Introduction
We report a case of a very unusual site of
metastasis of a renal cell carcinoma. Renal cell carcinoma
represents 2–3% of all malignancies (1), with an annual increase in incidence of
∼2%. Renal cell carcinoma represents ∼90% of kidney neoplasms
(2); 20–25% of the patients
initially present with advanced disease and ∼5% present with a
single metastatic site (3).
Patients affected by renal cell carcinoma will
develop metastasis during the follow-up period in ∼30% of cases
(4). The most common sites of renal
cell carcinoma metastases are the lung (50%), lymph nodes (35%),
liver (30%), bone (30%) and adrenal glands (5%) (5); skeletal muscle metastasis is a rare
occurrence.
Case report
A 76-year-old Caucasian female who was a non-smoker,
with a history of heart ischemic disease, hypertension, anemia and
diabetes, underwent a laparoscopic left radical nephrectomy for a
renal neoplasm of 10×7 cm in the superior left renal pole in 2011.
The postoperative course was uneventful and the patient was
discharged after 6 days. The histological examination revealed the
presence of a renal cell carcinoma, Fuhrman grade 2, with extensive
necrosis and phlogosis areas (TNM 2009 RCC pT2a). Informed consent
was obtained from the patient.
After discharge, the patient was readmitted for a
sciatica episode and underwent two abdomen ultrasonography
examinations, with no notable pathological findings.
After a few days, the patient noted an indolent
swelling in the proximal third of the right thigh. The patient
subsequently underwent ultrasonographic evaluation, revealing the
presence of a solid, vascularized mass that was ∼40×22 mm in
size.
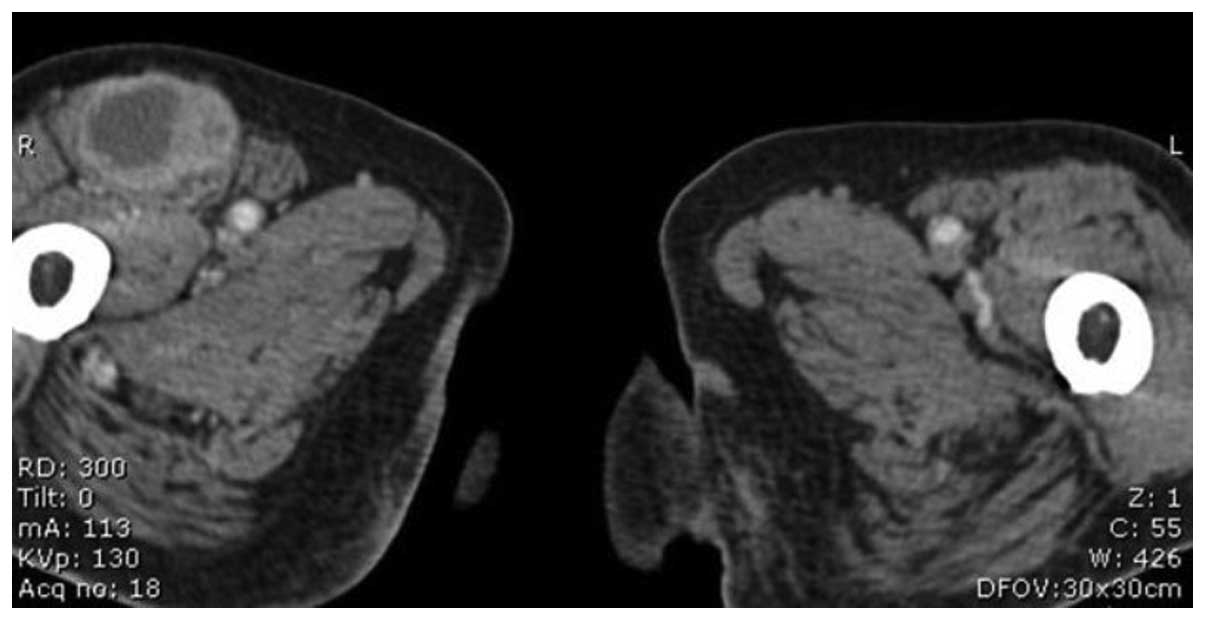
The subsequent CT documented the presence of a
pathological, solid, dishomogeneous bulk that was ∼4.5 cm diameter,
in the front of the right iliac vessels, immediately cranial to the
inguinal region. Another smaller (1.5 cm) lesion was observed in
the ipsilateral inguinale region, while an additional solid
expansive lesion was noted in the rectus femoris muscle
(Fig. 1).
