Introduction
Lung cancer is the leading cause of cancer-related
mortality worldwide. Platinum-based chemotherapy is recommended as
a front-line chemotherapy for advanced non-small cell lung cancer
(NSCLC) (1). The results of the
Four Arms Comparative Study, which analyzed 4 platinum-doublet
regimens as front-line therapies for advanced NSCLC, demonstrated
that the 4 regimens had similar efficacy (2,3). Thus,
carboplatin and paclitaxel combination therapy has been recognized
as a reference regimen based on its feasibility. In the standard
schedule, 200 mg/m2 paclitaxel and carboplatin [area
under the curve (AUC)=6] are administered on day 1 every 3 weeks.
However, several weekly schedules have been investigated to reduce
hematological toxicities (4–6).
Hirabayashi et al also reported a weekly schedule based on
the metronomic theory (7). In this
weekly schedule, 70 mg/m2 paclitaxel on days 1, 8 and
15, and AUC=6 of carboplatin on day 1 were administered every 4
weeks. All the studies, including the present study, demonstrated
that a weekly schedule reduced neutropenia and displayed a
comparable survival benefit compared to the standard schedule.
The survival benefit of treatment-related
neutropenia has been discussed in previous studies (8–11).
Consequently, a treatment schedule correlated with a reduced
incidence of neutropenia ought to be an unfavorable predictive
factor for overall survival (OS). However, a weekly schedule
associated with reduced neutropenia demonstrated a comparable
survival benefit to the standard schedule. Notably, there has been
no integrated analysis comparing the 2 schedules and concurrently
considering the worst grade of treatment-related hematological
toxicities. Therefore, we performed a retrospective analysis in
unselected patients who received standard tri-weekly or weekly
carboplatin in combination with paclitaxel to obtain complimentary
information regarding whether the treatment schedule and
treatment-related hematological toxicities were correlated with
survival outcome.
Patients and methods
Data collection
The medical records of all patients with NSCLC who
were treated between January 1999 and December 2010 at Kansai
Medical University Takii Hospital (Moriguchi, Japan) were
retrospectively reviewed; institutional review board approval was
obtained for this study. The patients were included in this study
if they had advanced NSCLC (stage IIIB or IV) that was treated with
front-line combination chemotherapy including carboplatin and
paclitaxel. The patients were assigned to 1 of 2 groups; the weekly
arm group (weekly schedule) and the standard arm group (standard
tri-weekly schedule). The clinical stage was assigned on the basis
of the Sixth Edition of the TNM Classification for Lung Cancer
(12,13). Data including gender, age, smoking
history, clinical stage, histological cancer type, history of
administration of an epidermal growth factor receptor tyrosine
kinase inhibitor (EGFR-TKI), Eastern Cooperative Oncology Group
(ECOG) performance status (PS), progression-free survival (PFS) and
OS were obtained retrospectively from the patient medical records.
There was no distinction between gefitinib and erlotinib, and both
agents were considered as EGFR-TKIs. Patients who underwent
previous palliative radiation treatment, including whole-brain
irradiation without curative intention, were included. The
crossover cases in the consecutive treatment courses between the
weekly and standard arms were excluded, as well as patients with
large cell neuroendocine carcinoma. All patients provided informed
consent prior to receiving front-line chemotherapy. The study was
performed according to the Declaration of Helsinki and was approved
by the Institutional Ethics Review Board (the Clinical Research
Board of Kansai Medical University Takii Hospital; ID No,
23-6).
