Introduction
Ameloblastic carcinoma is a rare odontogenic
carcinoma. Although ameloblastomas are well studied and documented
(over 3,600 cases of ameloblastomas have been described in the
literature), little is known about their malignant features, as
fewer than 60 cases of ameloblastic carcinoma have been reported
(1–4).
Malignant variants of ameloblastoma include
metastasizing ameloblastoma, which microscopically appears benign
but has metastasized, and ameloblastic carcinoma, which exhibits
malignant histopathological features. Ameloblastic carcinoma may be
classified into two types: a primary odontogenic malignancy and a
secondary type resulting from the malignant transformation of
ameloblastoma. Most secondary ameloblastic carcinomas result from
the malignant transformation of a primary lesion following repeated
postsurgical recurrences. Therefore, it is rare to find an
untreated secondary type presenting the histological features of
malignant transformation from an earlier benign lesion (5,6).
In order to provide a better understanding of the
many terms for ameloblastic malignant lesions, Hall et al
(7) presented the Elzay
classification (1982) of malignant odontogenic tumors, which has
been accepted by many pathologists, and its nomenclature remains in
use today. The term malignant ameloblastoma was used to describe a
tumor that is a histologically typical or classic ameloblastoma,
but which metastasizes. The ameloblastic carcinoma is characterized
as a tumor that has certain features of ameloblastoma but
demonstrates traditional histological features of malignancy and
acts much more aggressively than ameloblastoma.
In the 2005 World Health Organization (WHO)
histological classification of odontogenic tumors, ameloblastic
carcinoma was included as an odontogenic carcinoma with
histological features of ameloblastoma, but with cytological atypia
with or without metastasis (8).
Kruse et al (9) recommended a modified classification in
which a primary ameloblastoma is followed by secondary metastasis
with histopathological features of malignancy and without evidence
of malignancy in the primary location.
This carcinoma occurs in a wide range of age groups,
but the mean age is 30.1 years, as in ameloblastomas. The most
common site of occurrence is the posterior portion of the mandible.
It is very rare in the maxillary region. There is no apparent
gender predilection, but some authors have described predominance
in males. The most common indication described has been swelling,
although others include associated pain, rapid growth, trismus and
dysphonia (1,2,4,7,10).
The radiographic appearance of the ameloblastic
carcinomas described in the literature is generally consistent with
that of ameloblastomas, except perhaps for the presence of some
focal radiopacities, apparently reflecting dystrophic
calcifications. Signs of osseous destruction are found in
ameloblastic carcinomas as well as in ameloblastomas. These lytic
phenomena may be assessed by CT and MRI imaging (5).
The most common site of metastasis is the lung, but
brain or bony locations have also been reported. These tumors are
prone to numerous recurrences that justify a long follow-up
(5).
Being a rare disease, there are no treatment
guidelines; however, the standard treatment is usually a complete
surgical resection with or without radiotherapy (2,11).
The early, aggressive and complete removal of the
tumor appears to offer the best chance of survival (7). Some authors (1,2)
recommend surgical treatment usually involving maxillary resection
with 2 to 3 cm bony margins and consideration of contiguous neck
dissection, both prophylactic and therapeutic.
This study aims to present the clinical features and
treatment of a maxillary ameloblastic carcinoma case. The study was
approved by Ethics Committee of Univag Academic Center, Mato
Grosso, Brazil. Informed consent was obtained from the patient.
Case report
A 59-year-old males was examined by a dental surgeon
in the city of Tangará da Serra, Mato Grosso, Brazil. The patient
reported to have been experiencing bone pain and swelling for two
months. The surgeon identified the injured area and performed a
curettage. After 2 months, the pain reoccurred, and the patient was
again treated surgically, but gained no relief. The swelling
gradually increased, reaching a size which caused the patient
difficulty in eating, speaking and swallowing for 2–3 months prior
to him seeking assistance. A systems review was inconclusive. The
patient was not a user of tobacco or alcohol.
