Introduction
Carcinosarcoma is a rare tumor that is characterized
by malignant epithelial and mesenchymal components. These tumors
have been reported in a number of different organs, including the
uterus, lung, esophagus, kidney and pancreas (1). Carcinosarcoma of the gallbladder is
extremely rare. To date, <100 cases have been reported in the
English literature. Here, we report a case of carcinosarcoma of the
gallbladder accompanied with tumor thrombi. Written informed
consent was obtained from the patient.
Case report
Clinical presentation and diagnosis of
cancer
A 68-year-old female was admitted to the Huashan
Hospital (Shanghai, China) with right upper abdominal pain and
jaundice. The patient reported a past medical history of chronic
cholecystitis, cholecystolithiasis and tuberculosis. A physical
examination revealed a body temperature of 38.2°C and tenderness in
the right upper quadrant of the abdomen. A laboratory analysis
revealed leukocytosis (1.7×104 cells/mm3).
The tumor marker, serum carcinoembryonic antigen, carbohydrate
antigen 19-9 and α-fetoprotein (AFP) levels were elevated to 33.67
μg/l, 54.22 U/ml and 312.7 μg/l, respectively. In
addition, liver function tests revealed that the serum
concentrations of alanine aminotransferase and alkaline phosphatase
were increased to 411 U/l and 686 U/l, respectively. In addition,
the total bilirubin levels were increased to 35.3 μmol/l.
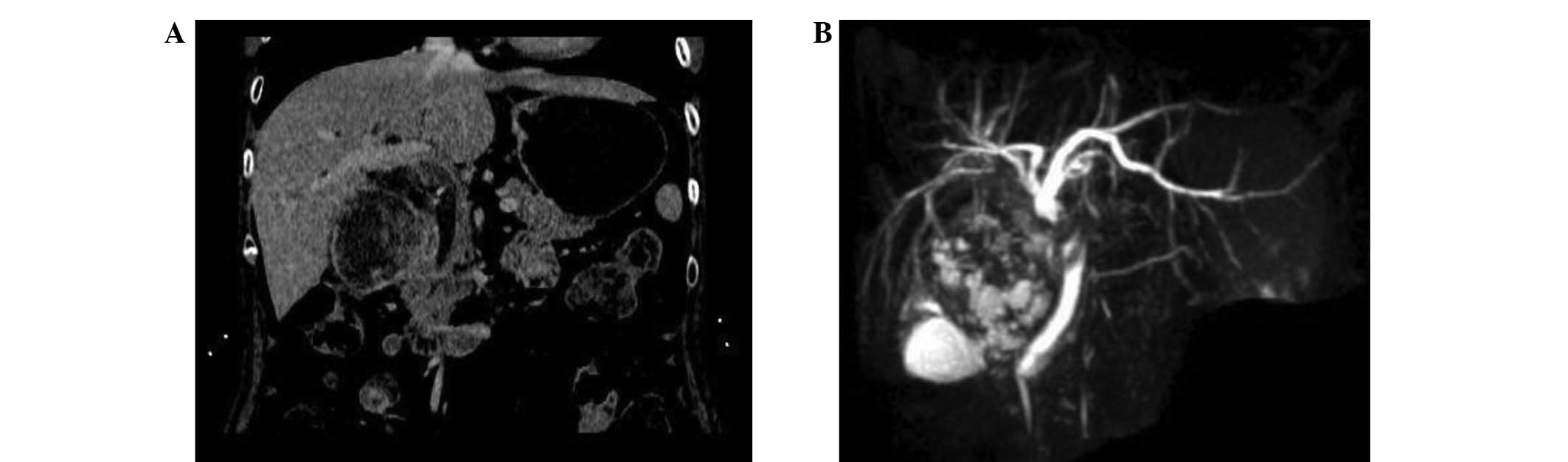
Computed tomography (CT), three-dimensional reconstructions of this
CT (Fig. 1A), ultrasonography and
magnetic resonance cholangiopancreatography (Fig. 1B) indicated a large solid mass
lesion in the gallbladder. Finally, a cholecystectomy with liver
segmentectomy (S4a+S5) and a lymph node dissection were performed.
The analysis of an intraoperative frozen section demonstrated that
the soft tissue lump in the common bile duct was formed from tumor
thrombi. Following this, a resection of the extrahepatic bile duct
and a Roux-en-Y type hepatic cholangiojejunostomy were
performed.
