Introduction
A number of prostate cancer patients have metastatic
growth at diagnosis and others develop metastases after potentially
curative surgery or radiotherapy. Combinations of chemotherapy
agents have some efficacy in these cases, but the prognosis for
long-term survival is poor, especially when the tumors have formed
distant metastases, e.g., in the skeleton. Receptor-targeted
therapy with radionuclides or toxins may improve the response and
survival times, especially in cases where chemotherapy and therapy
with tyrosine kinase inhibitors are not effective. Targeted
radionuclide therapy, supported by imaging for treatment planning,
dosimetry and follow-up of therapy effects, is one option (1,2).
In order for receptor-targeted therapy to be an
effective complement or alternative to chemotherapy, the
disseminated tumor cells and metastases must express the target
structure to at least a similar extent as the primary tumors. There
are several indications for various types of tumors that in cases
where the expression of members of the epidermal growth factor
receptor (EGFR) family is high in the primary tumor, it may also be
high in the metastases (2–4). The reason for this may be that the
receptor-expressing tumor cells require the growth factor-receptor
interactions for growth stimulation. If disseminated tumor cells
reduce or lose the expression of the receptor, for example due to
genomic instability, they may also lose growth capacity (3,5).
The EGFR family consists of EGFR, HER2, HER3 and
HER4, which have an extracellular ligand binding domain, a
hydrophobic transmembrane domain and an intracellular domain with
protein-tyrosine kinase activity. However, HER3 has no intrinsic
tyrosine kinase activity and no ligand for HER2 has been identified
to date, but they both contribute to intracellular signaling via
dimerization with each other or with other receptors in the family.
EGF and five other ligands bind to EGFR and neuregulins (NRGs) are
the ligands for HER3 and HER4. The overexpression of EGFR and HER2
has been reported to be associated with high malignancy (2–7).
Targeted therapy is a clinical reality for tumors
which express EGFR (cetuximab) or HER2 (trastuzumab), although
resistance has been reported in both cases (8–12).
EGFR and HER2 appear to be good targets for radionuclide- or
toxin-based tumor therapy, although whether this is the case for
prostate cancer is not clear (2,3). It
remains to be determined whether HER3 is also a suitable target in
prostate cancer (13). One problem
appears to be that in immunohistochemical staining for several
tumor types, including laryngeal, esophageal, base of tongue
carcinomas and colorectal tumors, HER3 is often observed to be
mainly localized to the cytoplasm (14–17)
(see also the protein atlas: http://www.proteinatlas.org/). This staining pattern
is not understood since HER3 contains a trans-membrane region. The
role of HER4 in tumor growth is not clear (2,3) and
therefore, HER4 was not analyzed in this study.
EGFR family-targeted radionuclide or toxin therapy
aims to target the often abundant native, not mutated, receptors
and the effect of such therapy is probably not dependent on whether
the targeting agent strongly interferes with intracellular
signaling. The cell killing properties of ionizing radiation and
toxins are well known and treatment-induced resistance for
radiation has, to the best of our knowledge, not been reported
(2). With this background as
inspiration, we investigated the expression of EGFR, HER2 and HER3
in 12 prostate cancer patients in primary tumors and corresponding
lymph node metastases.
Materials and methods
Patients and samples
A total of 12 patients with lymph node-positive
prostate cancer were diagnosed and treated in the Affiliated
Hospitals, Zhejiang University School of Medicine (Hangzhou,
China). They were included in this study after approval of the
Institutional Review Board. Primary tumor and lymph node metastases
samples were obtained from all patients following their
consent.
The primary tumor tissues and the lymph node
metastases samples were fixed in 4% buffered formalin, processed
and embedded in paraffin. Sections, 4-μm thick, were cut and
deparaffinized in xylene and hydrated through graded concentrations
of ethanol to distilled water (14–17).
The samples were then stained with hematoxylin and eosin for
routine clinical analysis and, for this specific research project,
with immunohistochemical receptor staining, as described below. The
patient and tumor characteristics are shown in Table I.
 | Table IPatient data. |
Table I
Patient data.
| Patient | Age (years) | Gleason score | T-stage |
|---|
| 1 | 63 | No record | T3 |
| 2 | 67 | 4+4=8 | T3 |
| 3 | 58 | 4+5=9 | T4 |
| 4 | 69 | 4+4=8 | T2 |
| 5 | 64 | 3+5=8 | T3 |
| 6 | 63 | 5+4=9 | T4 |
| 7 | 66 | 4+5=9 | T3 |
| 8 | 68 | 3+4=7 | T2 |
| 9 | 74 | 5+3=8 | T3 |
| 10 | 59 | 4+5=9 | T3 |
| 11 | 61 | 3+4=7 | T3 |
| 12 | 57 | 5+4=9 | T2 |
EGFR staining
EGFR was assessed by immunohistochemistry using a
streptavidin-biotin complex technique as previously described
(14,15,17).
