Introduction
Technological development has led, over time, to the
introduction and use of new devices in medicine and surgery. Laser
instruments (light amplification by stimulated emission of
radiation) have emerged in clinical practice based on the effects
of coherent and collimated monochromatic light radiation with high
brightness on chromophores or optical baits that are normally
present in biological tissues.
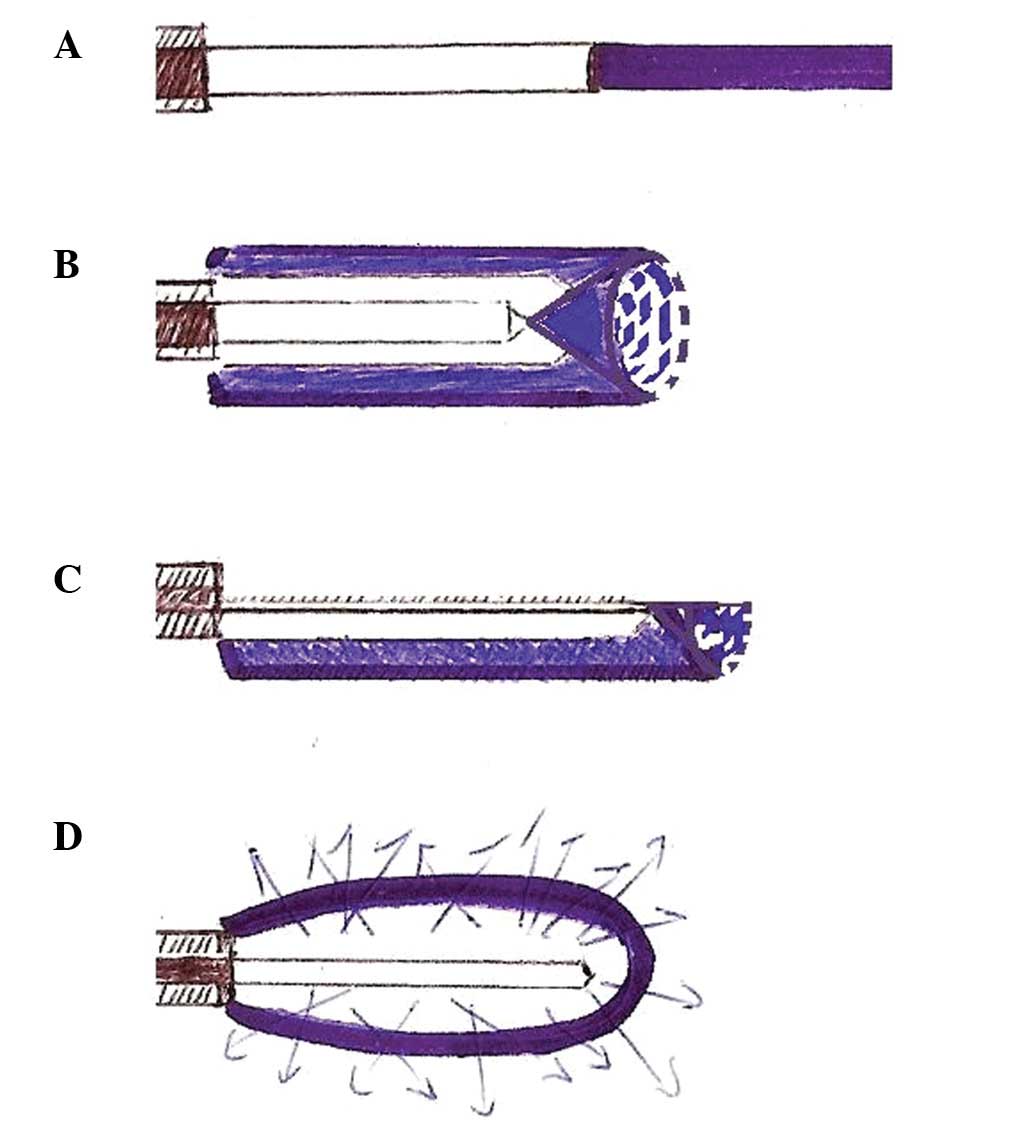
The use of lasers such as
neodymium:yttrium-aluminum-garnet (Nd:YAG) initially have been of
great importance in the field of endoscopy and surgery due to their
applications in coagulation. Moreover, lasers have the ability to
vaporize tissue with great penetrating capacity with the
possibility of spreading into the interstice by flexible fibers of
various sizes, shapes and sections, creating well-demarcated
necrosis without significant damage to the adjacent structures
(Fig. 1) (1–3).
