Introduction
Colorectal cancer (CRC) is the third most common
cancer in males and the second most common cancer in females
worldwide (1). In the Kashmir
valley, CRC represents the third most common gastrointestinal
cancer following esophageal and gastric cancer (2–4).
The Kashmiri population is exposed to a particular
set of environmental and dietary risks, including exposure to
nitroso compounds, amines and nitrates reported to be present in
local foodstuffs, the majority of which have been shown to contain
significant irritants and carcinogens (2,3,5,6).
Genetic polymorphisms in DNA repair genes, which
lead to amino acid substitution, may influence individual capacity
to repair DNA damage, which may be associated with increased
genetic instability and carcinogenesis (7). In mammalian cells, four major DNA
repair pathways have been identified: base excision repair (BER),
nucleotide excision repair (NER), double-strand break repair and
mismatch repair (8,9).
The DNA repair gene XRCC1, located at
19q13.2, codes for a scaffolding protein physically associated with
DNA polymerase β, DNA ligase III, human AP endonuclease,
polynucleotide kinase and poly (ADP-ribose) polymerase (8,10,11),
which function in a complex to facilitate BER and single-strand
break repair processes. The BER pathway mainly removes non-bulky
base adducts produced by methylation, oxidation or reduction by
ionizing radiation or oxidative damage (12). The XRCC1 protein is capable
of binding directly to both gapped and nicked DNA, as well as to
gapped DNA associated with DNA polymerase β, suggesting that this
protein may be independently involved in DNA damage recognition
(13).
Three polymorphisms occurring at conserved sequences
in the XRCC1 gene have been reported, and amino acid
substitutions were detected at codons 194 (Arg>Trp), 280
(Arg>His) and 399 (Arg>Gln) (14). Out of the 3 polymorphisms, the
XRCC1 codon 399 polymorphism has been studied most widely in
a number of cancers but with varied results (15–23).
While an increased risk has been reported in lung cancer (22) and breast cancer (17,18),
there is no definite correlation between XRCC1 339 status
and the risk of CRC. Abdel-Rahman et al(15) were the first to report that the
XRCC1 399Gln allele, similarly to the XRCC1
399Arg/Arg genotype, was associated with an increased risk of
developing CRC, particularly amongst young urban residents;
however, these results were not reproducible and have not been
demonstrated in any other population since. Stern et
al(24) reported that the
399SNP of the XRCC1 gene plays a role in modifying the risk
of CRC by interactions with fatty acids of the diet. There are also
some contradictory reports such as that of Mort et
al(20), who reported no
correlation between CRC risk and polymorphisms in any of the 4 NER
genes or in XRCC1. Yeh et al(21) investigated the involvement of the
DNA repair pathway genes in modulating the risk of CRC in a
Taiwanese population and found the Arg 399 form to cause an
increased cancer risk. Similarly, Skjelbred et
al(2006)(23) reported a
decreased risk of CRC with the Gln399 genotype. More recently, in a
study by Wang et al(2010) in a South East Indian population
(25), the XRCC1 Gln399
allele was found to significantly increase the risk of rectal
cancer. In the present study, we conducted a hospital-based
case-controlled investigation to evaluate the potential impact of
the XRCC1 Arg399Gln gene polymorphism on the risk of CRC in
a Kashmiri population. We also investigated whether there was a
correlation between the clinicopathological variables and the
XRCC1 variant genotype (Gln/Gln), and hence its role in
modulating the risk of CRC.
Materials and methods
Study population
This study included 130 CRC cases. All patients were
recruited from the Department of General Surgery, Sher-I-Kashmir
Institute of Medical Sciences, Kashmir, India. Blood samples were
collected from 160 ageand gender-matched individuals with no signs
of any malignancy to serve as external controls. The mean age in
the patient and control groups was 53 years (Table I).
 | Table IGenotype frequencies of the
XRCC1 gene polymorphism in CRC cases and controls. |
Table I
Genotype frequencies of the
XRCC1 gene polymorphism in CRC cases and controls.
