Introduction
Gastrointestinal stromal tumours (GISTs) are
uncommon mesenchymal neoplasias of the gastrointestinal tract that
may occur between the oesophagus and anus, and even in the omentum
and mesentery (1–7). GISTs are found infrequently in adults
prior to the age of 40, generally presenting with a peak incidence
during the fifth and sixth decades and without significant gender
differences (2,3,8). The
histogenesis of these tumours has been attributed to the
interstitial cells of Cajal, which are referred to as the pacemaker
cells of the gastrointestinal tract (3–6) and
which are immunohistochemically positive for CD117 (5–7,9).
The clinical presentation of a GIST is largely
dependent on the site of occurrence, as well as the size of the
tumours, although the clinical signs and symptoms, including
nausea, abdominal pain, weight loss, anaemia or melena are
non-specific and therefore not useful for the diagnosis (3–7).
However, patients may also present with signs of obstruction,
perforation, palpable masses and peritoneal seeding (2,6,7,10,11).
A large series of GIST cases revealed that these
tumours have a broad spectrum of clinical behavior at all sites of
occurrence. However, they are considered to be potentially
malignant (5,12–14)
and therefore require a multidisciplinary approach to optimise the
management of patients. An accurate and early diagnosis of these
rare tumours affects the treatment, primarily allowing the chance
of an optimal surgical resection, which may reduce the number of
unresectable or metastatic GIST cases. However, imatinib mesylate
is now regarded as the revolutionary standard care in the
first-line treatment of advanced GISTs (5,15–17).
The present study reports two cases of gastric GISTs
that occurred as submucosal or intramural nodules. The diagnosis of
a GIST was achieved by endoscopic ultrasound-guided fine-needle
aspiration cytology (EUS-FNAC) and immunocytochemistry, which was
further confirmed by post-surgical examination. Written informed
consent was obtained from both patients; the original
corrresponding declarations were available at the Department of
Human Pathology, University of Messina, Italy.
Case reports
Case 1
An 88-year-old female presented with melena that had
lasted 3 days. A general examination revealed a moderate pallor
without weight loss or pain and no evidence of free fluid in the
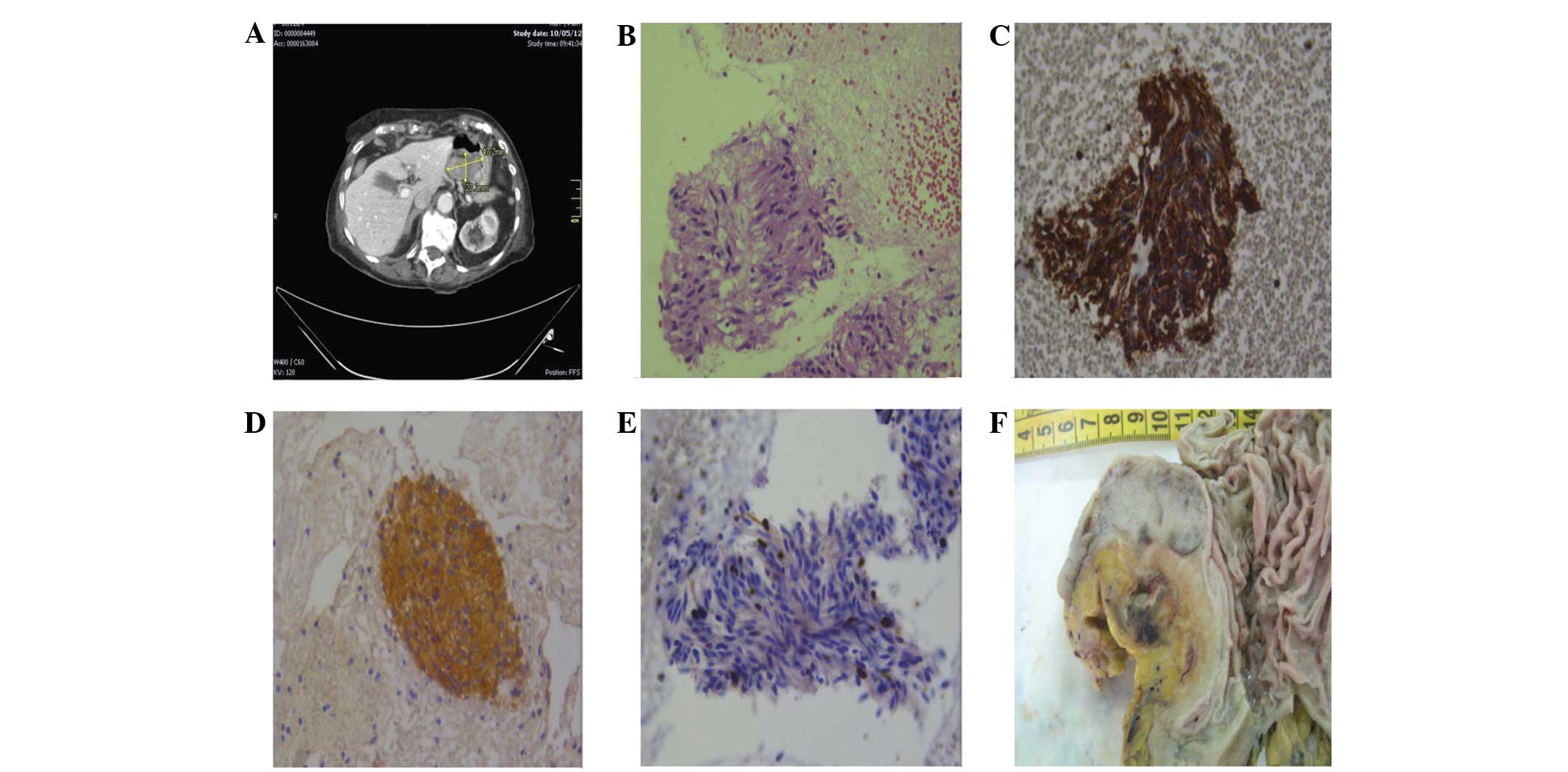
