Introduction
The occurrence of unilateral multiple breast cancer
is considered to be derived from multicentric and multifocal
tumorigenesis. One theory is that the isolated tumors independently
develop from distinctly separate origins and a further theory
suggests that the secondary tumor is formed through an intraductal
spread of the original tumor. The majority of unilateral multiple
breast cancer cases are thought to involve a multifocal tumor
derived from an intraductal spread (1).
We, herein, report the case of a post-menopausal
female with a unilateral multicentric cancer of the breast
containing two isolated tumors with different histopathologic
types.
Case report
A post-menopausal 78-year-old female presented with
a disintegrated tumor in the left breast that had been untreated
for one year despite her awareness of the tumor. Physical
examination revealed a solid tumor in the internal upper area and a
disintegrated tumor in the external lower area of the left
breast.
While there was an increase in the white blood cell
count in the peripheral blood (18,000/mm2) and serum
level of C-reactive protein (16.2 mg/dl) derived from an
inflammatory response to the disintegrated tumor of the breast,
there was no increase in the levels of carcinoembryonic antigen
(CEA) and cancer antigen 15-3 (CA15-3) in the sera.
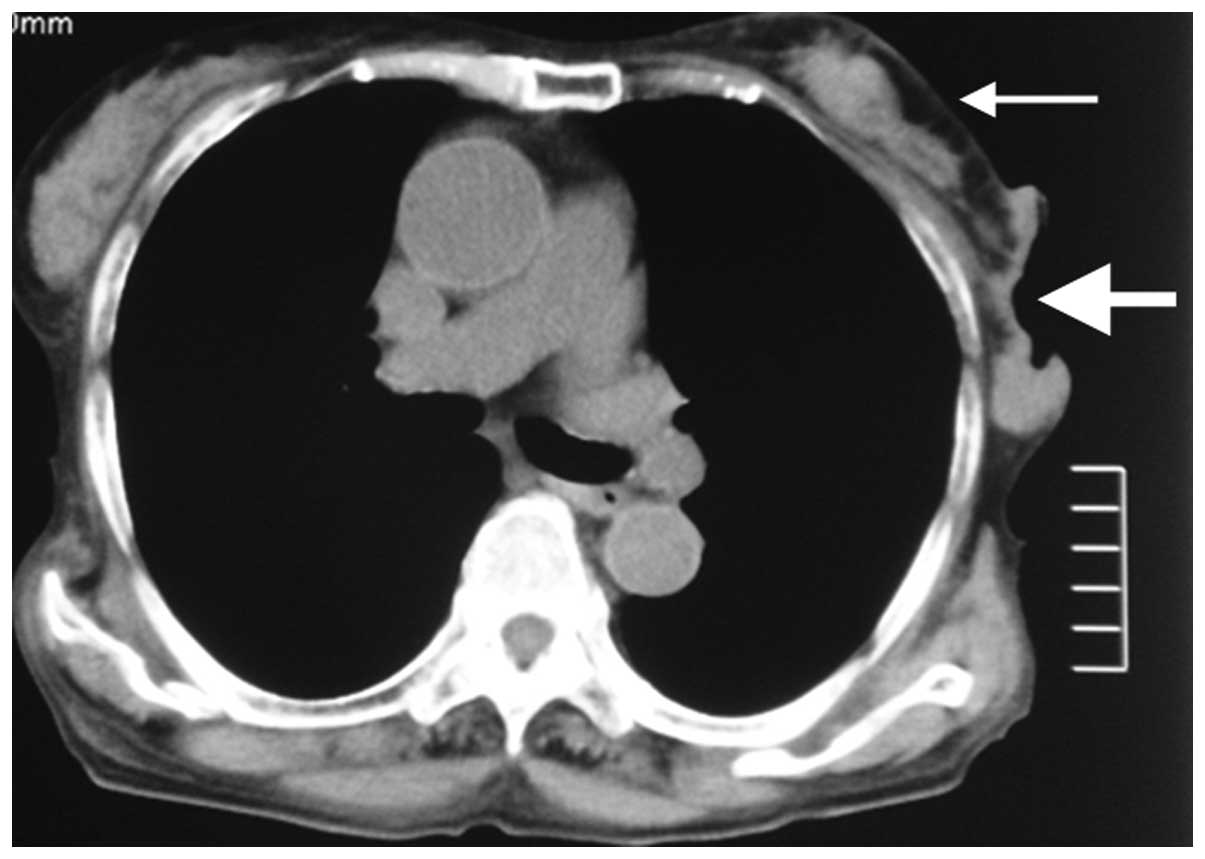
Preoperative computed tomography demonstrated two
isolated tumors in the left breast (Fig. 1).
