Introduction
The spine is the most common site of skeletal
metastases, with >18,000 new cases of spinal metastases
recognized annually (1,2). Between 5 and 10% of patients with
systemic cancer develop vertebral metastases (3–6). The
thoracic spine is the most common region involved in spinal
metastases (70%), followed by the lumbar spine (20%), while the
cervical region is affected in 10% of cases (7). Lung, prostate, breast, renal cell,
thyroid and gastrointestinal carcinomas are the most common tumors
that metastasize to the spinal column (4,8–10). The
most common symptom in cervical metastases is neck pain which
occurs in 90% of patients; 50% of cases complain of severe
deficits, such as acute weakness that may progress to quadriplegia
(11–13). The median survival time after the
first detection of skeletal metastasis is 3–6 months in squamous
cell lung carcinoma, 20 months in breast carcinoma and 40 months in
prostate carcinoma (14).
Metastatic destruction of the vertebral bodies may
result in pathological compression fractures, leading to angulated
kyphotic deformities that may be observed clinically or in imaging
studies (15,16). The upper cervical spine has the
largest spinal canal and therefore neurological symptoms typically
result from instability rather than compressive insult (16). The occipitoatlantoaxial spine is
rarely affected, particularly the C1 vertebra.
The majority of vertebral metastases originate via
hematogenous dissemination from primary carcinomas of the breast,
lung or prostate (17). In the
osteolytic form of vertebral metastasis, tumor cells infiltrate the
trabecular matrix of the bone, resulting in a loss of osseous
integrity, predisposing the spine to pathological fractures
(14).
Radiotherapy (RT) is important in palliating the
symptoms of patients with metastatic disease. RT techniques are
used in a broad range of circumstances, including as a prophylactic
measure against future pathological fractures and palliation of
bone pain, as well as severe symptoms associated with cord
compression and impending neurological compromise.
The beneficial effect of achieving analgesia of bone
metastases with RT is well documented. The response to RT has been
quantified and qualified with numerous criteria and instruments
over the past decades. Additionally, evidence reveals that 70–90%
of patients achieve a beneficial response due to analgesic-directed
RT with complete responses observed in up to 40% of patients
(18–20).
Modern advances in computer technology and the
delivery of RT have led to the development of treatment techniques,
such as 3-dimensional (3D) conformal, intensity-modulated and
proton beam therapy. However, since the majority of spinal tumors
are metastases, spinal RT is often delivered using conventional
2-dimensional (2D) or 3D conformal techniques.
Case report
The patient was a 31-year-old female suffering from
neck pain for 1 month prior to the discovery of a mass in the neck.
A physical examination revealed a tender mass and motion in the
cervical vertebrae was limited. At the time of examination, the
patient’s neck pain was constant in the suboccipital region, rated
at 3–4 out of 10 on a pain scale. Upon any movement, however, the
ache became a sharp pain, rated at 7–8 out of 10. The patient had
no history of neck trauma. Initial lateral and anteroposterior
open-mouth cervical spine radiographs and computed tomography (CT)
of the cervical spine were obtained when the patient first
experienced neck pain. The CT revealed osteolytic destruction
involving the C1 vertebra (images not shown).