From the early 1990s, however, new devices based on
a different technology were introduced. In particular, in 1992 the
argon-plasma-coagulation (APC) system was introduced in endoscopy
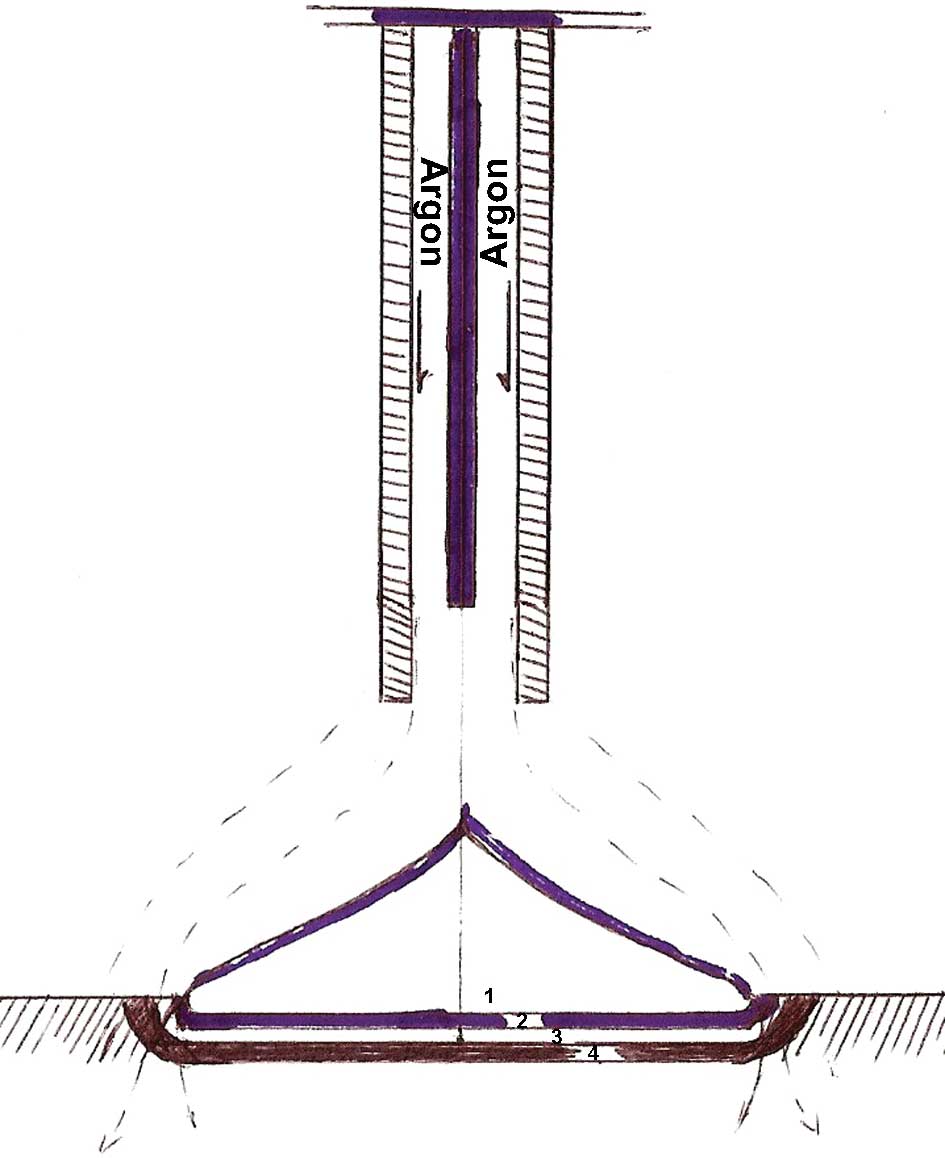
(4). The APC allows, without direct
contact, a high frequency monopolar current through a plasma gas
(argon) (4). The biological effect
of the high frequency carried by the plasma current to tissues is
heating of the tissue that is capable of leading to different
thermal effects: devitalization, coagulation, drying and
contraction (Fig. 2) (5). In the literature, various possible
endoscopic applications of this device have been reported.