Tumor characteristics
Upon gross examination of the surgical specimen, a
cross section revealed a 10×7×5-cm pedunculated polypoid solid mass
with hemorrhagic and necrotic changes, protruding into the lumen of
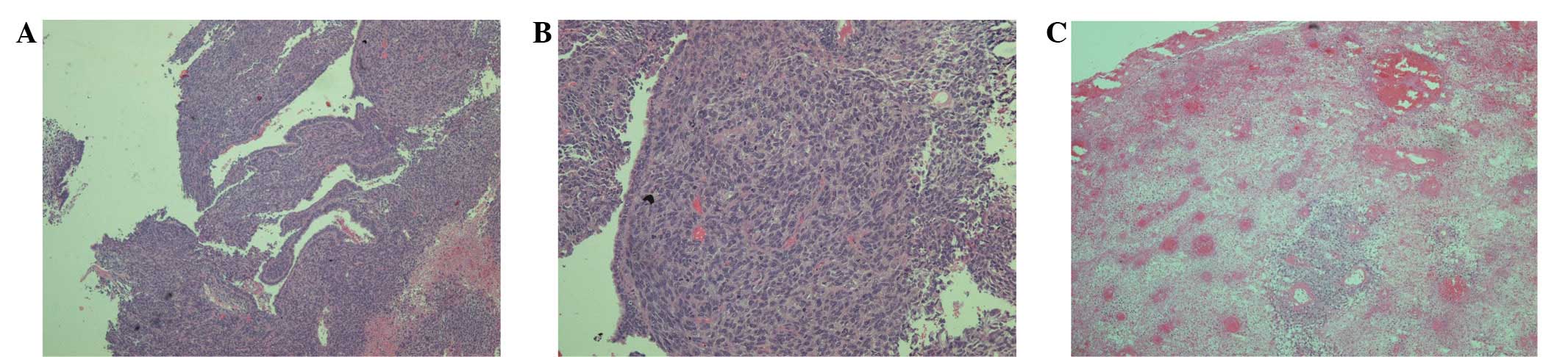
the gall-bladder. Histologically, the tumor was formed of two
distinct components, namely poorly-differentiated tubular
adenocarcinoma and sarcomatous tissue with rhabdomyosarcomatous
differentiation (Fig. 2A and B).
Following hematoxylin-eosin (HE) staining, the soft tissue mass
from the common bile duct was diagnosed as a tumor thrombus
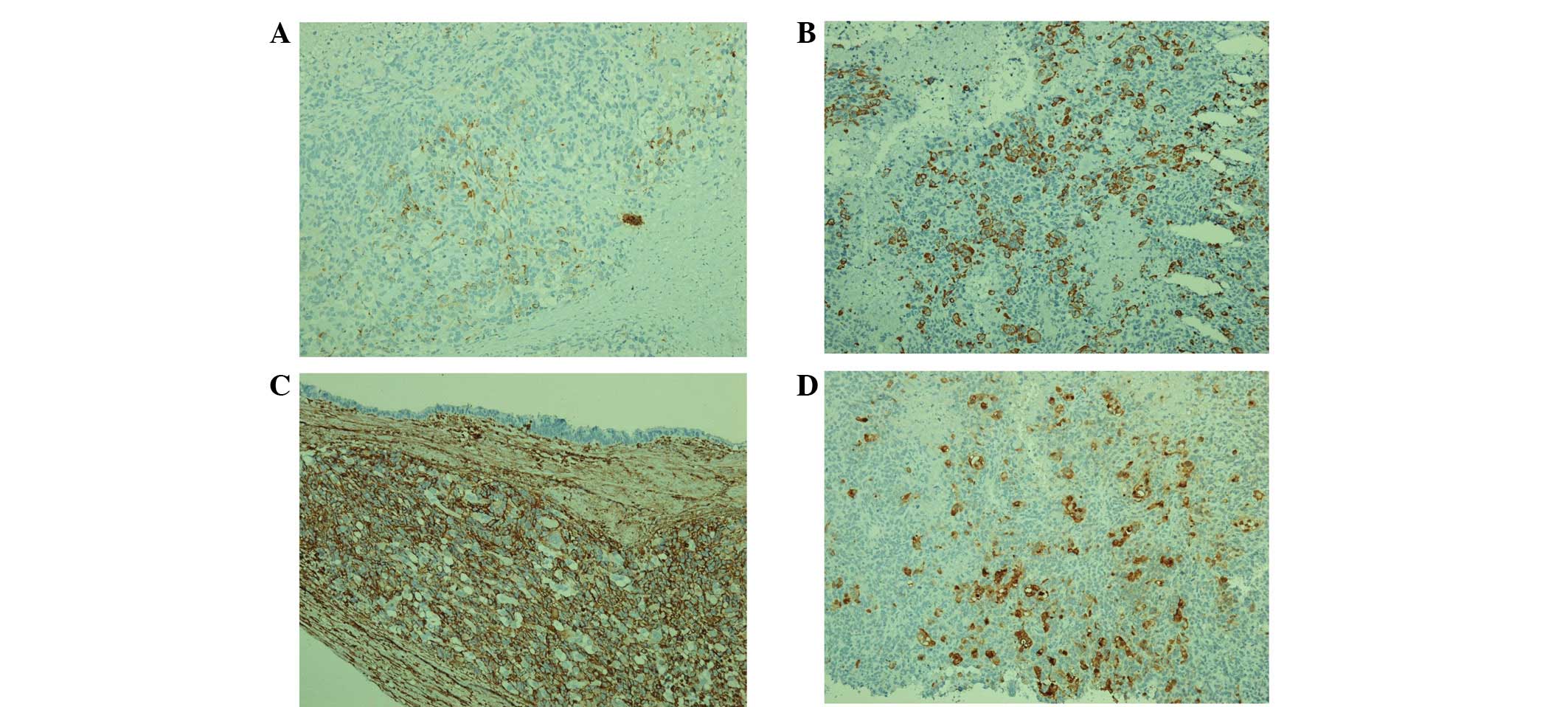
(Fig. 2C). Immunohistochemical
analysis revealed that the malignant epithelial component was
positive for cytokeratin (Fig. 3).
The spindle cells of the sarcomatous components, including the
rhabdomyosarcomatous differentiation, were stained with antibodies
against vimentin, desmin, myoglobin and cytokeratin (Fig. 3). The sample was negative for smooth
muscle actin, CD56 and S-100. In addition, the carcinomatous and
the sarcomatous areas were markedly positive for p53. The
proliferation index, as detected by the Ki-67 labeling index (LI),
was 70. The patient was discharged on post-operative day 11 and the
serum AFP levels had decreased to normal levels after 1.5
months.
Discussion
Carcinosarcomas, characterized by two intermingled
epithelial and mesenchymal components within the same tissue, are
an extremely atypical subset of gallbladder malignancies. The
epithelial component usually consists of adenocarcinoma and, in
rarer cases, elements of squamous cell, small cell and
undifferentiated carcinomas are also observed. Although the
sarcomatous component typically consists of undifferentiated
spindle cells and heterologous elements, including osteosarcoma,
chondrosarcoma, rhabdomyosarcoma and leiomyosarcoma, it may