Statistical analysis
Differences between the groups were compared using
the χ2 or Fisher’s exact test. OS was defined as the
time from the start of front-line systemic chemotherapy to the time
of death from any cause or the date the patient was last known to
be alive. PFS was defined as the time between the start of
treatment and disease progression, death or the last known
follow-up. The treatment-related adverse effects were evaluated
using the Common Terminology Criteria for Adverse Events version
4.0 (14). Objective tumor
responses to chemotherapy were evaluated using the Response
Evaluation Criteria in Solid Tumors version 1.0 (15). The objective response rate (ORR) was
defined as the number of patients displaying a complete response
(CR) or a partial response (PR), with respect to the total number
of patients evaluated. The disease control rate (DCR) was defined
as the number of patients displaying a CR, a PR or stable disease
(SD), with respect to the total number of patients evaluated. The
minimum time interval between the 2 measurements required for the
determination of SD was 6 weeks. The 95% confidence intervals (95%
CIs) for the ORR and DCR were calculated using a binomial
distribution. The univariate and multivariate analyses of PFS and
OS were performed with the Kaplan-Meier product-limit method using
the log-rank test and the Cox proportional hazards model,
respectively. The 95% CI for the survival rate was calculated using
Greenwood’s method, and that of the median survival time (MST) was
caluclated by the Brookmeyer and Crowley method. All statistical
analyses were conducted using JMP (version 9.0.2) software for
Windows (SAS Institute Inc, Cary, NC). All statistical tests were
two-sided, and P<0.05 was considered to indicate a statistically
significant difference.
Treatment plan
In the weekly arm (weekly schedule), 70
mg/m2 paclitaxel was administered on days 1, 8 and 15
together with carboplatin (AUC=6) on day 1 of each 4-week cycle. In
the standard arm (standard tri-weekly schedule), 200
mg/m2 paclitaxel was administered with carboplatin
(AUC=6) on day 1 of each 3-week cycle. Thirty minutes prior to
paclitaxel administration, the patients were treated with the
following premedications: dexamethasone (20 mg), diphenhydramine
(50 mg and a histamine receptor 2 (H2) blocker. The patients in the
weekly arm were permittted to have their premedications altered to
dexamethasone (8 mg), diphenhydramine (50 mg) and an H2 blocker.
The glomerular filtration rate was substituted by the calculated
value using the Cockroft equation. The treatment was continued up
to a maximum of 6 cycles or until disease progression in both
arms.
Results
Patient characteristics
A total of 402 patients with NSCLC were treated in
our hospital between January 1999 and December 2010. Of the 218
patients with advanced-stage disease, 167 met the eligibility
criteria. The characteristics of these 167 patients are summarized
in Table I. All patients were Asian
(Japanese, Korean or Chinese), the median patient age was 65 years
(range, 31–79 years) and patients comprised 42 females and 125
males. The numbers of patients with adenocarcinoma, squamous cell
carcinoma, large cell carcinoma and other types of carcinoma were
118, 44, 4 and 1, respectively. The weekly and standard arm
regimens were used as front-line chemotherapies in 73 and 94
