Introduction
Autophagy is a metabolic process in which
autophagosomes combine with the lysosome in eukaryotic cells and
degrade intracellular macromolecules and endogenous substrate to
maintain a stable internal environment. During nutritional
deficiency, autophagy provides nutrition (ATP, amino acids, etc.)
for cell survival by degrading intracellular components (1). Autophagy is an important regulatory
mechanism in cell growth, maturation and death and is associated
with a variety of human diseases, including tumors.
Chemotherapy agents, including cisplatin and
paclitaxel, may lead to an autophagic response, which is one
possible method of inducing apoptosis, or may be associated with
tumor resistance (2–5). Cisplatin and paclitaxel are commonly
used in the treatment of lung cancer as first-line chemotherapeutic
agents. Cisplatin induces apoptosis by interfering with DNA
replication and also promotes autophagic cell death. Studies have
shown that drugs, including cisplatin, are able to induce autophagy
in cancer cells and autophagy may be associated with drug
resistance in tumors (3–5). Paclitaxel is an effective mitotic
inhibitor and apoptosis-inducing agent, which is used to treat
malignant tumors and is widely used in lung cancer chemotherapy
(6). Paclitaxel is able to maintain
the stability of tubulin by promoting microtubule protein
polymerization and inhibiting depolymerization. It is also known to
induce apoptosis, thus it has become a first-line chemotherapeutic
agent for non-small cell lung cancer. Furthermore, the effect of
anti-cancer drugs on cancer cells may be increased by regulating
the level of autophagy (7). It has
been reported that paclitaxel induces autophagy and autophagic
inhibition by small interfering RNA against the autophagic gene
beclin 1, which may increase the rate of apoptosis induced by
paclitaxel (6).
There is an urgent requirement to improve
chemotherapy-induced apoptosis in cancer cells and increase the
sensitivity of cancer cells to chemotherapeutic drugs in clinics.
Therefore, we observed autophagy in A549 lung cancer cells, which
was induced by chemotherapeutic drugs, either alone or in
combination with an autophagic inhibitor (3-methyladenine, 3-MA),
to provide a scientific basis for improving chemotherapeutic drug
sensitivity.
Materials and methods
Cell and reagents
Human lung cancer A549 cells were obtained from The
Cell Bank of Chinese Academy of Sciences (Shanghai, China). A549
cells were supplemented with 10% fetal bovine serum and antibiotics
(100 U/ml penicillin and 100 μg/ml streptomycin). Cells were
incubated in a humidified incubator under 5% CO2 at
37°C. Cisplatin was purchased from Qilu Pharmaceutical Co., Ltd.
(Shandong, China). Paclitaxel was purchased from Wanle
Pharmaceutical Co., Ltd. (Shenzhen, China). 3-MA, Hoechst 33342,
dimethyl sulfoxide (DMSO), monodansylcadaverine (MDC) and methyl
thiazolyl tetrazolium (MTT) were obtained from Sigma-Aldrich (St.
Louis, MO, USA).
MTT assay for cell growth inhibition
Cells were seeded at a density of 1×105
cells in each well of the 96-well plates and incubated for 24 h. A
series of concentrations of cisplatin, paclitaxel or 3-MA were
added to the wells for 24, 48 or 72 h. MTT (5 g/l, 20
μl/well) was added to each well and incubated at 37°C for 4
h. DMSO was then added (100 μl/well) to each well to
dissolve any crystals and the plates were agitated for 10 min.
Absorbance values at 490 nm were detected by the microplate reader.
Cell growth inhibition was calculated on the basis of the following
formula: Cell growth inhibition rate (%) = [1 − A490 (experimental
group)/A490 (control group)] × 100. Each experiment was repeated
three times.
