Introduction
Squamous cell carcinoma of the head and neck (SCCHN)
is the sixth most frequent type of cancer worldwide (1), with more than half a million new cases
reported annually (2). The 5-year
survival rate is approximately 50%, which is one of the lowest
among the more common cancer types. Radiotherapy (RT) remains the
major approach to curative treatment despite improvements in
chemotherapy schedules (3,4), and it is therefore of interest to
study how RT affects potential biomarkers such as those below.
Hyaluronan (HA) is a linear disaccharide polymer
belonging to the family of glycosaminoglycans, which comprises the
major fraction of carbohydrates in the extracellular matrix (ECM).
The loose HA matrix provides a favourable environment for mitotic
cells and is essential for numerous functions, including cell
migration and tissue remodelling during the morphogenesis of
organs. HA is also thought to enhance wound healing, tumour growth
and metastasis (5). In SCCHN, HA
mediates the formation of a complex between the receptor CD44 and
the epidermal growth factor receptor (EGFR) (6) which is overexpressed in a large
proportion of SCCHN cases (7).
EGFR is a transmembrane protein receptor that plays
an essential role in regulating cellular processes such as
proliferation, differentiation and survival, and is also central to
the maintenance of normal epidermal tissue, where its expression is
highly regulated (8,9). When deregulated, EGFR aids in the
growth and survival of cancer cells, and is therefore an important
target in cancer therapy using monoclonal antibodies (10). EGFR-mediated pathways are involved
in the HA/CD44 promotion of chemoresistance in SCCHN (11).
Mast cells are among the first of several
immunological cell types migrating to the site of tissue damage,
e.g. radio-induced tissue injury. Mast cells cause inflammation by
secreting reactive oxygen species, vasoactive molecules, cytokines,
chemokines and proteases that remodel the ECM (12). SCCHN tumours, however, have shown a
lower number of mast cells than squamous cell carcinoma tumours in
other locations (13).
In order to further map the effect of RT in SCCHN we
explored the expression of HA and EGFR and presence of mast cells
in tumours and adjacent tissue before and after RT.
Materials and methods
Study population
Sixteen patients with SCCHN treated at the
Departments of Otolaryngology and Head and Neck Surgery and
Oncology, Umeå University Hospital (Umeå, Sweden) between 2001 and
2009 were included. Patients were selected from a larger cohort of
patients with the inclusion criteria that they had undergone RT and
also had biopsies before and after treatment. Medical records were
reviewed and relevant clinical data recorded, including survival,
age, tumour site and stage. All patients had at least two years of
follow-up (Table I). Informed
consent was obtained from the patients prior to the study.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Patient number | Site | TNM |
Differentiation | Irradiation
(Gy) | Surgery | Residual
tumour | Age at diagnosis
(years) | Gender | 2-year
survival |
|---|
| 1 | Piriform sinus | T4N3M0 | Poor | 68 | No | No | 70 | M | No |
| 2 | Palatine arch | T2N2cM0 | Moderate | 68 | Yes | No | 59 | M | Yes |
| 3 | Gingiva | T4N1M0 | Moderate | 68 | No | No | 51 | M | Yes |
| 4 | Gingiva | T4N2bM0 | Moderate | 68 | No | No | 80 | F | Yes |
| 5 | Hard palate | T4N0M0 | Moderate | 68 | Yes | No | 63 | M | Yes |
| 6 | Gingiva | T4N2bM0 | Moderate | 68 | No | No | 83 | M | Yes |
| 7 | Bucca | T4N0M0 | Poor | 68 | Yes | Yes | 85 | F | Yes |
| 8 | Tongue | T4N0M0 | Poor | 68 | No | No | 48 | M | Yes |
| 9 | Tongue | T4N2bM0 | Poor | 68 | No | No | 43 | M | No |
| 10 | Gingiva | T4N1M0 | Moderate | 68 | Yes | No | 73 | F | Yes |
| 11 | Tongue | T2N0M0 | Poor | 68 | Yes | No | 74 | M | Yes |
| 12 | Tongue | T4N2cM0 | Poor | 68 | No | No | 61 | M | Yes |
| 13 | Palatine arch | T3N2bM0 | Moderate | 68 | No | No | 52 | M | Yes |
| 14 | Floor of mouth | T4N2bM0 | Moderate | 68 | Yes | No | 78 | F | No |
| 15 | Tonsil | T2N2cM0 | Poor | 68 | Yes | No | 53 | M | Yes |
| 16 | Tongue | T4aN0M0 | Moderate | 66 | No | No | 70 | M | Yes |
In general, treatment for SCCHN was based on the TNM
classification, stage and patient performance. All patients were
discussed at a multidisciplinary conference and treatment was given
with curative intent.