The disintegrated tumor was necrotized, emitting a
strongly unpleasant smell and bleeding; however, the decision was
made to immediately perform a mastectomy.
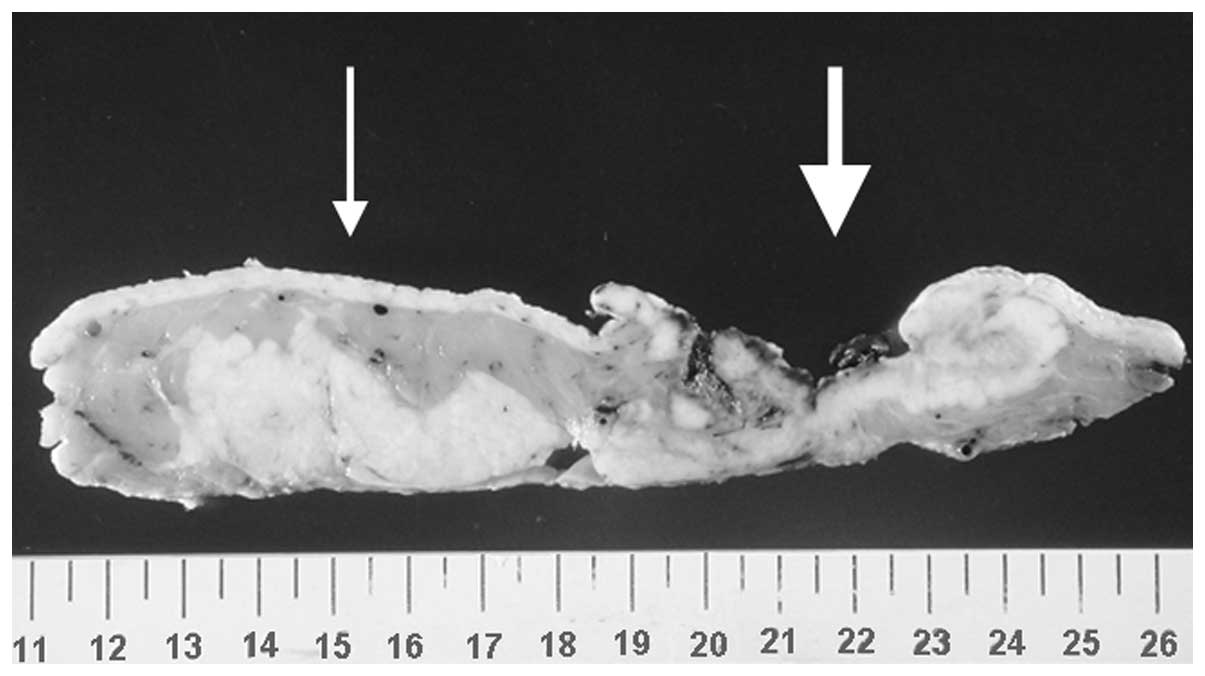
Macroscopic findings of the specimen revealed two
independent tumors measuring 3.5 cm and 5.0 cm in length,
respectively, that were distinctly separated (Fig. 2).