After deparaffinization of the sections, endogenous peroxidase was
blocked in 0.3% H2O2 in PBS for 20 min. Then,
enzymatic antigen retrieval was performed in 0.05% protease K (Code
no. S3020, Dako, Glostrup, Denmark) in PBS for 10 min at room
temperature. The slides were preincubated in PBS for 10 min. The
primary mouse monoclonal antibody directed against EGFR (clone
31G7, Zymed Laboratories, South San Francisco, CA, USA) was diluted
1:100 and incubated overnight at 4°C. The secondary biotinylated
antibodies (goat anti-mouse, Dako) and the peroxidase-labeled
streptavidin-biotin complex (Dako) were diluted 1:200 and incubated
for 30 min at room temperature. All slides were developed in 0.05%
diaminobenzidine (Sigma, St. Louis, MO, USA) for 5 min and
counterstained in Harris hematoxylin (Sigma). Finally, the slides
were dehydrated through graded alcohol to xylene and mounted in
organic mounting medium (Pertex®, Histolab, Gothenburg,
Sweden).
HER2 staining
The HER2 immunohistochemical staining was performed
as previously described (14,15,17).
After deparaffinization, the sections were incubated in methanol
and hydrogen peroxide for 30 min to quench endogenous peroxidase
activity. Antigen retrieval was performed in a waterbath at
95–98°C, pH 6.0, for 40 min. The glasses were then cooled to room
temperature and then washed in distilled water. Immunohistochemical
stainings were performed using the Elite ABC Kit (Vectastain,
Vector Laboratories, Burlingame, CA, USA). Blocking serum was
applied for 15 min and followed by incubation with rabbit
anti-human c-erbB-2 oncoprotein (code No. A 0485, Dako) diluted
1:350. Sections were then incubated with the biotinylated secondary
antibody and visualized using the peroxidase substrate
3-amino-9-ethylcarbazole (AEC; Sigma A-5754) as a chromogen.
Finally, the sections were counterstained with Mayer’s hematoxylin
and mounted with Aquamount (BDH Ltd., Poole, UK).
HER3 staining
The HER3 staining was performed as previously
described (14,15,17).
After deparaffinization, the sections were incubated in methanol
and hydrogen peroxide for 30 min to quench endogenous peroxidase
activity. Antigen retrieval was performed in a pressure chamber at
125°C, pH 9.0, for 4 min. The glasses were then cooled at room
temperature and washed in distilled water. Immunohistochemical
stainings were performed using the Elite ABC Kit (Vectastain,
Vector Laboratories). Blocking serum was applied for 15 min and
followed by incubation with the monoclonal antibody MAB4021
(Chemicon, Temecula, CA, USA) diluted 1:800. Sections were then
incubated with a biotinylated secondary antibody and visualized
using AEC as a chromogen. Finally, the sections were counterstained
with Mayer’s hematoxylin and mounted with Aquamount (BDH Ltd.).
EGFR and HER2 scores
The HER2 expression was scored using the HercepTest
scoring criteria. This is based on a scale where 0 corresponds to
tumor cells that were completely negative, 1+ corresponds to faint
perceptible staining of the tumor cell membranes, 2+ corresponds to
moderate staining of the entire tumor cell membranes and 3+ is
marked circumferential staining of the entire tumor cell membranes
creating a fishnet pattern. The Canadian and the Dako HercepTest
guidelines (21) that require
>10% of the tumor cells to be stained were applied. Cytoplasmic
staining was considered to be non-specific and was not included in
the scoring. As positive controls we used in-house positive control
tissue sections as well as positive control sections supplied by
Dako. As negative HER2 controls we used normal tissues, which are
expected not to express HER2, such as connective tissue observed in
the same sections as the tumor cells. In the metastases sections we
used lymphocytes and the surrounding capsule of the lymph nodes as
HER2-negative internal controls. The expression pattern of EGFR is
similar to that of HER2 and EGFR expression was therefore evaluated
using the same scoring criteria as for HER2. As EGFR-positive
controls we used in-house positive control skin tissue sections. As
negative controls we used connective tissue observed in the same
sections as the tumor cells. In the metastases sections we used
lymphocytes and the surrounding capsule of the lymph nodes as
EGFR-negative internal controls.
HER3 evaluation
The HER3 staining was evaluated as negative, weak or
strong staining (14,15,17).
Negative corresponded to tumor cells that were not at all stained,
weak corresponded to faint staining of the tumor cytoplasm with or
without stained granules and strong corresponded to intensive tumor
granular cytoplasmic staining. As positive controls we used normal
laryngeal epithelium (positive reference staining may also be found
at www.proteinatlas.org). As negative controls we
used tumor stroma of connective tissue character and non-tumor
invaded areas of lymph nodes.
Results
Since only 12 patients were included in the study
(Table I), we report results for
the primary tumors and metastases of each individual patient in
Tables II–IV.
| Table IIEGFR family (EGFR, HER2 and HER3)
scores in primary tumors and in the corresponding lymph node
metastases. |
Table II
EGFR family (EGFR, HER2 and HER3)
scores in primary tumors and in the corresponding lymph node
metastases.