APC has been used in endoscopic hemostatic treatment
for bleeding from several different sources and at different levels
(5), including in the treatment of
refractory ulcerative recto-colitis (6), Barrett’s esophagus (7), Dieulafoy’s lesions (8), stenosis in colon malignant tumors
(9), in radiation-induced proctitis
(10), adenomas (11,12)
and angiodysplasia (13).
The APC platform for endoscopic applications is
marketed in two models (Conmed, Utica, NY, USA; ERBE
Electromedizin, Tubingen, Germany) and includes a monopolar
frequency electrosurgical generator, a source of argon gas, a gas
flow meter, flexible catheters, a pedal of activation and a petri
dish to ground.
The probes consist of a Teflon tube coupled to a
ceramic nozzle hosting a monopolar tungsten electrode (Fig. 2). The APC is widely used due to the
easy application and lower rate of perforation compared to laser
therapy, by virtue of tissue penetration of 1–3 mm. Nevertheless,
the APC procedure is not risk-free. Rare complications cannot be
excluded and are capable of resulting in major injuries and
mortality (5).
With the increase in the number of possible
applications and the volume of patients, possible common or unusual
side effects have been reported in the literature. The most common
symptoms are anorectal pain for localized treatment near the
dentate line, meteorism and abdominal cramps with vagal signs of
visceral distension (14).
The most frequent complications are perforations by
penetration even in relatively infrequent loci (15), but cases of perforation by explosion
have also been described (16).
Manner et al (16) define
explosion as a sudden release of energy that leads to a rapid
increase in temperature and pressure. This event may occur when a
mixture of explosive gases reaches a trigger temperature. Normally
in the colon, hydrogen and methane are produced for the
fermentation of non-absorbable (lactulose, mannitol) or partially
absorbable (lactose, fructose, sorbitol) carbohydrates in the lumen
of the colon by resident bacterial flora (16).
Therefore, to minimize the possible risks associated
with a sudden release of energy, it is necessary to properly
prepare the colon, forbidding the use of preparations containing
these substances; however, enemas should be performed. It is also
important to take particular caution in the vicinity of tight
stenosis for the possible presence of gas pockets upstream of the
stenosis itself, which could be released by the procedure. This
report describes a case of colon explosion at a distance from the
surgically treated area.
This study was approved by the ethics committee of
the University of Perugia and of the Sapienza University of Rome.
The patient provided written informed consent for permission to
perform surgical and endoscopic procedures, to transfuse blood (in
case of need), to inform relatives (wife and/or parents) about the
patient clinical outcome and to use the data and/or pictures for
scientific purpose.
Case report
In this study, we report a 73-year-old patient, who
underwent emergency surgery for suspected colonic perforation
following endoscopic treatment with APC. The patient, who had a
history of hypertension and prostate cancer, underwent endoscopic
coagulation using APC for rectal angiodysplasia and bleeding
arising following radiotherapy performed for prostate cancer.
