Introduction
Primary breast lymphoma (PBL) is a rare condition
which affects less than 1% of patients with non-Hodgkin’s lymphoma
(NHL) and constitutes less than 2% of all extranodal NHLs (1). Neurolymphomatosis (NL) is a rare
manifestation characterized by the infiltration of peripheral
nerves, nerve roots, nervous plexuses or cranial nerves by
malignant lymphocytes (2).
Involvement of the cranial and peripheral nerves is an unusual
manifestation of NL which is occasionally difficult to diagnose
using conventional imaging modalities. 18F-FDG PET/CT is
being increasingly used for the diagnosis and staging of NHL and it
also appears to be a highly sensitive diagnostic method for
facilitating the identification of NL (2). The present case report describes a
patient in complete remission of PBL who demonstrated increasing
uptake of 18F-FDG in the cranial and peripheral nerves,
suggestive of NL. Informed consent was obtained from the patient
prior to the study.
Case report
A 45-year-old female was admitted complaining of
headache, impaired hearing on the right side, bilateral facial
hypesthesia, decreased vision, diplopia, lumbodorsal pain and
weakness in both inferior extremities. The patient had been
diagnosed with stage IIb non-Hodgkin’s lymphoma in her left breast
two years previously, which was identified as a CD20-positive
diffuse large B cell phenotype following lumpectomy. A total of 8
cycles of R-CHOP chemotherapy led to complete remission. However,
following 16 months, the patient developed multiple neurological
symptoms. Cerebrospinal fluid (CSF) analysis revealed increased
protein (325 mg/dl) and the cytology was positive for malignant
lymphocytes. CSF tests for tuberculosis, viruses and fungi were
negative.
Whole body 18F-FDG PET/CT was performed
to assess the extent of relapse. The patient fasted for at least 6
h prior to undergoing scanning and the fasting blood sugar level
was <6.1 mmol/l. To prevent muscular radiotracer uptake, the
patient was instructed to sit without speaking and avoid strenuous
activity prior to the examination and following injection of the
radioisotope. A standard dose of 18F-FDG 0.1 mCi/kg was
intravenously injected 60 min prior to scanning. The data were
acquired with a combined PET/CT in-line system (GE Discovery STE
16) with the following parameters: section thickness
3.75 mm, pitch 1.0 and FOV 70 cm. 18F-FDG PET/CT
revealed multiple nodular or linear hypermetabolic lesions along
the right acoustic nerve [maximum standardized uptake value
(SUVmax), 7.98; Fig. 1A], bilateral
trigeminal nerves (SUVmax, 8.91, 10.25; Fig. 1B), the optic chiasm (SUVmax, 4.73;
Fig. 1C), the left nerve root of
T11/12 (SUVmax, 4.79; Fig. 1D), the
right nerve root of T12/L1 (SUVmax, 4.52; Fig. 1E) and the right adrenal gland
(SUVmax, 4.05; Fig. 1F), while CT
imaging revealed that the right adrenal gland and optic chiasm were
normal. 18F-FDG PET/CT also revealed increased FDG
uptake in the left retroperitoneal space (SUVmax, 5.48; Fig. 1F) where CT identified a strip-like
