Introduction
β-adrenergic receptors (β-ARs) are G protein-coupled
molecules that activate the protein kinase A pathway by
accumulation of the secondary messenger cAMP. This signal
transduction pathway appears to increase VEGF gene expression,
resulting in enhanced tumor vascularization and more aggressive
growth. Although within a tumor mass β-ARs are mainly localized on
intra-tumor vessel walls, studies in cell lines show that they are
also expressed on the surface of tumor cells (1).
In vitro and in vivo studies have
revealed that adrenergic neurotransmitters are involved in the
progression and dissemination of several tumor types, including
breast (2), colon (3), prostate (4), pancreatic (5) and ovarian carcinomas (6) and melanoma (7). Increased angiogenesis may result from
catecholamine-induced VEGF production by tumor cells (8). A recent study revealed that
β-adrenergic signaling may also play a role in the growth and
metastatic dissemination in an orthotopic mouse model of breast
cancer (9).
Several epidemiological studies have documented a
significantly lower risk of cancer development or recurrence in
individuals treated with β-blocking agents (10–17).
Propranolol significantly inhibits norepinephrine-induced VEGF and
hypoxia-inducible factor (HIF)-1α expression and angiogenesis in
human prostate, breast and hepatocellular cancer cells (18).
In malignant brain tumors, such as medulloblastoma,
glioblastoma and anaplastic ependymoma, hypervascularization may
result also from an enhancement of the β-adrenergic signaling
pathway. Data on β-AR expression in brain tumors are conflicting
(19–25). To address this issue we examined the
expression of β-ARs in pediatric brain tumors.
Materials and methods
Patient population and data
collection
The population of this study was a subset of
pediatric brain tumor patients diagnosed and treated at Meyer
Children’s Hospital between 2004 and 2010. The study was approved
by the Hospital Ethical Committee and informed consent was obtained
from the parents/legal guardians of all patients.
We studied 12 primary malignant brain tumors of the
following types: medulloblastoma (WHO grade IV, n=5), anaplastic
ependymoma (WHO grade III, n=5) and glioblastoma multiforme (WHO
grade IV, n=2).
Mean overall survival (OS) for the twelve patients
was 35.5 months (range, 10–55 months); at the end of the study
seven (58%) were alive while 5 had succumbed to progressive
disease. Eight patients were treated with complete/gross tumor
resection followed by chemotherapy and/or radiotherapy, while the
remaining 4 medulloblastoma patients received high-dose,
myeloablative chemotherapy with autologous stem cell rescue. Ten of
the 12 patients received radiotherapy.
The main clinical characteristics of the patients
are summarized in Table I.
 | Table IClinical characteristics of primary
pediatric brain tumors. |
Table I
Clinical characteristics of primary
pediatric brain tumors.
| ID/gender | Age | Histology | Surgery | CT (BMT) | RT | OS (months) | Status |
|---|
| MB1/M | 2 months | Medulloblastoma | GTR | + (+BMT) | + | 10 | DOD |
| MB2/F | 3 months | Medulloblastoma | GTR | + (+BMT) | − | 49 | NED |
| MB3/M | 3 years | Medulloblastoma | GTR | + (+BMT) | + | 54 | NED |
| MB4/F | 8 years | Medulloblastoma | GTR | + | + | 41 | NED |
| MB5/F | 1 years | Medulloblastoma | GTR | + (+BMT) | − | 35 | NED |
| EP1/F | 9 years | Anaplastic
ependymoma | PTR | + | + | 44 | DOD |
| EP2/F | 3 years | Anaplastic
ependymoma | GTR | + | + | 55 | NED |
| EP3/F | 10 years | Anaplastic
ependymoma | GTR | + | + | 43 | NED |
| EP4/M | 15 years | Anaplastic
ependymoma | PTR | − | + | 14 | DOD |
| EP5/M | 5 years | Anaplastic
ependymoma | GTR | + | + | 42 | NED |
| GBM1/F | 8 years | Glioblastoma
multiforme | PTR | + | + | 27 | DOD |
| GBM2/M | 9 years | Glioblastoma
multiforme | PTR | + | + | 12 | DOD |
Cell lines and RNA isolation
The human cell lines DAOY (medulloblastoma), T98G
(glioblastoma multiforme) and U87MG (glioblastoma-astrocytoma) were
cultured in medium (Eagle’s MEM with Earle’s Balanced Salts; MEM
EBSS) supplemented with 10% fetal bovine serum (FBS), 1%
L-glutamine, 1 mM Na pyruvate, 0.1 mM non-essential amino acids and
1% penicillin/streptomycin antibiotics at 37°C in a humidified 5%
CO2 atmosphere. All media were purchased from Euroclone
(Devon, UK).