MTT assay for cell proliferation
The experiment was divided into five groups: the
control group (without drug intervention), the 3-MA group (3-MA
treatment alone), the cisplatin group (cisplatin treatment alone),
the paclitaxel group (paclitaxel treatment alone), the 3-MA and
cisplatin combined group (3-MA and cisplatin were added
simultaneously) and the 3-MA and paclitaxel combined group (3-MA
and paclitaxel were added simultaneously). Cells were plated as per
the above assay. Following incubation for 24 h, the drugs were
added according to the above experimental groups. Cells were
incubated in a humidified 5% CO2 atmosphere at 37°C for
24 h. MTT and DMSO were added to the wells in succession. Cell
proliferation was calculated using the following formula: Cell
proliferation (%) = A490 (experimental group)/A490 (control group)
× 100. Each group was assayed in triplicate.
MDC staining
A549 cells in the logarithmic growth phase were
treated with trypsin and plated in 24-well plates at a density of
1×105 cells. Following incubation for 24 h, drugs were
added at the corresponding concentrations to the five experimental
groups. After 24 h, cells were stained with MDC (50 μmol/l)
for 60 min at 37°C, washed with PBS three times, fixed with 4%
paraformaldehyde at 4°C for 15 min and washed with PBS a further
three times. Inverted fluorescence microscopy was used to observe
the change in autophagic vacuoles and to capture images. Cell
fluorescence intensity in the various groups was measured by flow
cytometry.
Hoechst 33342 staining
Cells were plated in 24-well plates and incubated
for 24 h. Drugs were added to each well according to the five
