Introduction
Cytokines exhibit pleiotropic effects and are
crucial for the regulation of cell growth and differentiation.
Previous studies have evaluated the cytokine network, which is
involved in the local inflammatory and immune responses against
tumors (1–4). Cytokines from tumors may either
regulate tumor growth or modify the antitumor immune responses
(5–8). Tumor and immune cells are capable of
producing cytokines, however the key difference between these two
cell types is that cytokines produced by tumor cells are not
regulated.
Tumor cells are known to produce various cytokines
and chemokines that attract leukocytes and promote their
transformation into one of the diverse leukocyte populations,
mainly granulocytes, monocytes/macrophages, dendritic cells (DCs)
and lymphocytes. Subsequently, each population is able to produce
an array of cytokines to allow it to escape the immune control of
the host (9,10). Cytokines and chemokines from tumor
cells also genetically alter epithelial cells and a variety of
‘normal’ cells, including endothelial cells, which form the tumor
vasculature, fibroblasts and inflammatory cells (e.g., lymphocytes,
macrophages, mast cells and granulocytes), thus building a
supportive microenvironment (11,12).
In the present study, we measured the level of
pro-inflammatory cytokines, tumor infiltrating granulocytes (TIGs)
and tumor-associated macrophages (TAMs), determined the
granulocyte/lymphocyte (G/L) ratio and examined the expression of
granulocyte colony-stimulating factor (tG-CSF) and macrophage
colony-stimulating factor (tM-CSF) in tumor cells to evaluate their
role in tumor progression.
Patients and methods
Patient and tumor specimens
A total of 30 patients with primary colorectal
carcinoma, who underwent curative surgical treatment between
January 2008 and December 2011 at the Department of Surgery, First
Affiliated Hospital of Dalian Medical University, Dalian, China,
were included in the study. All patients received fasting
hemospasia to determine the quantity of cytokines preoperatively.
The tumors were histopathologically classified according to the
1997 tumor node metastasis (TNM) classification, as recommended by
the International Union Against Cancer (5th edition). None of the
patients had received chemotherapy or radiotherapy prior to
surgery.
ELISA
The levels of immunoreactive serum G-CSF (sG-CSF),
sM-CSF, interleukin (IL)-1β, IL-6, IL-8 and tumor necrosis factor
(TNF)-α were measured using ELISA. The following commercially
available ELISA kits were used: IL-1β, IL-6, TNF-α, M-CSF and G-CSF
(R&D systems, Minneapolis, MN, USA) and IL-8 (Biosource Europe
S.A., Nivelles, Belgium). The procedures for the cytokine assays
were carried out according to the manufacturer's instructions.
Immunohistochemical analysis of tumor
tissues
Detection of TIGs and TAMs
Immunostaining procedures for TIGs and TAMs were
performed using the EnVision™+/HRP method (Dako, Carpinteria, CA,
USA) with heat-induced antigen retrieval. Paraffin sections (4
μm) containing the tumor margin were applied. TIGs and TAMs
were detected with mouse anti-granulocyte (clone SPM250, 1:50;
Spring Bioscience, Fremonet, Germany) and monoclonal mouse
anti-CD68 (clone KP1, 1:200; Dako) antibodies. Negative control
sections were stained by omitting the primary antibody.
Detection of M-CSF expression (tM-CSF)
and G-CSF expression (tG-CSF) in tumor cells
tM-CSF and tG-CSF in colorectal carcinomas were
detected by immunohisto-chemical staining with monoclonal
anti-G-CSF (clone 4-12-2, 1:100; Immuno-Biological Laboratories,
Gunma, Japan) and monoclonal anti-M-CSF (clone EP1179Y, 1:100;
Epitomics, Burlingame, CA, USA) antibodies. Negative control
sections were stained by omitting the primary antibody. Specimens
were considered to be positive for tG-CSF and tM-CSF when ≥20% of
the tumor cells exhibited positive immunoreactivity.
Statistical analysis
All data, including stage of disease and
pathological factors, were obtained from clinical and pathological
records. Pearson's correlation coefficient and Spearman's
correlation were used to assess the correlation between related
variables. Significant differences were determined using the
Kruskal-Wallis test. Binary logistic regression analysis was
employed to determine the significant predictors for lymph node
metastasis and depth of tumor invasion. P<0.05 was considered to
indicate a statistically significant difference.
Results
Cytokine production in colorectal
patients
A total of 30 patients underwent preoperative blood
sampling, however the data for sM-CSF and TNF-α were lost for 9
patients. Abnormal levels (a higher than normal value) of IL-1β,
IL-6, IL-8, TNF-α, sG-CSF and sM-CSF were detected in 1/30 (3.3%),
16/30 (53.3%), 15/30 (50%), 4/21(19%), 17/30 (56.7%) and 4/21 (19%)
cases, respectively.