Patients received RT from a linear accelerator in
one daily fraction of 2 Gy 5 days a week, with a mean total dose of
68 Gy.
Seven of the patients received combined modality
treatment (preoperative RT followed by surgical resection) and 9
patients single modality RT. The latter 9 patients showed clinical
complete response and underwent endoscopic examination at regular
intervals to assess the outcome of RT including biopsy of the
tumour region for histopathological examination.
Immunohistochemistry
Archival paraffin blocks were cut into 5-μm
sections and analysed using immunohistochemistry. Staining for HA
was performed according to Hellström et al (14). In brief, endogenous peroxidase
activity was quenched by incubation in 3%
H2O2 in phosphate-buffered saline (PBS) for 5
min at room temperature. Non-specific binding was then blocked with
1% bovine serum albumin followed by incubation with 100 μl
biotinylated HA binding protein (HABP) diluted at a concentration
of 1:40 overnight at 4°C. The Vectastain Elite avidin-biotin
complex reagent was then used according to the manufacturer’s
instructions (Vector Laboratories, Burlingame, CA, USA) together
with the diaminobenzidine (DAB) substrate kit (Vector
Laboratories). Slides were counterstained with Mayer’s
haematoxylin. Control slides were incubated with 50 U/ml of
Streptomyces hyaluronidase (Sigma, St. Louis, MO, USA), which
specifically degrades hyaluronan, for 4 h at 37°C.
For the detection of EGFR, a monoclonal anti-EGFR
antibody (Dako, clone E30) diluted at 1:50 was used. This antibody
reacts with an external domain present in the transmembrane 170 kDa
protein of both the wildtype EGFR and the EGFRvIII variant. For the
detection of mast cells, an antibody recognising tryptase (Dako,
clone AA1) diluted at 1:100 was used. The Ventana ES autostainer
(Ventana, Tucson, AZ, USA) was used according to the manufacturer’s
recommendations.
Assessment
All histological samples were reviewed and the grade
of differentiation was evaluated by one of the authors (K.N.) who
was blinded to the clinical outcome. Two independent scorers
(co-authors E.L.J. and K.N.) assessed the slides stained for EGFR
and tryptase, and three independent scorers (co-authors E.L.J.,
K.N. and L.H.) assessed the slides stained for HA.
Staining results for HA were scored in
histologically normal epithelium, connective tissue and tumour
tissue. Scores representing the percentage of tissue positive for
HA were as follows: 0, no staining; 1, 1–25% of the tissue stained;
2, 26–50% stained; 3, 51–75% stained and 4, 76–100% stained.
Staining intensity was scored as 0, no staining; 1, weak staining;
2, moderate staining and 3, strong staining. Cellular localisation
of HA was further scored as pericellular (PC), intra- and
pericellular (IPC), or intracellular (IC), as adapted from Melrose
et al (15).
EGFR was scored according to Kersemaekers et
al (16) examining
histologically normal epithelium and tumour tissue. The percentage
of cells stained as well as the intensity of staining were scored
the same way as for HA. The density of tryptase-expressing cells in
histologically normal epithelium, connective tissue and tumour was
scored in the whole biopsies or surgical specimens and the mean
from two independent scorers was calculated.