A, EGFR and HER2
scores
|
|---|
| Metastasis (patient
number)
|
|---|
| Primary tumor | 0 | 1+ | 2+ | 3+ |
|---|
| EGFR | | | | |
| 0 | 3,6 | - | - | - |
| 1+ | 5,9,10,11 | - | - | 7 |
| 2+ | - | - | 1,8,12 | - |
| 3+ | - | - | - | 2,4 |
| HER2 | | | | |
| 0 | 1,11 | - | - | - |
| 1+ | 8 | - | 2,5,6,7 | 4 |
| 2+ | 9 | - | 3,10 | - |
| 3+ | - | - | - | 12 |
B, HER3 scores
|
|---|
| Metastasis (patient
number)
|
|---|
| Primary tumor | Negative | Weak | Strong |
|---|
| Negative | 1,2,3 | - | - |
| Weak | 5,6,8,9,10,12 | - | 4 |
| Strong | 11 | 7 | - |
| Table IVCorrelation between EGFR and HER2 in
the studied primary tumor and metastasis samples. |
Table IV
Correlation between EGFR and HER2 in
the studied primary tumor and metastasis samples.
| HER2 (patient
number)
|
|---|
| EGFR | 0 | 1+ | 2+ | 3+ |
|---|
| Primary tumor | | | | |
| 0 | - | 6 | 3 | - |
| 1+ | 11 | 5,7 | 9,10 | - |
| 2+ | 1 | 8 | - | 12 |
| 3+ | - | 2,4 | - | - |
| Metastasis | | | | |
| 0 | 9,11 | - | 3,5,6,10 | - |
| 1+ | - | - | | - |
| 2+ | 1,8 | - | - | 12 |
| 3+ | - | - | 2,7 | 4 |
EGFR expression
Of the 12 primary tumors, 5 had 2+ or 3+ EGFR scores
(patients 1, 2, 4, 8 and 12). The EGFR expression in the
corresponding lymph node metastases was upregulated in one
metastasis (patient 7), so a total of 6 metastases were
EGFR-positive. No downregulation of EGFR from 2+ or 3+ in the
primary tumor to 0 or 1+ in the metastasis was observed (Table IIA).
HER2 expression
Of the 12 patients, 4 had strong HER2 expression (2+
or 3+) in the primary tumors (patients 3, 9, 10 and 12). There was
one downregulation (from 2+ to 0, patient 9) and 5 cases of
upregulation in the metastases (patients 2, 4, 5, 6 and 7), giving
a total of 8 HER2-positive metastases out of the 12 cases analyzed.
Thus, there was a marked tendency for the upregulation of HER2 in
the metastases (Table IIA).
HER3 expression
HER3 was weakly or strongly expressed in 9 out of
the 12 cases in the primary tumors (all except patients 1, 2, and
3) but downregulated in all but two (patients 4 and 7) in the
corresponding lymph node metastases. Thus, 7 metastases had
downregulated HER3 compared with the primary tumors (Table IIB).
Co-expression
There was positive co-expression of all three
receptors in only one of the primary tumors (patient 12) and that
patient was also the only one with positive co-expression of EGFR
and HER2 (2+ and 3+, respectively) when the primary tumors were
considered. However, there was positive co-expression of EGFR and
HER2 in 4 of the metastases (patients 2, 4, 7 and 12). Thus, there
was a marked tendency that the positive co-expression of EGFR and
HER2 increased in the lymph node metastases compared with the
primary tumors. The extensive downregulation of HER3 in the
metastases resulted in reduced co-expression of EGFR and HER3
(Tables III and IV).
| Table IIICo-expression of the receptors. |
Table III
Co-expression of the receptors.
