Introduction
Osteosarcoma (OS) is the most common malignant bone
tumor in adolescents and young adults. The use of neoadjuvant
chemotherapy and improvements in surgical technology have increased
the survival rate to 65–75% (1).
However, pulmonary metastasis occurs in approximately 40% of
patients and remains the major cause of mortality. With intensive
pre-operative chemotherapy, high rates of histological necrosis
(≥90%), and a strong prognostic factor predicting a favorable
outcome, have been reported in only 20–60% of patients (2,3),
making it necessary to identify new markers or gene sets that would
predict tumor response to chemotherapy, and allow more individually
adapted multimodality treatments.
Several candidate markers for chemosensitivity and
prognosis have been identified. Hypoxia-inducible factor 1 α
(HIF-1α) has been demonstrated to correlate with an unfavorable
prognosis in a number of types of cancer, and is known to be
significant in chemoresistance (4–6).
Findings of recent studies have shown a significant association
between the expression of HIF-1α and prognosis in OS (7,8),
inhibition of HIF-1α gene expression by siRNA decreased tumor
formation rate and growth speed in xenograft mice (9). Results of previous studies on human OS
cells demonstrated that hypoxia-induced overexpression of HIF-1α
was associated with the upregulation of the vascular endothelial
growth factor (VEGF) and tumor angiogenesis (10). VEGF is not only a key factor in the
angiogenesis pathway, but also a target for several therapeutics
approved by the U.S. Food and Drug Administration (11). Apurinic endonuclease 1 (APE1) has
been discussed as a potential drug target in various cancer types,
as its expression has been linked to chemosensitivity and prognosis
(12,13). In OS, a previous study indicated
that APE1 expression was an independent predictor of OS local
recurrence and/or metastasis (13).
The respect in which HIF-1α and APE1 are coexpressed in OS and the
impact of their coexpression on the tumor necrosis rate requires
further investigation. The expression of cycloogenase-2 (COX-2) is
known to be markedly correlated with clinical stage and prognosis
in patients with OS (14).
Inhibition of COX-2 is capable of inducing massive tumor necrosis
in xenograft mice (15). A previous
study revealed a correlation between COX-2 and VEGF in breast
ductal carcinoma (16). As with
APE1 and HIF-1α, the correlation has not been sufficiently examined
in OS.
In this study, we investigated the prognostic values
of HIF-1α, APE1, VEGF and COX-2 protein expression as well as their
interrelationships in OS. We further analyzed the correlation of
these proteins with clinical and histopathological variables,
including tumor size, primary American Joint Committee on Cancer
(AJCC) stage (17), metastasis,
survival, and particularly tumor necrosis rate following
neoadjuvant chemotherapy.
Materials and methods
Patients and treatment protocols
A total of 49 consecutive cases (28 males and 21
females; median age, 18.5 years; age range, 11–72 years) with
non-metastatic primary OS were selected for the study. The patients
were treated in the Department of Bone and Soft Tissue Tumors at
the Tianjin Medical University Cancer Institute and Hospital
between 2000 and 2009. All the patients underwent incisional biopsy
for diagnosis prior to neoadjuvant chemotherapy and we used the
remaining tissue for immunohistochemistry. The neoadjuvant
chemotherapy agents used were in accordance with those proposed and
proven previously, including methotrexate (MTX), adriamycin (ADM),
cisplatin (CDDP) and ifosfamide (IFO) (18). In brief, patients were administered
10 g/m2 of MTX in week 1 and 12 g/m2 of IFO
in week 2, followed by 80 mg/m2 of CDDP and 60
mg/m2 of combined ADM in week 3. Following two weeks of
rest, lesions were reassessed using computed tomography or magnetic
resonance imaging studies. The pre- and post-chemotherapy imaging
data were reviewed by radiologists who were blind to the clinical
data, and reassessed by surgical oncologists for resectability and
change in scope.