experimental groups, and incubated for 24 h. The cells were washed
with PBS three times and stained with Hoechst 33342 (1 mg/l) for 20
min at 37°C. Images of the Hoechst 33342 fluorescence were captured
using inverted fluorescence microscopy, after the cells were washed
with PBS three times. The fluorescence staining percentage of
positive cells was calculated according to the images.
Apoptosis detected by flow cytometry
Cells were seeded at 1×105 in each well
of the six-well plates and were pretreated with 3-MA, cisplatin or
paclitaxel for 24 h, according to the five experimental groups.
Cells were collected by trypsinization and washed with PBS. After
staining with Annexin V-fluorescein isothiocyanate (FITC) and
propidium iodide (PI) successively, the cells were immediately
detected using flow cytometry.
Statistical analysis
The results are expressed as the mean ± SD. SPSS
17.0 statistical software was used to analyze the results and a
single-factor analysis of variance was used to compare the
differences between groups. P<0.05 was considered to indicate a
statistically significant difference.
Results
Cell growth inhibition and proliferation
as detected by an MTT assay
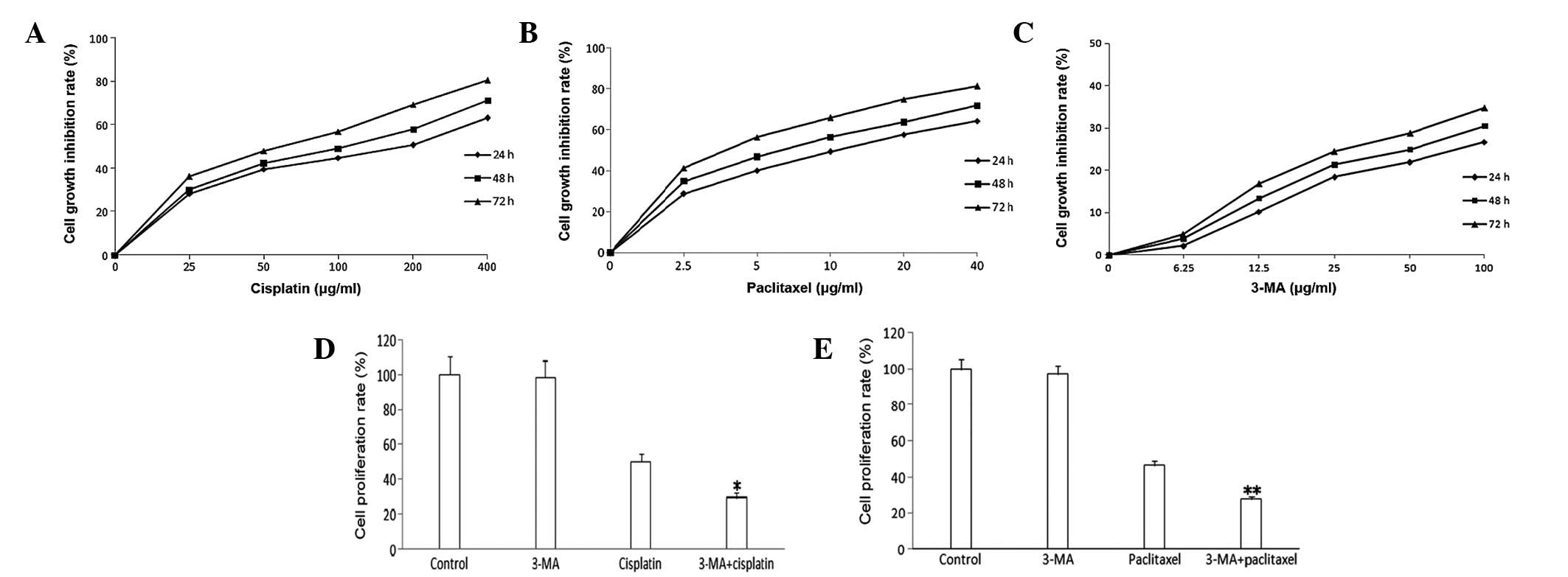
Different drug concentrations and treatment times
have varied effects on cell growth. Results from the MTT assay
showed that, as drug concentration and treatment time increased,
the rate of cell growth inhibition also increased. The
IC10 of A549 cells was 12.5 μg/ml after treatment
with 3-MA for 24 h. Following treatment with cisplatin or
paclitaxel for 24 h, the IC50 of A549 cells were 200 and
10 μg/ml, respectively. Therefore, the optimal