abdomen. Computed tomography (CT) revealed a 40-mm oval lesion with
defined margins measuring 56.4×33.5 mm. The lesion was localised in
the submucosal layer of the gastric wall between the corpus and the
antrum, along the small gastric curvature (Fig 1A). No lesions were evident in the
pancreas, biliary tree, duodenum and lymph nodes. EUS-FNAC was
performed using a convex array echoendoscope (EG 3870 UTK; Pentax,
Tokyo, Japan) and by making two passes with a 25 gauge needle. The
specimens were stained with haematoxylin and eosin, processed by an
in-room cytopathologist and then immediately examined for adequate
cellularity. A second slide was fixed in 95% ethanol and
Papanicolaou’s stain was applied. Any excessive material, including
the needle and syringe utilized in the procedure, was rinsed in 10
ml 50% ethanol in a specimen container. All content was centrifuged
in a 10 ml disposable centrifuge tube at 5,017 × g for 6 min to
create 1 or 2 pellets. The supernatant fluid was decanted and the
pelleted material was immediately fixed in a freshly prepared
solution of 4% neutral buffered formalin for 45 min. The cell
pellets were then placed in a cassette and stored in 80% ethanol
until they were ready for processing in an automatic tissue
processor (Leica TP1020; Leica Biosystems, Ltd., Mannheim,
Germany). The cell blocks that were obtained were embedded in
paraffin at 56°C and successive 3-μm thick sections were cut
and routinely stained by haematoxylin and eosin. Parallel serial
sections of the same thickness were mounted onto silane-coated
glasses and submitted for immunohistochemical procedures, as
previously described (18–20).
Case 2
A 76-year-old male presented to the Surgery
Department, University-Hospital Health Network ‘Polyclinic G.
Martino’, with gastric discomfort and pain in the mesogastric
region that had lasted three weeks. During a general examination,
the pain increased with palpation and a pale skin tone was noted.
Ultrasonography of the abdomen revealed a 22.4×17.4-mm hypoechoic
round lesion with a well-defined margin. The lesion was localized
in the superficial muscular layer of the gastric corpus, between
the posterior wall and the large gastric curvature (Fig. 2A). No lesions were evident elsewhere
in the abdominal organs. EUS-FNAC was performed with the same
procedures that had been utilized in case 1; adequate cellular
smears and one cell block were obtained.