Further treatments were performed according to the
reassessments. Patients expected to have a safe margin and
acceptable function outcome were assigned to surgery and
post-operative adjuvant chemotherapy. Patients with irresectable
diseases or those expected to have an unacceptable function
impairment were assigned to amputation when the disease progressed.
Patients with a tumor response to neoadjuvant chemotherapy, but no
decrease in scope of surgery were treated with second cycle
neoadjuvant chemotherapy followed by surgical resection. Tumor size
data were available based on a review of the pre-treatment imaging
studies and the pathology reports. We assessed chemotherapy
efficacy histologically using the Huvos grading system
post-operatively (19). According
to the percentage of dead cells, the 49 cases were divided into two
groups; tumors demonstrating a good response to pre-operative
chemotherapy (dead cells ≥90%, surviving cells ≤10%) and tumors
demonstrating a poor response (surviving cells >10%).
Post-operative chemotherapy was prescribed according to the tumor
necrosis rate. Patients with a good response were treated with the
same dosage of therapeutic agents as administered pre-operatively.
Patients with a poor response were treated with intensified doses
(MTX, 12 g/m2; IFO, 15g/m2; CDDP, 100
mg/m2 and ADM, 80 mg/m2). The mean follow-up
time was 29 months (range, 6–100). Disease-free survival (DFS) was
defined from the day of surgery until the first relapse of the
disease or mortality. Mortality from a cause other than OS, or
survival until the end of the observation period, was considered a
censoring event.
This study was approved by Fudan University Cancer
Center and Shanghai Medical College, as well as Tianjin Medical
University Cancer Institute and Hospital and Tianjin Key Laboratory
of Cancer Prevention and Treatment. Patient consent was obtained
prior to obtaining specimens and reviewing patient information.
Immunohistochemistry
Formalin-fixed, paraffin-embedded tissues obtained
in the biopsy procedures were cut consecutively into 3-μm sections.
The histological slides were deparaffinized in xylol. The slides
were heated in 0.01 M citrate buffer for 10 min in a microwave
oven. Following 20 min of cooling and washing in PBS, endogenous
peroxidase was blocked with methanol containing 0.3% hydrogen
peroxide for 30 min, followed by incubation with PBS for 30 min.
For the immunohistochemical detection of HIF-1α, specimens were
incubated overnight at 4°C with the primary antibodies; HIF-1α
(1:100, Santa Cruz Biotechnology Inc., Santa Cruz, CA, USA), APE1
(1:100, Abcam, Cambridge, UK), VEGF (1:200, Santa Cruz
Biotechnology Inc.) and COX-2 (1:100, Abcam). The quality (number,
intensity and pattern) of every staining procedure for the proteins
was comparatively evaluated using the consecutive control sections.
The tumor cell immunoreactivity of HIF-1α, APE1 and COX-2 were
separated into four groups (7,13,14):
negative, mild positive, moderate positive and strong positive. The
tumor cell immunoreactivity of VEGF was separated into two groups
as reported previously (8):
negative and positive. The assessments were performed independently
by two experienced investigators blinded to the patient
clinicopathological data.
Statistical analysis
SPSS 13.0 statistical software was used for
statistical analysis. The correlation between the protein
expression levels and the clinicopathological parameters were
tested using the Spearman’s test for bivariate correlations. The
variables considered for their prognostic value included age at
diagnosis, gender, tumor size, margin status, chemotherapy, tumor
necrosis rate and protein expression. Survival curves were computed
by the Kaplan-Meier method and compared by the log-rank test.
Multivariate analyses based on the stepwise Cox proportional
hazards model were used to identify the most significant factors
related to outcome. A stepwise forward selection procedure was
used, and a significance level of 5% was selected as the criterion
for entering factors in the multivariate model. The association
between HIF-1α expression and various clinicopathological
characteristics were analyzed using the Chi-square test. P<0.05
was considered to indicate a stastically significant
difference.
Results
Correlation of HIF-1α protein expression
with clinicopathological parameters and tumor necrosis rate
The clinicopathological characteristics of the
patients are shown in Table I.