| Patient number
| |
|---|
| Tissue | Positive | Negative | No. of
co-expression |
|---|
| Primary tumors | | | |
| EGFR, HER2,
HER3 | 12 | - | 1 |
| EGFR, HER2 | 12 | 5,6,7,11 | 5 |
| EGFR, HER3 | 4,8,12 | 3 | 4 |
| HER2, HER3 | 9,10,12 | 1,2 | 5 |
| Metastases | | | |
| EGFR, HER2,
HER3 | 4,7 | 9,11 | 4 |
| EGFR, HER2 | 2,4,7,12 | 9,11 | 6 |
| EGFR, HER3 | 4,7 | 3,5,6,9,10,11 | 8 |
| HER2, HER3 | 4,7 | 1,8,9,11 | 6 |
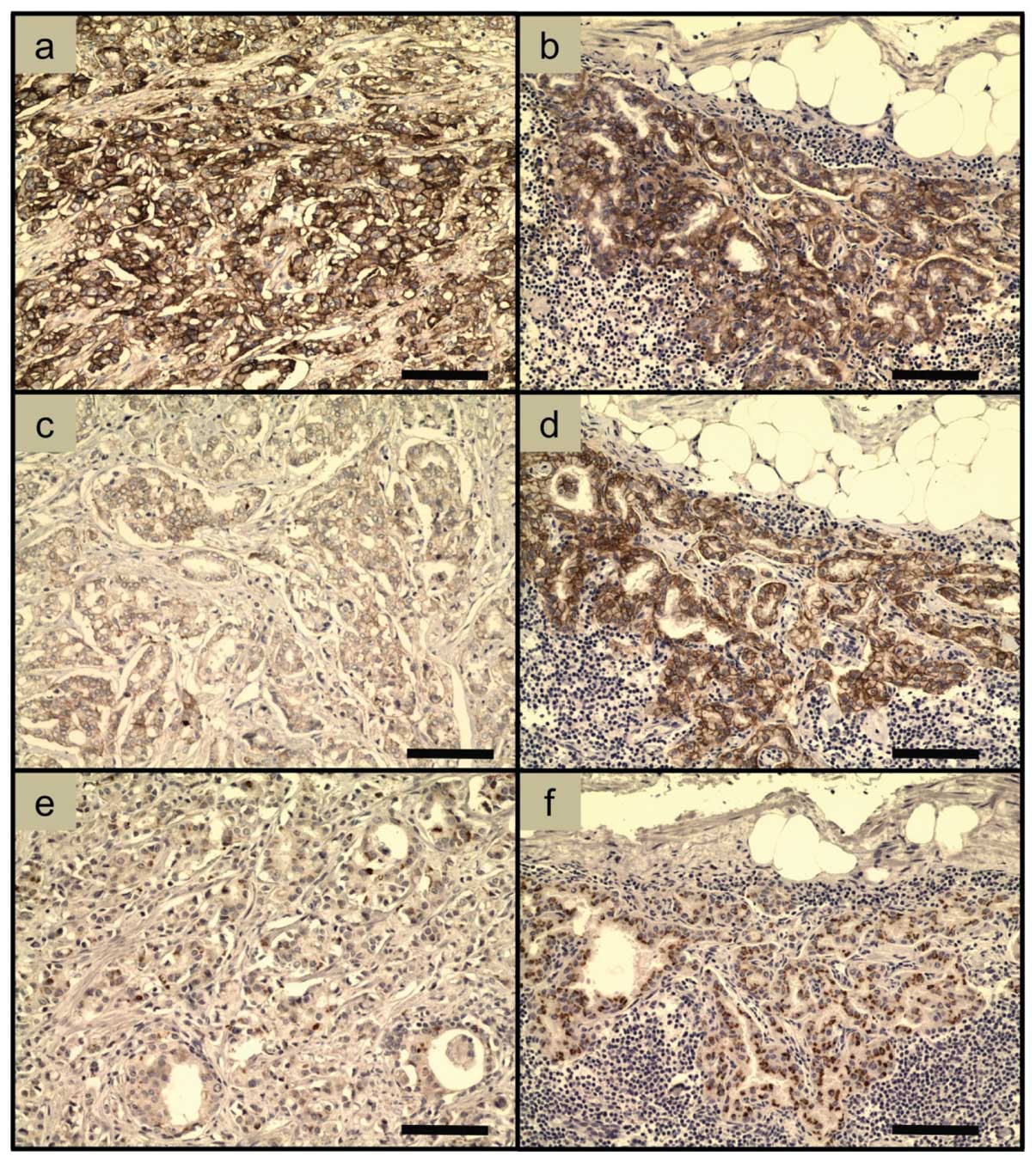
Immunohistochemical stainings
Examples of immunohistochemical EGFR, HER2 and HER3
stainings of samples from patient 4 are shown in Fig. 1. Note the strong EGFR staining in
both the primary tumor (Fig. 1a)
and the metastasis (Fig. 1b). HER2
was upregulated in the metastasis (Fig.
1d) compared with the primary tumor (Fig. 1c). The HER3 staining changed from
weak in the primary tumor (Fig. 1e)
to strong in the metastasis (Fig.
1f), in contrast to the HER3 stainings in all other
patients.
Discussion
There were several differences between the primary
tumors and the corresponding metastases, especially with regard to
the expression of HER2 and HER3. HER2 was upregulated in the
metastases of 5 out of the 8 patients with HER2-negative primary
tumors. There was positive co-expression of EGFR and HER2 in only
one of the primary tumors, while there was positive co-expression
of EGFR and HER2 in 4 of the metastases. Thus, there was a tendency
for both upregulation of HER2 and increased positive co-expression
of EGFR and HER2 in the lymph node metastases in comparison to the
primary tumors. Furthermore, there appeared to be a marked
downregulation of HER3 since 7 metastases had downregulated HER3,
from weak or strong expression in the primary tumors to negative in
the corresponding metastases.
Thus, it appears that the tumor cells forming the
metastases may be a subtype, most likely with a more aggressive
phenotype and/or genotype than the cells in the primary tumors.
However, there was no downregulation of EGFR, indicating that the
metastases originating from EGFR-positive primary tumors may be
dependent on continued EGFR expression. It has been indicated that
blocking EGFR reduces the invasive potential of prostate cancer
cells (22,23).