| XRCC1
genotype | CRC cases
(n=130) | Controls
(n=150) | OR (95% CI); P¥;
Fψ | χ2;
P-value (overall) |
|---|
| GG (wild) | 63 (48.5%) | 75 (50.0%) | 1 | 0.40; 0.81 |
| AG
(heterozygous) | 37 (28.5%) | 30 (20.0%) | 1.47 (0.82–2.64);
0.19; 0.23 | |
| AA (variant) | 30 (23.0%) | 45 (30.0%) | 0.79 (0.44–1.4);
0.43; 0.47 | |
Data on all CRC patients were obtained from personal
interviews with patients and/or their guardians, and their medical
records. All patients and/or guardians were informed about the
study and their willingness to participate was recorded on a
predesigned questionnaire (available on request). The collection
and use of blood samples (from patients and controls) for this
study had been previously approved by the appropriate institutional
ethics committee.
DNA extraction and polymerase chain
reaction
DNA extraction was performed using the ammonium
precipitation method. Genotyping for the XRCC1 R399Q
polymorphism was determined using a method described previously
(25). The oligonucleotide primers
used for the amplification of the target region were: forward
F-5′-TTG TGC TTT CTC TGT GTC CA-3′ and reverse R-5′-TCC TCC AGC CTT
TTC TGA TA-3′, which generated a 615-bp fragment.
The polymerase chain reaction (PCR) was carried out
in a final volume of 20 μl, containing 50 ng genomic DNA
template, 1X PCR buffer (Fermentas, Glen Burnie, MD, USA), with 2
mM MgCl2, 0.5 μM of each primer (Sigma-Aldrich,
Bangalore, India), 50 μM deoxynucleotide triphosphates
(dNTPs; Cinnagen, Tehran, Iran) and 0.25 units of DNA polymerase
(Invitrogen, Bangalore, India). For PCR amplification, the standard
programme was used as follows: one initial denaturation step at
94°C for 7 min, followed by 40 denaturation cycles of 30 sec at
94°C, 30 sec of annealing at 57°C and 30 sec of extension at 72°C
for 40 cycles, followed by a final elongation cycle at 72°C for 7
min.
The PCR product of XRCC1 was then digested
with 2 units of MspI in a reaction mixture of 20 μl
for 3 h at 37°C. The Arg allele revealed 374 and 241-bp fragments,
while the Gln allele was not digested (indicative of the absence of
the MspI cutting site; Fig.
1).
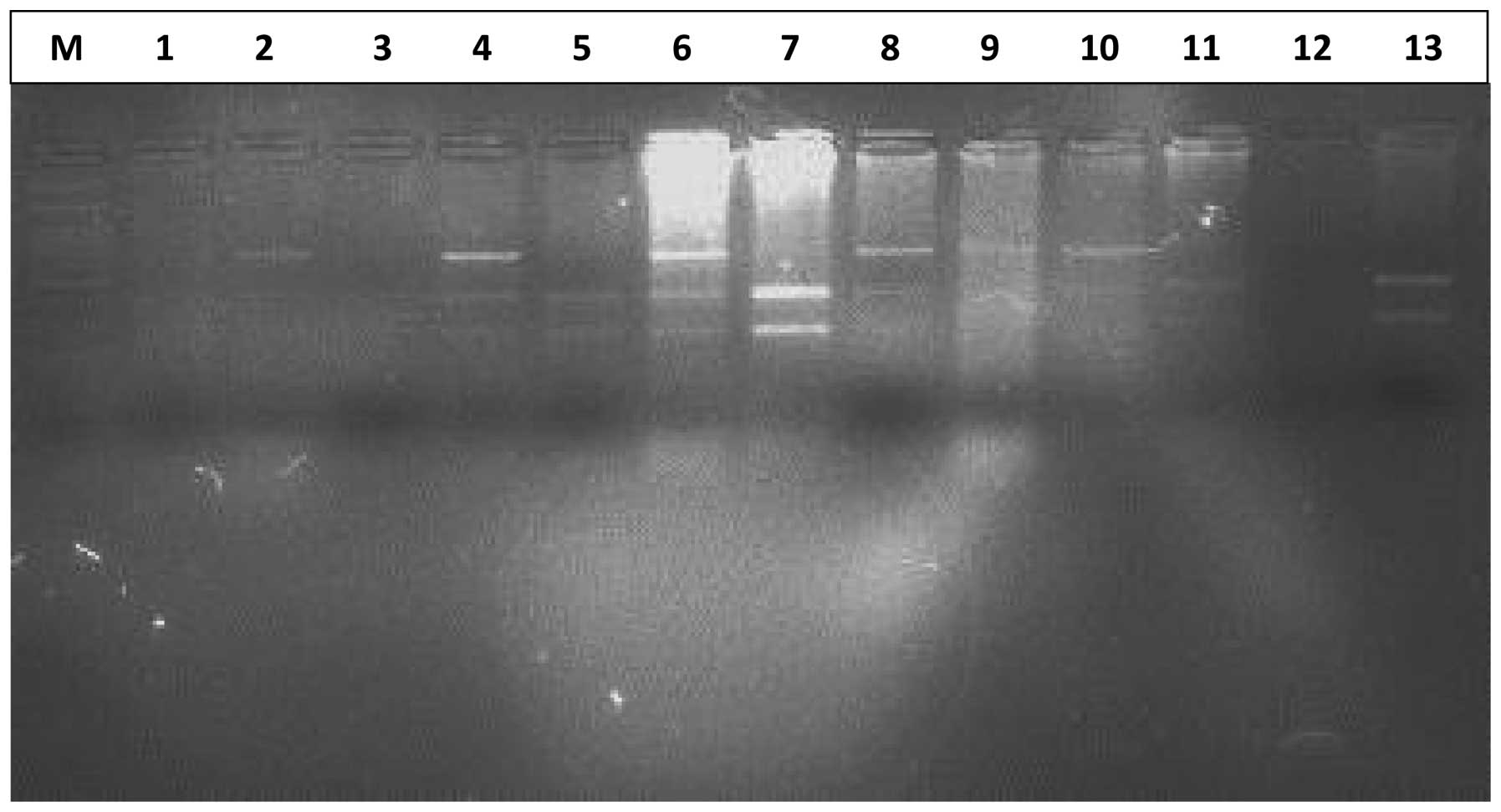 | Figure 1Representative gel of XRCC1