Ethical considerations
The study was approved by the University of Umeå
Institutional Review Board (registration numbers 01-057 and
03-201).
Results
Fifteen of the 16 patients showed clinical complete
response, and the remaining patient showed partial response. The
overall 2-year survival was 81% (13 of 16 patients). The median
time between RT and surgery was 53 days (range, 40–369) with one
outlier who was not initially intended for surgery, while the
median time between RT and control biopsy was 75 days (range,
42–305) as the patients undergoing endoscopic examination were not
biopsied at fixed intervals, only when a suspected lesion was found
during endoscopy.
Immunohistochemistry
Pre-RT biopsies were available for all 16 patients,
and were stained for EGFR, HA and tryptase. Two biopsies were
excluded from staining with HA and EGFR, and one from staining with
tryptase due to a limited amount of tumour tissue for proper
evaluation. The amount of connective tissue was limited in many of
the pre-RT biopsies but there was sufficient in all samples for
evaluation. Seven surgical specimens and nine control biopsies
post-RT were available for EGFR, HA and tryptase analyses. A viable
tumour was only observed in one specimen following RT
treatment.
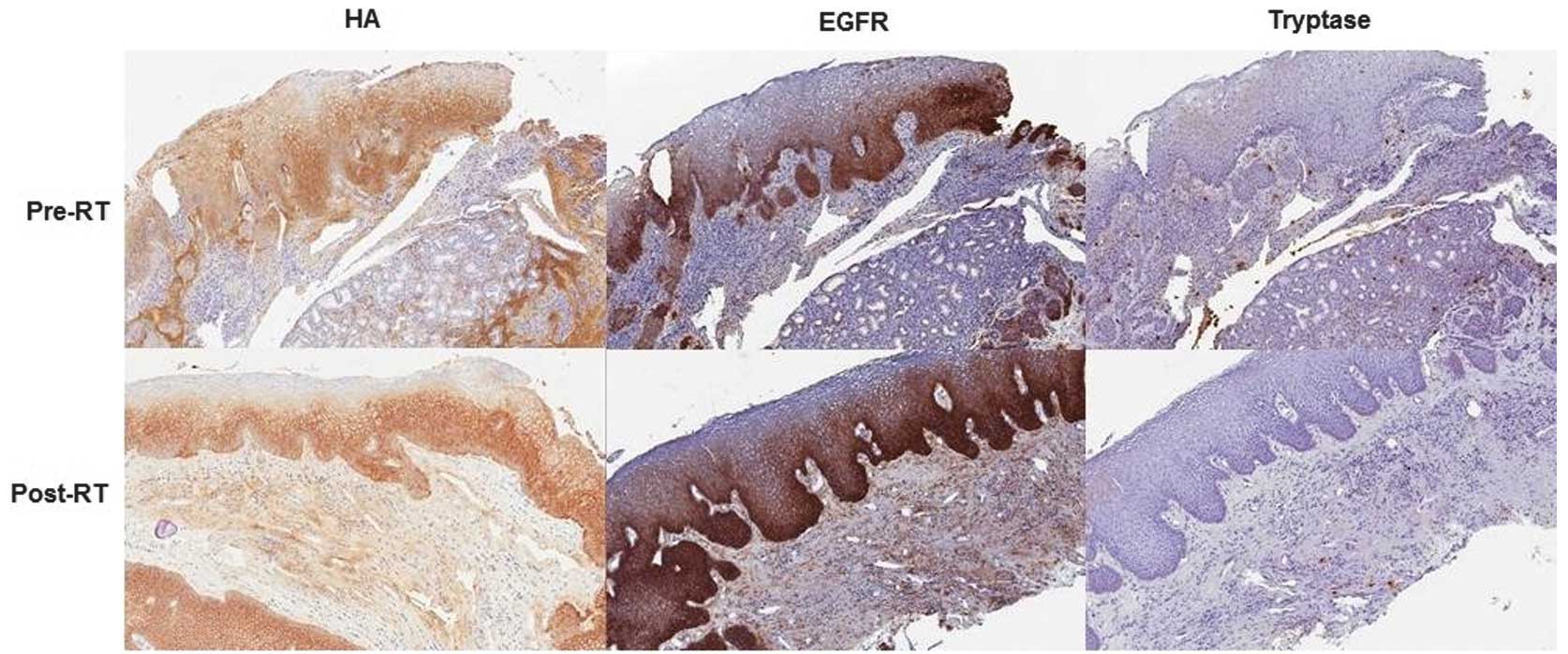
Expression of HA
In the 12 biopsies with histologically normal
epithelium, HA was mainly localised in the cell layers close to the
basal lamina, whereas the more suprabasal layers were negative. HA
staining was more intracellular (IC) in the basal and parabasal
layers and pericellular (PC) in the more superficial layers
(Fig. 1). No biopsies demonstrated
IC staining, whereas six biopsies demonstrated PC staining. All
tumours expressed HA with more intense staining observed in less
differentiated tumours; this was similar to HA staining in the
basal layers of histologically normal epithelium prior to RT. Two
biopsies with poorly differentiated SCC demonstrated IC staining,
whereas the remaining 14 tumours demonstrated IPC staining. The
localization of HA in histologically normal epithelium was not
significantly affected by RT (Fig.
1); the number of cases scored as PC or IPC, and the part of
epithelium stained were not affected by RT.
In the connective tissue, increased expression of HA
was observed post-RT, and the number of cases where the whole