soft tissue lesion between the left adrenal gland and abdominal
aorta. Although a nerve biopsy was not performed, relapse of
lymphoma and NL were diagnosed by 18F-FDG PET/CT and
positive CSF cytology. The symptoms were markedly relieved
following two cycles of R-CHOP chemotherapy.
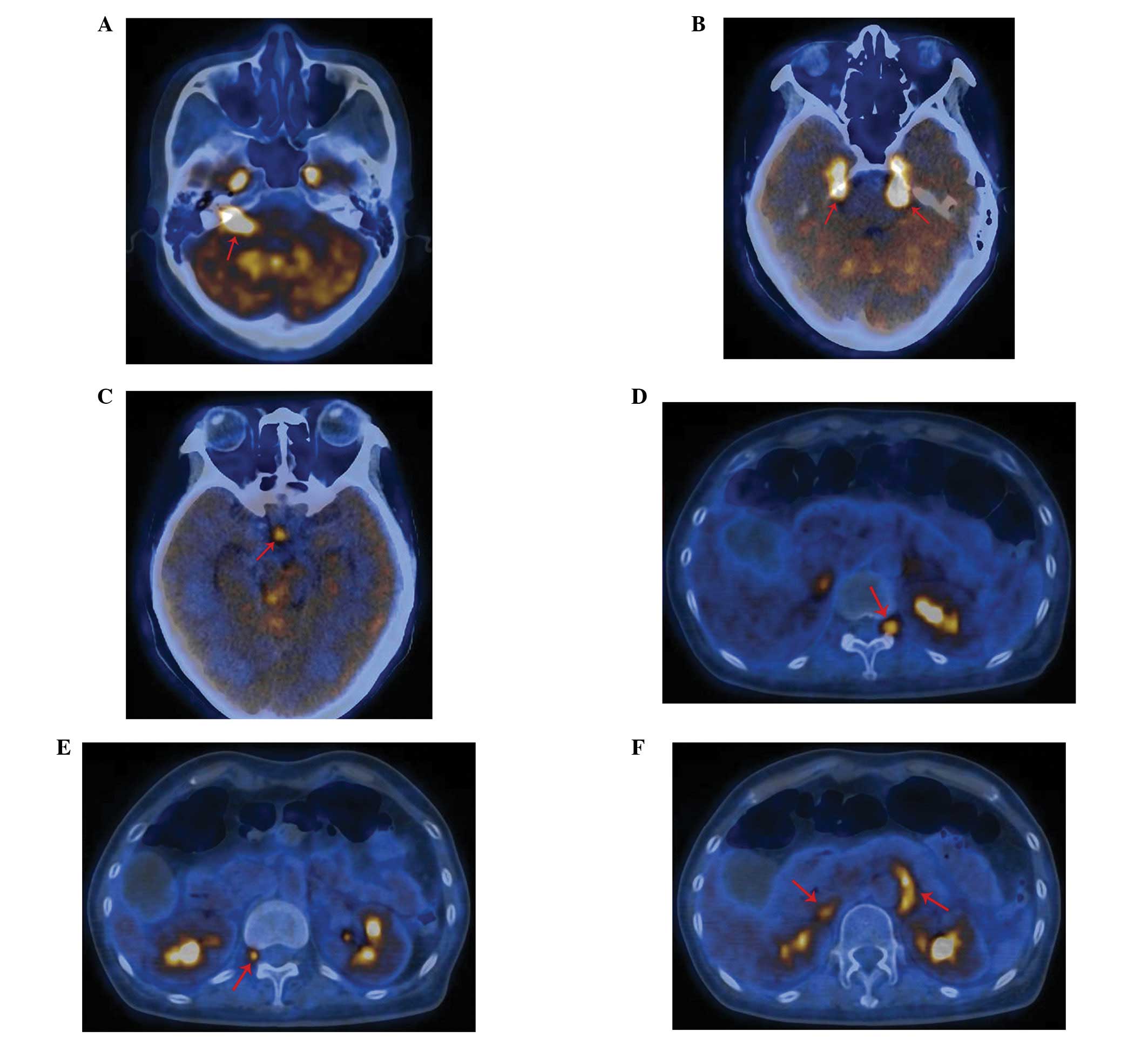 | Figure 118F-FDG PET/CT images
showing linear or nodular hypermetabolic lesions (red arrow)
involving multiple cranial and peripheral nerves, corresponding to
the patient’s complex neurological symptoms, including impaired
hearing in the right side, bilateral facial hypesthesia, decreased
vision, diplopia, lumbodorsal pain and weakness in both inferior
extremities. 18F-FDG PET/CT showing increased
18F-FDG uptake along (A) the right acoustic nerve, (B)
the bilateral trigeminal nerves and Meckel’s caves, (C) in the
optic chiasm. 18F-FDG PET/CT showing increased
18F-FDG uptake in (D) the left nerve root of T11/12, (E)
the right nerve root of T12/L1, (F) a strip-like soft tissue lesion
between the left adrenal gland and abdominal aorta. |
Discussion
PBL is used to define malignant lymphoma primarily
occurring in the breast in the absence of previously detected
lymphoma localizations. The most common type of PBL is the diffuse
large B cell type. In this case, the patient, without a notable
medical history, presented with a rapidly growing mass in the left
breast. A systemic examination revealed no extramammary lymphoma
and a lumpectomy was performed. Histopathological and
immunohistochemical findings confirmed a diffuse large B cell type
lymphoma.
NHL may involve the nervous system at every level,
including the peripheral nerves, spinal nerve roots, spinal cord,
meninges and brain. NL is a rare manifestation of malignant
lymphoma in which the malignant lymphocytes infiltrate the
peripheral nervous systems. NL is usually disclosed in proximal
sites, including roots, spinal ganglia, nervous plexuses and
proximal trunks (3). The
involvement of the cranial and peripheral nerves in patients with
PBL has rarely been documented. A study of 84 consecutive patients
with PBL treated in 20 institutions identified that 12 patients
suffered from a relapse in the central nervous system, but no
patients presented with relapse in the peripheral nerves (4). In the present case, the chief
complaints included multiple neurological symptoms, which were
consistent with certain pathological changes in the nervous system.
Further examinations were performed to assess the involvement of
the nervous system and the extent of relapse.
Diagnosis of NL is often difficult and depends on
the histopathological identification of infiltrating malignant
lymphocytes in the affected nerves. However, nerve biopsy may yield
false negative results despite the widespread lymphomatous
infiltration of peripheral nerves (5). CSF cytological examination may lead to
a false diagnosis since only a minority of NL cases reported
present with positive CSF cytology at the initial diagnosis.