For this purpose the patient had an evacuative
micro-enema without the addition of oral preparations. The operator
of the endoscopy heard a thump during the execution of the
procedure Therefore, the probe was immediately removed and an X-ray
of the abdomen was performed that revealed signs of
perforation.
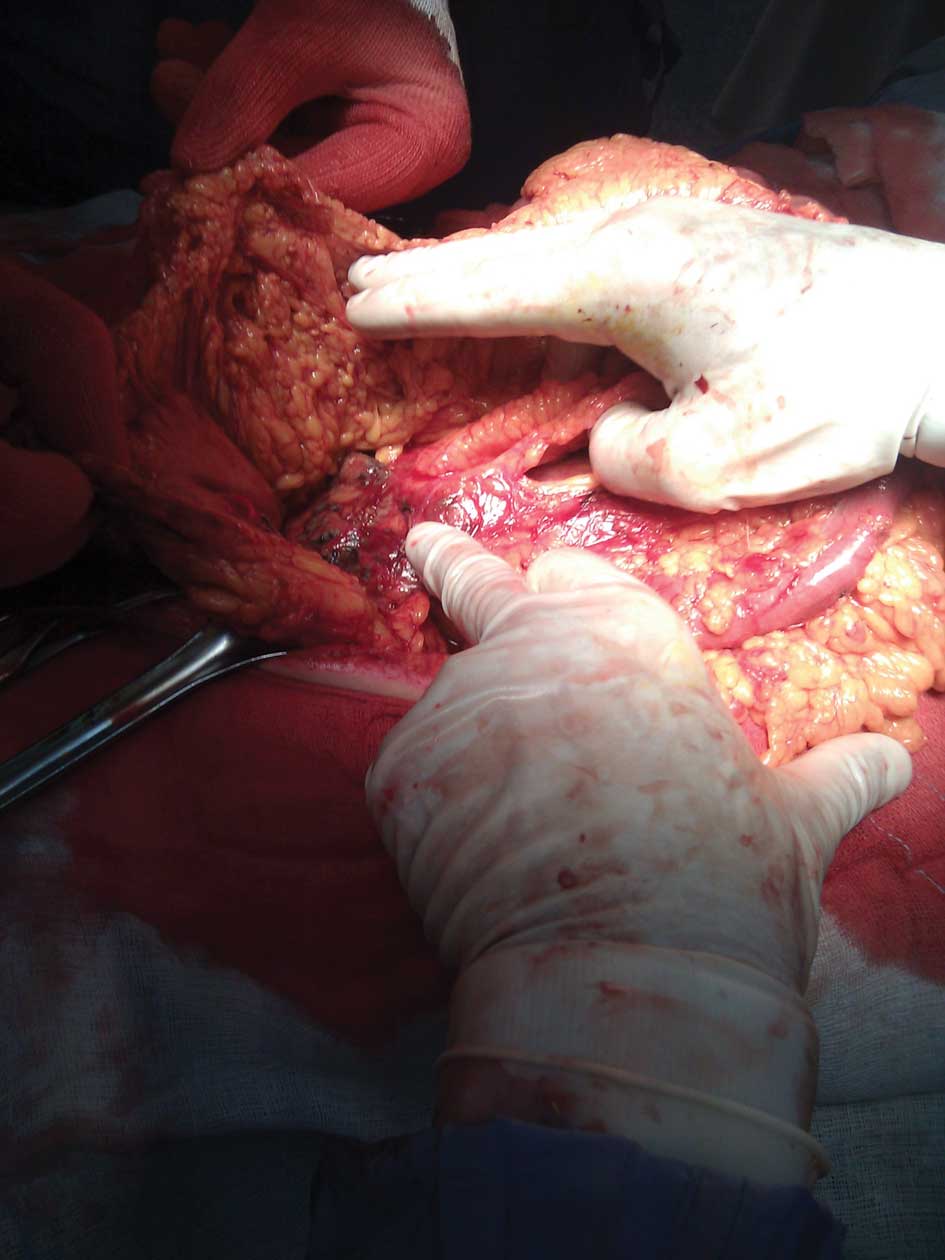
The patient underwent surgery for acute abdomen with
findings of fecal peritonitis of the pelvis and left iliac fossa by
double-tearing of the colon sigmoid associated with mesosigmoid
hematoma, vascular laceration and hemoperitoneum (Figs. 3 and 4). Resection of the bowel and the sinking
of the rectum by stapler were performed. The colostomy was
performed in the left iliac fossa, on the distal descending
colon.