connective tissue expressed HA also increased (Fig. 1). In the case with a remaining
viable tumour no change in HA expression was observed.
Expression of EGFR
Expression of EGFR in histologically normal
epithelium was similar to HA expression in the most basal cell
layers, and less intense in the more superficial and more
differentiated layers. EGFR also appeared to be intracellularly
located in the more basal layers of the epithelium. All tumours
also expressed EGFR, with more intense expression observed in less
differentiated tumours. Twelve of the 16 specimens demonstrated the
highest proportion of staining (76–100%), and staining was more
intense in tumours compared to histologically normal epithelium
(Table II). None of the biopsies
demonstrated EGFR staining in the connective tissue.
| Table II.Changes in the staining patterns
induced by radiotherapy (RT). |
Table II.
Changes in the staining patterns
induced by radiotherapy (RT).
| Pre-RT
| Post-RT
|
|---|
| Tissue | HA | EGFR | Tryptase | HA | EGFR | Tryptase |
|---|
| Histologically
normal epithelium | All samples
+ Basal or parabasal cell
layers | All samples
+ Basal or parabasal cell
layers | All samples
− | All samples
+ Basal or parabasal cell
layers | All samples
+ Basal or parabasal cell
layers | Few Basal or
parabasal cell layers |
| Connective
tissue | All samples
+ | All samples
− | All samples
+ | All samples
+ | All samples
− | All samples
+ |
| Tumour | All samples
+ Differentiation ↓ →
staining ↑ | All samples
+ Differentiation ↓ →
staining ↑ | All samples
+ | Remaining tumour
+ | Remaining tumour
+ | Remaining tumour
+ |
The percentage of EGFR-expressing cells in
histologically normal epithelium increased following RT. However,
RT did not induce EGFR expression in the connective tissue. In the
specimen containing a viable tumour following RT, neither the
intensity nor the percentage of EGFR-expressing cells changed but
still scored highest in their category.
Presence of mast cells
Mast cells could in general be observed throughout
the connective tissue, whereas almost no mast cells (mean count,
1.3) were observed in normal epithelium, and five samples were
completely devoid. The few mast cells present in the epithelium
pre-RT were located basally. Conversely, mast cells were observed
infiltrating tumours with a mean count of 2.0 tryptase-expressing
cells in pre-RT samples compared to 1.3 in normal epithelium.