Arg399Gln polymorphism, showing MspI digested amplicons. The Arg
allele is represented by 374 and 241-bp fragments, while the Gln
allele is represented by a 615-bp band. Lane M, 100-bp ladder;
lanes 2, 9 and 10, homozygous (Gln/Gln) genotype (615 bp); lanes 5,
7, 11 and 13, homozygous (Arg/Arg) genotype (374 and 241 bp); lanes
4, 6 and 8, homozygous (CC) genotype (615, 374 and 241 bp). |
DNA amplicons, as well as the digestion products,
were electrophoresed through a 2–3% agarose gel (Genie, Bangalore,
India) for resolution. The genotypes of >20% of the samples were
reassessed in a double-blind manner by two independent researchers,
to confirm the results. A random sample of 10% of each genotype was
re-checked with sequencing to confirm the results.
Statistical analysis
The observed frequencies of genotypes in CRC
patients were compared with controls using the Chi-square test, or
Fisher’s exact test when the expected frequencies were small. The
Chi-square test was used to verify whether the genotype
distributions were in Hardy-Weinberg equilibrium. P≤0.05 was
considered to indicate a statistically significant result.
Statistical analyses were performed using PASW version 18
software.
Results
A total of 130 CRC cases and 150 control subjects
were included in this study. The CRC patients consisted of 76 males
and 54 females (M/F ratio, 1.41) and the control subjects consisted
of 88 males and 72 females (M/F ratio, 1.2; data not shown). The
mean age in both the patient and control groups was 53 years. No
significant gender- or age-related differences were observed
between the groups (P>0.05). Furthermore, out of 130 confirmed
cases of CRC, 125 cases were sporadic, 4 were familial adenomatous
polyposis and one case was hereditary non-polyposis (Lynch
syndrome) CRC. All but one CRC case had adenocarcinoma and one had
squamous cell carcinoma of the basal cell type. Fifty-two cases had
carcinoma in the colon and 78 had carcinoma in the rectum; 78 were
rural and 39 urban, and 81 were smokers and 49 non-smokers
(Table II).
| Table IIAssociation between the XRCC1
polymorphism and clinicopathological characteristics. |
Table II
Association between the XRCC1
polymorphism and clinicopathological characteristics.