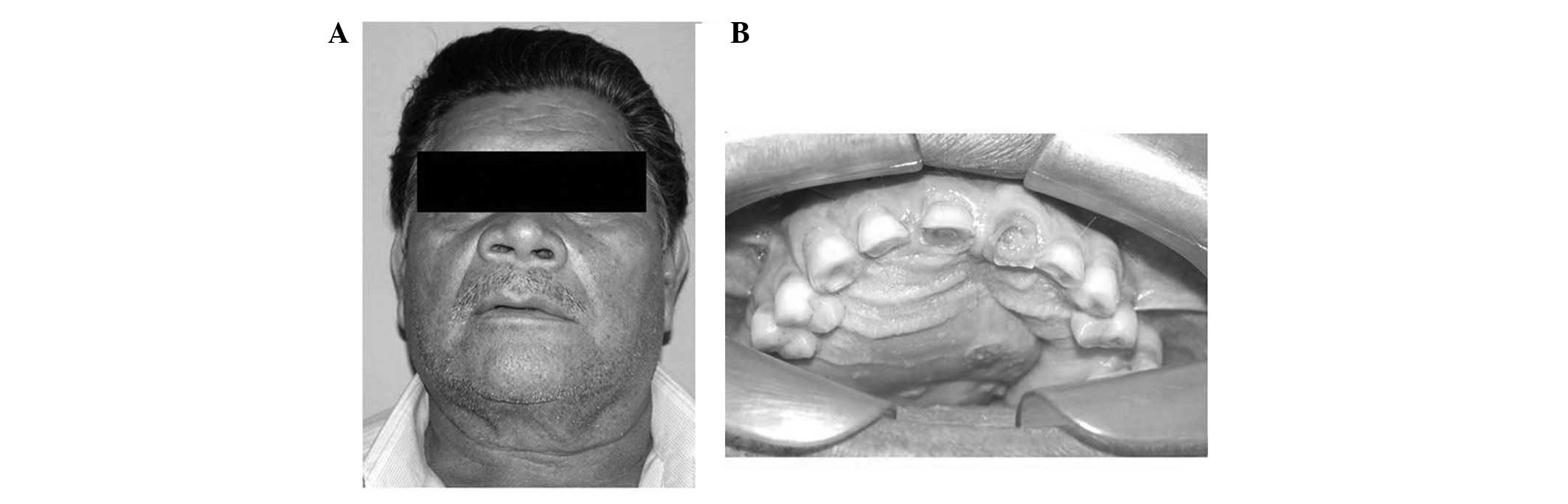
Extraoral examination revealed facial asymmetry,
increased right-side volume, alar nose elevation and erasing of the
nasolabial furrow (Fig. 1A). The
overlying skin was smooth and normal. No ulceration was observed.
The facial lymph nodes were nonpalpable. The results of the rest of
the head and neck examination were normal.
In the intraoral physical examination, there was an
increase in volume in the hard palate (Fig. 1B). The central and upper right
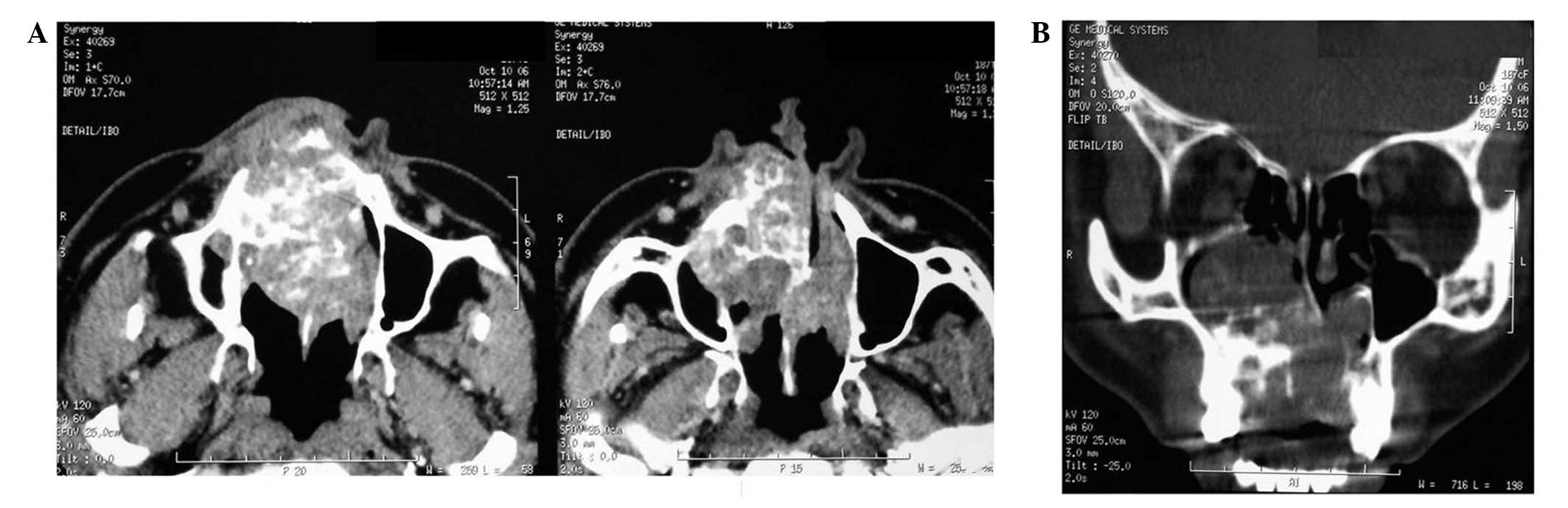
lateral incisors presented mobility. A panoramic view showed a
multilocular radiolucent lesion mainly in the right side of the
maxilla, extending across the midline to involve the left side.
Axial slice computed tomography (CT) scans were carried out,
revealing an oval corticated lucency occupying a large portion of
the right maxillary sinus (Fig. 2A)
and expansion and destruction of the alveolar cortical plate,
involving the nasal cavity and the eyeball. The coronal slice
showed a large, expansile, multilobulated cystic lesion of the
maxilla (Fig. 2B). Based on these
findings, a diagnosis of ameloblastoma involving the right maxilla
was made. Fine-needle aspiration of the mass proved inconclusive,
and incisional biopsy was also performed. A partial area was
surgically excised under local anesthesia and the material was sent
to the laboratory of oral pathology.
The histological sections revealed a fragmented
odontogenic tumor of epithelial origin, consisting of solid
parenchyma and also revealed basal cells resembling ameloblasts,
occasionally arranged in palisades. The most central cells were
arranged more loosely resembling the stellate reticulum of the
enamel organ. Metaplasia was also noted. The stroma consisted of
loose fibrous connective tissue (Fig.