RNA of tumors and cell lines was extracted using a
QIAamp RNA Blood Mini kit (Qiagen, Santa Clarita, CA, USA) and
quantified using a NanoDrop 2000 spectrophotometer (Thermo
Scientific, Logan, UT, USA). The RNA fragmentation state was
evaluated by 1.5% agarose gel electrophoresis.
Real-time quantitative (qRT)-PCR
All RNA samples (500 ng) were reverse transcribed to
cDNA using SuperScript™ First-Strand Synthesis System (Invitrogen,
Carlsbad, CA, USA) according to the manufacturer’s
instructions.
TaqMan real-time quantitative PCR was performed on
an ABI PRISM 7000 Sequence Detector System (Applied Biosystems,
Foster City, CA, USA).
PCR products for β1, β2 and β3-AR genes were
detected using gene-specific primers and probes labeled with the
reporter dye FAM (Applied Biosystems). The GAPDH
(glyceraldehyde-3-phosphate dehydrogenase) gene was used as an
endogenous control gene for normalization and was detected using
gene-specific primers and probes labeled with the reporter dye VIC
(Applied Biosystems).
PCR was carried out in triplicate on a 96-well plate
with 20 μl per well, using 1X TaqMan Universal PCR Master
mix. After incubation for 2 min at 50°C and 10 min at 95°C, the
reaction continued for 50 cycles of 95°C for 15 sec and 60°C for 1
min. The results were evaluated using the ABI 7000 PRISM software
and the Ct values were exported to Microsoft Excel.
The 2−ΔΔCt method described by Livak and
Schmittgen (26) was used to
analyse the results. The Ct values for each set of three reactions
were averaged for all subsequent calculations. For each tumor
sample the universal human reference RNA (Stratagene, Santa Clara,
CA, USA) was used as a control sample. Significance was estimated
according to the values in general use (P<0.05).
Immunohistochemistry
Surgical specimens were routinely formalin fixed and
paraffin embedded. Histological sections were stained with
hematoxylin-eosin (H&E) for histomorphological evaluation.
Sections (5 μm thick) of the most representative sample from
each tumor were mounted on electrostatic slides and used for
immunohistochemical staining. Immunohistochemical studies were
performed using the standard streptavidin-biotin technique and
commercially available reagents: rabbit polyclonal antibody
anti-adrenoceptor, β-1 (1:30 dilution; Santa Cruz Biotechnology,
Inc., Santa Cruz, CA, USA); rabbit polyclonal antibody
anti-adrenoceptor, β-2 (1:100 dilution; Chemicon, Temecula, CA,
USA). A positive control was normal skin. A negative control was
performed by substituting the primary antibody with a non-immune
serum at the same concentration. The control sections were treated
in parallel with the samples.
Immunohistochemical results were categorized using a
3-grade score: 0 (<10% positive tumor cells); 1 (10 to 49%
positive tumor cells); 2 (>50% positive tumor cells). In
addition, the immunostaining was also evaluated with regard to its
intensity: weak and strong.
Results
All 12 human brain tumor tissue samples and the
three tested cell lines (U87MG, T98G and DAOY) exhibited expression
of β1- and β2-ARs.