| | No. of cases
(n=130)a
| |
|---|
| Variables | No. (%) | GG (n=63) | AG (n=37) | AA (n=30) | χ2;
P-value |
|---|
| Age group | | | | | |
| ≤50 | 48 (36.9) | 14 | 20 | 14 | 11.73;
0.002 |
| >50 | 82 (63.1) | 49 | 17 | 16 | |
| Gender | | | | | |
| Female | 54 (41.54) | 22 | 12 | 20 | 10.20;
0.006 |
| Male | 76 (58.46) | 41 | 25 | 10 | |
| Dwelling | | | | | |
| Rural | 91 (70.0) | 36 | 33 | 22 | 11.61;
0.003 |
| Urban | 39 (30.0) | 27 | 4 | 8 | |
| Smoking status | | | | | |
| Ever | 81 (62.3) | 41 | 23 | 17 | 0.61; 0.737 |
| Never | 49 (37.7) | 22 | 14 | 13 | |
| Tumor location | | | | | |
| Colon | 52 (40.0) | 17 | 22 | 13 | 10.42;
0.005 |
| Rectum | 78 (60.0) | 46 | 15 | 17 | |
| Nodal status | | | | | |
| Involved | 88 (67.7) | 50 | 18 | 20 | 10.08;
0.006 |
| Not involved | 42 (32.3) | 13 | 19 | 10 | |
| Tumor grade | | | | | |
| WD | 98 (75.4) | 48 | 28 | 22 | 0.09;
0.956 |
| MD+PD | 32 (24.6) | 15 | 9 | 8 | |
Among the CRC cases, we found the frequency of the
XRCC1 genotype to be 48.5% GG (63/130), 28.5% AG (37/130)
and 23.0% AA (30/130), while the frequency in the general control
population was 50.0% GG (75/150), 20.0% AG (30/150) and 30.0% AA
(45/150). The overall association between the XRCC1
polymorphism and the CRC cases was found to be non-significant
(P>0.05; Table II). Furthermore,
an independent analysis for the AG and AA genotypes revealed a
significant correlation with the risk of CRC (P<0.05). The
overall hazard ratio of the XRCC1 A allele in CRC was 0.79
(95% CI, 0.44–1.4).
The correlation of the XRCC1 polymorphic
status with the clinicopathological characteristics was also
carefully analyzed. We found a significant association (P<0.05)
of the A allele with the age, gender, dwelling, tumor location,
nodal status and tumor grade of the patients (P<0.05; Table II).
Discussion
In this hospital-based case-control study of CRC
patients in Kashmir, we analyzed the polymorphism of the XRCC1
R399Q gene, a DNA repair gene, and its concomitant role in
modulating the risk of CRC.
The XRCC1 gene belongs to a DNA repair gene
family and encodes for a protein which plays a role in the repair
of single-strand breaks (SSB) and in base excision repair (BER)
(23). Shen et al(14) first of all reported the three common
polymorphisms for the XRCC1 gene occurring at its conserved
sequences, all of which affect the coding region of the gene. These
coding polymorphisms result in amino acid substitutions affecting
the overall activity of the synthesized proteins, which are
reported to affect codons 194 (Arg>Trp), 280 (Arg>His) and
399 (Arg>Gln) (23).
We found noteworthy results in our population
comparable to those of Abdel-Rahman et al(15), since we found the frequency of the
XRCC1 genotype to be 48.5% GG (63/130), 28.5% AG (37/130)
and 23.0% AA (30/130) in CRC cases. This frequency distribution is
also comparable to that observed in the study of Wang et
al(25).
In the case of the XRCC1 Arg194Trp
polymorphism, a few studies reported a reduced risk of cancer
associated with the 194Trp variant form (16) while another study by Skjelbred et
al(23) reported no association
of the codon 194 polymorphism with the risk of CRC. In one of the
studies, which involved the investigation of the XRCC1
Arg280His allele and the risk of cancer, no association was
observed (19). The XRCC1
Arg399Gln polymorphism has been well studied in many cancers and
positive correlations have been established; however, the results
from these studies are not consistent (15,17,19–21,26).
