Introduction
The most common site of breast cancer metastasis is
the bone. Other common metastatic sites include the lungs, pleura,
liver and brain (1). The majority
of metastatic lesions occur shortly after the detection of the
primary tumor (2). Metastasis to
the thyroid gland is rare (3). The
thyroid gland is also a rare site for metastatic disease to develop
(4,5) and metastatic lesions from non-thyroid
cancers are infrequent. However, since treatment strategies used to
control primary and metastatic malignancies are different, accurate
diagnosis appears important and may influence the prognosis and
likelihood of a cure for lesions of the thyroid. Therefore, when
encountering a patient with thyroid tumor, and with a long history
of breast cancer, clinicians should be aware of the possibility of
metastatic disease, until such a diagnosis can be ruled out. Then,
besides collecting full clinical information, further histological
analysis should be performed. Here, we report a case of thyroid
metastasis arising from breast cancer. The thyroid metastasis
appeared 3 years after the initial diagnosis of breast carcinoma
and was confirmed by histopathological analysis.
Case report
Clinical presentation and diagnosis
The patient, a 45-year-old female, was diagnosed
with an infiltrating ductal carcinoma in the right breast (cT3N1M0)
by fine needle aspiration biopsy in June 2009. The patient
subsequently received six cycles of neoadjuvant chemotherapy. A
follow-up mammectomy was performed in November 2009. In June 2012,
the patient presented with palpable masses on the right thyroid,
isthmus and lateral neck. Subsequently, the patient underwent a
bilateral subtotal thyroidectomy and lymphadenectomy. Histological
assessment of the surgical thyroid specimens and the neck lymph
nodes revealed multiple carcinoma foci. The microscopic and
immunohistochemical findings confirmed that the thyroid masses were
breast cancer metastases.
The primary lesion excised from the right breast was
a 20×18×15-mm infiltrating ductal carcinoma. The metastases excised
from the right and left thyroid three years later were 30×20×15 and
20×15×12 mm in size, respectively, and the lymph nodes contained
sheets of metastatic carcinoma (4/9). The diagnosis of metastatic
carcinoma was made based on immunostaining data for the estrogen
receptor (ER), progesterone receptor (PR) and CerbB-2 in neoplastic
cells. Additionally, staining for thyroglobulin (TG) and thyroid
transcription factor 1 (TTF-1), which are expressed in the thyroid
gland but not in breast cancer tissue, was performed to
differentiate the thyroid component from neoplastic breast
cells.
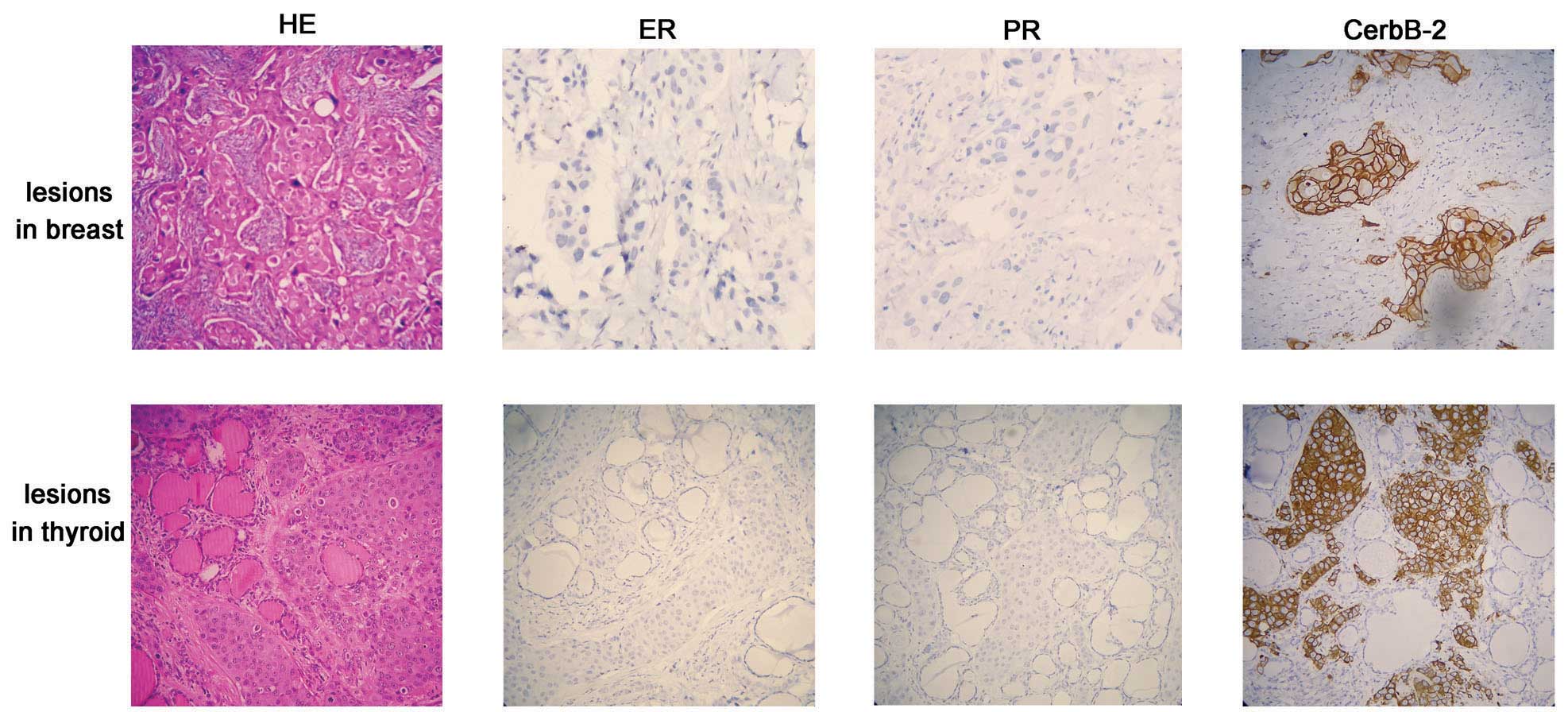
Histologically, pleomorphic tumor cells from the
breast carcinoma metastasis were intermingled with the thyroid
follicles (Fig. 1, hematoxylin and
eosin staining of the adenocarcinoma tissue in the breast and
thyroid gland). In the thyroid gland, clusters of metastatic breast
carcinoma cells were surrounded by a normal thyroid component.