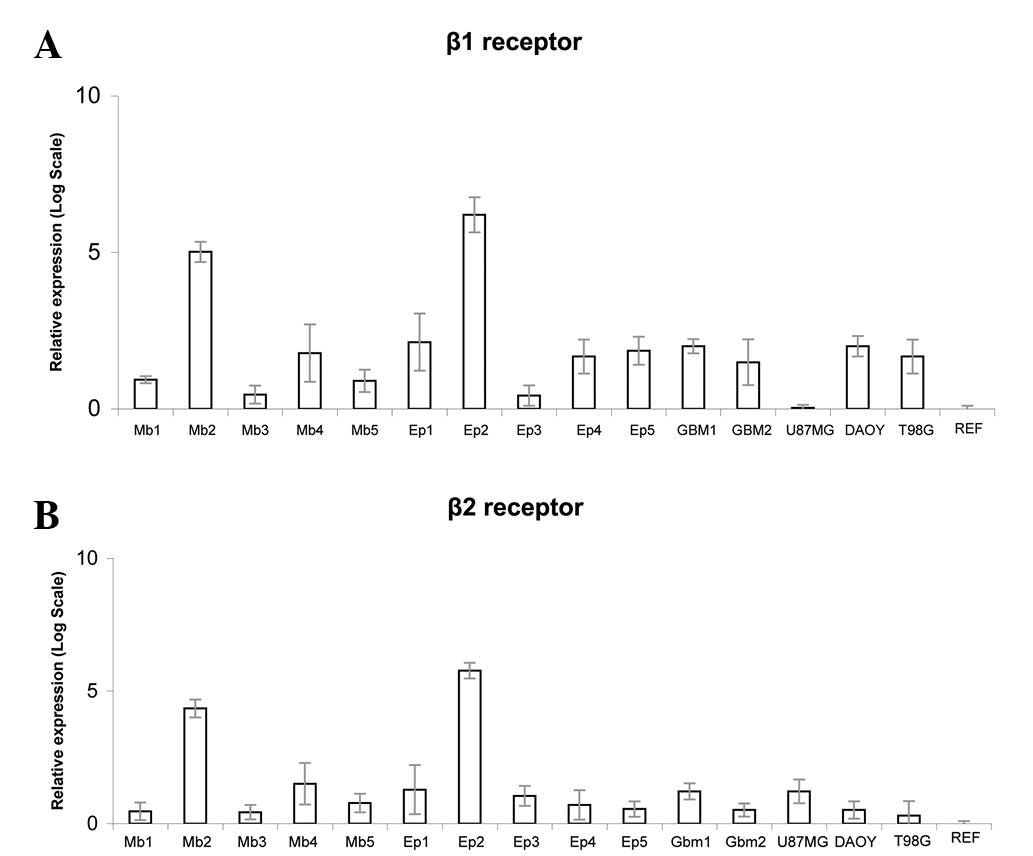
β1-AR expression was detected in all 12 tumor
samples and in the T98G and DAOY cell lines (Fig. 1A). β2-AR expression was detected in
all 12 tumor samples and in U87MG, T98G and DAOY cells (Fig. 1B). None of the tumor samples
expressed β3-AR, nor did the three cell lines or the universal
human reference RNA (Stratagene).
The mean absolute β1-AR mRNA level standardized to
GAPDH was 5.81 (range, −7.91 to 11.29) for tumors and 8.50 (range,
6.046 to 12.59) for cell lines (U87MG, DAOY and T98G). The median
absolute β2-AR mRNA level standardized for GAPDH was 4.74 (range,
−9.30 to 8.45) for tumor specimens and 7.62 (range, 5.85 to 8.88)
for cell lines. Human reference mRNA showed a value of 12.698 for
β1-AR and 9.887 for β2-AR. Values of β1- and β2-AR mRNA levels are
shown in Table II.
| Table IIβ1 and β2-AR analysis in pediatric
brain tumors. |
Table II
β1 and β2-AR analysis in pediatric
brain tumors.