Detection of TIGs and TAMs and their
correlation
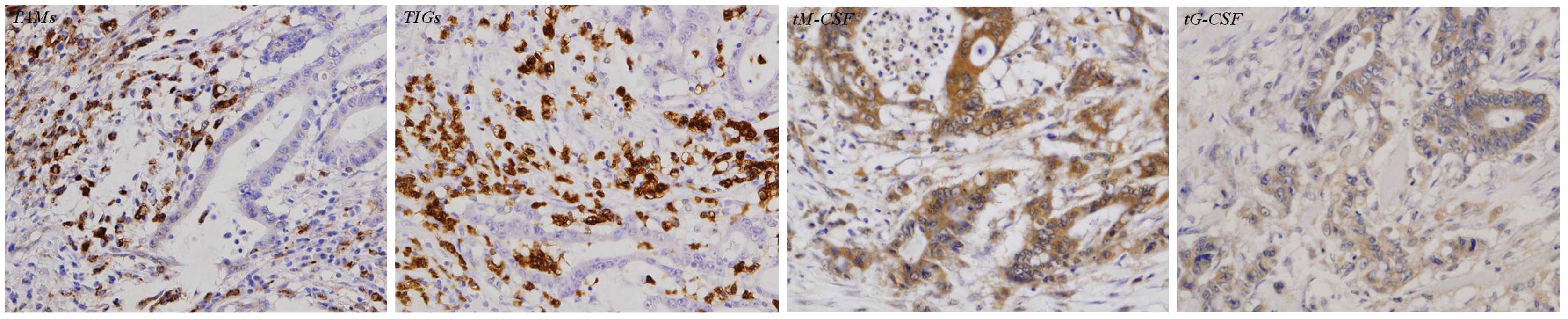
The average number of TIGs and TAMs was 47.3±26.1
and 32.5±33.8 per 10×40 hpf, respectively. TIGs were mainly located
at the site of tumor invasion, however TAMs were located in areas
of tumor invasion and the stroma (Fig.
1). Granulocytes and macrophages in necrotic regions were
excluded from the statistical analysis. No significant positive
correlation was identified between TIGs and TAMs (P= 0.58, Table I).
 | Table ICorrelation between cytokines and G/L
ratio. |
Table I
Correlation between cytokines and G/L
ratio.
| Variable | IL-6 | sM-CSF | sG-CSF | IL-8 | IL-1β | TNF-α | G/L ratio | TIGs |
|---|
| sM-CSF | | | | | | | | |
| R | 0.517b | | | | | | | |
| P-value | 0.017 | | | | | | | |
| sG-CSF | | | | | | | | |
| R | 0.369a | | | | | | | |
| P-value | 0.045 | 0.56 | | | | | | |
| IL-8 | | | | | | | | |
| R | | | | | | | | |
| P-value | 0.63 | 0.75 | 0.37 | | | | | |
| IL-1β | | | | | | | | |
| R | | | | | | | | |
| P-value | 0.90 | 0.99 | 0.56 | 0.43 | | | | |
| TNF-α | | | | | | | | |
| R | | | | | | | | |
| P-value | 0.44 | 0.69 | 0.44 | 0.89 | 0.62 | | | |
| G/L ratio | | | | | | | | |
| R | | | | | | | | |
| P-value | 0.24 | 0.89 | 0.45 | 0.58 | 0.65 | 0.67 | | |
| TIGs | | | | | | | | |
| R | | | | | | 0.43a | | |
| P-value | 0.945 | 0.320 | 0.364 | 0.445 | 0.297 | 0.050 | 0.888 | |
| TAMs | | | | | | | | |
| R | | | | 0.32a | | | | |
| P-value | 0.64 | 0.75 | 0.33 | 0.09 | 0.67 | 0.49 | 0.40 | 0.579 |
Correlation between cytokines
We analyzed the correlation between all the
cytokines which feature in this study. Pearson's correlation
coefficient test revealed that there was a positive linear
correlation between IL-6 and sM-CSF (P=0.017, R=0.517) and
Spearman's correlation test revealed that there was a significant
correlation between IL-6 and sG-CSF (P=0.045, R=0.369). However, no
significant correlation was identified between the remaining
combinations of cytokines (Table
I).