3A). The odontogenic parenchyma was composed of epithelial
cells showing intense cellular pleomorphism, numerous
hyper-chromatic cells, loss of the nuclear/nucleolus and nucleus/
cytoplasm and areas of necrosis (Fig.
3B). Certain parts of the architecture resembled that of an
ameloblastoma; however, the cytology of other areas confirmed the
diagnosis of ameloblastic carcinoma of the maxilla.
The patient was scheduled for definitive surgery,
including a right maxillectomy and radiotherapy. The patient was
followed up every 3 months. After 2 years follow-up, there were no
clinical or radiological signs of recurrence; however, the patient
is currently suffering from discomfort when eating and talking due
to bucosinusal communication. Treatment is in the prosthetic
rehabilitative phase.
Discussion
Ameloblastic carcinoma is an extremely rare,
aggressive malignant epithelial odontogenic tumor with a poor
prognosis. Two thirds of these tumors arise from the mandible while
one third originate in the maxilla. The most common symptom is a
rapidly progressing, painful swelling (4,5,11).
Clinically, these carcinomas are more aggressive
than most typical ameloblastomas. Perforation of the cortical
plate, extension into the surrounding soft tissue and numerous
recurrent lesions and metastasis, usually to cervical lymph nodes,
are associated with ameloblastic carcinomas (5). The facial lymph nodes in this case
were nonpalpable.
The lung is the most common area of distant
metastasis, but metastasis to the skull and lymph nodes has also
been described. In the present case, the patient had no metastasis
at the time of diagnosis (12);
however, metastases may also occur following treatment, emphasizing
the significance of clinical and radiographical follow-up (5). A systems review was inconclusive.