| mRNA expression
levels (ΔΔCt)
|
Immunohistochemistry
|
|---|
| Sample | β1 receptor | β2 receptor | β1 receptor | β2 receptor |
|---|
| MB1 | 9.598 | 8.345 | 2 | 2 |
| MB2 | −3.968 | −4.528 | 1 | 2 |
| MB3 | 11.193 | 8.451 | 2 | 2 |
| MB4 | 6.785 | 4.891 | 1 | 2 |
| MB5 | 9.721 | 7.293 | 2 | 2 |
| EP1 | 5.611 | 5.637 | 2 | 2 |
| EP2 | −7.911 | −9.264 | 1 | 2 |
| EP3 | 11.291 | 6.421 | 1 | 2 |
| EP4 | 7.141 | 7.551 | 1 | 2 |
| EP5 | 6.525 | 8.061 | 2 | 2 |
| GBM1 | 6.046 | 5.846 | 1 | 2 |
| GBM2 | 7.751 | 8.180 | 2 | 2 |
| U87MG | 12.59 | 5.846 | | |
| DAOY | 6.046 | 8.18 | | |
| T98G | 7.141 | 8.88 | | |
| Human ref. | 12.698 | 9.887 | | |
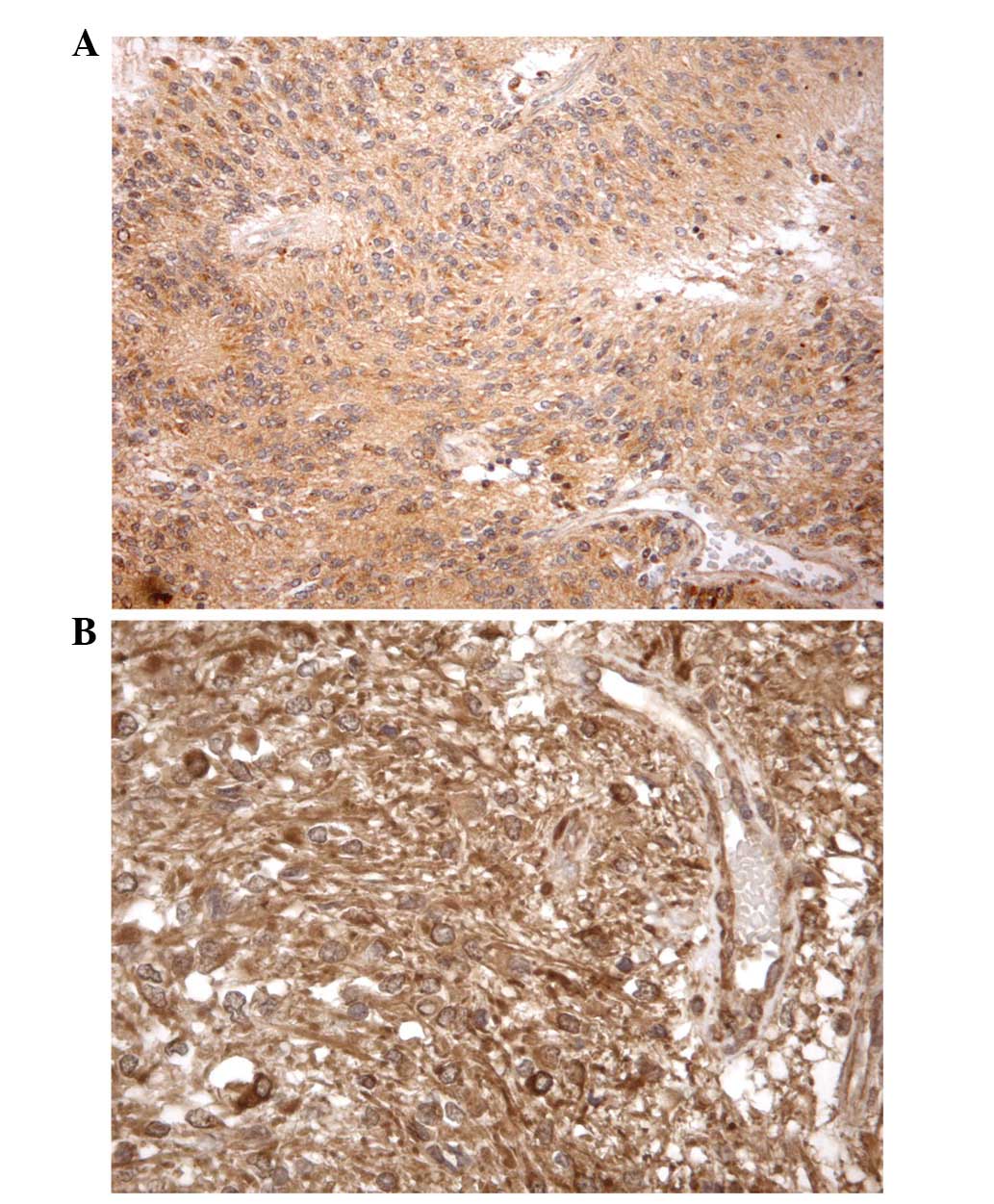
All brain tumor samples had a score of 2 at β2-AR
immunohistochemistry analysis. In immunohistochemistry for β1-AR, 6
tumors had a score of 2 and 6 had score 1, while none was
β1-AR-negative. Positive staining for β1-AR was observed in tissues
from 3 medulloblastoma, 2 anaplastic ependymoma and only 1
glioblastoma. Positive immunostaining was usually confined to the
cytoplasm of both the tumor cells (when present) and the
endothelial cells (which stained positively in all the cases
studied; Fig. 2).