occasionally comprise part of the mesenchymal component (2–4). In
the present case study, the carcinosarcoma of the gallbladder was
composed of carcinomatous and sarcomatous portions and the
sarcomatous differentiation revealed apparent rhabdomyosarcomatous
differentiation.
The exact histogenesis of carcinosarcoma of the
gall-bladder has not been clearly elucidated. At present, two
opposing theories have been hypothesized to explain the origin of
these morphologically diverse tumors. The multiclonal theory
(convergence hypothesis) regards a carcinosarcoma as a collision
tumor composed of the derivatives of two or more stem cells of
separate epithelial and mesenchymal origin. The monoclonal theory
(divergent hypothesis) proposes that carcinomatous and sarcomatous
elements are derived from a single pluripotential stem cell that
subsequently develops divergent differentiation along separate
epithelial and mesenchymal pathways (5). Through the detection of associated
gene fragments using molecular biology methods, specific studies
have demonstrated that carcinosarcomas originating from the uterus,
breast, lung and gastrointestinal tract are all monoclonal
(6). Dacic et al(7) performed an extensive comparative
genotypic analysis using microdissection to secure representative
mesenchymal and epithelial components. The study found identical
allelic losses shared by each tumor component, without discordant
losses. This was consistent with the hypothesis that the
carcinomatous and sarcomatous components of this neoplasm were
derived from a single pluripotent stem cell and that the tumor was
monoclonal. However, a larger series of cases and
microdissection-based genotypic analyses of selected chromosomal
loci must be performed to elucidate the precise mechanism of
evolution of carcinosarcomas.