Amputation was performed in 5 patients and the limb-salvage rate
was 90% (44/49) in all patients. Of the 49 patients, HIF-1α was
negative in 22 patients (44.9%), mild positive in 10 (20.4%),
moderate positive in 9 (18.4%) and strong positive in 8 (16.3%).
The correlation between HIF-1α expression and the
clinicopathological parameters is shown in Table II. HIF-1α expression was
significantly associated with tumor size (P<0.001), AJCC stage
(P=0.030), metastasis (P=0.007) and tumor necrosis rate (P=0.001).
Other clinicopathological parameters, including gender, age and
surgery type were not associated with HIF-1α expression.
 | Table IPatient characteristics (n=49). |
Table I
Patient characteristics (n=49).
| Parameters | n |
|---|
| Total | 49 (100%) |
| Age, median
(range) | 18.5 (11–72) |
| Gender |
| Male | 28 (57%) |
| Female | 21 (43%) |
| AJCCa stage |
| IIA | 11 (22%) |
| IIB/III | 38 (78%) |
| Size, cm |
| Median (range) | 10.0 (3.5–15.0) |
| Neoadjuvant
chemotherapy cycles |
| 1 cycle | 24 (49) |
| 2 cycles | 25 (51) |
| Surgery |
| Limb-salvage | 44 (90) |
| Amputation | 5 (10) |
| Follow-up (mean) | 29 |
| Table IICorrelation between
clinicopathological parameters and HIF-1α protein expression in
osteosarcoma (n=49). |
Table II
Correlation between
clinicopathological parameters and HIF-1α protein expression in
osteosarcoma (n=49).
| Parameters | HIF-1α | | |
|---|
|
| | |
|---|
| − | 1+ | 2++ | 3+++ | rs | P-value |
|---|