The mean count of tryptase-expressing cells in
histologically normal epithelium increased from 1.3 to 2.0 post-RT,
whereas the mean count in the connective tissue decreased from 18.0
to 11.0 post-RT. The increases and decreases are shown in Table II. In the specimen with viable
tumour tissue following RT, tryptase-expressing cells decreased
from 10.2 to 3.3.
Discussion
Radiotherapy (RT) remains the main choice of
treatment for most patients with SCCHN, either as a single modality
treatment or combined with surgery. In order to improve treatment
there is a need to better understand how SCCHN and adjacent tissues
react to RT, and which side effects the treatment may have. In the
present study, the expression of HA and EGFR and the presence of
mast cells were studied in biopsies and surgical specimens before
and after RT. HA and EGFR showed similar expression patterns before
RT both in tumour and histologically normal epithelium. The less
differentiated the tumour was, the more intense the staining of
both HA and EGFR, a staining pattern similar to that observed in
the more basal layers of normal epithelium. This is in accordance
with previous results (7,17), and proposed to be due to the role of
HA in cell proliferation (18).
Earlier studies have shown that staining intensity correlates with
the expression of HA (19). Our
results confirm the earlier findings of cytoplasmic HA and EGFR,
although their role in the cytoplasm is still unclear (20). Membranous staining of EGFR has been
shown in clinical studies to correlate with cervical lymph node
metastases and survival (21,22).
The major ligand for EGFR, EGF, induces migration in connective
tissue-derived cells (23). It has
been shown that RT induces migration in SCCHN cells in
vitro, something that is inhibited when EGFR is blocked,
suggesting a connection between the mechanisms (24). In vitro studies have shown
expression of EGFR in connective tissue fibroblasts (25,26),
something we could not confirm in the present study either before
or after RT. The HA and EGFR-correlated receptor CD44 is also known
to be expressed by fibroblasts, and higher HA concentration in cell
cultures induces less cell proliferation but more migration in
fibroblasts (27).
HA is not, as was earlier believed, just a passive
molecule in the ECM but is capable of interacting with ECM
macromolecules and cell surface receptors, including CD44 (28). The complex molecular mechanism,
including the promotion of CD44/EGFR interaction and EGFR-mediated
oncogenic signalling (29), makes
it even more significant to analyse a connection between these two
markers. Both EGFR and HA overexpression in tumours has been linked
to poorer prognosis (30). Our
results, in accordance with previous results, showed stronger EGFR
staining in tumour tissue compared to normal epithelium (7). We also observed that EGFR staining
intensity in normal epithelium increased post-RT, although not to
the same level as in tumour tissue pre-RT. The only case with no
clinical response/partial response to RT showed the highest EGFR
score both before and after RT. This is in accordance with earlier
findings that high EGFR expression is correlated with a reduced
cellular response to RT (31). Due
to its role in cell signalling, EGFR is considered both a
predictive marker and a target for cancer therapy. EGFR inhibitors
such as C225 (Cetuximab™), a monoclonal antibody to the
extracellular domain, have shown radiosensitivity enhancement with
amplification of radiation-induced apoptosis in tumour specimens
(32). Irradiation is known to
induce structural alterations of HA such as degradation (33) and cause alteration of the physical
properties; however, to which extent, is yet unknown. HA fragments
are further released by most solid tumour cells and activate
inflammatory cell signalling, promoting tumour motility (34). In the present study, however, we did
not detect any changes in HA expression in normal epithelium or in
the one sample with viable tumour cells following RT. A decrease in
mast cells was observed post-RT in the connective tissue, but with
no correlation to the interval between termination of RT and the
time of biopsy or surgical procedure. A minor increase in mast
cells in the epithelium was found following RT, and the tumour
remaining following RT was also surrounded by an abundance of mast
cells, in accordance with animal studies demonstrating an influx of
mast cells during RT (33,34). There is an established correlation
between chronic inflammation and cancer (35) and mast cells are known to contribute
to pre-malignant progression (36–39).