The EGFR expression frequency in primary prostate
cancer is, according to the few available previously published
studies, in the range of 40–45% and is higher in hormone refractory
(castration resistant) than in hormone sensitive prostate cancers
(2,24–26).
In the present study, 5 out of the 12 patients had EGFR-positive
primary tumors.
The HER2 expression frequency in hormone refractory
(castration resistant) prostate cancer has been reported in in wide
range 20–70% (2,27–30).
Thus, there are studies on both high and low frequencies of HER2
expression in the primary tumors and one study reported almost no
HER2 expression (31). However,
HER2 has been reported to be expressed at high frequencies in
metastases from prostate cancer and has, in one study, been found
in up to 90% of the analyzed cases (32). In the present study, 8 out of 12
metastases were HER2-positive. This indicates upregulation of HER2
in metastases. HER2-positive prostate cancer cells have also been
detected in the peripheral blood of prostate cancer patients
(33). By contrast, it has been
reported that HER2 was expressed in metastases at a similar level
as in the corresponding primary prostate tumors (34) and one study reported almost no HER2
expression in lymph node metastases from prostate cancer (31).
The reported variations between different studies on
HER2 expression are probably due to different patient inclusion and
receptor scoring criteria and there are also differences in
immunohistochemical retrieval techniques between the laboratories,
as can be observed in the original articles. It is important to
agree on common histological processing techniques and standardized
scoring criteria and the HercepTest applied for breast cancer
(21) is a good example. The
possibility that etiological differences play a role in the
variation of reported HER2 expression levels cannot be
excluded.
The HER3 expression frequency has been reported to
be 21% in primary prostate cancers (27) and HER3 appears to be expressed in
metastases (2,34). However, the indicated downregulation
of HER3 in prostate metastases in the present study has not
previously been reported. A secreted isoform of HER3, MDA-BF-1, has
been observed in metastatic prostate cancer (35).
There is a controversy since molecular biology
studies report HER3 to be a cell membrane-associated receptor
expressing a transmembrane region. This is in contrast to a number
of histopathological findings, with most of the HER3 staining in
the cytoplasm. It cannot be excluded that HER3 is, to a large
extent, associated with intracellular membranes and/or that
precursors of HER3 in the cytoplasm are stained. Furthermore, HER3
may be in the outer cell membrane for only a short time due to a
possible rapid turnover.
The expression of EGFR and HER2 in normal tissues
was characterized a number of years ago. EGFR is expressed in the
skin, liver, digestive tract and reproductive organs (36–38).
The distributions of EGFR in various tissues can also be found at
the human protein atlas (http://www.proteinatlas.org/). The HER2 expression in
normal tissues in adults is generally low (39–41)
(see also the human protein atlas: http://www.proteinatlas.org/).
The previously published receptor determinations,
together with our findings, indicate that prostate cancers have the
potential to express EGFR and HER2 in primary tumors and
metastases. It is noteworthy that four patients (numbers 2, 4, 7
and 12) out of the 12 studied may be candidates for combined
therapy, targeting both EGFR and HER2 in the metastases, at least
if the analyzed lymph node metastases are representative of any
other metastases that these four patients may suffer from. The
targeting process should then deliver radionuclides or toxins of
therapeutic use. This may be necessary since HER2-targeted therapy
of hormone refractory (castration resistant) prostate cancers with
antibodies without toxic agents, ‘naked antibodies’, has recently
been studied, thus far without positive results (42,43).
Furthermore, the use of tyrosine kinase inhibitors blocking both
HER2 and EGFR in hormone refractory (castration resistant) prostate
cancers has also not shown a good response (44), although there is hope for future
improvements (45,46). Delivery of toxic agents via the
receptors is most likely a better choice.
Thus, targeted therapy delivering radionuclides or
toxins is an alternative in cases with significant levels of
receptors, but with the tumor cells resistant to chemotherapy,
tyrosine kinase inhibitors and the action of ‘naked antibodies’.
However, the expression intensity per tumor cell of EGFR and HER2
in prostate cancer metastases may be low and/or heterogeneous
(3). This further indicates that
there may be a need for ‘multiple targeting’, e.g., a cocktail with
binders to both EGFR and HER2. The possibility to target more than
one receptor at the time should be considered since co-expression
of receptors may also be associated with high-grade malignancy
(6,7) and targeting against EGFR and HER2 may
also increase the targeting specificity. More research is needed
regarding this.
We are especially interested in targeted
radionuclide therapy since that relies on several years of clinical
experience to kill tumor cells and severe resistance has thus far
not been associated with radiation therapy. Targeted radionuclide
therapy using radiolabeled somatostatin analogs
(177Lu-Octreotate) for treatment of neuroendocrine
tumors and radiolabeled anti-CD20 antibodies
(90Y-Zevalin) for treatment of chemotherapy-resistant
lymphomas are accepted modalities (1,2). The
promising therapeutic results in these cases suggest that targeted
radionuclide therapy may also be successful in the treatment of
prostate cancers and that more patients may be treated with a
curative instead of palliative intention.