Alternatively, imaging studies are of great value in diagnosing NL
prior to histopathological confirmation. In the past, the imaging
evaluation and follow-up of lymphoma patients was based solely on
the findings from contrast-enhanced CT. However, contrast-enhanced
CT has limited sensitivity in detecting lymphomatous involvement of
normal-sized lymph nodes, bone marrow, spleen and extranodal
tissues (6). Magnetic resonance
imaging (MRI) is the most commonly used modality in the diagnosis
and therapy of patients with lymphomatous infiltration of nerves. A
retrospective study by Grisariu et al (2) of 50 patients with NL revealed that
18F-FDG PET/CT and MRI was positive in 84 and 77% of
patients, respectively. While MRI typically shows the enlargement
and enhancement of affected nerves, it does not always provide
optimal visualization of lymphomatous involvement of peripheral
nerves. In such cases, 18F-FDG PET/CT provides
additional information that aids the correct identification of
recurrence or exclusion of other diseases (7). In a previous systematic review, the
overall sensitivity and specificity of 18F-FDG PET/CT
for the initial staging of NHL and Hodgkin’s disease were 97 and
100%, respectively (8). A case
report of NL on 18F-FDG PET/CT and MRI findings
demonstrated that 18F-FDG PET/CT detected peripheral nerve
infiltration by malignant lymphoma earlier than MRI (9). A study by Bronstein et al
(10) indicated that
18F-FDG PET/CT is useful in diagnosing the malignant
involvement of the peripheral nerves, particularly when findings
from anatomical imaging (MRI or CT) are negative. The advanced
technique of 18F-FDG PET/CT provides improved anatomical
details of less commonly involved peripheral nerves, particularly
in cases with NL. However, similar to MRI, 18F-FDG
PET/CT also has diagnostic limitations. 18F-FDG uptake
is highly sensitive for tumors but is not specific and may also be
observed in any process where the rate of glycolysis is increased,
including infection or neoplastic diseases. According to Hong et
al (9) and Bronstein et
al (10), the diagnosis of NHL
required integrated clinical information from 18F-FDG
PET/CT as well as CSF cytological examination.
In the present case, CT imaging revealed the
enlargement of multiple cranial and peripheral nerves, while PET
imaging revealed increased 18F-FDG uptake along these
nerves. Subsequently, positive CSF cytology also aided the
diagnosis of NL. The diagnosis was confirmed following careful
integration of all the relevant clinical findings from 18F-FDG
PET/CT and CSF cytological examination. The symptoms, including
headache and lumbodorsal pain, were markedly relieved following two
cycles of R-CHOP chemotherapy.
In cases of known treated malignancy involving the
peripheral nerves, follow-up by 18F-FDG PET/CT has the
advantage of high sensitivity in detecting local recurrence.
Therefore, it is recommended that 18F-FDG PET/CT should
be performed to evaluate the possibility of NL in patients with a
history of lymphoma presenting with neurological symptoms.
References
|
1.
|
HS MasonV JohariDE MarchGM CrisiPrimary
breast lymphoma: radiologic and pathologic findingsBreast
J11495496200510.1111/j.1075-122X.2005.00167.x16297110
|
|
2.
|
S GrisariuB AvniTT
BatchelorNeurolymphomatosis: an International Primary CNS Lymphoma
Collaborative Group
reportBlood11550055011201010.1182/blood-2009-12-25821020368468
|
|
3.
|
S KahramanH SabuncuogluO GunhanMA GursesS
SirinA rare reason of foot drop caused by primary diffuse large
b-cell lymphoma of the sciatic nerve: case reportActa Neurochir
(Wien)152125128201010.1007/s00701-009-0339-919415174
|
|
4.
|
V StefoniA BroccoliC PellegriniE
DerenziniM FinaPL ZinzaniCNS recurrence of primary mediastinal
large b-cell lymphoma after complete remissionJ
Neurooncol95135139200910.1007/s11060-009-9898-019381440
|
|
5.
|
MJ van den BentHG de BruinGM BosG Brutel
de la RivièrePA Sillevis SmittNegative sural nerve biopsy in
neurolymphomatosisJ Neurol24611591163199910653308
|
|
6.
|
FM PaesDG KalkanisPA SiderasAN SerafiniFDG
PET/CT of extranodal involvement in non-Hodgkin lymphoma and
Hodgkin
diseaseRadiographics30269291201010.1148/rg.30109508820083598
|
|
7.
|
H PalmedoH UrbachH BenderFDG-PET in
immunocompetent patients with primary central nervous system
lymphoma: correlation with MRI and clinical follow-upEur J Nucl Med
Mol Imaging33164168200610.1007/s00259-005-1917-616220304
|
|
8.
|
E Even-SapirG LievshitzC PerryY HerishanuH
LermanU MetserFluorine-18 fluorodeoxyglucose PET/CT patterns of
extranodal involvement in patients with Non-Hodgkin lymphoma and
Hodgkin’s diseaseRadiol Clin North Am45697709vii2007
|
|
9.
|
CM HongS-W LeeHJ LeeNeurolymphomatosis on
F-18 FDG PET/CT and MRI findings: A case reportNucl Med Mol
Imaging457678201110.1007/s13139-010-0070-824899982
|
|
10.
|
Y BronsteinS TummalaE RohrenF-18 FDG
PET/CT for detection of malignant involvement of peripheral nerves:
case series and literature reviewClin Nucl
Med3696100201110.1097/RLU.0b013e318203bb0e21220969
|