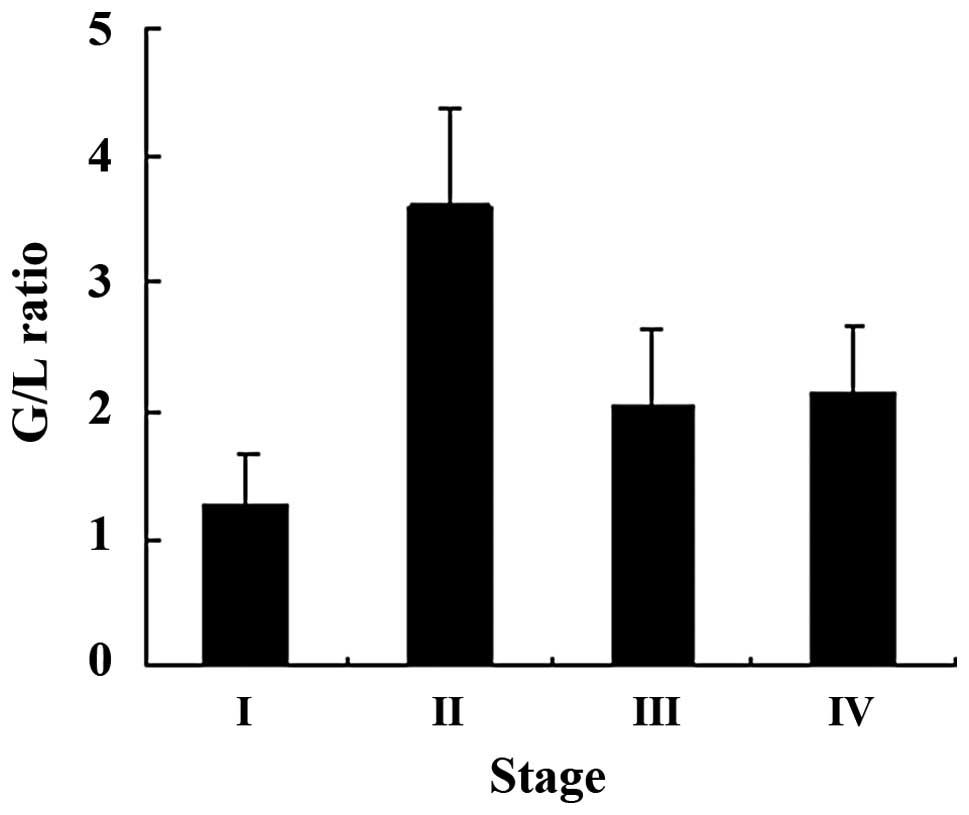
Association of G/L ratio with tumor
stage and cytokines
We investigated the association between the tumor
stage/cytokines and the G/L ratio; a significant correlation was
identified for tumor stage (P= 0.037, Fig. 2), however, the G/L ratio was not
associated with the levels of cytokines (Table I).
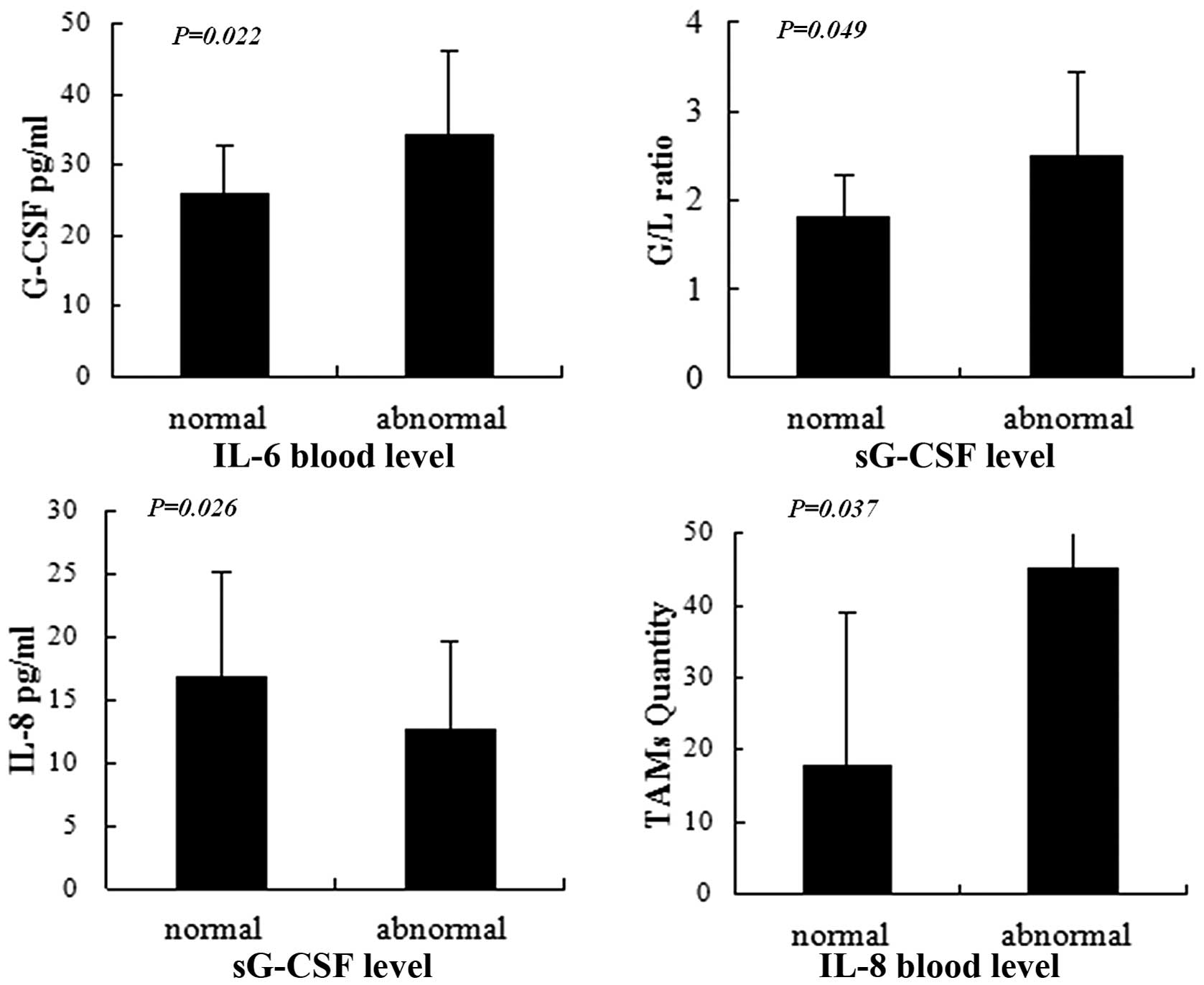
Association of cytokines with TIGs and
TAMs
The patients were divided into groups for normal or
abnormal cytokine levels. Kruskal-Wallis testing revealed that the
level of sG-CSF was significantly increased in the abnormal IL-6
level group (P=0.022), the G/L ratio was significantly increased in
the abnormal sG-CSF level group (P=0.049), the level of IL-8 was
significantly decreased in the abnormal sG-CSF level group
(P=0.026) and TAM levels were significantly increased in the
abnormal IL-8 level group (P=0.037; Fig. 3).
Association of cytokines, TIGs and
TAMs with clinico-pathological factors
Analysis revealed that sG-CSF was significantly
associated with the depth of tumor invasion (P=0.039) and a more