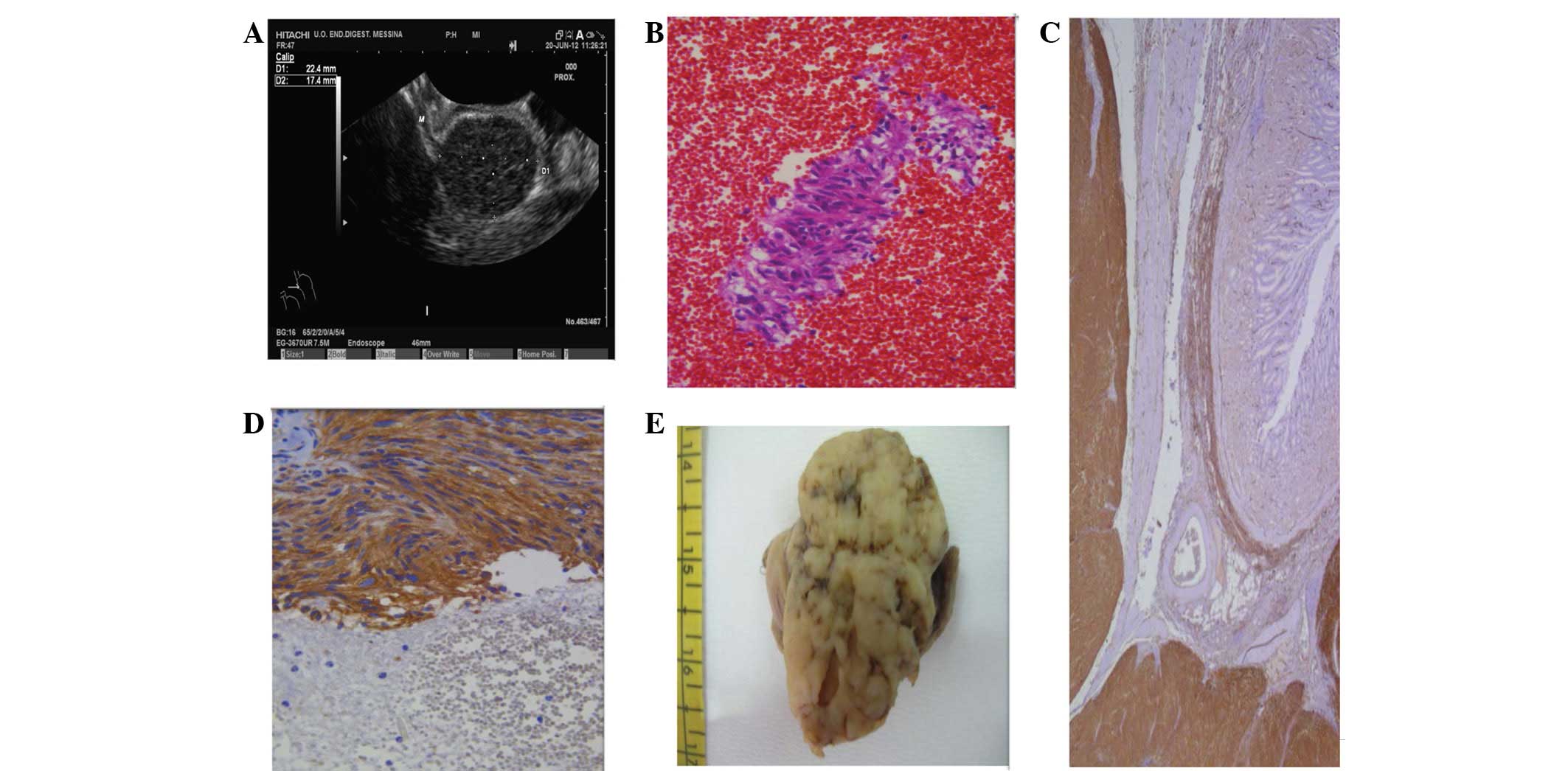 | Figure 2Case 2. (A) EUS scanning revealed a
22.4×17.4-mm, hypoechoic, well-delimited lesion, originating from
the muscle layer. (B) The cytology of the lesion was strongly
suggestive of a GIST, being formed of clusters of spindle cells
(immunoperoxidase staining; magnification, ×200). (C) Upon
histological examination, a diffuse cytoplasmic CD117
immunoreactivity was found in the proliferative spindle cell
elements of the gastric wall (immunoperoxidase staining;
magnification, ×120). (D) The clusters of spindle cells were
reactive for CD117, but also for CD34 (immunoperoxidase staining;
magnification, ×160). (E) The cut surface of the surgical specimen
showed a white-greyish nodular feature. EUS, endoscopic ultrasound;
GIST, gastrointestinal stromal tumour. |
Following the FNAC procedures, the two patients were
observed for a period of 48 h for any procedure-related
complications.