patients, respectively. In 108 patients, ≥1 regimen of
chemotherapy, including EGFR-TKI, was administered following the
front-line chemotherapy. A history of EGFR-TKI treatment was
reported in 66 patients, whereas the remaining 101 patients had not
received EGFR-TKI treatment. There were no significant differences
in age, gender, PS, clinical stage and smoking history between the
2 groups.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Characteristics | Weekly arm
(n=73) | Standard arm
(n=94) | P-value |
|---|
| Age (years) | | | 0.2361 |
| Median | 64 | 65.5 | |
| Range | 31–78 | 32–79 | |
| Gender | | | 0.3723 |
| Female | 21 | 21 | |
| Male | 52 | 73 | |
| ECOG PS | | | 0.5402 |
| 0–2 | 61 | 85 | |
| 3 or 4 | 12 | 9 | |
| Smoking history | | | 0.7300 |
| Never smoked | 19 | 27 | |
| Past or current
smoker | 54 | 67 | |
| Histological
diagnosis | | | 0.1581a |
| Squamous cell
carcinoma | 15 | 29 | |
| Adenocarcinoma | 57 | 61 | |
| Large cell
carcinoma | 1 | 3 | |
| Other | 0 | 1 | |
| Initial clinical
stage | | | 0.5890 |
| IIIB | 19 | 21 | |
| IV | 54 | 73 | |
| EGFR-TKI
treatment | | | 0.2667 |
| Not used | 41 | 60 | |
| Used | 32 | 34 | |
| Objective
response | | | |
| CR | 1 | 2 | |
| PR | 26 | 28 | |
| SD | 27 | 40 | |
| PD | 19 | 24 | |
| ORR (%) | 37.0 | 31.9 | 0.5143 |
| DCR (%) | 74.0 | 74.5 | 1.000 |
Treatment-related adverse effects
The treatment-related grade 2 or worse adverse
effects observed in this study are summarized in Table II. Grade 3 or 4 neutropenia was
observed in 37.0 and 70.2% of the patients in the weekly and
standard arms, respectively, indicating that severe (grade 3 or 4)
neutropenia was significantly more frequent in the standard arm
(P<0.0001). Grade 3 or 4 thrombocytopenia was observed in 11.0
and 12.8% of the patients in the weekly and standard arms,
respectively (P=0.8127). Grade 3 or 4 peripheral neuropathy was
observed in 0% and 8.5% of the patients in the weekly and standard
arms, respectively (P=0.0188). Grade 4 neuropathy was not observed
in the weekly arm, although it was observed in 3.2% of patients in
the standard arm. The other hematological or non-hematological
adverse effects observed were found to be moderate and manageable
in both groups.
| Table IIAdverse events (≥grade 2) according to
the treatment schedule. |
Table II
Adverse events (≥grade 2) according to
the treatment schedule.
| Weekly arm (n=73)
| Standard arm (n=94)
| |
|---|
| Toxicity | G2 | G3 | G4 | ≥G3 (%) | G2 | G3 | G4 | ≥G3 (%) | P-value |
|---|
| Hematological | | | | | | | | | |
| Neutropenia | 15 | 19 | 8 | 37.0 | 6 | 25 | 41 | 70.2 | <0.0001a |
|
Thrombocytopenia | 7 | 5 | 3 | 11.0 | 22 | 8 | 4 | 12.8 | 0.8127 |
| Anemia | 34 | 9 | 6 | 20.5 | 38 | 17 | 9 | 27.7 | 0.4651 |
|
Nonhematological | | | | | | | | | |
| Neuropathy | 0 | 0 | 0 | 0.0 | 9 | 5 | 3 | 8.5 | 0.0188a |
| Transaminase | 7 | 1 | 0 | 1.4 | 5 | 4 | 0 | 4.3 | 0.3875 |
| Total
bilirubin | 0 | 0 | 0 | 0.0 | 5 | 2 | 1 | 3.2 | 0.2574 |
| Serum
creatinine | 3 | 0 | 0 | 0.0 | 5 | 0 | 0 | 0.0 | n.d. |
Tumor response
The tumor responses are listed in Table I. The ORRs of the weekly and
standard arms were 37.0% (95% CI, 26.0–49.1) and 31.9% (95% CI,
22.7–42.3), respectively. The DCRs of the weekly and standard arms
were 74.0% (95% CI, 62.4–83.6) and 74.5% (95% CI, 64.4–82.9),
respectively. There were no significant differences in ORR and DCR
between the 2 groups.