concentrations of cisplatin, paclitaxel and 3-MA were 200, 10 and
12.5 μg/ml, respectively (Fig.
1A–C). 3-MA had no significant effect on cell proliferation.
Cisplatin or paclitaxel treatment lead to a marked decline in cell
proliferation. Compared with cispatin or paclitaxel treatment, the
rates of cell proliferation were markedly declined in the 3-MA
combined groups (Figs. 1D and
E).
Chemotherapeutic drugs trigger autophagy
in A549 cells
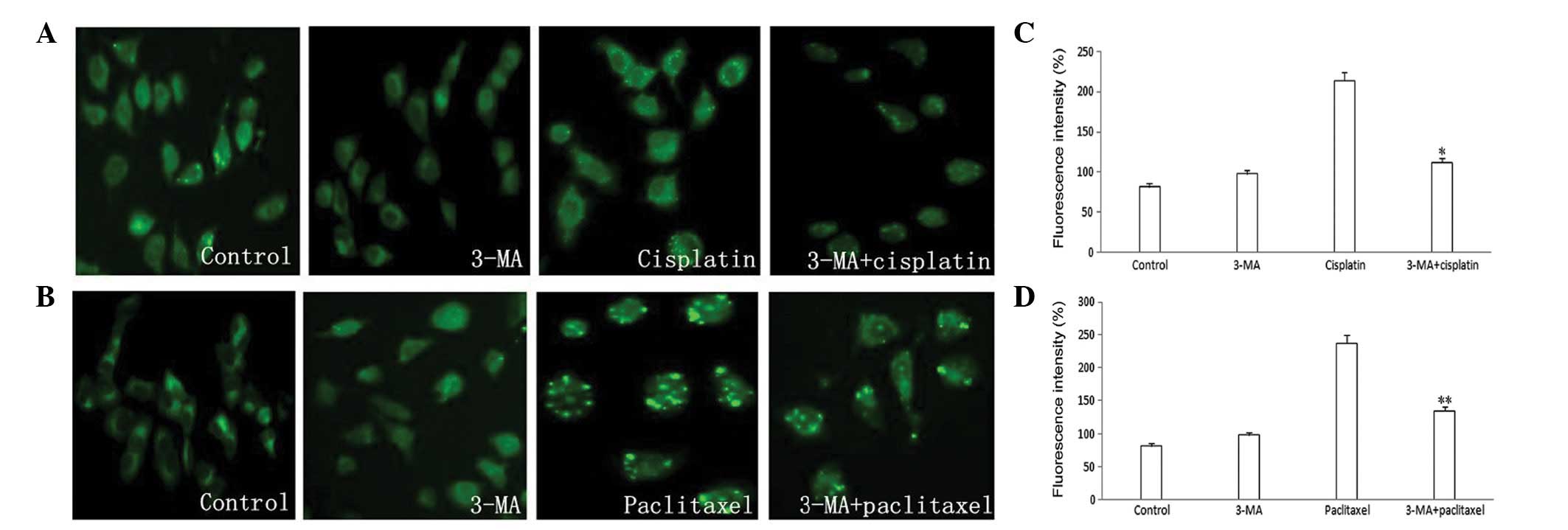
Due to the MDC gathered in autophagic vacuoles of
the treated cells, blue-green and yellow-green punctate structures
were visualized around the nucleus. No significant autophagic
vacuoles appeared in the 3-MA group and compared with the control
group, there was no significant difference in the MDC fluorescence
intensity. Chromatin condensation and a large number of autophagic
vacuoles appeared in the cisplatin and paclitaxel groups and
fluorescence intensity was markedly increased. Compared with the
cisplatin and paclitaxel groups, autophagic vacuoles were reduced
and fluorescence intensity was decreased in the 3-MA combined group
(Fig. 2).
Apoptosis as detected by Hoechst 33342
staining in A549 cells
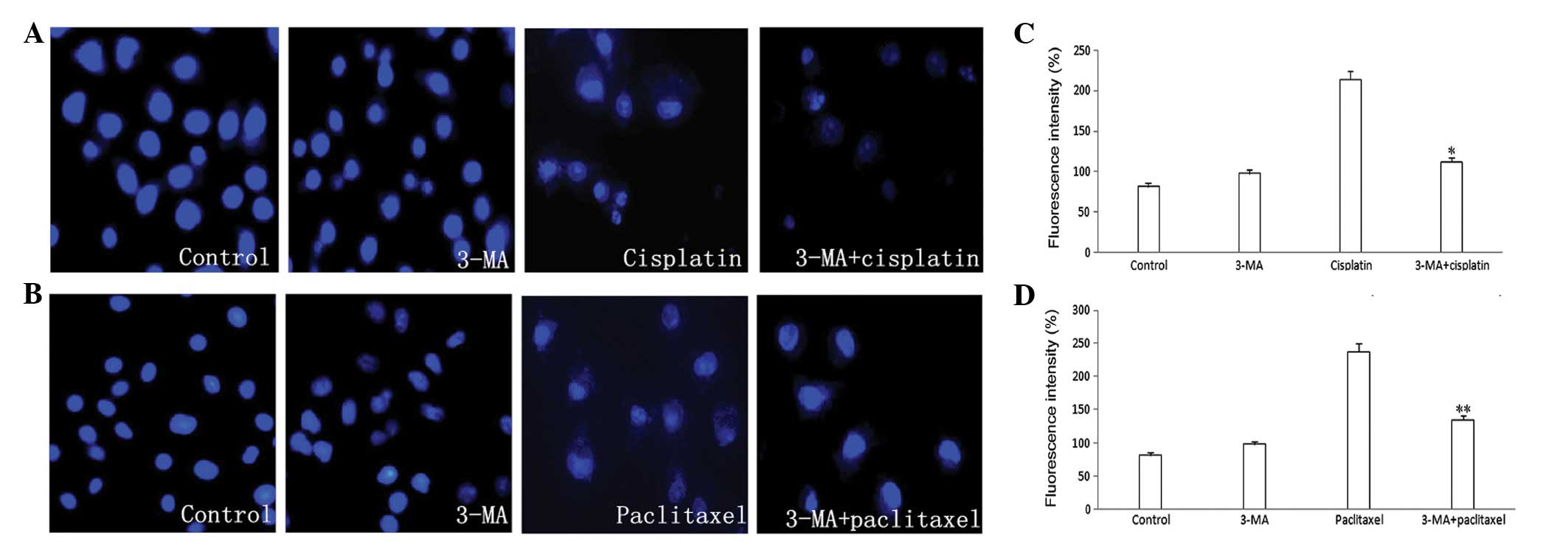
A change in cell morphology was not apparent in the
3-MA group. Results from Hoechst 33342 staining indicated that the
percentage of positive cells was small. Nucleus cleavage and
chromatin condensation appeared in the cisplatin and paclitaxel
groups, which suggests that apoptosis occurred. In the 3-MA
combined groups, apoptosis and the percentage of positive cells was
increased significantly (Fig.