advanced tumor stage (P=0.023). However, significant correlation
was not identified between cytokines and lymph node metastasis and
between TIGs or TAMs and tumor stage, depth of invasion and lymph
node metastasis (Table II).
| Table IIAssociation of cytokines with
clinicopathological factors. |
Table II
Association of cytokines with
clinicopathological factors.
| Variable | Cytokines according
to tumor features (pg/ml) |
|---|
|
|---|
| Lymph node
metastasis | Depth of
invasion | Tumor stage |
|---|
|
|
|
|---|
| Absent | Present | P-value | Under muscle
layera | Beyond muscle
layer | P-value | Stage 0 and I | Stage II, III and
IV | P-value |
|---|
| sG-CSF | 26.5±7.6 | 32.2±11.2 | NS | 23.9±4.1 | 31.4±11.1 | 0.039 | 22.7±4.1 | 32.4±10.7 | 0.023 |
| sM-CSF | 504±241.4 | 359.2±172.5 | NS | 407.3±208.82 | 399±138.9 | NS | 470.7±295.1 | 389.0±188.9 | NS |
| IL-1β | 0.32±0.2 | 0.28±0.2 | NS | 0.4±0.3 | 0.2±0.1 | 0.086 | 0.35±0.2 | 0.28±0.2 | NS |
| IL-6 | 23.3±62.5 | 5.0±7.1 | NS | 2.4±1.4 | 12.9±17.2 | NS | 2.52±2.1 | 12.48±38.4 | NS |
| IL-8 | 10.9±4.2 | 16.1±14.4 | NS | 9.9±2.0 | 16.0±8.9 | NS | 10.2±2.5 | 15.6±13.6 | NS |