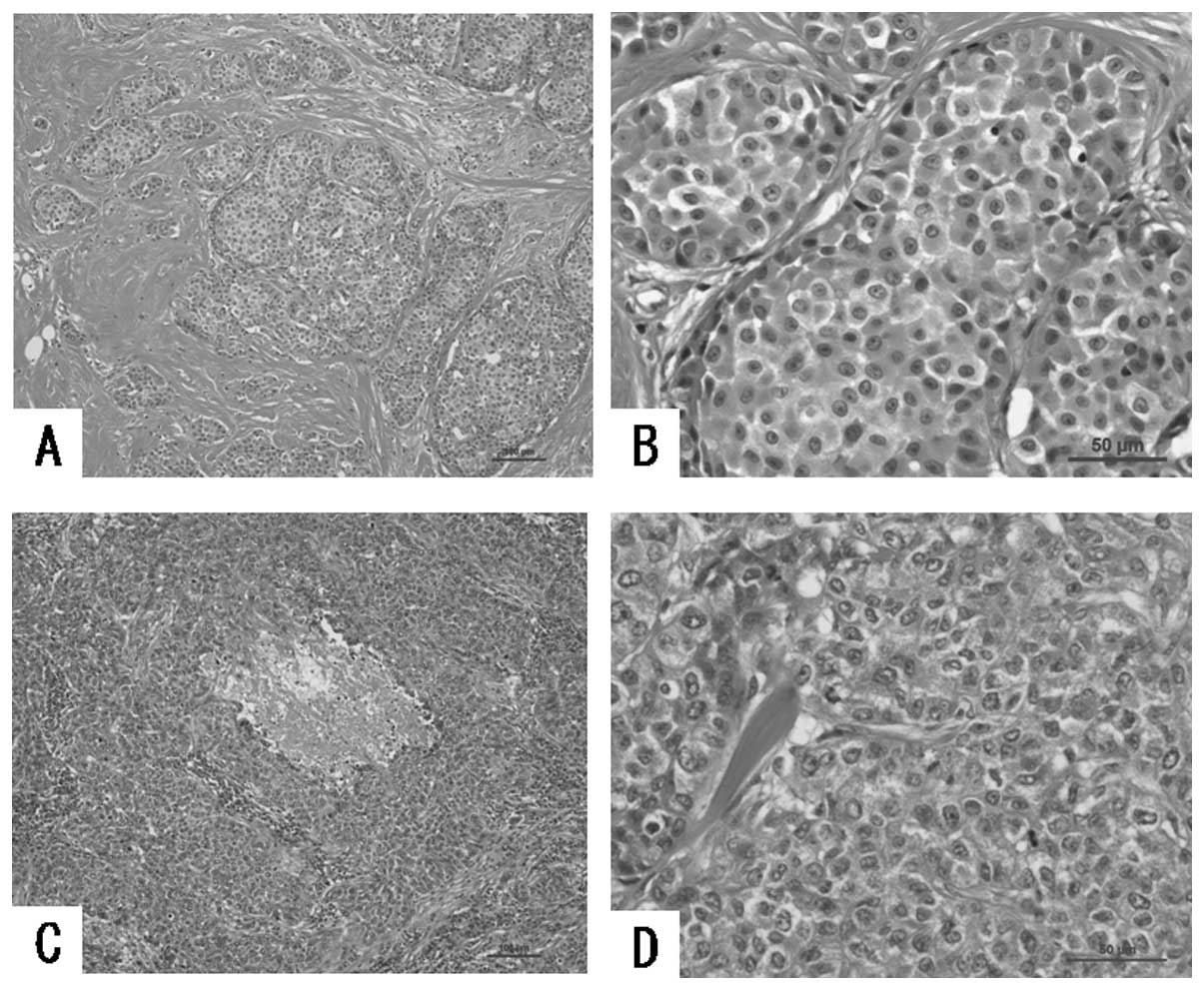
Histopathological examination revealed a tumor in
the internal upper area and a disintegrated tumor in the external
lower area of the left breast containing the features of invasive
lobular carcinoma and papillo-tubular carcinoma, respectively
(Fig. 3). Furthermore, an
immunohistochemical examination revealed that the former tumor had
positive expression of the estrogen receptor (ER) and progesterone
receptor (PgR), but not the HER2 receptor; however, the latter,
which comprised the main tumor, expressed none of these receptors
(triple negative cancer).
Following mastectomy with an axillary lymph node
dissection, radiotherapy (total dose of 50 Gy) and adjuvant
chemotherapy, consisting of 4 cycles of FEC (5-fluorouracil 500
mg/m2, epirubicin 100 mg/m2 and
cyclophosphamide 500 mg/m2) every 3 weeks followed by 4
cycles of DOC (docetaxel 75 mg/m2) every 3 weeks, were
performed. The patient was subsequently treated with an oral intake
of tamoxifen in our outpatient clinic and to date, has been in a
satisfactory condition without any evidence of tumor
recurrence.
The study was approved by the ethics committee of
Fukuoka Higashi Medical Center, Koga, Japan. Informed consent was
obtained from the patient.