| Agea | 18.5 (11–72) | 1.584 | 0.663 |
| Tumor size
(cm)b | 8.28±2.53 | 9.91±2.73 | 11.59±0.93 | 12.75±1.20 | 10.189 | <0.001 |
| pTNM stage | | | | | 0.310 | 0.030 |
| IIA | 7 | 4 | 0 | 0 | | |
| IIB/III | 15 | 6 | 9 | 8 | | |
| Metastasis | | | | | 0.380 | 0.007 |
| No | 18 | 5 | 4 | 3 | | |
| Yes | 4 | 5 | 5 | 5 | | |
| Tumor necrosis
rate | | | | | −0.464 | 0.001 |
| <90% | 3 | 6 | 6 | 5 | | |
| ≥90% | 19 | 4 | 3 | 3 | | |
HIF-1α expression was correlated to
prognostic factors APE1, VEGF and COX-2 in patients with
osteosarcoma
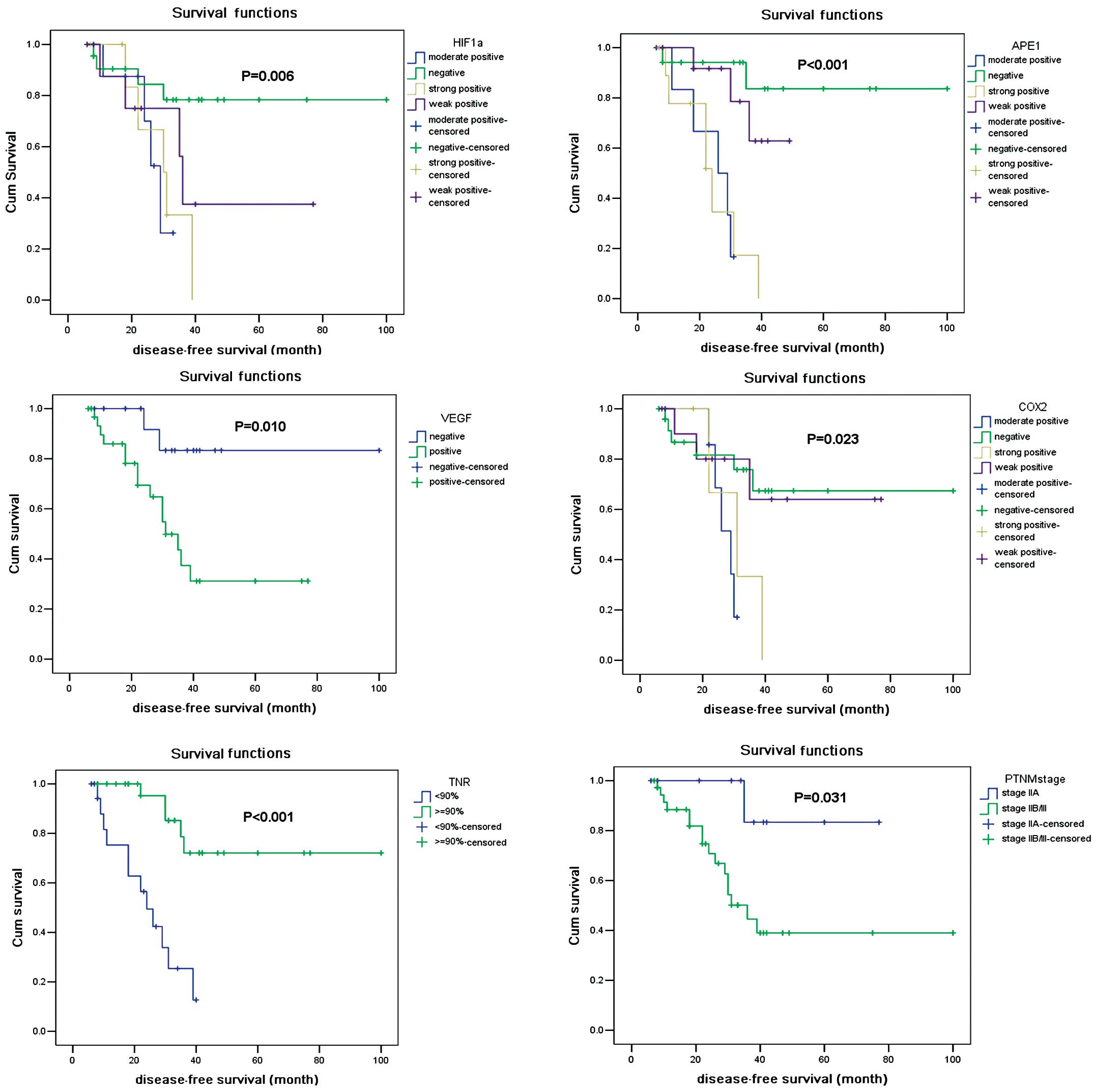
We firstly observed that HIF-1α expression was
associated with DFS using a univariate analysis (Fig. 1A), and an independent prognosticator
in OS (P=0.038) (Table III). APE1
was recognized as a co-factor that modulates the expression of
HIF-1α. We then investigated whether APE1 expression was prognostic
in OS and its correlation with HIF-1α. Of the 49 patients, the APE1
protein was negative in 17 patients (34.7%), mild positive in 13
(26.5%), moderate positive in 8 (16.3%) and strong positive in 11
patients (22.5%). APE1 protein expression was significantly
associated with DFS (P<0.001) (Fig.
1B). Expression of APE1 significantly correlated with HIF-1α
expression (P<0.001) and tumor necrosis rate (P<0.001).
| Table IIIMultivariate analysis of factors
associated with prognosis in osteosarcoma (n=49). |
Table III
Multivariate analysis of factors
associated with prognosis in osteosarcoma (n=49).