| TNF-α | 1.0±0.6 | 1.3±0.4 | NS | 1.0±0.3 | 1.2±0.6 | NS | 1.0±0.5 | 1.2±0.8 | NS |
| TIGs | 33.9±12.5 | 53.1±22.9 | 0.065 | 40.3±16.5 | 49.5±23.1 | NS | 40.6±18.2 | 50.2±21.9 | NS |
| TAMs | 32.4±16.8 | 32.5±28.3 | NS | 42.6±22.5 | 29.4±25.5 | NS | 46.2±39.0 | 26.6±20.4 | NS |
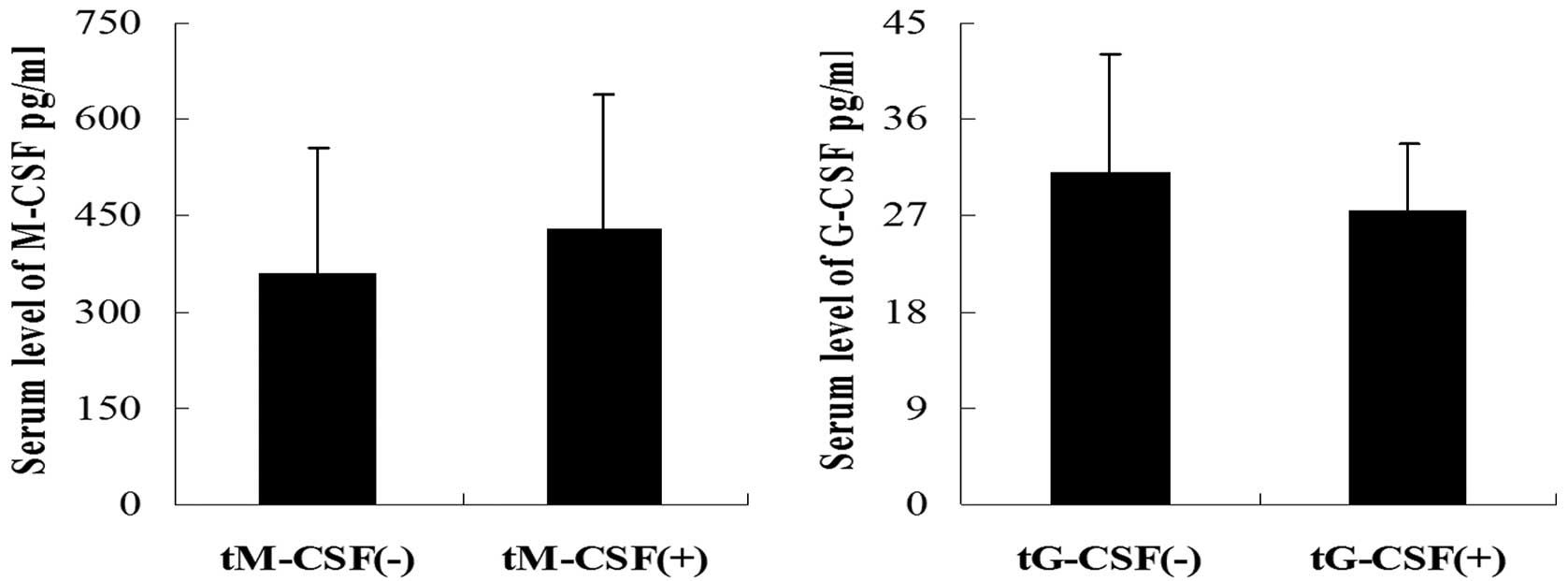
Detection of tM-CSF and tG-CSF by
immunostaining
Immunostaining, which used antibodies against tM-CSF
and tG-CSF (Fig. 1), revealed that
tM-CSF and tG-CSF in tumor cells was detected in 17/30 (56.7%) and
5/30 (16.7%) of cases, respectively. No significant correlation was
identified between CSF expression in tumor cells and the serum
levels of CSF for M-CSF (P=0.442) or G-CSF (P=0.498; Fig. 4).
Logistic regression analysis of risk
factors for lymph node metastasis and depth of tumor invasion
Logistic univariate analysis revealed that TIGs were
correlated with lymph node metastasis, however, in logistic
multivariate analysis, they were not identified as a significant
independent risk factor for lymph node metastasis (P=0.069).