The hospital stay was complicated by two episodes:
pulmonary edema with bilateral pleural effusion and atelectasis on
the eighth day, as shown by CT scan, which was solved with medical
therapy; a wound dehiscence that was treated with convac. The
patient was discharged in good health on the 32nd day while waiting
for recanalization.
Discussion
In the literature, during the last decade, several
cases of colonic explosions during APC procedures have been
reported. Such cases were observed in the treatment of stenosis of
the colon, adenomas, angiodysplasia and proctitis caused by
radiation (Table I). The incidence
has been significantly higher in those cases where the colon was
prepared locally than in those where oral preparations occurred
(9,11,12).
 | Table IOverview of cases of colonic
explosion during treatment with APC. |
Table I
Overview of cases of colonic
explosion during treatment with APC.
| Year | No. | Author | Diagnosis | Preparation | Complication |
|---|
| 1999 | 1 | Zinsser et
al (9) | Neoplastic stenosis
of the recto-sigmoid junction | Enema | Explosion without
perforation |
| 2004 | 1 | Pichon et al
(12) | Adenoma of the
sigmoid colon | Enema | 3 perforated
lesions of sigmoid |
| 2004 | 3 | Ben-Soussan et
al (10) | Radiation
proctitis | Enema | 1 perforation |
| 2007 | 1 | Townshend et
al (11) | Adenoma of rectum
with bleeding | Enema | Explosion of sigma
with laceration, Hartmann intervention |
| 2007 | 1 | Nurnberg et
al (13) | Angiodysplasia of
right colon | Macrogol
solution | 2 perforations of
cecum and ascending colon, right hemicolectomy |
| 2010 | 1 | Trastulli et
al (Present study) | Angiodysplasia of
the rectum due to radiation | Mini enema | Explosion of sigma
with laceration, Hartmann intervention |
Ben-Soussan et al treated 27 patients with
APC for radiation-induced hemorrhagic proctitis. Prior to treatment
with APC, the colon was prepared with enema polyethylene glycol or
sodium phosphate. During treatment, in two patients there were
three explosions of the colon. The first patient experienced two
explosions in succession. The second patient had an explosion that
led to an immediate perforation of an area away from that treated
endoscopically (10).
In 2007, Nurnberg et al reported a case of a
69-year-old patient with an explosion of the colon during treatment
with APC. In contrast to the literature, in this case the patient
was prepared with Macrogol solution (13). This was the first case described in
the literature of a perforated colon during endoscopic treatment
with APC in a patient prepared with Macrogol solution.
The following adverse events may be the trigger for
explosive gas mixtures (16): The
use of oral preparations that may lead to fermentation (13); or simple enemas to evacuate the
large bowel, but without oral preparation (10). To date, there is no consensus on the
guidelines for the intestinal preparation before APC, also in
regards of drugs for oral preparation (17). In our case, the preparation was
further reduced and although the endoscopist worked in the lower
rectum, with the reasonable assumption of the absence of pockets of
gas, there was, however, a distant explosion, which led to serious
injury and risk to the life of the patient.
Subsequently, it appears that the risk of explosion
with this method is real even for minor endoscopic procedures, it
may occur in the more distant colonic segments and it is clearly
machine- or operator-independent. It depends only on the
unpredictable amount of intestinal gases and their motion.