Discussion
The incidence of unilateral multiple breast cancer
has been reported to account for approximately 5% of all breast
cancers (1). These cases may
contain multiple tumors derived from multifocal cancers primarily
caused by intraductal spread of the tumor.
According to the criteria presented by Wakabayashi
et al(2), unilateral
multifocal breast cancer is defined as a histopathologically
discontinuous cancer not derived from intraductal spread,
containing at least one tumor-free section separating the tumors
and involving a large primary tumor and other small secondary
tumors.
While the tumors in the present study had different
histological types, it was evident that the tumors had been formed
by multicentric tumorigenesis.
Unilateral multifocal breast cancer is usually
diagnosed following a detailed histological examination of the
dissected specimens. Computed tomography (CT) (3) and magnetic resonance imaging (MRI)
(4) have been reported to reveal an
unilateral multiple breast cancer prior to surgery, as was
demonstrated in our patient, for whom preoperative CT revealed two
distinct tumors in the left breast.
In the criteria suggested by Wakabayashi et
al(2), there was no reference
to the size of the secondary tumors. In the present case, the
secondary tumor diagnosed as invasive lobular carcinoma was found
to be comparatively smaller than the primary tumor, and its
coexistence could only be found by a preoperative physical
palpation. The tumor diagnosed as papillo-tubular carcinoma was
found to be larger; possibly due to its earlier development.
However, although a tumor diagnosed as invasive lobular carcinoma
may appear first, a secondary tumor diagnosed as papillo-tubular
carcinoma may possess an aggressive behavior caused by the
characteristics of triple negative expression (negative for ER, PgR
and HER2), causing it to grow rapidly and surpass the other tumor
in size.
While the occurrence of multifocal breast cancers
has been reported to be more frequent among invasive lobular
carcinomas (5), physicians should
be cautious not to overlook the secondary tumor in cases of
invasive lobular carcinoma of the breast. Moreover, the proportion
of tumor recurrence in the abdominal organs including the
gastrointestinal tract, ovary and peritoneum has been revealed to
be higher in patients who have invasive lobular carcinoma (6,7), and
it is well known that tumor recurrence is much more frequent in
cases of triple negative breast cancer (8). Therefore, a meticulous follow-up may
be mandatory.
In the present study, following mastectomy with an
axillary lymph node dissection, radiotherapy and adjuvant
chemotherapy, the patient was administered an oral intake of
tamoxifen. These treatments may be effective in preventing tumor
recurrence.
References
|
1
|
Koida T, Kimura M, Yanagita Y, et al:
Clinicopathological study of unilateral multiple breast cancer.
Breast Cancer. 8:202–205. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wakabayashi T, Tsuchiya SI and Asano G:
Unilateral multi-centric breast carcinoma studied by whole mammary
gland serial sectioning. Breast Cancer. 2:91–98. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Taira N, Ohsumi S, Takabatake D, et al:
Contrast-enhanced CT evaluation of clinically and mammographically
occult multiple breast tumors in women with unilateral early breast
cancer. Jpn J Clin Oncol. 38:419–425. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sardanelli F, Giuseppetti GM, Panizza P,
et al: Italian Trial for Breast MR in Multifocal/Multicentric
Cancer. Sensitivity of MRI versus mammography for detecting foci of
multifocal, multicentric breast cancer in fatty and dense breasts
using the whole-breast pathologic examination as a gold standard.
Am J Roentgenol. 183:1149–1157. 2004. View Article : Google Scholar
|
|
5
|
Dedes KJ and Fink D: Clinical presentation
and surgical management of invasive lobular carcinoma of the
breast. Breast Dis. 30:31–37. 2009.PubMed/NCBI
|
|
6
|
Arpino G, Bardou VJ, Clark GM, et al:
Infiltrating lobular carcinoma of the breast: tumor characteristics
and clinical outcome. Breast Cancer Res. 6:149–156. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
McLemore EC, Pockaj BA, Reynolds C, et al:
Breast cancer: presentation and intervention in women with
gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol.
12:886–894. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nozoe T, Mori E, Iguchi T, et al:
Immunohistochemical expression of epidermal growth factor receptor
in breast cancer. Breast Cancer. 18:37–41. 2011. View Article : Google Scholar : PubMed/NCBI
|