Survival data
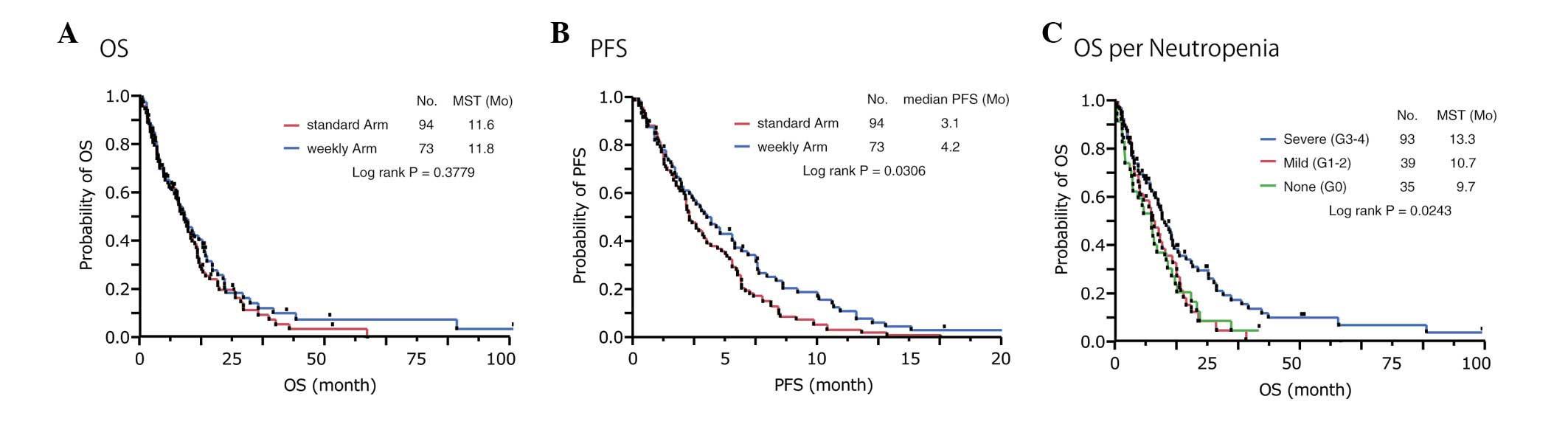
We conducted a series of survival analyses on
September 1, 2012. At that time, 136 patients had died, 28 patients
had been lost to follow-up and 3 patients were alive. Consequently,
the censoring rate was estimated at 18.6%. The MSTs were 11.8
months (95% CI, 8.4–16.8) and 11.6 months (95% CI, 9.5–14.6) for
the patients in the weekly and standard arms, respectively
(Fig. 1A). The 1-year survival
rates were 49.2% (95% CI, 37.1–61.3) and 48.8% (95% CI, 38.3–59.2)
for the patients in the weekly and standard arms, respectively. The
median PFS times were 4.2 months (95% CI, 2.7–5.5) and 3.1 months
(95% CI, 2.8–4.0) for the patients in the weekly and standard arms,
respectively (Fig. 1B). In the
univariate analyses, the PFS was significantly longer in the weekly
arm group (P=0.0306). The hazard ratio (HR) for the PFS of patients
in the weekly arm versus the standard arm was 0.576 (P=0.0024).
Univariate analyses for OS
In the univariate analyses, the OS was significantly
longer in the patients treated with EGFRTKIs (P=0.0007), females
(P=0.0051), individuals who had never smoked (P=0.0043), those with
PS 0/1/2 (P=0.0062), those with nonsquamous cell carcinoma
(P=0.0280) and those with stage IIIB disease (P=0.0248), compared
with the respective counterparts. However, the front-line
chemotherapy schedules (P=0.3779) and patient age (P=0.6135) were
not statistically significant prognostic factors for OS (Table III). We also analyzed the
contribution of the worst grade of treatment-related hematological
toxicity to OS. The correlation between OS and thrombocytopenia was
not statistically significant (P= 0.3718). The OS was significantly
shorter in patients with severe anemia (grade 3 or 4; P=0.0002). On
the contrary, the results of the alternative analyses clearly
indicated that OS was significantly longer in patients with severe
(grade 3 or 4) neutropenia (P=0.0243; Fig. 1C).
| Table IIIUnivariate analysis of OS. |
Table III
Univariate analysis of OS.
| Variable | MST (months) | P-value |
|---|
| Weekly arm vs.
standard arm | 11.8 vs. 11.6 | 0.3779b |
| Female vs.
male | 17.1 vs. 10.4 | 0.0051a |
| Never smoked vs.
smoker | 16.2 vs. 10.0 | 0.0043a |
| Age <70 vs. ≥70
years | 11.6 vs. 11.8 | 0.6135b |
| PS 0/1/2 vs.