Tumor cells in metastatic foci exhibited negative staining for the
ER and PR and strong positive staining for CerbB-2, similar to the
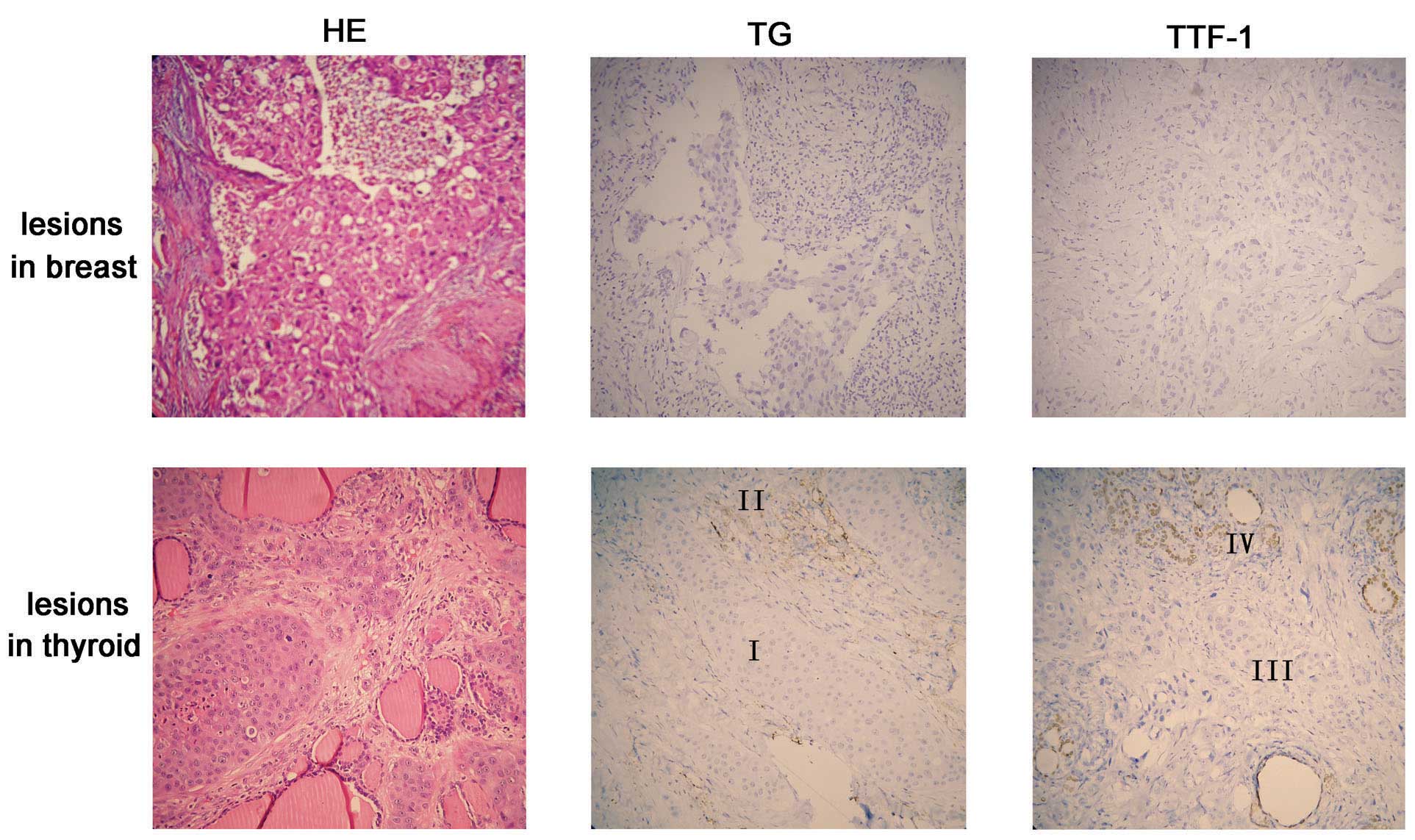
staining pattern of the primary breast lesion. The adjacent normal
thyroid tissue was positive for TTF-1 (Fig. 2, lower panel, region IV) and TG
(Fig. 2, lower panel, region II);
however, the metastatic tumor cells were negative for both markers
(Fig. 2, lower panel, regions III
and I). These two markers indicate that the cancer lesions did not
originate from the thyroid component.