Logistic univariate analysis also revealed that levels of TAMs were
correlated with depth of invasion, however, in logistic
multivariate analysis, they were not identified as an independent
risk factor for depth of invasion (P=0.063; Table III).
| Table IIILogistic regression analysis of risk
factors for lymph node metastasis and depth of invasion. |
Table III
Logistic regression analysis of risk
factors for lymph node metastasis and depth of invasion.
| | Multivariate
|
|---|
| Variable | Univariate
P-value | P-value | RR (95% CI) |
|---|
| Lymph node
metastasisa |
| G-CSF | 0.269 | | |
| M-CSF | 0.124 | | |
| IL-1β | 0.731 | | |
| IL-6 | 0.15 | | |
| IL-8 | 0.703 | | |
| TNF-α | 0.452 | | |
| TIGs | 0.019 | 0.069 | 1.087
(0.994–1.188) |
| TAMs | 0.353 | | |
| sG-CSF | 0.517 | | |
| sM-CSF | 0.676 | | |
| Depth of
invasionb |
| G-CSF | 0.083 | 0.071 | 1.301
(0.978–1.733) |
| M-CSF | 0.939 | | |
| IL-1β | 0.083 | | |
| IL-6 | 0.517 | | |
| IL-8 | 0.567 | | |
| TNF-α | 0.59 | | |
| TIGs | 0.262 | | |
| TAMs | 0.029 | 0.063 | 0.64
(0.927–1.002) |
| sG-CSF | 0.619 | | |
| sM-CSF | 0.422 | | |
Discussion
This study aimed to clarify the correlation between
pro-inflammatory cytokines, immune cells and tumors. This has
previously been investigated by numerous studies, which showed that
cytokines regulate cell growth and, more importantly, cell
proliferation, and they may be produced by tumor or immune cells.
However, the role of cytokines in inducing granulocytes or
macrophages to become involved in the anti-tumor immune response
was unclear.
G-CSF is produced by normal monocytes, macrophages
and granulocytes. In the present study, we identified abnormal
levels of sG-CSF in 17/30 (56.7%) cases, however, only a few cases
of G-CSF-producing colorectal carcinomas have ever been reported.
We also examined tG-CSF expression in tumor cells using
immunohistochemical staining. A reaction for tG-CSF was observed in
only 5 cases and this was not associated with the level of sG-CSF
(P=0.498). The levels of immunoreactive sM-CSF, IL-1β, IL-6, IL-8
and TNF-α were measured by ELISA and a positive linear correlation
was identified between the levels of IL-6 and sM-CSF. The level of
sG-CSF was significantly increased in the abnormal IL-6 level
group. M-CSF expression in tumor cells was examined using
immunostaining and immunoreactivity was observed in 17/30 (56.7%)
cases, which is similar to results from previous studies on M-CSF
production by tumor cells (13–16).
However, only 4 patients (19%) had abnormal levels of sM-CSF and
there was no significant correlation between tM-CSF and sM-CSF
(P=0.442). A study by Ashizawa et al(17) showed that immunohistochemical
staining revealed positive results for IL-6 expression in the
cytoplasm of colorectal cancer cells in patients with a high serum
level of IL-6, however there was no evidence of positive results
for IL-6 expression in patients with a normal serum level of IL-6.
This suggests that IL-6 may be able to induce the production of
CSFs from numerous types of cells, in addition to tumors (16). IL-6 is a pleiotropic cytokine which
is secreted by a wide variety of cell types, including lymphocytes,
monocytes and tumor cells (17,18).
Sato et al(19) demonstrated
that IL-6, sG-CSF and sM-CSF appear to contribute to neutrophilia
in cases of anaplastic thyroid carcinoma. A high count of
peripheral neutrophils was correlated with poor prognosis in
patients with a variety of cancer types, including breast, head and
neck cancer and sarcoma (20–24).
Therefore, we measured the G/L ratio, which
represents the relative number of these two major leukocyte
populations, indicates fluctuations in their numbers and reveals
their potential impact on the progression and prognosis of cancer.
Hence, the G/L ratio, which is easily measured in a clinical
setting, is a valuable indicator of tumor progression (25) and is useful for selecting patients
who are appropriate for surgery (26). Our results revealed that the G/L
ratio was significantly associated with a more advanced tumor stage
(P=0.037) and it was significantly increased in the abnormal sG-CSF
level group. Thus it is hypothesized that sG-CSF, sM-CSF and IL-6
may indirectly assist tumor growth and progression by neutrophilia.
Next, we analyzed the correlation between cytokines and tumor
features. The results revealed that sG-CSF levels were positively
associated with deeper tumor invasion and a more advanced tumor
stage.
In carcinogenesis, cytokines and chemokines from
tumor cells are able to build a supportive microenvironment and
induce inflammatory cells, which contribute to tumor growth,
progression and metastasis (27–29).