It is known from animal models that mastocytosis in irradiated lung
tissue is followed by increased deposition of HA (40,41),
which is known to affect the lymphocytic response (42). Our finding that HA was expressed
more intensely in the connective tissue stroma post-RT could most
probably be viewed as a result of the fibrosis caused by
irradiation. This is supported by studies having suggested a
possible role for mast cells in fibrosis as a late effect of RT
(41).
In conclusion, we have shown RT to have an effect on
the expression of HA and EGFR as well as the presence of mast cells
in SCCHN tumours. These tumours are, however, known to be
heterogeneous (43); therefore, in
order to properly evaluate the effect of RT in SCCHN tumours, the
tumours should be divided based on subsites in future studies.
Acknowledgements
We gratefully thank Cathrine Johansson
and Astrid Höglund for their skilful technical assistance. This
study was supported by grants from the Lion’s Cancer Research
Foundation, Umeå University, and the Acta Otolaryngologica
Foundation.
References
|
1.
|
D MurdochStandard, and novel cytotoxic and
molecular-targeted, therapies for HNSCC: an evidence-based
reviewCurr Opin
Oncol19216221200710.1097/01.cco.0000264952.98166.9917414639
|
|
2.
|
ES KimM KiesRS HerbstNovel therapeutics
for head and neck cancerCurr Opin
Oncol14334342200210.1097/00001622-200205000-0001411981281
|
|
3.
|
BP TooleHyaluronan in morphogenesisSemin
Cell Dev Biol127987200110.1006/scdb.2000.0244
|
|
4.
|
P HeldinE KarousouB BernertH PorschK
NishitsukaSS SkandalisImportance of hyaluronan-CD44 interactions in
inflammation and tumorigenesisConnect Tissue
Res49215218200810.1080/0300820080214332318661346
|
|
5.
|
MA SimpsonJA WeigelPH WeigelSystemic
blockade of the hyaluronan receptor for endocytosis (HARE) prevents
lymph node metastasis of prostate cancerInt J
Cancer131E836E840201210.1002/ijc.2742722234863
|
|
6.
|
SJ WangLY BourguignonHyaluronan and the
interaction between CD44 and epidermal growth factor receptor in
oncogenic signaling and chemotherapy resistance in head and neck
cancerArch Otolaryngol Head Neck
Surg132771778200610.1001/archotol.132.7.77116847188
|
|
7.
|
T EkbergM NestorM EngströmH NordgrenK
WesterJ CarlssonM AnnikoExpression of EGFR, HER2, HER3, and HER4 in
metastatic squamous cell carcinomas of the oral cavity and base of
tongueInt J Oncol2611771185200515809707
|
|
8.
|
J MendelsohnJ BaselgaEpidermal growth
factor receptor targeting in cancerSemin
Oncol33369385200610.1053/j.seminoncol.2006.04.00316890793
|
|
9.
|
O RiestererL MilasKK AngCombining
molecular therapeutics with radiotherapy for head and neckJ Surg
Oncol97708711200810.1002/jso.2101118493923
|
|
10.
|
O DassonvilleJL FormentoM FrancoualA
RamaioliJ SantiniM SchneiderF DemardG MilanoExpression of epidermal
growth factor receptor and survival in upper aerodigestive tract
cancerJ Clin Oncol111873187819938410112
|
|
11.
|
LY BourguignonC EarleG WongCC SpevakK
KruegerStem cell marker (Nanog) and Stat-3 signaling promote
MicroRNA-21 expression and chemoresistance in
hyaluronan/CD44-activated head and neck squamous cell carcinoma
cellsOncogene31149160201210.1038/onc.2011.22221685938
|
|
12.