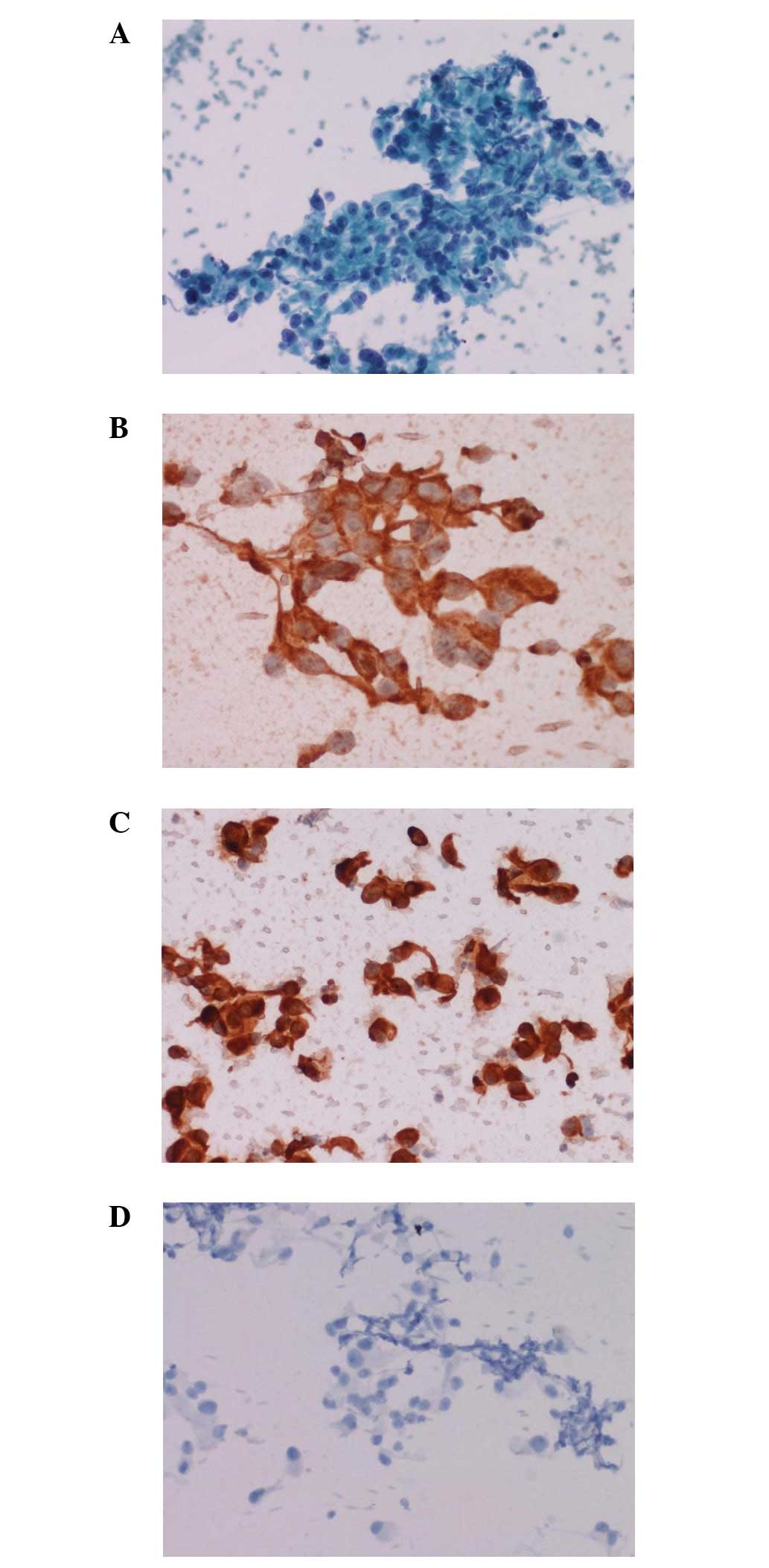
The fine needle biopsy of the muscle mass documented
a metastasis of renal cell carcinoma (Fig. 2). The histochemical analysis
revealed positive staining for vimentin and CAM, and negative
staining for cytokeratin 7.
Moreover, we performed a cerebral CT and a total
body bone scan, in order to achieve a complete stadiation of the
patient. Neither of the examinations revealed further meta-static
localization.
A joint evaluation of the patient was performed with
the oncologist, the general surgeon and the radiotherapist. With
regard to the pathological stage of the disease and the comorbidity
of the patient, it was decided to refer the patient for targeted
therapy with sunitinib.
Therefore, the patient underwent 2 cycles of
sunitinib therapy. Subsequently, due to the onset of edema in the
right lower limb, the patient underwent an abdominal CT, revealing
a nodal progression of the disease along the right femoral and
iliac vessels. The patient underwent 6 further cycles of salvage
therapy with sorafenib, which were well tolerated. The subsequent
CT scan revealed a lymphonodal progression of disease.
Discussion
Renal cell carcinoma presents a unpredictable
behavior, even after surgical therapy, and the median time to
recurrence may be extensive. McNichols et al demonstrated
that 11% of meta-static RCC cases occurred more than 10 years after
the initial diagnosis, even after complete resection (6).