3/4 | 12.5 vs. 3.2 | 0.0062a |
| Non-sq vs. sq | 12.6 vs. 9.7 | 0.0280a |
| TKI used vs. never
used | 16.5 vs. 9.7 | 0.0007a |
| Stage IIIB vs.
IV | 14.6 vs. 10.7 | 0.0248a |
| Neutropenia (G3 or
G4 vs. G1 or G2 vs. G0) | 13.3 vs. 10.7 vs.
9.7 | 0.0243a |
| Anemia (G3 or G4
vs. G1 or G2 vs. G0) | 4.7 vs. 12.8 vs.
23.0 | 0.0002a |
| Thrombocytopenia
(G3 or G4 vs. G1 or G2 vs. G0) | 5.2 vs. 12.6 vs.
10.6 | 0.3718b |
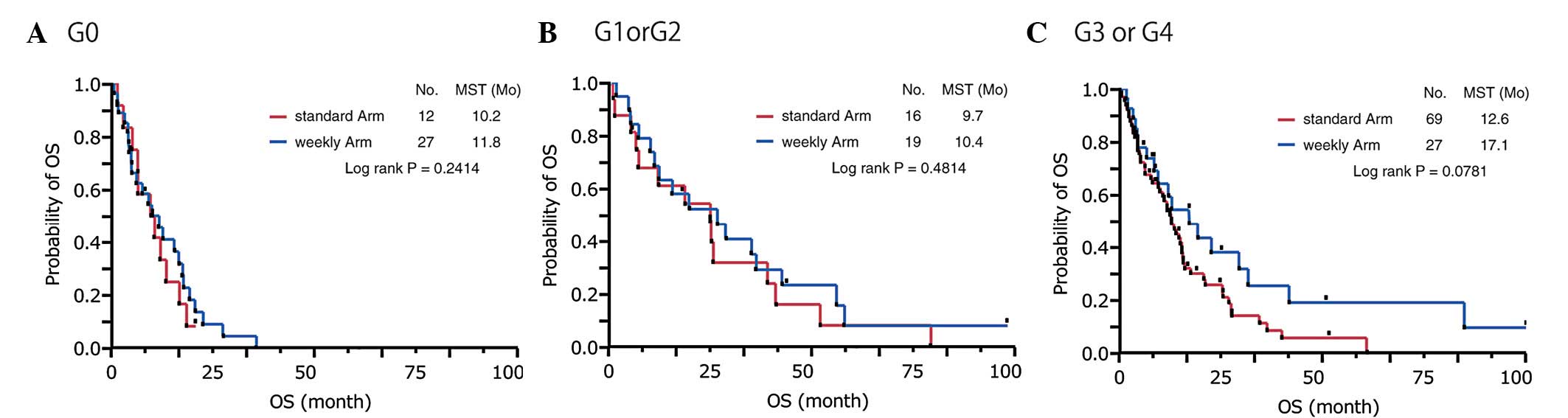
We had demonstrated that severe neutropenia more
frequently occurred with the standard schedule (70.2 vs. 37.0%),
which indicated a significant survival impact, than in the weekly
schedule; however, the survival curves of the 2 schedules almost
overlapped (Fig. 1A). Subsequently,
we conducted an alternative subanalysis for OS according to the
worst grade of neutropenia (Fig.
2). In the subpopulations of mild (grade 1 or 2) and no (grade
0) neutropenia, comparable survival was demonstrated for the 2
schedules (Fig. 2A and B). However,
in the subpopulation of severe (grade 3 or 4) neutropenia, the
patients in the weekly schedule arm tended to have better survival
that those in the standard schedule arm (P=0.0781; Fig. 2C). To evaluate the independent
survival impact of the covariates, we subsequently conducted a
multivariate analysis that included the severity of hematological
toxicities as covariates.