The Arg399Gln polymorphism of the XRCC1 gene
resides at the C-terminal side of the poly (ADP-ribose) polymerase
interacting domain which has been indicated as a protein-protein
interaction module in many proteins involved in DNA repair
mechanisms in the cell (27).
The majority of epidemiological case-control studies
did not find any significant correlation between the XRCC1
399Gln variant and the risk of CRC (23,24,28,29),
However, a case-control study carried out on a Taiwanese population
found that an increased risk of CRC correlated with the
XRCC1 399Arg/Arg genotype when compared with the
XRCC1 399Gln in younger subjects (21). Although a study on a Norwegian
population by Skjelbred et al(23) reported the XRCC1 399Gln
allele to be related to a reduction in the incidence of high-risk
adenomas, there was no association with any risk of carcinomas. In
contrast to these reports, Abdel-Rahman et al(15) observed a significantly increased
risk of CRC with the XRCC1 399Gln allele in their study on
an Egyptian population and this effect was shown to be more
significant among urban residents. In addition, Hong et
al(19) demonstrated a positive
association for this polymorphism in their study on a South Korean
population.
Although our study on a Kashmiri population did not
find any significant correlation between the XRCC1 Arg399Gln
polymorphism and an increased risk of CRC, similarly to many of the
already reported studies, we did find an increased risk of CRC
among Arg/Gln heterozygous cases compared to the controls (OR=1.47;
95% CI, 0.82–2.64). We also found a significant correlation between
the 399Gln allele and the various clinicopathological parameters
(Table II), particularly for gender
(females), dwelling (rural) and tumor location (rectum). As already
noted by Wang et al(25),
differences due to gender may arise either due to physiologically
different effects of the XRCC1 399Gln allele or due to
different dietary habits, lifestyles and other genetic factors.
The interaction of the polymorphism with various
environmental factors causes an increase in the overall
susceptibility to CRC in any population (30,31).
Therefore, we also hypothesize that since our population is exposed
to certain environmental and dietary risks, including the
consumption of sun-dried and smoked fish and meat, dried and
pickled vegetables, red chilli, hakh (a leafy vegetable of the
Brassica family), hot noon chai (salted tea) and hukka (water pipe)
smoke (2,3,5), these
may play a significant role in modulating the effect of the
polymorphism in a dominant model of inheritance. As previously
reported, the etiology and incidence of various gastrointestinal
cancers in this population has been attributed to probable exposure
to nitroso compounds, amines and nitrates, reported to be present
in local foodstuffs, the majority of which have been shown to
contain significant irritants and carcinogens (6).
The effect of 399Gln is also increasingly amplified
in the carriers due to the impairment (or reduction) of the repair
pathways, which in turn is reflected in significantly higher DNA
adduct levels and an increased sister chromosome exchange frequency
when compared with 399Arg (32).
We conclude that there is a significant correlation
between the XRCC1 A870G polymorphism and the risk of CRC in
the ethnic Kashmiri population. These correlations now need to be
authenticated in a large sample study, in order to discern racial
differences and determine the aggressiveness of CRC.
Acknowledgements
The authors wish to thank the CRC
patients who took part in this study and cooperated during the
interview and sample collection. The authors gratefully acknowledge
the financial support provided by the Sher-I-Kashmir Institute of
Medical Sciences, Kashmir, for this study. We also thank the head
and technical staff of the operating theatre in the Department of
General Surgery at Sher-I-Kashmir Institute of Medical Sciences who
helped us with tissue procurement, and the anonymous pathologists
in the Department of Pathology, Sher-I-Kashmir Institute of Medical
Sciences, for the histo-pathological assessment of the tumor
tissues.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E, et al: Global cancer statistics. CA Cancer J Clin. 61:69–90.