Skeletal muscle metastasis is rare, regardless of
the site of origin. A limited number of cases concerning skeletal
muscle metastasis have been described in the literature, and its
prevalence is ∼1.6% (7). Possibly
the first case of skeletal metastasis originating from an RCC was
reported in 1979 by Chandler et al, describing a slowly
enlarging biceps muscle mass as an atypical presentation of RCC,
diagnosed with a soft tissue biopsy needle (8). More recently, Ali et al
reported the occurrence of a persistent left arm swelling
accompanied by wrist drop as an atypical presentation of renal cell
carcinoma (9).
Several other studies have demonstrated the
development of muscular metastasis during the follow-up period
after radical nephrectomy, with onset times varying between a
number of months and 19 years. Additionally, muscular metastasis
has been found in various muscular localizations, such as,
respectively, the thigh (at the level of the great adductor muscle
or, in our case, the rectus femoris), the iliopsoas muscle
or the erector spine muscle (10–12).
The mechanism involved in the metastatic spreading
to the skeletal muscular tissue is not fully understood. Several
explanations have been suggested, such as direct invasion or
hematogenous spreading. Moreover, Merimsky et al suggested
that the relative resistance of the muscular tissue to the
meta-static spreading should be investigated further (13).
The surgical resection of a solitary RCC metastasis
improves the survival of patients with metastatic RCC. In the
present case, with regard to the presence of multiple metastases
and the comorbidity, and in accordance with the wishes of the
patient, we decided to refrain from administering surgical
treatment and the patient was referred to the oncologist.
At present, there is no agreement with regard to a
surveillance protocol for patients treated for RCC. Additionally,
it is unclear whether an early recurrence diagnosis will improve
the survival of the patients (14).
However, an early recognition of tumor recurrences means that the
therapeutic approach to the disease, whether it be surgical
metastasectomy or systemic treatment, through the use of targeted
therapies, will be more effective.
The unpredictable behaviour of RCC suggests the need
to perform a thorough follow-up of patients, and to investigate all
soft tissue masses, including cytopathologically, that develop in
patients with a history of RCC.
References
|
1
|
European Network of Cancer Registries:
Eurocim version 4.0. European incidence database V2.3, 730 entity
dictionary (2001), Lyon, 2001.
|
|
2
|
Kovacs G, Akhtar M, Beckwith BJ, Bugert P,
Cooper CS, Delahunt B, Eble JN, Fleming S, Ljungberg B, Medeiros
LJ, et al: The Heidelberg classification of renal cell tumours. J
Pathol. 183:131–133. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gupta K, Miller JD, Li JZ, Russell MW and
Charbonneau C: Epidemiologic and socioeconomic burden of metastatic
renal cell carcinoma (mRCC): a literature review. Cancer Treat Rev.
34:193–205. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Flamigan RC, Campbell SC, Clark JI and
Picken MM: Metastatic renal cell carcinoma. Curr Treat Options
Oncol. 4:385–390. 2003. View Article : Google Scholar
|
|
5
|
Hanno P, Wein A and Malkowicz SB: Clinical
Manual of Urology. 3rd edition. McGraw Hill; New York, NY: 498.
2001
|
|
6
|
McNichols DW, Segura JW and DeWeerd JH:
Renal cell carcinoma: long term survival and late recurrence. J
Urol. 126:17–23. 1981.PubMed/NCBI
|
|
7
|
Vidart A, Fehri K and Pfister C: Unusual
metastasis of renal carcinoma. Ann Urol (Paris). 40:211–219.
2006.(In French).
|
|
8
|
Chandler RW, Shulman I and Moore TM: Renal
cell carcinoma presenting as a skeletal muscle mass: a case report.
Clin Orthop Relat Res. 145:227–229. 1979.PubMed/NCBI
|
|
9
|
Ali SH, Chugtai H, Alali F, Fiaczok B and
Verardi M: Wrist drop: an atypical presentation of renal cell
carcinoma. Am J Med Sci. 342:170–173. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Picchio M, Mascetti C, Tanga I and
Spaziani E: Metastasis from renal cell carcinoma presenting as
skeletal muscle mass: a case report. Acta Chir Belg. 110:399–401.
2010.PubMed/NCBI
|
|
11
|
Taira H, Ishii T, Inoue Y and Hiratsuka Y:
Solitary psoas muscle metastasis after radical nephrectomy for
renal cell carcinoma. Int J Urol. 12:96–97. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hur J, Yoon CS and Jung WH: Multiple
skeletal metastases from renal cell carcinoma 19 years after
radical nephrectomy. Acta Radiol. 48:238–241. 2007.PubMed/NCBI
|
|
13
|
Merimsky O, Levine T and Chiatchik S:
Recurrent solitary metastasis of renal cell carcinoma in skeletal
muscle. Tumori. 67:407–409. 1990.
|
|
14
|
Ljungberg B, Cowan NC, Hanbury DC, Hora M,
Kuczyk MA, Merseburger AS, Patard JJ, Mulders PF and Sinescu IC;
European Association of Urology Guideline Group: EAU guidelines on
renal cell carcinoma: the 2010 update. Eur Urol. 58:398–406. 2010.
View Article : Google Scholar : PubMed/NCBI
|