|
SR JunankarA EichtenA KramerKE de VisserLM
CoussensAnalysis of immune cell infiltrates during squamous
carcinoma developmentJ Investig Dermatol Symp
Proc113643200610.1038/sj.jidsymp.565002417069009
|
|
13.
|
AC PariziRL BarbosaJL PariziGA NaiA
comparison between the concentration of mast cells in squamous cell
carcinomas of the skin and oral cavityAn Bras
Dermatol85811818201021308304
|
|
14.
|
S HellströmA TengbladC JohanssonU HedlundE
AxelssonAn improved technique for hyaluronan histochemistry using
microwave irradiationHistochem J2267768219901706695
|
|
15.
|
J MelroseM TammiS SmithVisualisation of
hyaluronan and hyaluronan-binding proteins within ovine vertebral
cartilages using biotinylated aggrecan G1-link complex and
biotinylated hyaluronan oligosaccharidesHistochem Cell
Biol117327333200210.1007/s00418-002-0392-4
|
|
16.
|
AM KersemaekersGJ FleurenGG KenterLJ Van
den BroekSM UljeeJ HermansMJ Van de VijverOncogene alterations in
carcinomas of the uterine cervix: overexpressionClin Cancer
Res5577586199910100709
|
|
17.
|
C WangM TammiH GuoR TammiHyaluronan
distribution in the normal epithelium of esophagus, stomach, and
colon and their cancersAm J Pathol1481861186919968669472
|
|
18.
|
M InoueC KatakamiThe effect of hyaluronic
acid on corneal epithelial cell proliferationInvest Ophthalmol Vis
Sci342313231519938505213
|
|
19.
|
C LaurentG Johnson-WellsS HellströmA
Engström-LaurentAF WellsLocalization of hyaluronan in various
muscular tissuesCell Tissue
Res263201205199110.1007/BF003187612007249
|
|
20.
|
M EricksonR SternChain gangs: new aspects
of hyaluronan metabolismBiochem Res
Int2012893947201210.1155/2012/89394722216413
|
|
21.
|
A MahipalMJ McdonaldA WitkiewiczBI
CarrCell membrane and cytoplasmic epidermal growth factor receptor
expression in pancreatic ductal adenocarcinomaMed
Oncol29134139201110.1007/s12032-010-9802-y21264542
|
|
22.
|
MG NoordhuisJJ EijsinkKA Ten
HoorExpression of epidermal growth factor receptor (EGFR) and
activated EGFR predict poor response to (chemo)radiation and
survival in cervical cancerClin Cancer
Res1573897397200910.1158/1078-0432.CCR-09-1149
|
|
23.
|
Q KongRJ MajeskaM VazquezMigration of
connective tissue-derived cells is mediated by ultra-low
concentration gradient fields of EGFExp Cell
Res31714911502201110.1016/j.yexcr.2011.04.00321536028
|
|
24.
|
AC PickhardJ MargrafA KnopfInhibition of
radiation induced migration of human head and neck squamous cell
carcinoma cells by blocking of EGF receptor pathwaysBMC
Cancer11388201110.1186/1471-2407-11-38821896192
|
|
25.
|
MD HollenbergP CuatrecasasEpidermal growth
factor: receptors in human fibroblasts and modulation of action by
cholera toxinProc Natl Acad Sci
USA7029642968197310.1073/pnas.70.10.29644355377
|
|
26.
|
G CarpenterKJ LembachMM MorrisonS
CohenCharacterization of the binding of 125-I-labeled epidermal
growth factor to human fibroblastsJ Biol Chem250429743041975
|
|
27.
|
M YagiN SatoY MitsuiHyaluronan modulates
proliferation and migration of rabbit fibroblasts derived from
flexor tendon epitenon and endotenonJ Hand Surg
Am35791796201010.1016/j.jhsa.2010.02.01020438995
|
|
28.