| Disease-free
survival |
|---|
|
|
|---|
| Factors | Risk ratio | 95% confidence
interval | P-value |
|---|
| pTNM stage
III/II | 2.339 | 0.232–23.578 | 0.019 |
| Tumor necrosis rate
≥90%/≤90% | 0.123 | 0.023–0.663 | 0.015 |
| HIF-1α
positive/negative | 6.068 | 1.107–33.257 | 0.038 |
| APE1
positive/negative | 9.728 | 1.408–67.190 | 0.021 |
VEGF was accepted to be a target of HIF-1α and its
expression was reported to be associated with tumor growth and
metastasis. A previous study has demonstrated that in OS patients
the survival rate of those with VEGF expression was substantially
worse than patients without VEGF expression (20). Of the 49 patients, the VEGF protein
was negative in 17 patients (34.7%) and positive in 32 (65.3%). The
VEGF protein expression was confirmed to be predictive for DFS
(Fig. 1C) (P=0.010). The expression
of VEGF was significantly correlated with HIF-1α expression
(P=0.032). This correlation is in accordance with a previous study
in OS cell lines (21). VEGF
expression was also corrrelated with APE1 (P=0.014).
COX-2 is a significant mediator in tumor invasion
and metastasis, and has been investigated to be a target for cancer
therapy (14). In our study, COX-2
protein was negative in 25 patients (51.0%), mild positive in 12
(24.5%), moderate positive in 7 (14.3%) and strong positive in 5
(10.2%). COX-2 expression was also associated with DFS (P=0.023)
(Fig. 1D). As shown in Table II, expression of COX-2 was
significantly correlated with HIF-1 (P<0.001), APE1 (P<0.001)
and VEGF (P=0.033).
Sensitivity and specificity in predicting
tumor necrosis rate
We aimed to find a marker to predict the tumor
necrosis rate prior to adjuvant chemotherapy in OS patients. As a
single predictor, a high expression of HIF-1α and/or APE1 was
significantly associated with poor tumor necrosis rate. A total of
71.9% (23/32) of patients with a negative/mild positive HIF-1α
expression had a good pathological response to neoadjuvant
chemotherapy, and 80.0% (24/30) of patients with a negative/mild
positive APE1 expression had a tumor necrosis rate of no less than
90%. By contrast, 64.7% (11/17) of patients with moderate/strong
positive HIF-1α expression revealed a poor response to neoadjuvant
chemotherapy, while 73.7% (14/19) of patients with a
moderate/strong positive APE1 expression had a tumor necrosis rate
of <90%. In patients with a negative/mild positive expression of
HIF-1α and APE1, 88.5% (23/26) of patients had a good pathological
response to neoadjuvant chemotherapy, while in those with a
moderate/strong positive expression of HIF-1α and APE1, 75.0%
(9/12) had a tumor necrosis rate of <90%, indicating that the
expression of HIF-1α and APE1 is a potential marker in predicting
tumor responses to chemotherapy in OS.
Discussion
In this study, we determined the protein expression
of HIF-1α, VEGF, APE1 and COX-2 in the pre-chemotherapy biopsy
samples of OS patients and determined the tumor necrosis rate in
their post-chemotherapy tumors. By using immunohistochemistry
analysis, we hoped to achieve a more precise understanding of the
associations of these protein expressions with each other and with
patients’ prognosis. Using the multivariate Cox regression
analysis, it was revealed that HIF-1α and APE1 protein expression
demonstrated the most significant impact on DFS in our patient
cohort (P=0.009).
The tumor necrosis rate following pre-operative
chemotherapy (histological response) is generally accepted to be
the strongest prognostic factor for OS patients without metastases
at initial diagnosis and it is also an indicator for post-operative
chemotherapy (22). Our study also
demonstrated that the tumor necrosis rate (Fig. 1E) and the AJCC stage (Fig. 1F) were prognostic factors in OS.
Recently, increasing efforts have emerged to find accessible
markers to predict tumor response prior to administration of
neoadjuvant chemotherapy in OS, but the significance of RANKL
expression in predicting a pathological response was concluded from
a small cohort study, in which the pathological response to
pre-operative chemotherapy was not correlated with survival
(23). Other markers, including
plasma proteome and microRNAs, require invasive procedures and are
unable to present the intrinsic characteristics of the tumor
samples or provide potential targets for improvements prior to
neoadjuvant chemotherapy (24,25).