Multivariate analysis for OS
Unexpectedly, the multivariate analysis revealed
that the weekly schedule was an independent favorable prognostic
factor for OS (HR=0.634; P=0.0262), whereas the results of the
univariate analysis failed to indicate a significant difference. In
addition, PS 0/1/2 (P=0.0002), stage IIIB disease (P=0.0011), a
history of EGFR-TKI treatment (P=0.0007), female gender (P=0.0320),
grade 3 or 4 neutropenia (P=0.0002) and grade 0 anemia
(P<0.0001) were also independent favorable prognostic factors
(Table IV). However, no significant
difference in OS was observed between patients with grade 1 or 2
neutropenia and those with grade 0 neutropenia (P=0.5392).
| Table IVMultivariate analysis of OS. |
Table IV
Multivariate analysis of OS.
| Covariate | HR | 95% CI | P-value |
|---|
| Weekly arm vs.
standard arm | 0.634 | 0.422–0.948 | 0.0262a |
| Female vs.
male | 0.528 | 0.289–0.947 | 0.0320a |
| Never smoked vs.
smoker | 0.727 | 0.415–1.255 | 0.2557b |
| Age <70 years
vs. ≥70 years | 1.078 | 0.714–1.647 | 0.7245b |
| PS 0/1/2 vs.
3/4 | 0.296 | 0.167–0.550 | 0.0002a |
| Non-sq vs. sq | 0.957 | 0.610–1.526 | 0.8501b |
| TKI used vs. never
used | 0.495 | 0.327–0.744 | 0.0007a |
| Stage IIIB vs.
IV | 0.485 | 0.301–0.756 | 0.0011a |
| Neutropenia | | | |
| (G3 or G4 vs.
G0) | 0.372 | 0.215–0.654 | 0.0007a |
| (G1 or G2 vs.
G0) | 0.825 | 0.448–1.527 | 0.5392b |
| (G3 or G4 vs. G1
or G2) | 0.450 | 0.281–0.728 | 0.0013a |
| Anemia | | | |
| (G3 or G4 vs.
G0) | 9.527 | 3.415–29.301 | <0.0001a |
| (G1 or G2 vs.
G0) | 3.514 | 1.422–9.775 | 0.0056a |
| (G3 or G4 vs. G1
or G2) | 2.711 | 1.641–4.404 | 0.0001a |
|
Thrombocytopenia | | | |
| (G3 or G4 vs.
G0) | 0.870 | 0.424–1.709 | 0.6290b |
| (G1 or G2 vs.
G0) | 0.785 | 0.525–1.177 | 0.2407b |
| (G3 or G4 vs. G1
or G2) | 1.108 | 0.570–2.047 | 0.7538b |
Discussion
The weekly schedule of paclitaxel and carboplatin
combination treatment was investigated with 2 aims: one was to
reduce the incidence of treatment-related toxicities, and the other
was to assess the alternative antitumor effect based on the
metronomic theory (16). To date,
several weekly treatment schedules have been investigated (4–6). We
applied the weekly schedule scheme (weekly arm) demonstrated by
Hirabayashi et al(7). The
efficacy and feasibility of this regimen were confirmed in an
alternative phase II study described by Komuta et
al(17). A previous randomized
study described by Sakakibara et al compared these 2
schedule plans in an elderly patient (≥70 years of age) setting and
observed that in addition to its comparable survival benefit, the
weekly schedule was less toxic than the standard schedule (18).
However, the close correlation between
chemotherapy-related hematological toxicity and survival benefit
has been discussed extensively for various malignant tumors
(8–11). Kishida et al demonstrated
that treatment-related neutropenia was a favorable predictive
factor for the OS of patients with advanced NSCLC (JMTOG LC00-03)
(9). Two additional studies have
supported these findings (10,11).
We also demonstrated that grade 3 or 4 neutropenia was an
independent favorable prognostic factor for OS in this study.