|
CL ArteagaEpidermal growth factor receptor
dependence in human tumors: more than just
expression?Oncologist73139200210.1634/theoncologist.7-suppl_4-3112202786
|
|
29.
|
SK BlickLJ ScottCetuximab: a review of its
use in squamous cell carcinoma of the head and neck and metastatic
colorectal
cancerDrugs6725852607200710.2165/00003495-200767170-0000818034592
|
|
30.
|
K RopponenM TammiJ ParkkinenTumor
cell-associated hyaluronan as an unfavorable prognostic factor in
colorectal cancerCancer Res5834234719989443415
|
|
31.
|
U Kasten-PisulaJ SakerW EichelerCellular
and tumor radiosensitivity is correlated to epidermal growth factor
receptor protein expression level in tumors without EGFR
amplificationInt J Radiat Oncol Biol
Phys8011811188201110.1016/j.ijrobp.2011.02.043
|
|
32.
|
JA BonnerPM HarariJ GiraltRadiotherapy
plus cetuximab for locoregionally advanced head and neck cancer:
5-year survival data from a phase 3 randomised trial, and relation
between cetuximab-induced rash and survivalLancet
Oncol1121282010
|
|
33.
|
E DaarL KingA NisbetViscosity changes in
hyaluronic acid: irradiation and rheological studiesAppl Radiat
Isot68746750201010.1016/j.apradiso.2009.10.02219910202
|
|
34.
|
Y WuQ ZhaoC PengNeutrophils promote
motility of cancer cells via a hyaluronan-mediated TLR4/PI3K
activation loopJ Pathol225438447201110.1002/path.294721826665
|
|
35.
|
F BalkwillA MantovaniCancer and
inflammation: implications for pharmacology and therapeuticsClin
Pharmacol Ther87401406201010.1038/clpt.2009.31220200512
|
|
36.
|
LM CoussensWW RaymondG BergersInflammatory
mast cells up-regulate angiogenesis during squamous epithelial
carcinogenesisGenes
Dev1313821397199910.1101/gad.13.11.138210364156
|
|
37.
|
D RibattiMG EnnasA VaccaTumor vascularity
and tryptase-positive mast cells correlate with a poor prognosis in
melanomaEur J Clin
Invest33420425200310.1046/j.1365-2362.2003.01152.x12760367
|
|
38.
|
M SawatsubashiT YamadaN
FukushimaAssociation of vascular endothelial growth factor and mast
cells with angiogenesis in laryngeal squamous cell
carcinomaVirchows
Arch436243248200010.1007/s00428005003710782883
|
|
39.
|
A ImadaN ShijuboH KojimaMast cells
correlate with angiogenesis and poor outcome in stage I lung
adenocarcinomaEur Respir
J1510871093200010.1034/j.1399-3003.2000.01517.x10885428
|
|
40.
|
K NilssonR HenrikssonS HellströmHyaluronan
reflects the pre-fibrotic inflammation in irradiated rat lung:
concomitant analysis of parenchymal tissues and bronchoalveolar
lavageInt J Radiat Biol58519530199010.1080/09553009014551861
|
|
41.
|
K NilssonL BjermerS HellströmA mast cell
secretagogue, compound 48/80, prevents the accumulation of
hyaluronan in lung tissue injured by ionizing irradiationAm J
Respir Cell Mol Biol2199205199010.1165/ajrcmb/2.2.199
|
|
42.
|
PL BollykyBA FalkRP WuIntact extracellular
matrix and the maintenance of immune tolerance: high molecular
weight hyaluronan promotes persistence of induced CD4+CD25+
regulatory T cellsJ Leukoc Biol86567572200919401397
|
|
43.
|
L BoldrupPJ CoatesG LaurellK
NylanderDifferences in p63 expression in SCCHN tumours of different
sub-sites within the oral cavityOral
Oncol47861865201110.1016/j.oraloncology.2011.07.00221802344
|