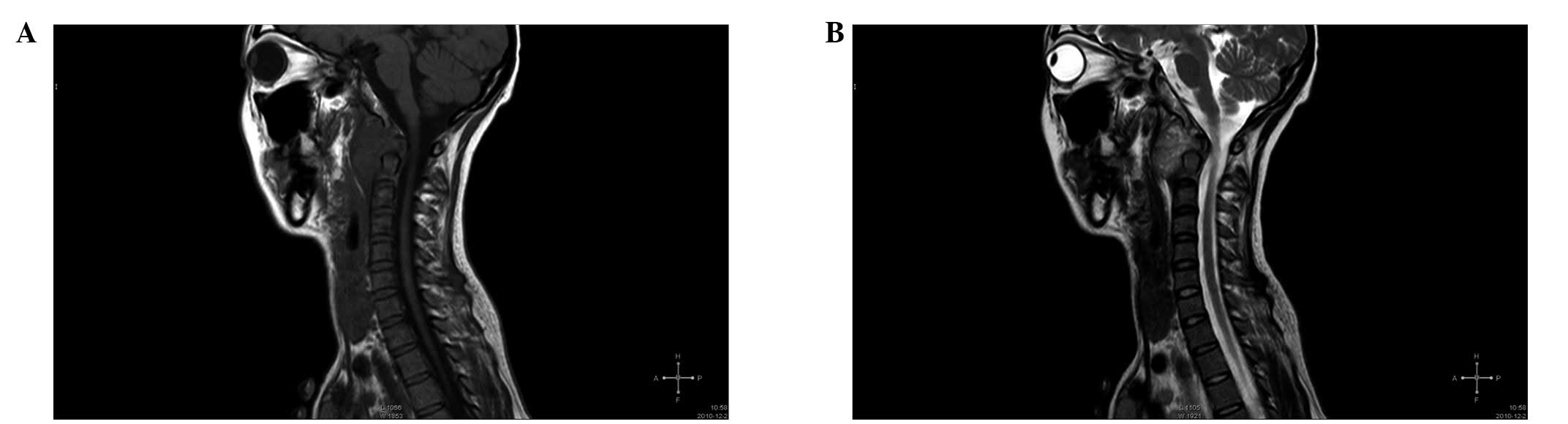
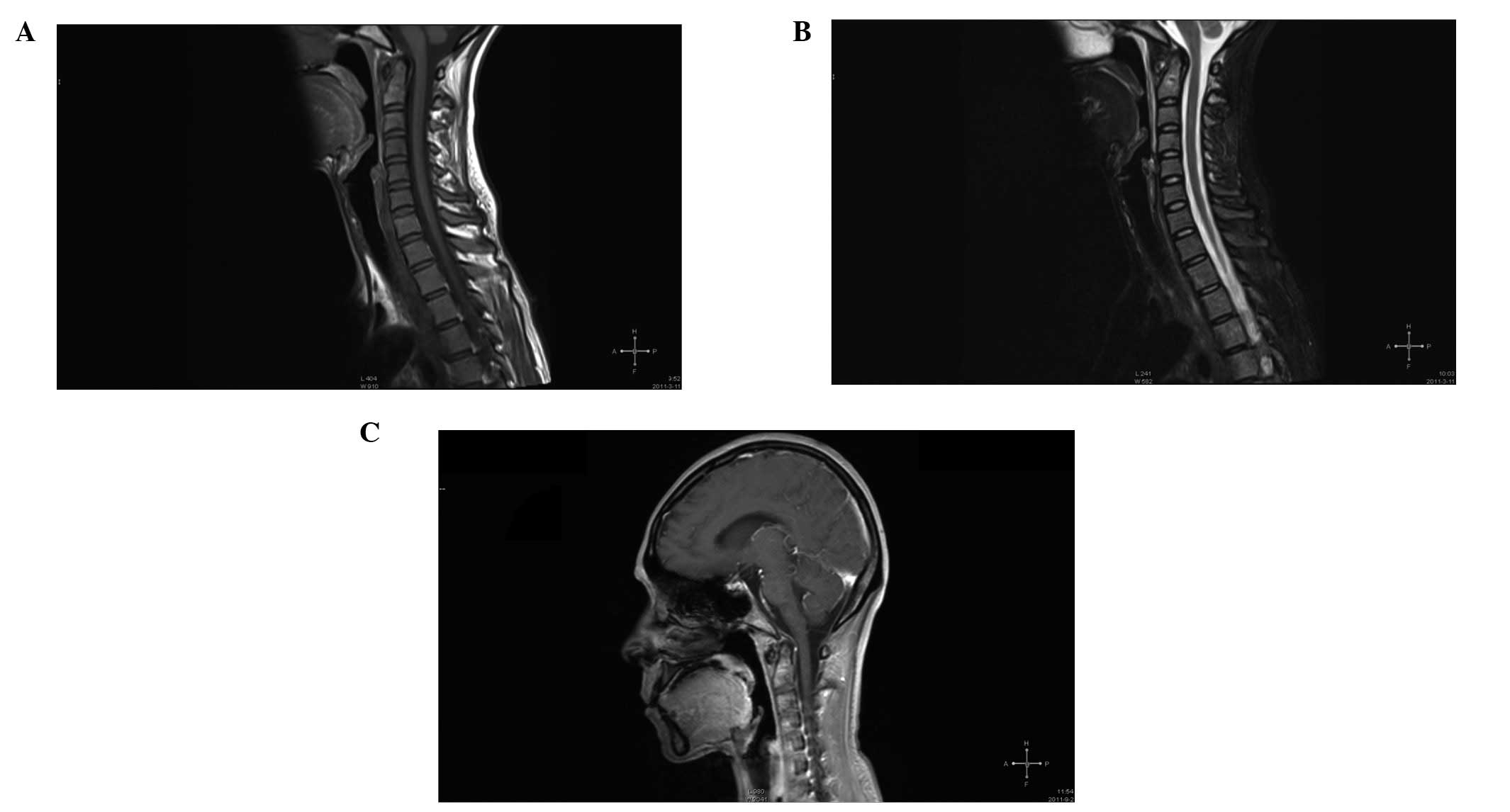
Magnetic resonance imaging (MRI) scans revealed an
extremely large tumor centered on the C1 vertebra, as well as a
soft tissue mass beside the C1 vertebra, which extended into the
anterior aspects of C2 (Fig. 1).