3).
Inhibition of autophagy by 3-MA promotes
chemotherapeutic drug-induced apoptotic cell death
Tumor cell apoptosis was detected using flow
cytometry. Compared with control group, the 3-MA group showed no
change in the apoptosis rate. The apoptosis rate in the combined
3-MA groups was significantly higher than in the cisplatin and
paclitaxel groups. This indicates that 3-MA played a role in the
process of promoting apoptosis.
Discussion
Lung cancer is one of the most common malignancies
worldwide. The failure of chemotherapy is often a result of drug
resistance. Improving chemosensitivity is necessary for clinical
improvements. Numerous studies have shown that autophagy, under
specific treatment conditions, may be activated in various cancer
cells and may play an important role in the process of
tumorigenesis and tumor development (8). It has also been suggested that the
development of malignant tumors is related to the disorder of
autophagic regulatory mechanisms. However, the specific role of
autophagy in the process of tumorigenesis and tumor development
remains to be clarified.
Cisplatin is used for a variety of malignant tumors
(including in lung cancer); it inhibits cancer cells during DNA
replication and causes damage to the cell membrane structure,
however, tumor resistance has been problematic in clinical
treatment (9). Studies have shown
that drugs, such as cisplatin, cause autophagy in tumor cells and
that autophagy has a unique association with tumor resistance
(3–5). Paclitaxel is able to maintain tubulin
stability and inhibit cell mitosis, thus inducing apoptosis by
promoting tubulin polymerization and inhibiting depolymerization.
Adjusting autophagy appropriately may increase the cytotoxicity of
anticancer drugs in tumor cells (7). In this study, we demonstrated that the
autophagic inhibitor 3-MA significantly enhanced the cytotoxic
effects of cisplatin and paclitaxel in A549 cells. This suggests
that inhibitors of autophagy may be a novel sensitizer to improve
the effects of chemotherapy drugs. Results from the MTT assays,
Hoechst 33342 staining and flow cytometry show that autophagy,
induced by cisplatin or paclitaxel, protected cancer cells from
apoptosis and autophagic inhibitor 3-MA may potentiate the toxicity
of cisplatin and paclitaxel and increase the rate of apoptosis.
This indicates that autophagy is associated with chemoresistant
mechanisms in A549 lung cancer cells.
During the course of chemotherapy, inhibition of
autophagy to reduce the scavenging of damaged cells may allow an
increase in the rate of apoptosis. Numerous studies have indicated
that inhibition of autophagy increases the sensitivity of cancer
cells to anticancer drugs, which causes DNA damage (10). This was consistent with previous
studies, which suggested that the majority of chemotherapeutic
drugs induce autophagy and inhibition of autophagy enhanced the
effect of chemotherapy (11,12).
In certain cases, autophagy and apoptosis have been induced at the
same time (13,14) and autophagy has been shown to
restrain apoptosis in specific circumstances (11,15,16).
In conclusion, our results indicate that autophagy
was induced in lung cancer A549 cells, along with cisplatin- or
paclitaxel-induced apoptosis and inhibition of autophagy was able
to potentiate the toxicity of cisplatin and paclitaxel. They also
demonstrated the existence of a connection between autophagy and
apoptosis in certain cases. Thus we speculate that autophagy may
play a protective role in the process of cisplatin- or
paclitaxel-induced apoptosis, however, further study is required to
determine whether autophagic inhibition could be utilized in
clinics.