Discussion
β-ARs are G protein coupled receptors (GPCRs) that
initiate the adenylyl cyclase/cAMP/PKA/CREB pathway which interacts
with the EGFR and Src/STAT pathways as well as the arachidonic acid
cascade (8). These signal
transduction pathways are positive regulators of tumor development
and progression and may therefore represent a possible novel target
for treatment.
In the present study we evaluated the expression of
β-ARs in malignant primary brain tumors of children. This issue has
been considered controversial due to conflicting results. The
absence of β-AR in capillaries isolated from glial tumors has been
demonstrated (19). Subsequently,
rat astroglial and neuronal cell lines have been shown to express
β-AR on their surface (20).
Our study population included highly vascularized
brain tumors, such as glioblastoma multiforme, anaplastic
ependymoma and medulloblastoma. Our findings demonstrate by qRT-PCR
and immunohistochemistry that β2-AR was overexpressed in all
tumors, whereas overexpression of β1-AR was found in 6 of 12
patients. There was no correlation between β-AR expression and the
presenting features of the patient or histological pattern of the
tumor.
β-ARs are known to have a widespread distribution in
numerous tissues and cell lines. We have been particularly
interested in β-AR located on blood vessels: possible targets
include endothelial cells, adventitial cells, pericytes,
fibroblasts, macrophages, adipocytes, perivascular axons and
Schwann cells. Autoradiography methods have demonstrated the
presence of both β1 and β2 antagonist binding sites in all three
layers of blood vessel walls (1).
Preclinical studies suggest that the β-adrenergic
system affects tumor progression by promoting proangiogenic factors
(18,27) and propranolol shows an inhibitory
effect on cancer cell proliferation (28) or appears to potentiate the efficacy
of antineoplastic drugs (29).
These observations, together with the evidence that metastasis
(migration of tumor cells via blood or lymphatic vessels from the
primary tumor site) is strictly regulated by exogenous cell
signaling molecules, including ligands of GPCRs (30,31)
may speculate a correlation between cancer and GPCRs/GPCR ligands,
including β-blockers.
A number of previous clinical observations or
laboratory models have studied the role of β-ARs in cancer
pathophysiology and the possibility of influencing cancer-specific
survival by pharmacological targeting of β-AR. Due to the wide
use/intake of propanolol and propanolol-derived drugs, a number of
epidemiological and observational studies about clinical features
of patients treated with β-blocking agents are now available,
including studies revealing an unexpected preventive effect of
primary cancer occurrence in patients receiving β-blockers
(10–14,16,32).
The mechanism by which propranolol reduces tumor
recurrence rates is not completely understood, but may relate to
its capacity to impair metastases formation which involves
migration of malignant cells from the primary tumor via lymphatic
routes or blood vessels. This process is tightly regulated by
exogenous signaling molecules (30,31).
Cell migration has been demonstrated to be mediated by β-ARs and
this process is inhibited by propranolol (3,4). In
vitro β-adrenergic stimulation compromises NK cell activity and
resistance to tumor metastasis in rats, while propranolol appears
to block this phenomenon (33).
Brain tumor secretion of matrix metalloproteinase-9 (MMP-9), a
protein which favors the dissemination of glioma tumoral cells by
disruption of the blood-brain barrier, is abrogated by
pharmacological targeting β-AR with propanolol (24,34).
One promising hypothesis is that the β-adrenergic
system plays an important role in the promotion of angiogenesis
that may be counteracted by propranolol (18,27).
Notably, in a mouse model of proliferative
retinopathy, the pharmacological blockade of β-AR with propranolol
has been demonstrated to reduce retinal levels of HIF-1α and,
consequently, of proangiogenic factors (VEGF and IGF-1), markedly
reducing retinal neoangiogenesis (35).
In conclusion, data from a small number of previous
studies indicate that β-blockers may have a role as novel
therapeutic agents in reducing tumor metastasis, tumor recurrence
and cancer-specific mortality. Although further studies are needed
to better define β-AR expression in pediatric CNS tumors, a
possible effect of propranolol and other β-blockers on the natural
history is conceivable. The demonstration of the presence of β-ARs
on pediatric malignant brain tumors may be the basis for an
experimental clinical use of propranolol.