Cytological and immunocytochemical
findings
The smears from the two cases exhibited haemorrhagic
backgrounds with a well-represented cellularity. They were
organized in cohesive groups, arranged in three-dimensional
clusters or as single cells (Figs.
1B and 2B). The elements were
spindle-shaped with scant, lightly eosinophilic cytoplasm and
elongated/oval plump nuclei. The chromatin was clumped with
indistinct nucleoli and mild pleomorphisms (Figs. 1B and 2B). No mitoses were identified. In case 2,
the spindle cell elements occasionally exhibited paranuclear
vacuoles with an epithelioid feature. A presumptive diagnosis of
gastric GIST was made for the two cases.
The cell blocks documented an equivalent morphology
characterized by monotonous sheets and groups of spindle-shaped
cells with oval nuclei and well-defined cellular borders. Mitotic
activity was virtually absent. Immunohistochemical procedures were
carried out on the 3-μm serial sections, utilizing the
following commercially obtained antisera from DakoCytomation
(Copenhaghen, Denmark): CD117 [(working dilution) w.d., 1:150],
CD34 (w.d., 1:200), smooth muscle actin (SMA; w.d., 1:200),
vimentin (w.d., 1:250), S-100 (w.d., 1:400), desmin (w.d., 1:250),
glial fibrillary acidic protein (GFAP; w.d., 1:300) neurofilaments
(NF; w.d., 1:300) and Ki67 (MIB-1; w.d., 1:50). In cases 1 and 2, a
strong and diffuse cytoplasmic immunostaining was encountered for
vimentin (Fig. 1C), CD117 (Fig. 1D) and CD34 (Fig. 2C). The majority of the
spindle-shaped clusters also exhibited immunoexpression for SMA. No
immunostaining was recorded for desmin, S100, GFAP or NF. The
growth fraction, determined by Ki67 as the MIB-1 labeling-index,
was extremely low, showing <5% of positively-labelled nuclei
(Fig. 1E).
Gross and microscopic examination
The patients of cases 1 and 2 underwent surgical
laparotomy and were alive and well at 12 and 8 months post-surgery,
respectively. The resected tumours were sent for histological
analysis. In case 1, a gross examination revealed a white-greyish
nodular growth measuring 40×21 mm, situated below the mucosal
surface of the stomach (Fig. 1F),
while case 2 showed an intraparietal whitish nodular mass with a
maximum diameter of 23 mm (Fig.
2D). Upon microscopic examination, the two lesions were
observed to be formed from uniform sheets and interlacing fascicles
of spindle-shaped cells, exhibiting elongated or oval nuclei,
without atypia and with occasional mitoses. The immunohistochemical
analysis documented an intense cytoplasmic positivity for CD117
(Fig. 2E), CD34, SMA and vimentin,
while desmin, S100, GFAP and NF were largely unreactive.
Immunoreactive nuclei for Ki67 were encountered in <5% of the
proliferating spindle-shaped elements.
Discussion
EUS-FNAC and endoscopic ultrasound-guided tru-cut
biopsy (EUS-TCB) have been proven to be of significant value in the
diagnostic evaluation of benign and malignant diseases, as well as
for the staging of malignant tumours of the gastrointestinal tract
and adjacent organs (21–23). The diagnostic yield of EUS-FNAC
partially depends on the site, size and characteristics of the
target tissues as well as certain technical/procedural factors.
However, it is mainly dependent on the expertise, training and
interaction between the endosonographer and cytopathologist.
EUS-TCB utilizes a stiffer device that appears to be marginally
more difficult to use than the standard FNAC. Currently, there are
no accepted standards for when EUS-TCB should be used to improve
diagnostic accuracy (24). In the
present study, adequate cellular smears and corresponding cell
blocks were obtained using the EUS-FNAC approach to gastric GISTs.
Subsequently, spindle shaped cells with scant cytoplasm and
elongated/oval nuclei were identified, which were strongly
suggestive for a cytological diagnosis of a GIST. Moreover, a
confirmatory immunocytochemical investigation was performed on the
available material, with evidence of CD117, CD34, vimentin and SMA
immunostaining in the considered cellular proliferations. These
morphological data have been verified by histology and
immunohistochemistry following a post-surgical examination of the
resected tumours. Thus, an early, accurate diagnosis ensured the
use of an appropriate therapy for the patients, and the two cases
should be included in the suggested algorithm (CD117, CD34,
vimentin and SMA) for GISTs, as has previously been described
(5,14).