Discussion
This study reports the observation of an uncommon
metastatic site (thyroid gland) of breast carcinoma in a patient
with a three-year history of breast cancer. Clinically evident
metastases of non-thyroid malignancies to the thyroid gland are
uncommon and usually, patients with metastatic thyroid lesions
present with similar symptoms to primary lesions. Particularly in
breast cancer, metastasis to the thyroid gland is rarely observed.
In addition, given the long interval between the primary cancer and
subsequent thyroid metastases, diagnosis of thyroid metastasis from
breast carcinoma may be difficult. However, importantly, the
diagnosis influences the prognosis and likelihood of a cure for
lesions of the thyroid gland, and the treatment strategy used to
control metastatic breast carcinoma is different from that used to
treat primary thyroid malignancies. Therefore, a diagnosis of
metastatic disease should be considered when new aggregates are
identified in the thyroid glands of patients with a long-term
history of breast cancer, until such a diagnosis can be ruled
out.
To ascertain metastatic breast carcinoma in the
thyroid gland, immunohistochemistry should be performed for the
detection of specific markers. There are at least two types of
marker that are required to be evaluated; the markers which possess
a similar expression status in original and metastatic lesions and
those that are capable of differentiating between metastatic
lesions and the surrounding thyroid components. Clinically, ER, PR
and CerbB-2 (HER2/neu) statuses are known to be correlated with
breast cancer. As they provide important therapeutic and prognostic
markers in the management of breast carcinoma (6), they are routinely evaluated. In this
study, immunohistochemical staining of the ER, PR and CerbB-2 in
postoperative thy roid specimens of patients were performed and
they all demonstrated a similar expression pattern with primary
breast carcinoma; negative for ER and PR, and strongly positive for
CerbB-2 (Fig. 1).
Furthermore, TG (7)
and TTF-1 (8), the functional
markers for medullary thyroid carcinoma, are useful to distinguish
breast metastatic lesions from primary thyroid lesions. As shown in
Fig. 2, normal thyroid follicular
cells, but not malignant cells, are stained strongly for TG and
TTF-1, which confirms that lesions are not thyroid in origin.
Based on the present study, we conclude that
although knowledge of a patient’s complete clinical history is
extremely useful, immunohistopathological analysis should be
performed to confirm the diagnosis of metastatic breast cancer.
Negative immunohistochemical staining for TG and TTF-1 in the
thyroid lesions and similar staining results for ER, PR and CerbB-2
in breast and thyroid lesions may aid the diagnosis of thyroid
carcinoma derived from metastatic breast cancer.
Acknowledgements
This study was supported by a grant
from the National Natural Science Foundation of China (No.
81202076).
References
|
1
|
Irvin W Jr, Muss HB and Mayer DK: Symptom
management in metastatic breast cancer. Oncologist. 16:1203–1214.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lam KY and Lo CY: Metastatic tumors of the
thyroid gland: a study of 79 cases in Chinese patients. Arch Pathol
Lab Med. 122:37–41. 1998.PubMed/NCBI
|
|
3
|
Gerges AS, Shehata SR and Gouda IA:
Metastasis to the thyroid gland; unusual site of metastasis. J
Egypt Natl Canc Inst. 18:67–72. 2006.PubMed/NCBI
|
|
4
|
Chen H, Nicol TL and Udelsman R:
Clinically significant, isolated metastatic disease to the thyroid
gland. World J Surg. 23:177–180. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Willis RA: Metastatic Tumours in the
Thyreoid Gland. Am J Pathol. 7:187–208. 1931.PubMed/NCBI
|
|
6
|
Idirisinghe PK, Thike AA, Cheok PY, et al:
Hormone receptor and c-ERBB2 status in distant metastatic and
locally recurrent breast cancer. Pathologic correlations and
clinical significance. Am J Clin Pathol. 133:416–429. 2010.
View Article : Google Scholar
|
|
7
|
Wagner K, Arciaga R, Siperstein A, et al:
Thyrotropin receptor/thyroglobulin messenger ribonucleic acid in
peripheral blood and fine-needle aspiration cytology: diagnostic
synergy for detecting thyroid cancer. J Clin Endocrinol Metab.
90:1921–1924. 2005. View Article : Google Scholar
|
|
8
|
Katoh R, Miyagi E, Nakamura N, et al:
Expression of thyroid transcription factor-1 (TTF-1) in human C
cells and medullary thyroid carcinomas. Hum Pathol. 31:386–393.
2000. View Article : Google Scholar
|