The design of suitable receptor-binding agents with
high binding to prostate cancer cells and low uptake in critical
normal tissues is a challenge. However, there is potential for
development since new knowledge is continuously emerging about
biodistribution, pharmacokinetics and the cellular processing of
different types of targeting agents and the research on molecular
design of new targeting agents is rapidly expanding (47). The development of peptides and small
proteins, such as affibody molecules (48), is one strategy and the area of
antibody engineering is rapidly developing. Various forms of
antibody fragments, including minimal recognizing units, single
chain fragments (scFvs) and dimeric scFvs, are drawing increasing
interest (49,50). Bifunctional molecules, with capacity
to bind two different receptors at the same time are, as indicated
above, a possible approach for therapy. Liposomes containing toxic
substances and conjugated with targeting agents may be of use for
the killing of disseminated tumor cells in the systemic circulation
(51).
To summarize, the indicated increase in HER2
expression and co-expression of EGFR and HER2 in the metastases may
be promising for the use of agents that deliver therapeutically
useful radionuclides or toxins in at least a subpopulation of
prostate cancer patients. HER3 may be of less use, based on the
results of the present limited study. The results are encouraging
for studies involving more patients.
Acknowledgements
This study was funded by the Swedish
Cancer Society (no. 11 0565; J. Carlsson) and grants from National
Natural Science Foundation of China (no. 81071823; Q. Wei) and from
the Young Investigator Fund from Health Bureau of Zhejiang China
(no. 2008QN020; Q. Wei).
References
|
1
|
Sharkey RM and Goldenberg DM: Cancer
radioimmunotherapy. Immunotherapy. 3:349–370. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Carlsson J: Potential for clinical
radionuclide-based imaging and therapy of common cancers expressing
EGFR-family receptors. Tumour Biol. 33:653–659. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Carlsson J: EGFR-family expression and
implications for targeted radionuclide therapy. Targeted
Radionuclide Tumor Therapy, Biological Aspects. Stigbrand T, Adams
G and Carlsson J: Springer Verlag; pp. 25–58. 2008, View Article : Google Scholar
|
|
4
|
Houssami N, Macaskill P, Balleine RL,
Bilous M and Pegram MD: HER2 discordance between primary breast
cancer and its paired metastasis: tumor biology or test artefact?
Insights through meta-analysis. Breast Cancer Res Treat.
129:659–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pecorino L: Molecular Biology of Cancer:
Mechanisms, Targets, and Therapeutics. Oxford University Press;
Oxford: 2005
|
|
6
|
Citri A and Yarden Y: EGF-ERBB signalling:
towards the systems level. Nat Rev Mol Cell Biol. 7:505–516. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bublil EM and Yarden Y: The EGF receptor
family: spearheading a merger of signaling and therapeutics. Curr
Opin Cell Biol. 19:124–134. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Morgillo F, Bareschino MA, Bianco R,
Tortora G and Ciardiello F: Primary and acquired resistance to
anti-EGFR targeted drugs in cancer therapy. Differentiation.
75:788–799. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lièvre A, Bachet JB, Boige V, Cayre A, Le
Corre D, Buc E, Ychou M, Bouché O, Landi B, Louvet C, et al: KRAS
mutations as an independent prognostic factor in patients with
advanced colorectal cancer treated with cetuximab. J Clin Oncol.
26:374–379. 2008.
|
|
10
|
Di Nicolantonio F, Martini M, Molinari F,
Sartore-Bianchi A, Arena S, Saletti P, De Dosso S, Mazzucchelli L,
Frattini M, Siena S and Bardelli A: Wild-type BRAF is required for
response to panitumumab or cetuximab in metastatic colorectal
cancer. J Clin Oncol. 26:5705–5712. 2008.
|
|
11
|
Nahta R and Esteva FJ: Trastuzumab:
triumphs and tribulations. Oncogene. 26:3637–3643. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Berns K, Horlings HM, Hennessy BT,
Madiredjo M, Hijmans EM, Beelen K, Linn SC, Gonzalez-Angulo AM,
Stemke-Hale K, Hauptmann M, et al: A functional genetic approach
identifies the PI3K pathway as a major determinant of trastuzumab
resistance in breast cancer. Cancer Cell. 12:395–402. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jathal MK, Chen L, Mudryj M and Ghosh PM:
Targeting ErbB3: the New RTK(id) on the Prostate Cancer Block.
Immunol Endocr Metab Agents Med Chem. 11:131–149. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wei Q, Sheng L, Shui Y, Hu Q, Nordgren H
and Carlsson J: EGFR, HER2, and HER3 expression in laryngeal
primary tumors and corresponding metastases. Ann Surg Oncol.
15:1193–1201. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wei Q, Chen L, Sheng L, Nordgren H, Wester
K and Carlsson J: EGFR, HER2 and HER3 expression in esophageal
primary tumours and corresponding metastases. Int J Oncol.