Therefore, it is desirable that proper preparation
for colon cleansing both orally and through enemas occurs, as well
as a reduction of meteorism by administering a proper diet to the
patient in preparation for the procedure and the use of aids such
as a rectal tube placed just before the procedure to drain any
pockets of gas present in the colonic segments.
In case of explosion the injuries are extremely
serious due to the association of peritonitis and hemoperitoneum,
and the treatment should be limited to the minimum according to the
theory of ‘damage control surgery’.
References
|
1.
|
C PhilippE RohdeHP BerlienNd:YAG laser
procedures in tumor treatmentSemin Surg
Oncol11290298199510.1002/ssu.29801104047481366
|
|
2.
|
TJ VoglMG MackR StraubA RogganR
FelixMagnetic resonance imaging-guided abdominal interventional
radiology: laser-induced thermotherapy of liver
metastasesEndoscopy29577583199710.1055/s-2007-1004261
|
|
3.
|
E RohdeI Mesecke-von RheinbarenA RogganH
PodbielskaM HopfG MullerInterstitial laser-induced thermotherapy
(LITT): comparison of in-vitro irradiation effects of Nd:YAG (1064
nm) and diode (940 nm) laserMed Laser
Appl168190200110.1078/1615-1615-00014
|
|
4.
|
JJ VargoClinical applications of the argon
plasma coagulatorGastrointest
Endosc598188200410.1016/S0016-5107(03)02296-X14722558
|
|
5.
|
KE GrundT StraubG FarinNew haemostatic
techniques: argon plasma coagulationBaillieres Best Pract Res Clin
Gastroenterol136784199910.1053/bega.1999.000911030635
|
|
6.
|
J DumortierJY ScoazecT PonchonArgon plasma
coagulation therapy for refractory ulcerative colitisGastrointest
Endosc60317319200410.1016/S0016-5107(04)01562-7
|
|
7.
|
JP BateMN SchoemanArgon plasma coagulation
for Barrett’s esophagusTech Gastrointest Endosc1240432010
|
|
8.
|
JC YarzeArgon plasma coagulation of
Dieulafoy’s lesionsGastrointest Endosc637332006
|
|
9.
|
E ZinsserU WillP GottschalkBowel gas
explosion during argon plasma
coagulationEndoscopy31S26199910376468
|
|
10.
|
E Ben-SoussanM AntoniettiG SavoyeArgon
plasma coagulation in the treatment of hemorrhagic radiation
proctitis is efficient but requires a perfect colonic cleansing to
be safeEur J Gastroenterol
Hepatol1613151318200410.1097/00042737-200412000-00013
|
|
11.
|
AP TownshendWP GoddardJA CidBowel
perforation requiring emergency laparotomy and a Hartmann’s
procedure after a gas explosion induced by argon plasma
coagulationEndoscopy39E1200720148255
|
|
12.
|
N PichonF MaisonnetteF CessotColonic
perforations after gas explosion induced by argon plasma
coagulationEndoscopy36573200410.1055/s-2004-81443115202067
|
|
13.
|
D NurnbergH PannwitzKD BurkhardtGas
explosion caused by argon plasma coagulation of colonic
angiodysplasiasEndoscopy39E182200710.1055/s-2007-96640417614056
|
|
14.
|
A PostgateB SaundersJ TjandraArgon plasma
coagulation in chronic radiation
proctitisEndoscopy39361365200710.1055/s-2007-966284
|
|
15.
|
B ProstG PoncetJ ScoazecUnusual
complications of argon plasma coagulationGastrointest
Endosc59929932200410.1016/S0016-5107(04)01268-415173821
|
|
16.
|
H MannerN PlumO PechC EllMD EnderleColon
explosion during argon plasma coagulationGastrointest
Endosc6711231127200810.1016/j.gie.2008.02.03518513555
|
|
17.
|
ASGE Technology CommitteeP MamulaDG
AdlerJD ConwayColonoscopy preparationGastrointest
Endosc6912011209200910.1016/j.gie.2009.01.035
|