In this study, measuring the quantity of TIGs and TAMs revealed
that levels of TIGs were increased with tumor progression, however
TAM levels were decreased. Next, the correlation between cytokines
and TIGs or TAMs was tested; a significantly positive correlation
was identified between IL-8 and TAMs and the IL-8 level was
significantly decreased in the high sG-CSF level group. Based on
the above-mentioned results for sG-CSF, we hypothesized that IL-8
should decrease with tumor progression, however, the present study
failed to demonstrate this. This may be due to the complicated role
of TAMs in tumor progression; since TAMs have a dual role in
neoplasms, it is difficult to accurately evaluate the correlation
between IL-8 and TAMs. IL-8 is known to recruit inflammatory
neutrophils and promote the interaction between tumor cells and
inflammatory cells (30) and it is
also a potent angiogenic and growth factor in malignant tumors
(31,32). Therefore, we hypothesized that IL-8
may selectively induce the infiltration of immune cells into
tumors, in order to assist tumor progression. The present study
evaluated the risk factors for lymph node metastasis and depth of
invasion by logistic regression analysis. Univariate analysis
revealed that TIGs were correlated with lymph node metastasis,
however, logistic multivariate analysis determined that P=0.069,
which is close to 0.05. Further univariate analysis revealed that
TAMs were correlated with depth of invasion and multivariate
analysis revealed that P=0.063, which is also close to 0.05. It is
possible that significant results were not obtained due to the
small sample size, however, we believe that TIGs and TAMs should be
risk factors for lymph node metastasis and depth of invasion,
respectively.
Due to the pleiotropy of cytokines, it is difficult
to confirm the roles of cytokines in the growth and progression of
tumors. However, the present study reveals a correlation between
tumors and immune cells, which secrete cytokines, and this suggests
that cytokines may indirectly promote the growth, progression and
metastasis of tumors..
Acknowledgements
The authors thank Tsutomu Kohda for
technical assistance.
References
|
1
|
Schoenfeld J, Jinushi M, Nakazaki Y, et
al: Active immunotherapy induces antibody responses that target
tumor angiogenesis. Cancer Res. 70:10150–10160. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Noori S, Taghikhani M, Hassan ZM, Allameha
A and Mostafaei A: Tehranolide molecule modulates the immune
response, reduce regulatory T cell and inhibits tumor growth in
vivo. Mol Immunol. 47:1579–1584. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lesterhuis WJ, Punt CJ, Hato SV, et al:
Platinum-based drugs disrupt STAT6-mediated suppression of immune
responses against cancer in humans and mice. J Clin Invest.
121:3100–3108. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wieder T, Braumüller H, Kneilling M,
Pichler B and Röcken M: T cell-mediated help against tumors. Cell
Cycle. 7:2974–2977. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Forte G, Sorrentino R, Montinaro A, et al:
Inhibition of CD73 improves B cell-mediated anti-tumor immunity in
a mouse model of melanoma. J Immunol. 189:2226–2233. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kandasamy M, Bay BH, Lee YK and Mahendran
R: Lactobacilli secreting a tumor antigen and IL15 activates
neutrophils and dendritic cells and generates cytotoxic T
lymphocytes against cancer cells. Cell Immunol. 271:89–96. 2011.
View Article : Google Scholar
|
|
7
|
Schwandt A, Garcia JA, Elson P, et al:
Clinical and immunomodulatory effects of celecoxib plus
interferon-alpha in metastatic renal cell carcinoma patients with
COX-2 tumor immunostaining. J Clin Immunol. 31:690–698. 2011.
View Article : Google Scholar
|
|
8
|
Yamamoto M, Kamigaki T, Yamashita K, et
al: Enhancement of anti-tumor immunity by high levels of Th1 and
Th17 with a combination of dendritic cell fusion hybrids and
regulatory T cell depletion in pancreatic cancer. Oncol Rep.
22:337–343. 2009.PubMed/NCBI
|
|
9
|
Kuper H, Adami HO and Trichopoulos D:
Infections as a major preventable cause of human cancer. J Intern
Med. 248:171–183. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mareel M and Madani I: Tumour-associated
host cells participating at invasion and metastasis: targets for
therapy? Acta Chir Belg. 106:635–640. 2006.PubMed/NCBI
|
|
11
|
de Visser KE and Coussens LM: The
inflammatory tumor micro-environment and its impact on cancer
development. Contrib Microbiol. 13:118–137. 2006.
|
|
12
|
Kenny PA and Bissell MJ: Tumour reversion:
correction of malignant behavior by microenvironmental cues. Int J
Cancer. 107:688–695. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Revoltella RP, Menicagli M and Campani D:
Granulocyte-macrophage colony-stimulating factor as an autocrine
survival-growth factor in human gliomas. Cytokine. 57:347–359.
2012. View Article : Google Scholar
|
|
14
|
Curran CS, Evans MD and Bertics PJ: GM-CSF
production by glioblastoma cells has a functional role in
eosinophil survival, activation, and growth factor production for
enhanced tumor cell proliferation. J Immunol. 187:1254–1263. 2011.