HIF-1α overexpression was proven to be associated with a decreased
response to chemotherapy in various cancer types (4,5), but
little data were available which correlated HIF-1α and APE1
expression with the tumor necrosis rate in OS. In this study, we
determined that HIF-1α and APE1 expression may be reliable
predictors of pathological responses to neoadjuvant chemotherapy in
OS patients, indicating that a positive expression of HIF-1α and
APE1 may be new markers for selecting patients in whom neoadjuvant
chemotherapy is not enough and a combinational targeted therapy is
required.
The results of this pilot study also demonstrate a
strong correlation between HIF-1α and VEGF, which emphasizes the
role of HIF-1α in angiogenesis and its most prominent markers VEGF
and OS. Although we did not find a significant correlation between
VEGF expression and the tumor necrosis rate, our results showed
that a high VEGF expression significantly correlated with poorer
survival (P=0.010).
COX-2 expression has recently been correlated with
HIF-1α and VEGF. As a novel target, COX-2 has been investigated for
cancer therapy. In our study, COX-2 is significantly associated
with metastasis, indicating that patients, particularly with a
positive expression of COX-2, may require anti-COX-2 treatment in
adjuvant therapies to prevent tumor metastasis and improve long
term metastasis-free survival.
In conclusion, our study has provided supporting
evidence that HIF-1α protein expression is associated with the
pathological response and outcome in OS patients. This expression
correlated with upstream APE1 and downstream VEGF and COX-2. The
protein expression of HIF-1α and APE1 may be a potential marker and
predict pathological response to neoadjuvant chemotherapy. More
studies are required to investigate whether their inhibitors are
capable of increasing chemosensitivity and improving prognosis in
osteosarcoma patients, particularly those with poor pathological
responses to neoadjuvant chemotherapy.
Acknowledgements
This project was financially supported by the
National Natural Science Foundation of China (Grant Number
30900596). The authors thank Dr FengJu Song from the Department of
Epidemiology in the Key Laboratory of Cancer Prevention and
Treatment in Tianjin for statistical assistance.
References
|
1
|
Mankin HJ, Hornicek FJ, Rosenberg AE,
Harmon DC and Gebhardt MC: Survival data for 648 patients with
osteosarcoma treated at one institution. Clin Orthop Relat Res.
429:286–291. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bramwell VHC: The role of chemotherapy in
osteogenic sarcoma. Crit Rev Oncol Hematol. 20:61–85. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bramwell VHC: The role of chemotherapy in
the management of non-metastatic operable extremity osteosarcoma.
Semin Oncol. 24:561–571. 1997.PubMed/NCBI
|
|
4
|
Liu L, Ning X, Sun L, Zhang H, Shi Y, Guo
C, et al: Hypoxia-inducible factor-1 alpha contributes to
hypoxia-induced chemoresistance in gastric cancer. Cancer Sci.
99:121–128. 2008.PubMed/NCBI
|
|
5
|
Quintero M, Mackenzie N and Brennan PA:
Hypoxia-inducible factor 1 (HIF-1α) in cancer. Eur J Surg Oncol.
30:465–468. 2004.
|
|
6
|
Russell DL, Ian S and Adrian L: The role
of hypoxia-inducible factor-1 in three dimensional tumor growth,
apoptosis and regulation by the insulin-signaling pathway. Cancer
Res. 65:4147–4152. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang QC, Zeng BF, Dong Y, Shi ZM, Jiang ZM
and Huang J: Overexpression of hypoxia-inducible factor-1a in human
osteosarcoma: correlation with clinicopathological parameters and
survival outcome. Jpn J Clin Oncol. 37:127–134. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mizobuchi H, Castellano JMG, Philip S,
Healey JH and Gorlick R: Hypoxia markers in human osteosarcoma: an
exploratory study. Clin Orthop Relat Res. 466:2052–2059. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu Q, Yang SH, Ye SN and Wang RY:
Therapeutic effects of RNA interference targeting HIF-1 alpha gene
on human osteosarcoma. Nail Med J Chin. 85:409–413. 2005.PubMed/NCBI
|
|
10
|
Cai W, Chen A, Guo F and Zhu B: Effects of
HIF-1α antisense oligonucleotides on the expression of HIF-1α and
VEGF in the osteosarcoma cell line MG-63. Chi J Clin Oncol. 33:1–5.