2011. View Article : Google Scholar
|
|
2
|
Sameer AS, Nissar S, Abdullah S, Chowdri
NA and Siddiqi MA: DNA repair gene 8-oxoguanine DNA glycosylase
Ser326Cys polymorphism and colorectal cancer risk in a Kashmiri
population. DNA Cell Biol. 31:541–546. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sameer AS, Shah ZA, Nissar S, Mudassar S
and Siddiqi MA: Risk of colorectal cancer associated with the
methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism in
the Kashmiri population. Genet Mol Res. 10:1200–1210. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Javid G, Zargar SA, Rather S, Khan AR,
Khan BA, et al: Incidence of colorectal cancer in Kashmir valley,
India. Indian J Gastroenterol. 30:7–11. 2011. View Article : Google Scholar
|
|
5
|
Rasool S, Ganai BA, Kadla SA, Ahanger AG,
Qazi F, et al: The ECRG1 290Arg/Gln polymorphism is related to risk
of esophageal squamous cell carcinoma in Kashmir. Asian Pac J
Cancer Prev. 12:265–269. 2011.PubMed/NCBI
|
|
6
|
Siddiqi M, Kumar R, Fazili Z,
Spiegelhalder B and Preussmann R: Increased exposure to dietary
amines and nitrate in a population at high risk of oesophageal and
gastric cancer in Kashmir (India). Carcinogenesis. 13:1331–1335.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
de Boer JG: Polymorphisms in DNA repair
and environmental interactions. Mutat Res. 509:201–210. 2002.
|
|
8
|
Yu Z, Chen J, Ford BN, Brackley ME and
Glickman BW: Human DNA repair systems: an overview. Environ Mol
Mutagen. 33:3–20. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Christmann M, Tomicic MT, Roos WP and
Kaina B: Mechanisms of human DNA repair: an update. Toxicology.
193:3–34. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wood RD, Mitchell M, Sgouros J and Lindahl
T: Human DNA repair genes. Science. 291:1284–1289. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Caldecott KW, Aoufouchi S, Johnson P and
Shall S: XRCC1 polypeptide interacts with DNA polymerase beta and
possibly poly (ADP-ribose) polymerase, and DNA ligase III is a
novel molecular ‘nick-sensor’ in vitro. Nucleic Acids Res.
24:4387–4394. 1996.PubMed/NCBI
|
|
12
|
Duarte MC, Colombo J, Rossit AR, Caetano
A, Borim AA, Wornrath D and Silva AE: Polymorphisms of DNA repair
genes XRCC1 and XRCC3, interaction with environmental exposure and
risk of chronic gastritis and gastric cancer. World J
Gastroenterol. 11:6593–6600. 2005.PubMed/NCBI
|
|
13
|
Marintchev A, Mullen MA, Maciejewski MW,
Pan B, Gryk MR and Mullen GP: Solution structure of the
single-strand break repair protein XRCC1 N-terminal domain. Nat
Struct Biol. 6:884–893. 1999. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shen MR, Jones IM and Mohrenweiser H:
Nonconservative amino acid substitution variants exist at
polymorphic frequency in DNA repair genes in healthy humans. Cancer
Res. 58:604–608. 1998.PubMed/NCBI
|
|
15
|
Abdel-Rahman SZ, Soliman AS, Bondy ML,
Omar S, El-Badawy SA, Khaled HM, Seifeldin IA and Levin B:
Inheritance of the 194Trp and the 399Gln variant alleles of the DNA
repair gene XRCC1 are associated with increased risk of early-onset
colorectal carcinoma in Egypt. Cancer Lett. 159:79–86. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Goode EL, Ulrich CM and Potter JD:
Polymorphisms in DNA repair genes and associations with cancer
risk. Cancer Epidemiol Biomarkers Prev. 11:1513–1530.
2002.PubMed/NCBI
|
|
17
|
Nexo BA, Vogel U, Olsen A, Ketelsen T,
Bukowy Z, Thomsen BL, Wallin H, Overvad K and Tjonneland A: A
specific haplotype of single nucleotide polymorphisms on chromosome
19q13.2-3 encompassing the gene RAI is indicative of
post-menopausal breast cancer before age 55. Carcinogenesis.