In the present case, the patient presented with
acute biliary inflammation and obstructive jaundice as the initial
complaint, as a result of an obstruction of the superior segment of
the common bile duct caused by tumor thrombi. This presentation has
rarely been reported in previous comparable studies (8). In the majority of these cases, the
clinical symptoms included right upper abdominal pain and a mass,
fever, jaundice, poor appetite, weight loss, general fatigue,
nausea and vomiting. In addition, 75% of the cases presented with
simultaneous cholecystolithiasis. The mechanism of tumor thrombi
formation remains unclear and its clinical and pathological
characteristics are undefined. We hypothesized that in the present
study, a fragment of a necrotic tumor migrated to the common bile
duct and caused an obstruction, or that a hemorrhage from the tumor
may have partially or completely filled the biliary tract with
tumor-containing blood clots. The only recognized treatment for
gallbladder carcinosarcoma is surgery and there have been no
reports of effective chemotherapy or radiotherapy for this tumor
type. In the present study, the biliary tumor thrombi were
successfully removed via choledochotomy. Following this, an
extrahepatic bile duct resection and a reconstruction using a
Roux-en-Y jejunal limb were performed.
AFP is a clinically useful and reliable marker for
the diagnosis of primary hepatocellular carcinoma, hepatoblastoma
and yolk-sac tumors (9). However,
AFP-producing tumors arising from the gallbladder are extremely
rare. In the present case study there was no evidence of liver
metastasis and the serum AFP levels were elevated to 312.7
μg/l; this decreased to within normal levels
post-operatively. Hayashi et al hypothesized that
AFP-producing carcinomas of the gallbladder more frequently
metastasize to the liver, indicating a poorer prognosis than that
of carcinomas that do not produce AFP (10). In addition, Ki-67, an indicator of
proliferative activity, was previously reported to have a
prognostic value. Kubota et al performed
immunohistochemistry to investigate Ki-67 LI in 1 case of
carcinosarcoma of the gallbladder and 11 cases of ordinary
gallbladder adenocarcinoma classified as stage IV, to clarify the
higher malignant proliferative potential of the former. The results
revealed that the Ki-67 LI of the carcinosarcoma was 68, which was
higher than the average level of ∼47 in the ordinary gallbladder
adenocarcinomas (11).
In the current patient, the Ki-67 LI was 70, which
was indicative of a higher proliferative and malignant potential
and a subsequent poorer prognosis. However, the patient follow-up
was uneventful and the individual remains healthy. A further
detailed follow-up of this patient is vital in view of the
aggressive biological behavior of this tumor.
Acknowledgements
The present study was supported by the
Shanghai Young Doctor Training Plan.
References
|
1
|
Shimada K, Iwase K, Aono T, et al:
Carcinosarcoma of the gallbladder producing alpha-fetoprotein and
manifesting as leukocytosis with elevated serum granulocyte
colony-stimulating factor: report of a case. Surg Today.
39:241–246. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kim MJ, Yu E and Ro JY: Sarcomatoid
carcinoma of the gall bladder with a rhabdoid tumor component. Arch
Pathol Lab Med. 127:e406–e408. 2003.PubMed/NCBI
|
|
3
|
Takahashi Y, Fukushima J, Fukusato T and
Shiga J: Sarcomatoid carcinoma with components of small cell
carcinoma and undifferentiated carcinoma of the gallbladder. Pathol
Int. 54:866–871. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ajiki T, Nakamura T, Fujino Y, et al:
Carcinosarcoma of the gallbladder with chondroid differentiation. J
Gastroenterol. 37:966–971. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Uzun MA, Koksal N, Gunerhan Y, et al:
Carcinosarcoma of the gallbladder: report of a case. Surg Today.
39:168–171. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sung MT, Wang M, MacLennan GT, et al:
Histogenesis of sarcomatoid urothelial carcinoma of the urinarv
bladder: evidence for a common clonal origin with divergent
differentiation. J Pathol. 211:420–430. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dacic S, Finkelstein SD, Sasatomi E, et
al: Molecular pathogenesis of pulmonary carcinosarcoma as
determined by microdissection-based allelotyping. Am J Surg Pathol.
26:510–516. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Born MW, Ramey WG, Ryan SF and Gordon PE:
Carcinosarcoma and carcinoma of the gallbladder. Cancer.
53:2171–2177. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu JT: Serum alpha-fetoprotein and its
lectin reactivity in liver diseases: a review. Ann Clin Lab Sci.
20:98–105. 1990.PubMed/NCBI
|
|
10
|
Hayashi K, Hiraki M, Yamashita Y, et al: A
case of cancer of the gallbladder with a high level of
alphafetoprotein. Nippon Rinsyo Geka Gakkai Zasshi (J Jpn Soc Clin
Surg). 55:3161–3165. 1994.(In Japanese).
|
|
11
|
Kubota K, Kakuta Y, Kawamura S, et al:
Undifferentiated spindle-cell carcinoma of the gallbladder: an
immunohistochemical study. J Hepatobiliary Pancreat Surg.
13:468–471. 2006. View Article : Google Scholar : PubMed/NCBI
|