Abbreviations:
|
β-ARs
|
β-adrenergic receptors;
|
|
GPCRs
|
G protein-coupled receptors;
|
|
OS
|
overall survival;
|
|
MMP-9
|
matrix metalloproteinase-9
|
Acknowledgements
This study was supported by
Associazione Italiana per la Ricerca sul Cancro (AIRC), grant
RG-6232; ‘Amicodivalerio’ Onlus; ‘NOI PER VOI’ Onlus; Fondazione
Tommasino Bacciotti; Fondazione Anna Meyer.
References
|
1
|
Daly CJ and McGrath JC: Previously
unsuspected widespread cellular and tissue distribution of
β-adrenoceptors and its relevance to drug action. Trends Pharmacol
Sci. 32:219–226. 2011.PubMed/NCBI
|
|
2
|
Drell TL IV, Joseph J, Lang K, Niggemann
B, Zaenker KS and Entschladen F: Effects of neurotransmitters on
the chemokinesis and chemotaxis of MDA-MB-468 human breast
carcinoma cells. Breast Cancer Res Treat. 80:63–70. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Masur K, Niggemann B, Zanker KS and
Entschladen F: Norepinephrine-induced migration of SW 480 colon
carcinoma cells is inhibited by beta-blockers. Cancer Res.
61:2866–2869. 2001.PubMed/NCBI
|
|
4
|
Palm D, Lang K, Niggemann B, Drell TL IV,
Masur K, Zaenker KS and Entschladen F: The norepinephrine-driven
metastasis development of PC-3 human prostate cancer cells in
BALB/c nude mice is inhibited by beta-blockers. Int J Cancer.
118:2744–2749. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Al-Wadei HA, Al-Wadei MH and Schuller HM:
Prevention of pancreatic cancer by the beta-blocker propranolol.
Anticancer Drugs. 20:477–482. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sood AK, Bhatty R, Kamat AA, et al: Stress
hormone-mediated invasion of ovarian cancer cells. Clin Cancer Res.
12:369–375. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yang EV, Kim SJ, Donovan EL, et al:
Norepinephrine upregulates VEGF, IL-8, and IL-6 expression in human
melanoma tumor cell lines: implications for stress-related
enhancement of tumor progression. Brain Behav Immun. 23:267–275.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schuller HM: Is cancer triggered by
altered signalling of nicotinic acetylcholine receptors? Nat Rev
Cancer. 9:195–205. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sloan EK, Priceman SJ, Cox BF, et al: The
sympathetic nervous system induces a metastatic switch in primary
breast cancer. Cancer Res. 70:7042–7052. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Algazi M, Plu-Bureau G, Flahault A, Dondon
MG and Lê MG: Could treatments with beta-blockers be associated
with a reduction in cancer risk? Rev Epidemiol Sante Publique.
52:53–65. 2004.(In French).
|
|
11
|
Perron L, Bairati I, Harel F and Meyer F:
Antihypertensive drug use and the risk of prostate cancer (Canada).
Cancer Causes Control. 15:535–541. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Powe DG, Voss MJ, Zänker KS, Habashy HO,
Green AR, Ellis IO and Entschladen F: Beta-blocker drug therapy
reduces secondary cancer formation in breast cancer and improves
cancer specific survival. Oncotarget. 1:628–638. 2010.PubMed/NCBI
|
|
13
|
Ganz PA, Habel LA, Weltzien EK, Caan BJ
and Cole SW: Examining the influence of beta blockers and ACE
inhibitors on the risk for breast cancer recurrence: results from
the LACE cohort. Breast Cancer Res Treat. 129:546–556.
2011.PubMed/NCBI
|
|
14
|
Barron TI, Connolly RM, Sharp L, Bennett K
and Visvanathan K: Beta blockers and breast cancer mortality: a
population-based study. J Clin Oncol. 29:2635–2644. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Melhem-Bertrandt A, Chavez-Macgregor M,
Lei X, et al: Beta-blocker use is associated with improved
relapse-free survival in patients with triple-negative breast
cancer. J Clin Oncol. 29:2645–2652. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
De Giorgi V, Grazzini M, Gandini S,
Benemei S, Lotti T, Marchionni N and Geppetti P: Treatment with
β-blockers and reduced disease progression in patients with thick
melanoma. Arch Intern Med. 171:779–781. 2011.
|
|
17
|
Lemeshow S, Sørensen HT, Phillips G, et
al: β-Blockers and survival among Danish patients with malignant
melanoma: a population-based cohort study. Cancer Epidemiol
Biomarkers Prev. 20:2273–2279. 2011.