31:493–499. 2007.PubMed/NCBI
|
|
16
|
Ekberg T, Nestor M, Engström M, Nordgren
H, Wester K, Carlsson J and Anniko M: Expression of EGFR, HER2,
HER3, and HER4 in metastatic squamous cell carcinomas of the oral
cavity and base of tongue. Int J Oncol. 26:1177–1185.
2005.PubMed/NCBI
|
|
17
|
Wei Q, Shui Y, Zheng S, Wester K, Nordgren
H, Nygren P, Glimelius B and Carlsson J: EGFR, HER2 and HER3
expression in primary colorectal carcinomas and corresponding
metastases: Implications for targeted radionuclide therapy. Oncol
Rep. 25:3–11. 2011.PubMed/NCBI
|
|
18
|
Gleason DF; The Veteran’s Administration
Cooperative Urologic Research Group: Histologic grading and
clinical staging of prostatic carcinoma. Urologic Pathology: The
Prostate. Tannenbaum M: Lea and Febiger; Philadelphia: pp. 171–198.
1977
|
|
19
|
Gleason DF: Histology grading of prostate
cancer: a perspective. Hum Path. 23:273–279. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Held-Warmkessel J: Contemporary Issues in
Prostate Cancer: A Nursing Perspective. Jones & Bartlett;
Learning: pp. 107–125. 2006
|
|
21
|
Bilous M, Dowsett M, Hanna W, Isola J,
Lebeau A, Moreno A, Penault-Llorca F, Rüschoff J, Tomasic G and van
de Vijver M: Current perspectives on HER2 testing: a review of
national testing guidelines. Mod Pathol. 16:173–182. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim SJ, Uehara H, Karashima T, Shepherd
DL, Killion JJ and Fidler IJ: Blockade of epidermal growth factor
receptor signaling in tumor cells and tumor-associated endothelial
cells for therapy of androgen-independent human prostate cancer
growing in the bone of nude mice. Clin Cancer Res. 9:1200–1210.
2003.
|
|
23
|
Festuccia C, Angelucci A, Gravina GL,
Biordi L, Millimaggi D, Muzi P, Vicentini C and Bologna M:
Epidermal growth factor modulates prostate cancer cell invasiveness
regulating urokinase-type plasminogen activator activity.
EGF-receptor inhibition may prevent tumor cell dissemination.
Thromb Haemost. 93:964–975. 2005.
|
|
24
|
Scher HI, Sarkis A, Reuter V, Cohen D,
Netto G, Petrylak D, Lianes P, Fuks Z, Mendelsohn J and
Cordon-Cardo C: Changing pattern of expression of the epidermal
growth factor receptor and transforming growth factor alpha in the
progression of prostatic neoplasms. Clin Cancer Res. 1:545–550.
1995.PubMed/NCBI
|
|
25
|
Shah RB, Ghosh D and Elder JT: Epidermal
growth factor receptor (ErbB1) expression in prostate cancer
progression: correlation with androgen independence. Prostate.
66:1437–1444. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Festuccia C, Gravina GL, Millimaggi D,
Muzi P, Speca S, Ricevuto E, Vicentini C and Bologna M: Uncoupling
of the epidermal growth factor receptor from downstream signal
transduction molecules guides the acquired resistance to gefitinib
in prostate cancer cells. Oncol Rep. 18:503–511. 2007.
|
|
27
|
Hernes E, Fossá SD, Berner A, Otnes B and
Nesland JM: Expression of the epidermal growth factor receptor
family in prostate carcinoma before and during
androgen-independence. Br J Cancer. 90:449–454. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bartlett JM, Brawley D, Grigor K, Munro
AF, Dunne B and Edwards J: Type I receptor tyrosine kinases are
associated with hormone escape in prostate cancer. J Pathol.
205:522–529. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Morote J, de Torres I, Caceres C, Vallejo
C, Schwartz S Jr and Reventos J: Prognostic value of
immunohistochemical expression of the c-erbB-2 oncoprotein in
metastasic prostate cancer. Int J Cancer. 84:421–425. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Reese DM, Small EJ, Magrane G, Waldman FM,
Chew K and Sudilovsky D: HER2 protein expression and gene
amplification in androgen-independent prostate cancer. Am J Clin
Pathol. 116:234–239. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Liu HL, Gandour-Edwards R, Lara PN Jr, de
Vere White R and LaSalle JM: Detection of low level HER-2/neu gene
amplification in prostate cancer by fluorescence in situ
hybridization. Cancer J. 7:395–403. 2001.PubMed/NCBI
|
|
32
|
Carles J, Lloreta J, Salido M, Font A,
Suarez M, Baena V, Nogue M, Domenech M and Fabregat X: Her-2/neu
expression in prostate cancer: a dynamic process? Clin Cancer Res.