However, the results of our univariate analyses clearly
demonstrated that the OS times were similar between the 2 treatment
schedules, whereas the incidence of grade 3 or 4 neutropenia was
significantly lower in the weekly schedule arm than in the standard
schedule arm. We hypothesized that an alternative survival benefit
arising from the weekly schedule may overcome the disadvantage of
the decreased incidence of neutropenia in that group. One possible
explanation for this finding is that the metronomic activity of the
weekly schedule may result in an alternative antitumor effect,
leading to an additional survival benefit. Low-dose metronomic
(LDM) chemotherapy consists of the administration of a relatively
low dose of a cytotoxic drug without a long interval (19,20). A
number of experimental studies have demonstrated that LDM
chemotherapy exerts an alternative antitumor effect different from
the direct cytotoxic effect of the drug (16,21).
Notably, the result of our multivariate analysis revealed that the
weekly schedule was an independent favorable prognostic factor for
OS. Based on our rationale, optimization of the dose and schedule
ought to achieve a superior survival benefit for the weekly
schedule. Katsumata et al clearly demonstrated that a
myelosuppressive ‘dose-dense’ weekly schedule has a superior
survival benefit for ovarian cancer compared with the standard
tri-weekly schedule (22). These
findings strongly support our hypothesis. Therefore, the next
question is whether escalation of the relative dose density leads
to superior survival benefits. This will not be consistently true
because the metronomic power is not augmented in a dose-dependent
manner. The maximum metronomic power of a drug is defined by the
optimal biological dose (OBD) rather than the maximum tolerated
dose (23). There is no reliable
surrogate marker to determine OBD.
Despite the retrospective nature and small scale of
the present study, our results clearly demonstrated that the weekly
schedule of carboplatin and paclitaxel was less toxic than and
potentially superior to the standard tri-weekly schedule. However,
further modification of the dose and schedule is warranted.
References
|
1
|
D’Addario G, Pintilie M, Leighl NB, et al:
Platinum-based versus non-platinum-based chemotherapy in advanced
non-small-cell lung cancer: a meta-analysis of the published
literature. J Clin Oncol. 23:2926–2936. 2005.PubMed/NCBI
|
|
2
|
Ohe Y, Ohashi Y, Kubota K, et al:
Randomized phase III study of cisplatin plus irinotecan versus
carboplatin plus paclitaxel, cisplatin plus gemcitabine, and
cisplatin plus vinorelbine for advanced non-small-cell lung cancer:
Four-Arm Cooperative Study in Japan. Ann Oncol. 18:317–323. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schiller JH, Harrington D, Belani CP, et
al: Comparison of four chemotherapy regimens for advanced
non-small-cell lung cancer. N Engl J Med. 346:92–98. 2002.
View Article : Google Scholar
|
|
4
|
Belani CP, Ramalingam S, Perry MC, et al:
Randomized, phase III study of weekly paclitaxel in combination
with carboplatin versus standard every-3-weeks administration of
carboplatin and paclitaxel for patients with previously untreated
advanced non-small-cell lung cancer. J Clin Oncol. 26:468–473.
2008. View Article : Google Scholar
|
|
5
|
Socinski MA, Ivanova A, Bakri K, et al: A
randomized phase II trial comparing every 3-weeks
carboplatin/paclitaxel with every 3-weeks carboplatin and weekly
paclitaxel in advanced non-small cell lung cancer. Ann Oncol.
17:104–109. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Quoix E, Zalcman G, Oster JP, et al:
Carboplatin and weekly paclitaxel doublet chemotherapy compared
with monotherapy in elderly patients with advanced non-small-cell
lung cancer: IFCT-0501 randomised, phase 3 trial. Lancet.