|
|
18
|
Park SY, Kang JH, Jeong KJ, et al:
Norepinephrine induces VEGF expression and angiogenesis by a
hypoxia-inducible factor-1α protein-dependent mechanism. Int J
Cancer. 128:2306–2316. 2011.PubMed/NCBI
|
|
19
|
Magnoni MS, Frattola L, Piolti R, Govoni
S, Kobayashi H and Trabucchi M: Glial brain tumors lack
microvascular adrenergic receptors. Eur Neurol. 28:27–29. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ruck A, Millns P, Kendall DA and Hill SJ:
Expression of beta 2-adrenoceptors mediating cyclic AMP
accumulation in astroglial and neuronal cell lines derived from the
rat CNS. Biochem Pharmacol. 40:2371–2375. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sokołowska P and Nowak JZ: Constitutive
activity of beta-adrenergic receptors in C6 glioma cells. Pharmacol
Rep. 57:659–663. 2005.PubMed/NCBI
|
|
22
|
Lung HL, Shan SW, Tsang D and Leung KN:
Tumor necrosis factor-alpha mediates the proliferation of rat C6
glioma cells via beta-adrenergic receptors. J Neuroimmunol.
166:102–112. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Annabi B, Lachambre MP, Plouffe K,
Moumdjian R and Béliveau R: Propranolol adrenergic blockade
inhibits human brain endothelial cells tubulogenesis and matrix
metalloproteinase-9 secretion. Pharmacol Res. 60:438–445. 2009.
View Article : Google Scholar
|
|
24
|
Annabi B, Vaillancourt-Jean E, Weil AG and
Béliveau R: Pharmacological targeting of β-adrenergic receptor
functions abrogates NF-κB signaling and MMP-9 secretion in
medulloblastoma cells. Onco Targets Ther. 3:219–226. 2010.
|
|
25
|
Toll L, Jimenez L, Waleh N, et al:
{Beta}2-adrenergic receptor agonists inhibit the proliferation of
1321N1 astrocytoma cells. J Pharmacol Exp Ther. 336:524–532.
2011.
|
|
26
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chakroborty D, Sarkar C, Basu B, Dasgupta
PS and Basu S: Catecholamines regulate tumor angiogenesis. Cancer
Res. 69:3727–3730. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang D, Ma Q, Shen S and Hu H: Inhibition
of pancreatic cancer cell proliferation by propranolol occurs
through apoptosis induction: the study of beta-adrenoceptor
antagonist’s anticancer effect in pancreatic cancer cell. Pancreas.
38:94–100. 2009.PubMed/NCBI
|
|
29
|
Pasquier E, Ciccolini J, Carre M, et al:
Propranolol potentiates the anti-angiogenic effects and anti-tumor
efficacy of chemotherapy agents: implication in breast cancer
treatment. Oncotarget. 2:797–809. 2011.PubMed/NCBI
|
|
30
|
Entschladen F, Drell TL IV, Lang K, Joseph
J and Zaenker KS: Tumour-cell migration, invasion, and metastasis:
navigation by neurotransmitters. Lancet Oncol. 5:254–258. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Entschladen F, Drell TL IV, Lang K, Joseph
J and Zaenker KS: Neurotransmitters and chemokines regulate tumor
cell migration: potential for a new pharmacological approach to
inhibit invasion and metastasis development. Curr Pharm Des.
11:403–411. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Diaz E, Karlan B, Cass I, Walsh C and Li
A: Impact of beta blockers on epithelial ovarian cancer survival.
Gynecol Oncol. 120(Suppl 1): S362011. View Article : Google Scholar
|
|
33
|
Shakhar G and Ben-Eliyahu S: In vivo
beta-adrenergic stimulation suppresses natural killer activity and
compromises resistance to tumor metastasis in rats. J Immunol.
160:3251–3258. 1998.PubMed/NCBI
|
|
34
|
Lakka SS, Gondi CS and Rao JS: Proteases
and glioma angiogenesis. Brain Pathol. 15:327–341. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ristori C, Filippi L, Dal Monte M, et al:
Role of the adrenergic system in a mouse model of oxygen-induced
retinopathy: antiangiogenic effects of beta-adrenoreceptor
blockade. Invest Ophthalmol Vis Sci. 52:155–170. 2011. View Article : Google Scholar : PubMed/NCBI
|