In 2007, 37 cases of ameloblastic carcinoma in
patients ranging in age from 15 to 84 years were reviewed (13). The male to female ratio was 5:3,
with the majority of cases occurring in patients aged 50–60. The
present case involved a 59-year-old male. In the 2007 study
(13), 12 of the 37 tumors were
located in the maxilla. Expansion or a hard mass was the main
complaint, followed by pain or discomfort. Others signs and
symptoms included trismus, dysphonia and paresthesia. The reported
cases of spindle-cell ameloblastic carcinoma occurred more often in
the mandible than in the maxilla, at a ratio of 3:1. In the present
case, the lesion was present in the right-side maxilla, extending
across to the left side. The patient in this case presented with
swelling in the right maxilla, facial asymmetry, associated pain,
rapid growth, dysphagia and dysphonia.
The radiographical features of ameloblastic
carcinoma are similar to ameloblastomas. In the majority of cases,
a radiolucent intraosseous lesion is revealed (1,5), as
was demonstrated in the present case. In our case study, the
radiographical appearance of the lesion was consistent with that of
an ameloblastoma except for the presence of some focal
radiopacities, apparently reflecting the dystrophic calcifications
revealed by CT.
An additional consideration in the differential
diagnosis is a squamous cell carcinoma arising in the lining of an
odontogenic cyst. Histologically, this lesion tends to more closely
resemble oral squamous cell carcinoma than what we have described
for ameloblastic carcinoma. However, it is important to point out
that ameloblastic carcinoma may arise from the cystic lining. The
squamous odontogenic tumor may also be mistaken for ameloblastic
carcinoma. It is composed of islands of squamous epithelium that
lack stellate reticulum-like zones and peripheral palisading. In
addition, microcystic changes and dystrophic calcifications are
occasionally observed in this lesion. However, the epithelium of
the squamous odontogenic tumor lacks any cytologic evidence of
malignant disease (14). Thus, the
term ameloblastic carcinoma may be applied to our case, which
showed focal histological evidence of malignant disease including
cytologic atypia and mitoses along with the indisputable features
of classic ameloblastoma.
It is generally accepted that maxillary
ameloblastomas should be treated as radically as possible due to
the spongy maxillary bone architecture (9); however, controversy still exists
regarding the treatment of ameloblastic carcinoma. As ameloblastic
carcinomas are rare, there is no consensus on their treatment.
Certain authors have suggested surgery plus radiotherapy, while
others doubt the effectiveness of this combination. There are few
reports on chemotherapy regimens for ameloblastic carcinoma
(1). Preoperative radiotherapy has
been suggested to decrease the tumor size and may be used to treat
some rapidly growing tumors prior to radical surgery. The role of
chemotherapy has not yet been proven (11). In the present case, treatment
consisted of surgical resection and adjuvant radiation.
The prognosis is dominated by the possibility of
local recurrences, even after a long relapse, and distant
metastases. Metastases generally occur in the lung but may also
occur in the bone and the brain. A systematic assessment of the
chest by periodic imaging is recommended (3).
Reconstruction of the post-resection defect should
proceed as normal following any head or neck carcinoma resection;
however, sufficient time should be allotted prior to reconstruction
due to potential tumor recurrence (4).
Microscopically, the benign and malignant
ameloblastoma are very similar, often only differentiated correctly
when a contained metastasis in the lung is revealed by
histopathological examination of images. Ameloblastic carcinoma
presents with atypical mitotic figures, intense cellular
pleomorphism among other areas of necrosis, which are not usually
observed in ameloblastoma and malignant ameloblastoma, and features
which enable differentiation and a more precise diagnosis, as was
observed in the present case.
We have had no report of metastasis in the case
presented in this study, although we must keep in mind the
possibility that this may still occur. It is essential that, in the
future, these lesions are accurately identified and followed up so
that their natural history and prognosis may be further
defined.
In conclusion, ameloblastic carcinoma is a very rare
malignant odontogenic tumor with characteristic histopathological
and clinical features, which requires aggressive surgical treatment
and surveillance.
Diagnosis at an early stage and close periodical
screening for metastasis are necessary to improve patient
prognosis.