24:899–904. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Moullan N, Cox DG, Angele S, Romestaing P,
Gerard JP and Hall J: Polymorphisms in the DNA repair gene XRCC1,
breast cancer risk, and response to radiotherapy. Cancer Epidemiol
Biomarkers Prev. 12:1168–1174. 2003.PubMed/NCBI
|
|
19
|
Hong YC, Lee KH, Kim WC, Choi SK, Woo ZH,
Shin SK and Kim H: Polymorphisms of XRCC1 gene, alcohol consumption
and colorectal cancer. Int J Cancer. 116:428–432. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mort R, Mo L, McEwan C and Melton DW: Lack
of involvement of nucleotide excision repair gene polymorphisms in
colorectal cancer. Br J Cancer. 89:333–337. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yeh C-C, Sung F-C, Tang R, Chang-Chieh C
and Hsieh L-L: Polymorphisms of the XRCC1, XRCC3, & XPD genes,
and colorectal cancer risk: a case-control study in Taiwan. BMC
Cancer. 5:122005.
|
|
22
|
Ratnasinghe D, Yao SX, Tangrea JA, Qiao
YL, Andersen MR, Barrett MJ, Giffen CA, Erozan Y, Tockman MS and
Taylor PR: Polymorphisms of the DNA repair gene XRCC1 and lung
cancer risk. Cancer Epidemiol Biomarkers Prev. 10:119–123.
2001.PubMed/NCBI
|
|
23
|
Skjelbred CF, Saebø M, Wallin H, Nexø BA,
Hagen PC, Lothe IM, Aase S, Johnson E, Hansteen IL, Vogel U and
Kure EH: Polymorphisms of the XRCC1, XRCC3 and XPD genes and risk
of colorectal adenoma and carcinoma, in a Norwegian cohort: a case
control study. BMC Cancer. 6:672006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Stern MC, Siegmund KD, Corral R and Haile
RW: XRCC1 and XRCC3 polymorphisms and their role as effect
modifiers of unsaturated fatty acids and antioxidant intake on
colorectal adenomas risk. Cancer Epidemiol Biomarkers Prev.
14:609–615. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang J, Zhao Y, Jiang J, Gajalakshmi V,
Kuriki K, Nakamura S, Akasaka S, Ishikawa H, Suzuki S, Nagaya T and
Tokudome S: Polymorphisms in DNA repair genes XRCC1, XRCC3 and XPD,
and colorectal cancer risk: a case-control study in an Indian
population. J Cancer Res Clin Oncol. 136:1517–1525. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Vogel U, Nexo BA, Wallin H, Overvad K,
Tjonneland A and Raaschou-Nielsen O: No association between base
excision repair gene polymorphisms and risk of lung cancer. Biochem
Genet. 42:453–460. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Masson M, Niedergang C, Schreiber V,
Muller S, Menissier-de Murcia J and de Murcia G: XRCC1 is
specifically associated with poly (ADP-ribose) polymerase and
negatively regulates its activity following DNA damage. Mol Cell
Biol. 18:3563–3571. 1998.PubMed/NCBI
|
|
28
|
Sliwinski T, Krupa R,
Wisniewska-Jarosinska M, Lech J, Morawiec Z, Chojnacki J and
Blasiak J: No association between the Arg194Trp and Arg399Gln
polymorphisms of the XRCC1 gene and colorectal cancer risk and
progression in a Polish population. Exp Oncol. 30:253–254.
2008.PubMed/NCBI
|
|
29
|
Improta G, Sgambato A, Bianchino G, Zupa
A, Grieco V, La Torre G, Traficante A and Cittadini A:
Polymorphisms of the DNA repair genes XRCC1 and XRCC3 and risk of
lung and colorectal cancer: a case-control study in a Southern
Italian population. Anticancer Res. 28:2941–2946. 2008.PubMed/NCBI
|
|
30
|
Zhang LQ, Huang X, Wang J, Shang JQ, Bai
J, et al: The cyclin D1 G870A polymorphism and colorectal cancer
susceptibility: a meta-analysis of 20 populations. Asian Pacific J
Cancer Prev. 12:81–85. 2011.
|
|
31
|
Palmqvist R, Stenling R, Oberg A, et al:
Expression of cyclin D1 and retinoblastoma protein in colorectal
cancer. Eur J Cancer. 34:1575–1581. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lunn RM, Langlois RG, Hsieh LL, Thompson
CL and Bell DA: XRCC1 polymorphisms: effects on aflatoxin B1-DNA
adducts and glycophorin A variant frequency. Cancer Res.
59:2557–2561. 1999.PubMed/NCBI
|