2006.
|
|
11
|
Ho QT and Kuo CJ: Vascular endothelial
growth factor: biology and therapeutic applications. Int J Biochem
Cell Biol. 39:1349–1357. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sak SC, Harnden P, Johnston CF, Paul AB
and Kiltie AE: APE1 and XRCC1 protein expression levels predict
cancer-specific survival following radical radiotherapy in bladder
cancer. Clin Cancer Res. 11:6205–6211. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yang JL, Yang D, Cogdell D, Du XL, Li HX,
Pang Y, et al: APEX1 gene amplification and its protein
overexpression in osteosarcoma: correlation with recurrence,
metastasis and survival. Technol Cancer Res Treat. 9:161–169. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Geng YH, Wan CX and Chen PH: Expressions
of Cox-2 and HIF-lα and their relationship with clinicopathologic
characteristics of osteosarcoma. Tumor. 28:427–430. 2008.
|
|
15
|
Dickens S and Cripe TP: Effect of combined
cyclooxygenase-2 and matrix metalloproteinase inhibition on human
sarcoma xenografts. J Pediatr Hematol Oncol. 25:709–714. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Subbaramaiah K and Dannenberg AJ:
Cyclooxygenase 2: a molecular target for cancer prevention and
treatment. Trends Pharmacol Sci. 24:96–102. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
American Joint Committee on Cancer. AJCC
Cancer Staging Manual. Greene FL, Balch CM, Page DL, Haller DG,
Fleming ID, Morrow M and Fritz AG: 6th edition. Springer-Verlag;
New York: 2002, View Article : Google Scholar
|
|
18
|
Ferrari S and Palmerini E: Adjuvant and
neoadjuvant combination chemotherapy for osteogenic sarcoma. Curr
Opin Oncol. 19:341–346. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rosen G, Caparros B, Huvos AG, et al:
Preoperative chemotherapy for osteogenic sarcoma: selection of
post-operative adjuvant chemotherapy based on the response of the
primary tumor to preoperative chemotherapy. Cancer. 49:1221–1230.
1982. View Article : Google Scholar
|
|
20
|
Kaya M, Wada T, Akatsuka T, et al:
Vascular endothelial growth factor expression in untreated
osteosarcoma is predictive of pulmonary metastasis and poor
prognosis. Clin Cancer Res. 6:572–577. 2000.PubMed/NCBI
|
|
21
|
Wu Q, Yang SH, Wang RY, Ye SN, Xia T and
Ma DZ: Effect of silencing HIF-1α by RNA interference on expression
of vascular endothelial growth factor in osteosarcoma cell line
SaOS-2 under hypoxia. Chin J Cancer. 24:531–535. 2005.
|
|
22
|
Bielack SS, Kempf-Bielack B, Delling G, et
al: Prognostic factors in high-grade osteosarcoma of the
extremities or trunk: an analysis of 1,702 patients treated on
neoadjuvant cooperative osteosarcoma study group protocols. J Clin
Oncol. 20:776–790. 2002. View Article : Google Scholar
|
|
23
|
Lee JA, Jung JS, Kim DH, et al: RANKL
expression is related to treatment outcome of patients with
localized, high-grade osteosarcoma. Pediatr Blood Cancer.
56:738–743. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li Y, Dang TA, Shen J, Hicks J,
Chintagumpala M, Lau CC, et al: Plasma proteome predicts
chemotherapy response in osteosarcoma patients. Oncol Rep.
25:303–314. 2011.PubMed/NCBI
|
|
25
|
Gougelet A, Pissaloux D, Besse A, Perez J,
Duc A, Dutour A, et al: Micro-RNA profiles in osteosarcoma as a
predictive tool for ifosfamide response. Int J Cancer. 129:680–690.
2011. View Article : Google Scholar : PubMed/NCBI
|