View Article : Google Scholar
|
|
15
|
Liao HH, Wang YC, Chen MC, et al:
Down-regulation of granulocyte-macrophage colony-stimulating factor
by 3C-like proteinase in transfected A549 human lung carcinoma
cells. BMC Immunol. 12:162011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Inoue H, Iga M, Nabeta H, et al:
Non-transmissible Sendai virus encoding granulocyte macrophage
colony-stimulating factor is a novel and potent vector system for
producing autologous tumor vaccines. Cancer Sci. 99:2315–2326.
2008. View Article : Google Scholar
|
|
17
|
Ashizawa T, Okada R, Suzuki Y, et al:
Study of interleukin-6 in the spread of colorectal cancer: the
diagnostic significance of IL-6. Acta Med Okayama. 60:325–330.
2006.PubMed/NCBI
|
|
18
|
Bao B, Ahmad A, Kong D, et al: Hypoxia
induced aggressiveness of prostate cancer cells is linked with
deregulated expression of VEGF, IL-6 and miRNAs that are attenuated
by CDF. PLoS One. 7:e437262012. View Article : Google Scholar
|
|
19
|
Sato T, Omura M, Saito J, Hirasawa A,
Kakuta Y, Wakabayashi Y and Nishikawa T: Neutrophilia associated
with anaplastic carcinoma of the thyroid: production of macrophage
colony-stimulating factor (M-CSF) and interleukin-6. Thyroid.
10:1113–1118. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Riesco A: Five-year cancer cure: relation
to total amount of peripheral lymphocytes and neutrophils. Cancer.
25:135–140. 1970.PubMed/NCBI
|
|
21
|
Atzpodien J, Royston P, Wandert T and
Reitz M: DGCIN - German Cooperative Renal Carcinoma
Chemo-Immunotherapy Trials Group: Metastatic renal carcinoma
comprehensive prognostic system. Br J Cancer. 88:348–353. 2003.
View Article : Google Scholar
|
|
22
|
Négrier S, Escudier B, Gomez F, et al:
Prognostic factors of survival and rapid progression in 782
patients with metastatic renal carcinomas treated by cytokines: a
report from the Groupe Français d'Immunothérapie. Ann Oncol.
13:1460–1468. 2002.
|
|
23
|
Donskov F and von der Maase H: Impact of
immune parameters on long-term survival in metastatic renal cell
carcinoma. J Clin Oncol. 24:1997–2005. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schmidt H, Suciu S, Punt CJ, et al
American Joint Committee on Cancer Stage IV Melanoma; EORTC 18951:
Pretreatment levels of peripheral neutrophils and leukocytes as
independent predictors of overall survival in patients with
American Joint Committee on Cancer Stage IV Melanoma: results of
the EORTC 18951 Biochemotherapy Trial. J Clin Oncol. 25:1562–1569.
2007. View Article : Google Scholar
|
|
25
|
Liu H, Tabuchi T, Takemura A, et al: The
granulocyte/lymphocyte ratio as an independent predictor of tumour
growth, metastasis and progression. Mol Med Rep. 1:699–704.
2008.PubMed/NCBI
|
|
26
|
Ietomi K: A study on the role of
granulocytes in carcinoma-bearing hosts - G/L ratio as a new host
indicator. Nippon Gan Chiryo Gakkai Shi. 25:662–671. 1990.(In
Japanese).
|
|
27
|
Lee YS, Choi I, Ning Y, et al:
Interleukin-8 and its receptor CXCR2 in the tumour microenvironment
promote colon cancer growth, progression and metastasis. Br J
Cancer. 106:1833–1841. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jung MY, Kim SH, Cho D and Kim TS:
Analysis of the expression profiles of cytokines and
cytokine-related genes during the progression of breast cancer
growth in mice. Oncol Rep. 22:1141–1147. 2009.PubMed/NCBI
|
|
29
|
Balkwill F and Mantovani A: Inflammation
and cancer: back to Virchow? Lancet. 357:539–545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Arenberg DA, Kunkel SL, Polverini PJ,
Glass M, Burdick MD and Strieter RM: Inhibition of interleukin-8
reduces tumori-genesis of human non-small cell lung cancer in SCID
mice. J Clin Invest. 97:2792–2802. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ferrara N and Davis-Smyth T: The biology
of vascular endothelial growth factor. Endocr Rev. 18:4–25. 1997.
View Article : Google Scholar
|
|
32
|
Mizukami Y, Jo WS, Duerr EM, et al:
Induction of interleukin-8 preserves the angiogenic response in
HIF-1alpha-deficient colon cancer cells. Nat Med. 11:992–997.
2005.PubMed/NCBI
|