MRI is the most sensitive test available for the evaluation of the
soft tissue extent of the tumor. The MRI appearance was
nonspecific, with T1-weighted images showing a low signal (Fig. 1A) and T2-weighted images showing an
intermediate-to-high signal within the mass (Fig. 1B).
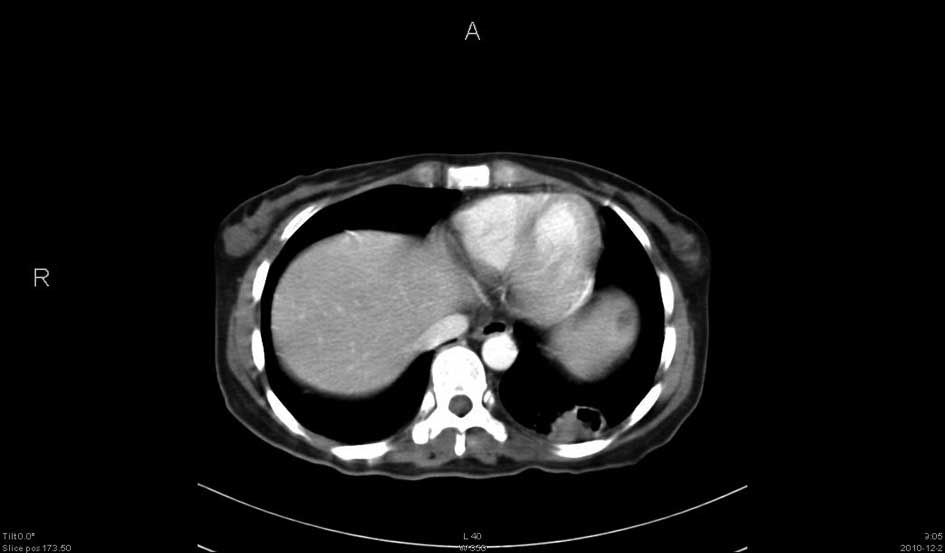
Chest and CT scans then revealed lung carcinoma
changes involving the left lung (Fig.