Acknowledgements
This study was supported in part by
the Youth Innovation Fund Project of the First Affiliated Hospital
of Zhengzhou University and grant 122300410158 from the Foundation
and Advanced Technology Research Program of Henan province.
References
|
1
|
Kang R and Tang D: Autophagy in pancreatic
cancer pathogenesis and treatment. Am J Cancer Res. 2:383–396.
2012.PubMed/NCBI
|
|
2
|
Zeng X and Kinsella TJ: Impact of
autophagy on chemotherapy and radiotherapy mediated tumor
cytotoxicity: ‘to live or not to live’. Front Oncol.
1:302011.PubMed/NCBI
|
|
3
|
Ren JH, He WS, Nong L, et al: Acquired
cisplatin resistance in human lung adenocarcinoma cells is
associated with enhanced autophagy. Cancer Biother Radiopharm.
25:75–80. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Harhaji-Trajkovic L, Vilimanovich U,
Kravic-Stevovic T, Bumbasirevic V and Trajkovic V: AMPK-mediated
autophagy inhibits apoptosis in cisplatin-treated tumour cells. J
Cell Mol Med. 13:3644–3654. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Claerhout S, Verschooten L, Van Kelst S,
De Vos R, Proby C, Agostinis P and Garmyn M: Concomitant inhibition
of AKT and autophagy is required for efficient cisplatin-induced
apoptosis of metastatic skin carcinoma. Int J Cancer.
127:2790–2803. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xi G, Hu X, Wu B, Jiang H, Young CY, Pang
Y and Yuan H: Autophagy inhibition promotes paclitaxel-induced
apoptosis in cancer cells. Cancer Lett. 307:141–148. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shingu T, Fujiwara K, Bögler O, et al:
Inhibition of autophagy at a late stage enhances imatinib-induced
cytotoxicity in human malignant glioma cells. Int J Cancer.
124:1060–1071. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mathew R, Karantza-Wadsworth V and White
E: Role of autophagy in cancer. Nat Rev Cancer. 7:961–967. 2007.
View Article : Google Scholar
|
|
9
|
Köberle B, Tomicic MT, Usanova S and Kaina
B: Cisplatin resistance: preclinical findings and clinical
implications. Biochim Biophys Acta. 1806:172–182. 2010.PubMed/NCBI
|
|
10
|
Li J, Hou N, Faried A, Tsutsumi S and
Kuwano H: Inhibition of autophagy augments 5-fluorouracil
chemotherapy in human colon cancer in vitro and in vivo model. Eur
J Cancer. 46:1900–1909. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Katayama M, Kawaguchi T, Berger MS and
Pieper RO: DNA damaging agent-induced autophagy produces a
cytoprotective adenosine triposphate surge in malignant glioma
cells. Cell Death Differ. 14:548–558. 2007. View Article : Google Scholar
|
|
12
|
Pan Y, Gao Y, Chen L, et al: Targeting
autophagy augments in vitro and in vivo antimyeloma activity of
DNA-damaging chemotherapy. Clin Cancer Res. 17:3248–3258. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang YH, Wu YL, Tashiro S, Onodera S and
Ikejima T: Reactive oxygen species contribute to oridonin-induced
apoptosis and autophagy in human cervical carcinoma HeLa cells.
Acta Pharmacol Sin. 32:1266–1275. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang L, Yu C, Lu Y, et al: TMEM166, a
novel transmembrane protein, regulates cell autophagy and
apoptosis. Apoptosis. 12:1489–1502. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Colell A, Ricci JE, Tait S, et al: GAPDH
and autophagy preserve survival after apoptotic cytochrome c
release in the absence of caspase activation. Cell. 129:983–997.
2007. View Article : Google Scholar
|
|
16
|
Viola G, Bortolozzi R, Hamel E, et al:
MG-2477, a new tubulin inhibitor, induces autophagy through
inhibition of the Akt/mTOR pathway and delayed apoptosis in A549
cells. Biochem Pharmacol. 83:16–26. 2012. View Article : Google Scholar : PubMed/NCBI
|