10:4742–4745. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ady N, Morat L, Fizazi K, Soria JC,
Mathieu MC, Prapotnich D, Sabatier L and Chauveinc L: Detection of
HER-2/neu-positive circulating epithelial cells in prostate cancer
patients. Br J Cancer. 90:443–448. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Myers RB, Srivastava S, Oelschlager DK and
Grizzle WE: Expression of p160erbB-3 and p185erbB-2 in prostatic
intraepithelial neoplasia and prostatic adenocarcinoma. J Natl
Cancer Inst. 86:1140–1145. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Vakar-Lopez F, Cheng CJ, Kim J, Shi GG,
Troncoso P, Tu SM, Yu-Lee LY and Lin SH: Up-regulation of MDA-BF-1,
a secreted isoform of ErbB3, in metastatic prostate cancer cells
and activated osteoblasts in bone marrow. J Pathol. 203:688–695.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gusterson B, Cowley G, Smith JA and Ozanne
B: Cellular localisation of human epidermal growth factor receptor.
Cell Biol Int Rep. 8:649–658. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Damjanov I, Mildner B and Knowles BB:
Immunohistochemical localization of the epidermal growth factor
receptor in normal human tissues. Lab Invest. 55:588–592.
1986.PubMed/NCBI
|
|
38
|
Dittadi R, Gion M, Pagan V, Brazzale A,
Del Maschio O, Bargossi A, Busetto A and Bruscagnin G: Epidermal
growth factor receptor in lung malignancies. Comparison between
cancer and normal tissue. Br J Cancer. 64:741–744. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Natali PG, Nicotra MR, Bigotti A, Venturo
I, Slamon DJ, Fendly BM and Ullrich A: Expression of the p185
encoded by HER2 oncogene in normal and transformed human tissues.
Int J Cancer. 45:457–461. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Press MF, Cordon-Cardo C and Slamon DJ:
Expression of the HER-2/neu proto-oncogene in normal human adult
and fetal tissues. Oncogene. 5:953–962. 1990.PubMed/NCBI
|
|
41
|
Gutierrez C and Schiff R: HER2: biology,
detection, and clinical implications. Arch Pathol Lab Med.
135:55–62. 2011.PubMed/NCBI
|
|
42
|
Agus DB, Sweeney CJ, Morris MJ, Mendelson
DS, McNeel DG, Ahmann FR, Wang J, Derynck MK, Ng K, Lyons B,
Allison DE, Kattan MW and Scher HI: Efficacy and safety of
single-agent pertuzumab (rhuMAb 2C4), a human epidermal growth
factor receptor dimerization inhibitor, in castration-resistant
prostate cancer after progression from taxane-based therapy. J Clin
Oncol. 25:675–681. 2007. View Article : Google Scholar
|
|
43
|
de Bono JS, Bellmunt J, Attard G, Droz JP,
Miller K, Flechon A, Sternberg C, Parker C, Zugmaier G,
Hersberger-Gimenez V, et al: Open-label phase II study evaluating
the efficacy and safety of two doses of pertuzumab in castrate
chemotherapy-naive patients with hormone-refractory prostate
cancer. J Clin Oncol. 25:257–262. 2007.PubMed/NCBI
|
|
44
|
Solit DB and Rosen N: Targeting HER2 in
prostate cancer: where to next? J Clin Oncol. 25:241–243. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Gallick GE, Corn PG, Zurita AJ and Lin SH:
Small-molecule protein tyrosine kinase inhibitors for the treatment
of metastatic prostate cancer. Future Med Chem. 4:107–119. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Chen L, Mooso BA, Jathal MK, Madhav A,
Johnson SD, van Spyk E, Mikhailova M, Zierenberg-Ripoll A, Xue L,
Vinall RL, et al: Dual EGFR/HER2 inhibition sensitizes prostate
cancer cells to androgen withdrawal by suppressing ErbB3. Clin
Cancer Res. 17:6218–6228. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Stigbrand T, Carlsson J and Adams GP:
Developmental trends in targeted radionuclide therapy - biological
aspects. Targeted Radionuclide Tumor Therapy, Biological Aspects.
Stigbrand T, Adams G and Carlsson J: Springer Verlag; pp. 387–397.
2008, View Article : Google Scholar
|
|
48
|
Frejd YF: Novel alternative scaffolds and
their potential use for tumor targeted radionuclide therapy.
Targeted Radionuclide Tumor Therapy, Biological Aspects. Stigbrand
T, Adams G and Carlsson J: Springer Verlag; pp. 89–116. 2008,
View Article : Google Scholar
|
|
49
|
Govindan SV and Goldenberg DM: New
antibody conjugates in cancer therapy. Scientific World Journal.
10:2070–2089. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Adams GP and Weiner LM: Monoclonal
antibody therapy of cancer. Nat Biotechnol. 23:1147–1157. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Gedda L, Fondell A, Lundqvist H, Park JW
and Edwards K: Experimental radionuclide therapy of HER2-expressing
xenografts using two-step targeting nuclisome particles. J Nucl
Med. 53:480–487. 2012. View Article : Google Scholar : PubMed/NCBI
|