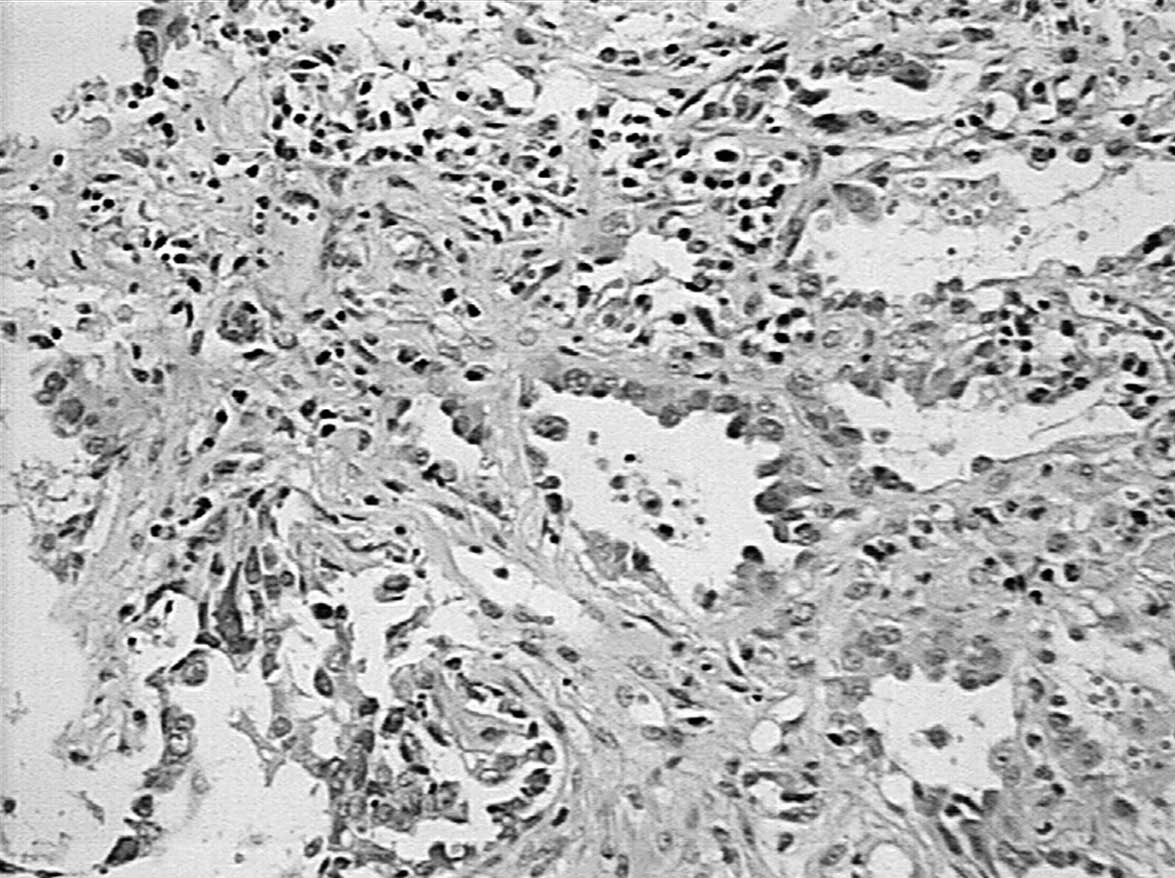
2). A paraffinized section of a biopsy obtained via
bronchoscopy was stained with HE. The biopsy confirmed
adenocarcinoma of the left lung (Fig.
3).
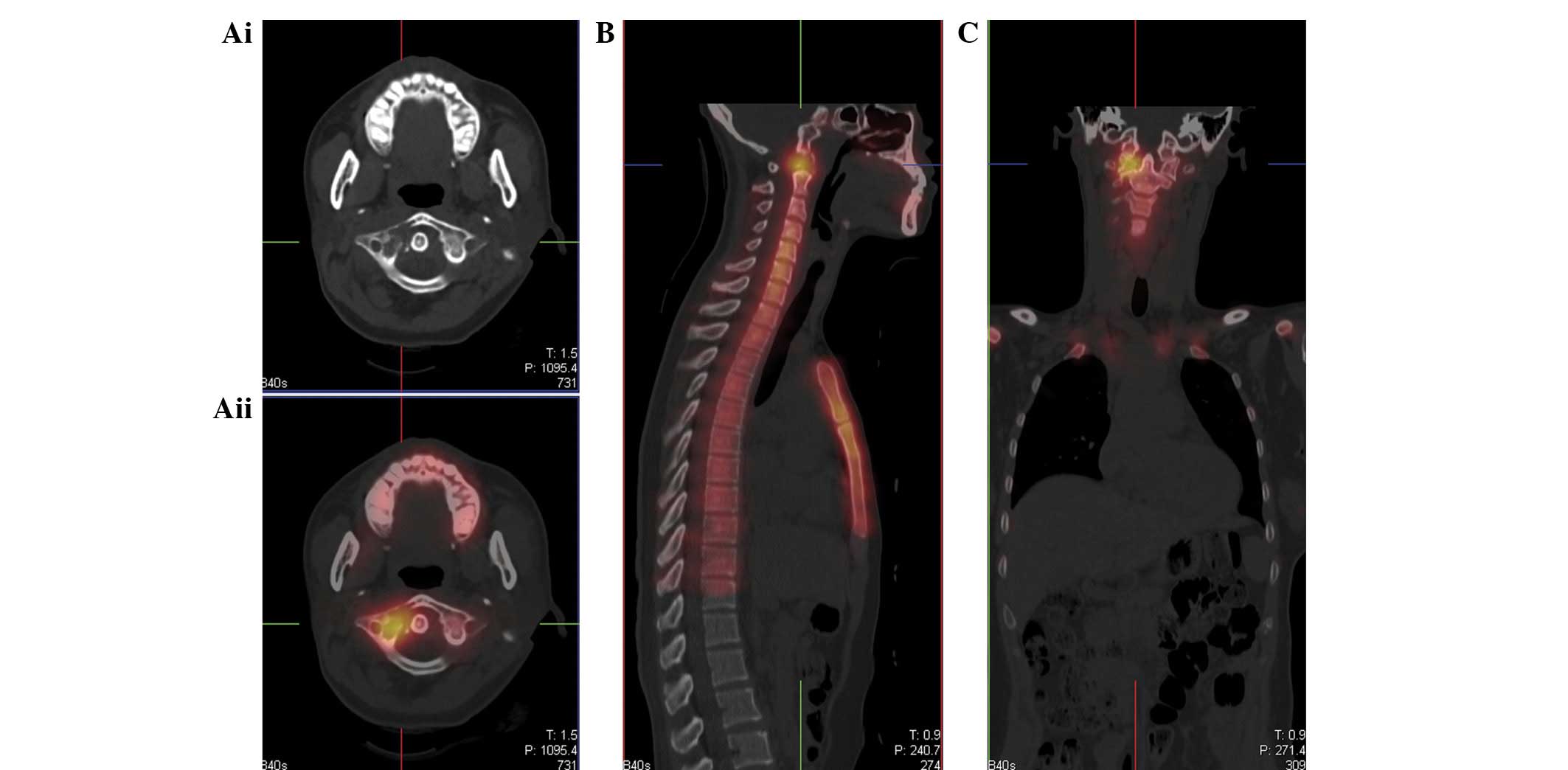
Axial CT scanning showed evident osteolytic
destruction of the C1 vertebra (Fig.
4Ai). A whole-body radionuclide bone scan exhibited increased
pharmaceutical uptake in the region of the known lesion in the
upper cervical spine (Fig. 4Aii, B and
C), as well as the proximal portion of the left femur (images
not shown), consistent with further metastatic infiltration. The
patient was then fitted with a rigid cervical spine brace in an
attempt to stabilize the spine and limit cord compression.
Neurosurgeons were consulted and declined to
intervene due to the poor overall prognosis and the patient elected
to avoid aggressive treatment. A management plan, consisting of
radiation therapy on the cervical spine, analgesic medication and
close monitoring with radiography and advanced imaging, was
initiated.
The patient agreed to proceed with radiation therapy
for the disease after the first MRI scan. The schedule was
conventional RT with 5 daily 4-Gy fractions. After RT, the patient
felt that the pain had been significantly relieved and reported no
swallowing dysfunction. Chemotherapy was administered after the RT.
Subsequent follow-up MRI scans at 3 (Fig. 5A and B) and 9 months (Fig. 5C) after RT revealed no progression
of the osseous destruction. At 3 months after RT, the rigid
cervical spine brace was removed from the patient. At present, the
overall survival (OS) time is 11 months. At the 9-month follow-up
examination, the main neck symptoms had disappeared.
Discussion
The present study describes the case of a patient
undergoing cervical spine radiation therapy for a known lung cancer
who was referred to a neck pain department.
Spinal symptoms are the first indication of skeletal
metastasis in 20% of cancer patients (15). The most common clinical feature in a
patients with vertebral metastases is pain, although neurological
symptoms may also be present (17).
Trivial trauma should be taken seriously in patients with cancer
and evaluated with appropriate diagnostic imaging.
