure endocrine cell carcinoma with sarcoma
components) of the stomach. Pathol Int. 53:552–556. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sato Y, Shimozono T, Kawano S, et al:
Gastric carcinosarcoma, coexistence of adenosquamous carcinoma and
rhabdomyosarcoma: a case report. Histopathology. 39:543–544. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ota S, Kato A, Kobayashi H, et al:
Monoclonal origin of an esophageal carcinosarcoma producing
granulocyte-colony stimulating factor: a case report. Cancer.
82:2102–2111. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nikitakis NG, Drachenberg CB and
Papadimitriou JC: MDM2 and CDK4 expression in carcinosarcoma of the
esophagus: comparison with squamous cell carcinoma and review of
the literature. Exp Mol Pathol. 73:198–208. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Meyer R: Current findings for the
interpretation of ‘tight junctions’ as lipid structures. Acta
Histochem Suppl. 30:291–296. 1984.
|
|
16
|
Nakagawa S, Nishimaki T, Suzuki T, et al:
Histogenetic heterogeneity in carcinosarcoma of the esophagus:
report of a case with immunohistochemical and molecular analyses.
Dig Dis Sci. 44:905–909. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Suzuki H, Moriya J, Nakahata A, et al:
Cyclin D1 gene amplification in esophageal carcinosarcoma shown by
differential polymerase chain reaction. Hum Pathol. 29:662–667.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Iwaya T, Maesawa C, Tamura G, et al:
Esophageal carcinosarcoma: a genetic analysis. Gastroenterology.
113:973–977. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Suzuki H, Fujioka Y and Nagashima K:
Cyclin D1 gene amplification and p16 gene deletion in patients with
esophageal carcinosarcoma. Diagn Mol Pathol. 7:253–259. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Momand J, Jung D, Wilczynski S, et al: The
MDM2 gene amplification database. Nucleic Acids Res. 26:3453–3459.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dong Y, Sui L, Sugimoto K, et al: Cyclin
D1-CDK4 Complex: a possible critical factor for cell proliferation
and prognosis in laryngeal squamous cell carcinomas. Int J Cancer.
95:209–215. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hung JJ, Li AF, Liu JS, Lin YS and Hsu WH:
Esophageal carcinosarcoma with basaloid squamous cell carcinoma and
osteosarcoma. Ann Thorac Surg. 85:1102–1104. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pesenti C, Bories E, Danisi C, et al:
Endoscopic treatment of esophageal carcinosarcoma: report of a
case. Endoscopy. 36:952004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ziauddin MF, Rodriguez HE, Quiros ED,
Connolly MM and Podbielski FJ: Carcinosarcoma of the
esophagus-pattern of recurrence. Dig Surg. 18:216–218. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ikeda Y, Kosugi S, Nishikura K, et al:
Gastric carcinosarcoma presenting as a huge epigastric mass.
Gastric Cancer. 10:63–68. 2007. View Article : Google Scholar : PubMed/NCBI
|