378:1079–1088. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hirabayashi M, Endoh K, Teramachi M, et
al: Phase II study of carboplatin and weekly paclitaxel combination
chemotherapy in advanced non-small cell lung cancer: a Kansai
Clinical Oncology Group study. Lung Cancer. 44:355–362. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shitara K, Matsuo K, Oze I, et al:
Meta-analysis of neutropenia or leukopenia as a prognostic factor
in patients with malignant disease undergoing chemotherapy. Cancer
Chemother Pharmacol. 68:301–307. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kishida Y, Kawahara M, Teramukai S, et al:
Chemotherapy-induced neutropenia as a prognostic factor in advanced
non-small-cell lung cancer: results from Japan Multinational Trial
Organization LC00-03. Br J Cancer. 101:1537–1542. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Di Maio M, Gridelli C, Gallo C, et al:
Chemotherapy-induced neutropenia and treatment efficacy in advanced
non-small-cell lung cancer: a pooled analysis of three randomised
trials. Lancet Oncol. 6:669–677. 2005.PubMed/NCBI
|
|
11
|
Pallis AG, Agelaki S, Kakolyris S, et al:
Chemotherapy-induced neutropenia as a prognostic factor in patients
with advanced non-small cell lung cancer treated with front-line
docetaxel-gemcitabine chemotherapy. Lung Cancer. 62:356–363. 2008.
View Article : Google Scholar
|
|
12
|
Mountain CF: Revisions in the
International System for Staging Lung Cancer. Chest. 111:1710–1717.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sobin L and Wittekind CH: TNM
Classification of Malignant Tumours. 6th edition. Wiley-Liss; New
York, NY: pp. 99–103. 2002
|
|
14
|
National Cancer Institute (NCI): Common
Terminology Criteria for Adverse Events (CTCAE) version 4.0. May
28–2009, http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf.
Accessed October 9, 2012.
|
|
15
|
Therasse P, Arbuck SG, Eisenhauer EA, et
al: New guidelines to evaluate the response to treatment in solid
tumors. European Organization for Research and Treatment of Cancer,
National Cancer Institute of the United States, National Cancer
Institute of Canada. J Natl Cancer Inst. 92:205–216. 2000.
View Article : Google Scholar
|
|
16
|
Jiang H, Tao W, Zhang M, Pan S, Kanwar JR
and Sun X: Low-dose metronomic paclitaxel chemotherapy suppresses
breast tumors and metastases in mice. Cancer Invest. 28:74–84.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Komuta K, Osaki T, Mori M, et al: A phase
II study directed by a clinical pathway for carboplatin and weekly
paclitaxel in previously untreated patients with unresectable
non-small cell lung cancer. Chemotherapy. 56:39–45. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sakakibara T, Inoue A, Sugawara S, et al:
Randomized phase II trial of weekly paclitaxel combined with
carboplatin versus standard paclitaxel combined with carboplatin
for elderly patients with advanced non-small-cell lung cancer. Ann
Oncol. 21:795–799. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Browder T, Butterfield CE, Kräling BM, et
al: Antiangiogenic scheduling of chemotherapy improves efficacy
against experimental drug-resistant cancer. Cancer Res.
60:1878–1886. 2000.PubMed/NCBI
|
|
20
|
Drevs J, Fakler J, Eisele S, et al:
Antiangiogenic potency of various chemotherapeutic drugs for
metronomic chemotherapy. Anticancer Res. 24:1759–1763.
2004.PubMed/NCBI
|
|
21
|
Kamat AA, Kim TJ, Landen CN Jr, Lu C, Han
LY, Lin YG and Sood AK: Metronomic chemotherapy enhances the
efficacy of antivascular therapy in ovarian cancer. Cancer Res.
67:281–288. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Katsumata N, Yasuda M, Takahashi F, et al:
Dose-dense paclitaxel once a week in combination with carboplatin
every 3 weeks for advanced ovarian cancer: a phase 3, open-label,
randomised controlled trial. Lancet. 371:1331–1338. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shaked Y, Emmenegger U, Man S, et al:
Optimal biologic dose of metronomic chemotherapy regimens is
associated with maximum antiangiogenic activity. Blood.
106:3058–3061. 2005. View Article : Google Scholar : PubMed/NCBI
|