The most widely available imaging modality is
conventional radiography. However, bone scans are relatively
nonspecific and present difficulties in differentiating between
infection, fracture, spondylosis and tumors (16). MRI is sensitive and specific and has
become the gold standard for evaluating vertebral metastases
(17,21,22).
MRI is extremely sensitive to pathological changes in bone marrow,
as well as the detection of cord and nerve compression (17).
Prior to RT, cervical spine biopsies had not been
obtained from the patient since biopsies of the cervical spine have
significant risks as the tumor is surrounded by the vertebral
artery, spinal cord and nerve root.
In general, the treatment of spinal tumors is
surgical and en bloc resection with negative margins has been shown
to decrease the rates of local and metastatic recurrence (23–26).
En bloc resection is now the standard of care for numerous primary
tumors of the thoracic, lumbar and sacral spine. However, several
factors complicate the performing of this procedure in the cervical
spine, including the proximity of the vertebral arteries, intricate
bony architecture and importance of the cervical nerve roots.
Furthermore, en bloc excision of cervical spinal tumors involves
long operative times and significant perioperative morbidity.
It is difficult to remove tumors en bloc from the
cervical spine and there is a high rate of recurrence and
metastasis. Due to these factors, as well as the relative rarity of
cases, this technique has not been widely adopted in the cervical
spine.
RT may be used in place of surgery, serve as an
adjunct to surgery or as a preparative regimen to make a tumor more
readily resectable. RT in the complicated and uncomplicated spinal
metastasis setting is commonly prescribed for the posterior wall of
the vertebral body (or anterior aspect of the spinal cord proper).
There is no standard treatment approach insofar as there are
numerous dose fractionation schedules for uncomplicated spinal
skeletal metastasis.
The majority of practitioners prefer a more
protracted course of RT in cases of cord compression and courses
vary from 5 daily fractions of 4 Gy to 23 daily fractions of 2 Gy
(19). In the USA, the most common
schedule is 10 daily 3-Gy fractions. A number of study series
included patients treated with a single 8-Gy fraction course and no
significant difference was observed in the clinical outcomes or
late toxicity (27,28). However, the available data appear to
indicate no significant benefits of one fractionation schedule over
another when analyzing the functional outcomes (27–30).
Patients complaining of new onset back or neck pain
should be assumed to have vertebral metastasis until proven
otherwise. Trivial trauma should be taken seriously in these cases
and investigated with appropriate clinical, laboratory and imaging
examinations.
However, RT should be used with caution, as the
spinal cord is sensitive to radiation; local irradiation is
suggested. A schedule of 5 daily 4-Gy fractions was successful for
the present patient. In MRI scans, there was a nearly complete
response in the C1 vertebra.
References
|
1
|
Gokaslan ZL, York JE, Walsh GL, et al:
Transthoracic vertebrectomy for metastatic spinal tumors. J
Neurosurg. 89:599–609. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hatrick NC, Lucas JD, Timothy AR and Smith
MA: The surgical treatment of metastatic disease of the spine.
Radiother Oncol. 56:335–339. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sciubba DM and Gokaslan ZL: Diagnosis and
management of metastatic spine disease. Surg Oncol. 15:141–151.
2006. View Article : Google Scholar
|
|
4
|
Sundaresan N, Boriani S, Rothman A and
Holtzman R: Tumors of the osseous spine. J Neurooncol. 69:273–290.
2004. View Article : Google Scholar
|
|
5
|
Sundaresan N, Galicich JH, Lane JM, Bains
MS and McCormack P: Treatment of neoplastic epidural cord
compression by vertebral body resection and stabilization. J
Neurosurg. 63:676–684. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
White AP, Kwon BK, Lindskog DM,
Friedlaender GE and Grauer JN: Metastatic disease of the spine. J
Am Acad Orthop Surg. 14:587–598. 2006.PubMed/NCBI
|
|
7
|
Black P: Brain metastasis: current status
and recommended guidelines for management. Neurosurgery. 5:617–631.
1979. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Alfieri A, Mazzoleni G, Schwarz A, et al:
Renal cell carcinoma and intradural spinal metastasis with cauda
equina infiltration: case report. Spine (Phila Pa 1976).