In addition to local long-term control, specific
attention should be paid to potential pulmonary involvement.
References
|
1.
|
GA NaiRN GrossoFine-needle aspiration
biopsy of ameloblastic carcinoma of the mandible: a case reportBraz
Dent J22254257201110.1590/S0103-6440201100030001321915525
|
|
2.
|
AD JensenS EckerM EllerbrockA NikoghosyanJ
DebusMW MünterCarbon ion therapy for ameloblastic carcinomaRadiat
Oncol615201110.1186/1748-717X-6-1321294917
|
|
3.
|
H MatsuzakiN KataseM HaraJ AsaumiY YanagiT
UnetsuboM HisatomiH KonouchiH NagatsukaAmeloblastic carcinoma: a
case report with radiological features of computed tomography and
magnetic resonance imaging and positron emission tomographyOral
Surg Oral Med Oral Pathol Oral Radiol
Endod1124047201110.1016/j.tripleo.2011.01.023
|
|
4.
|
S PundirS SaxenaV RathodP
AggrawalAmeloblastic carcinoma: Secondary dedifferentiated
carcinoma of the mandible - Report of a rare entity with a brief
reviewJ Oral Maxillofac
Pathol15201204201110.4103/0973-029X.8450122529581
|
|
5.
|
A BenlyazidM Lacroix-TrikiR AzizaA
Gomez-BrouchetM GuichardJ SariniAmeloblastic carcinoma of the
maxilla: case report and review of the literatureOral Surg Oral Med
Oral Pathol Oral Radiol
Endod1041724200710.1016/j.tripleo.2007.05.026
|
|
6.
|
K KarakidaT AokiH SakamotoM TakahashiT
AkamatsuG OguraY SekidoY OtaAmeloblastic carcinoma, secondary type:
a case reportOral Surg Oral Med Oral Pathol Oral Radiol
Endod1103337201010.1016/j.tripleo.2010.08.018
|
|
7.
|
JM HallDR WeathersKK UnniAmeloblastic
carcinoma: An analysis of 14 casesOral Surg Oral Med Oral Pathol
Oral Radiol
Endod103799807200710.1016/j.tripleo.2006.11.04817448710
|
|
8.
|
C JindalS PalaskarH KaurM
ShankariLow-grade spindle-cell ameloblastic carcinoma: report of an
unusual case with immunohistochemical findings and review of the
literatureCurr Oncol175257201010.3747/co.v17i5.58020975879
|
|
9.
|
ALD KruseRA ZwahlenKW GrätzNew
classification of maxillary ameloblastic carcinoma based on an
evidence-based literature review over the last 60 yearsHead Neck
Oncol131200919674470
|
|
10.
|
A SuomalainenJ HietanenS RobinsonJS
PeltolaAmeloblastic carcinoma of the mandible resembling
odontogenic cyst in a panoramic radiographOral Surg Oral Med Oral
Pathol Oral Radiol
Endod101638642200610.1016/j.tripleo.2005.07.03316632277
|
|
11.
|
S OzlugedikM OzcanO BasturkO DerenE
KaptanogluG AdanaliA UnalAmeloblastic carcinoma arising from
anterior skull baseSkull
Base15269272200510.1055/s-2005-91862116648889
|
|
12.
|
Y AbikoH NagayasuM TakeshimaM YamazakiM
NishimuraK KusanoH KitajoM SaitohT KawakamiI ChibaT
KakuAmeloblastic carcinoma ex ameloblastoma: report of a
case-possible involvement of CpG island hypermethylation of the p16
gene in malignant transformationOral Surg Oral Med Oral Pathol Oral
Radiol Endod1037276200710.1016/j.tripleo.2006.01.02117178497
|
|
13.
|
S AkrishA BuchnerY ShoshaniM VeredD
DayanAmeloblastic carcinoma: report of a new case, literature
review and comparison to ameloblastomaJ Oral Maxillofac
Surg65777783200610.1016/j.joms.2005.11.11617368379
|
|
14.
|
SL AvonJ McCombC CrokieAmeloblastic
carcinoma: case report and literature reviewJ Can Dent
Assoc69573576200314653932
|