30:161–163. 2005. View Article : Google Scholar
|
|
9
|
Andreula C and Murrone M: Metastatic
disease of the spine. Eur Radiol. 15:627–632. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Perrin RG and McBroom RJ: Metastatic
tumors of the cervical spine. Clin Neurosurg. 37:740–755.
1991.PubMed/NCBI
|
|
11
|
Liu JK, Apfelbaum RI and Schmidt MH:
Surgical management of cervical spinal metastasis: anterior
reconstruction and stabilization techniques. Neurosurg Clin N Am.
15:413–424. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu JK, Rosenberg WS and Schmidt MH:
Titanium cage-assisted polymethylmethacrylate reconstruction for
cervical spinal metastasis: technical note. Neurosurgery. 56(1
Suppl 1): E2072005.PubMed/NCBI
|
|
13
|
Wegener B, Müller PE, Jansson V, Krödel A,
Heinert G and Dürr HR: Cervical spine metastasis of multiple
myeloma: a case report with 16 years of follow-up. Spine (Phila Pa
1976). 29:E368–E372. 2004.PubMed/NCBI
|
|
14
|
Coleman RE: Skeletal complications of
malignancy. Cancer. 80(8 Suppl): 1588–1594. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Abdu WA and Provencher M: Primary bone and
metastatic tumors of the cervical spine. Spine (Phila Pa 1976).
23:2767–2777. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jenis LG, Dunn EJ and An HS: Metastatic
disease of the cervical spine. A review. Clin Orthop Relat Res.
359:89–103. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Perrin RG and Laxton AW: Metastatic spine
disease: epidemiology, pathophysiology, and evaluation of patients.
Neurosurg Clin N Am. 15:365–373. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jacobs WB and Perrin RG: Evaluation and
treatment of spinal metastases: an overview. Neurosurg Focus.
11:e102001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Agarawal JP, Swangsilpa T, van der Linden
Y, Rades D, Jeremic B and Hoskin PJ: The role of external beam
radiotherapy in the management of bone metastases. Clin Oncol (R
Coll Radiol). 18:747–760. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sze WM, Shelley M, Held I and Mason M:
Palliation of metastatic bone pain: single fraction versus
multifraction radiotherapy - a systematic review of the randomised
trials. Cochrane Database Syst Rev. 2002.CD0047212004.
|
|
21
|
Khaw FM, Worthy SA, Gibson MJ and Gholkar
A: The appearance on MRI of vertebrae in acute compression of the
spinal cord due to metastases. J Bone Joint Surg Br. 81:830–834.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sze G: Magnetic resonance imaging in the
evaluation of spinal tumors. Cancer. 67(4 Suppl): 1229–1241. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Boriani S, Bandiera S, Biagini R, et al:
Chordoma of the mobile spine: fifty years of experience. Spine
(Phila Pa 1976). 31:493–503. 2006.PubMed/NCBI
|
|
24
|
Boriani S, De Iure F, Bandiera S, et al:
Chondrosarcoma of the mobile spine: report on 22 cases. Spine
(Phila Pa 1976). 25:804–812. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Talac R, Yaszemski MJ, Currier BL, et al:
Relationship between surgical margins and local recurrence in
sarcomas of the spine. Clin Orthop Relat Res. 397:127–132. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tomita K, Kawahara N, Murakami H and
Demura S: Total en bloc spondylectomy for spinal tumors:
improvement of the technique and its associated basic background. J
Orthop Sci. 11:3–12. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hoskin PJ, Grover A and Bhana R:
Metastatic spinal cord compression: radiotherapy outcome and dose
fractionation. Radiother Oncol. 68:175–180. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rades D, Stalpers LJ, Veninga T, et al:
Evaluation of five radiation schedules and prognostic factors for
metastatic spinal cord compression. J Clin Oncol. 23:3366–3375.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Maranzano E, Bellavita R, Rossi R, et al:
Short-course versus split-course radiotherapy in metastatic spinal
cord compression: results of a phase III, randomized, multicenter
trial. J Clin Oncol. 23:3358–3365. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Rades D, Fehlauer F, Stalpers LJ, et al: A
prospective evaluation of two radiotherapy schedules with 10 versus
20 fractions for the treatment of metastatic spinal cord
compression: final results of a multicenter study. Cancer.
101:2687–2692. 2004. View Article : Google Scholar : PubMed/NCBI
|