Another notable point from the present study is the
pre-surgical opportunity to perform a correct differential
diagnosis of gastric GISTs from other mesenchymal neoplasias,
including leiomyoma, schwannoma and solitary fibrous tumours, or
alternatively, metastatic diseases, such as spindle cell amelanotic
melanoma or carcinoma. The additional value that
immunohistochemistry may provide as a diagnostic confirmatory
procedure, together with the specific cytological findings, should
be considered either in smears or in cell blocks. Leiomyomas are
strongly positive for desmin and SMA, but negative for CD117 and
CD34, while schwannomas show positivity for S100 protein, with a
lack of CD117 and CD34 expression (2,3,6,7).
Although a solitary fibrous tumour is typically CD34
immunoreactive, CD117 and SMA are generally absent or marginally
and focally represented (2,3,6,7).
Finally, the differential diagnosis with spindle cell amelanotic
melanoma or carcinoma should be performed on the basis of the
absence of immunoreactivity for CD117 and CD34 and the appearance
of intense staining for melanoma-associated antigens, such as
HMB-45, melan-A or cytokeratins.
Predicting the clinical behavior of GISTs remains a
complex and noteworthy task, as numerous indicators have been
proposed and extensively evaluated without a widespread consensus
being achieved (1,3,4,7,12,13,25–29).
The most relevant and largely applied morphological parameters have
been considered to be tumour size (<5 or >5 cm) and mitotic
count (number of mitoses per 50 HPFs) (1,3,4,12,26).
Moreover, the site of the GIST has been regarded as a significant
predictive aspect. GISTs generally confer a better survival outcome
for the patient than tumours of a similar size and mitotic activity
occurring in the small intestine, colon and ano-rectum (1,3,4,30).
However, the crucial purpose of GIST management is to assess the
correct diagnosis in an early phase of the disease in order to
realize an adequate curative surgical resection. This is as at a
later stage, GISTs may become unresectable or metastatic (5,12,31).
In the present study, taking into consideration the aforementioned
parameters as guides for evaluating GIST malignancy, it may be
concluded that the tumours of the two cases are most likely to be
benign, particularly since the maximum diameter of the tumours was
<5 cm and ≤3 mitoses were encountered per 50 HPFs. Moreover, the
growth fraction of the tumours, as determined by the Ki67
labeling-index, was extremely low, showing <5% of
positively-labelled nuclei. However, it has been observed that a
certain number of these small and mitotically inactive tumours are
later characterized by local recurrence and metastatic disease
(1,4,12).
Finally, it may be argued that further molecular characterization,
for example, the identification of specific KIT mutations that
affect various gene domains, may be significant in the selection of
tumour subgroups and the prediction of their clinical outcome and
response to selective therapy.
References
|
1
|
Emory TS, Sobin LH, Lukes L, Lee DH and
O’Leary TJ: Prognosis of gastrointestinal smooth-muscle (stromal)
tumours: dependence on anatomic site. Am J Surg Pathol. 23:82–87.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumours - definition, clinical, histological,
immunohistochemical, and molecular genetic features and
differential diagnosis. Virchows Arch. 438:1–12. 2001. View Article : Google Scholar
|
|
3
|
Graadt van Roggen JF, van Velthuysen ML
and Hogendoorn PC: The histopathological differential diagnosis of
gastrointestinal stromal tumours. J Clin Pathol. 54:96–102.
2001.PubMed/NCBI
|
|
4
|
Miettinen M, El-Rifai W, Sobin L and
Lasota J: Evaluation of malignancy and prognosis of
gastrointestinal stromal tumours: a review. Hum Pathol. 33:478–483.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wong DW, Lupton SC, Bhatt L, Gross L,
Tanière P, Peake DR, Spooner D and Geh JI: Use of imatinib mesylate
in gastrointestinal stromal tumours: Pan-Birmingham Cancer Network
experience. Clin Oncol (R Coll Radiol). 20:517–522. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Versaci A, Macrì A, Ieni A, Terranova M,
Leonello G, Saladino E, Speciale G and Famulari C: Gastrointestinal
stromal tumour: our experience. Chir Ital. 61:161–169. 2009.(In
Italian).
|
|
7
|
Maheshwari V, Alam K, Varshney M, Jain A,
Asif Siddiqui F and Bhargava S: Fine-needle aspiration diagnosis of
GIST: a diagnostic dilemma. Diagn Cytopathol. 40:834–838. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chan JK: Mesenchymal tumours of the
gastrointestinal tract: a paradise for acronyms (STUMP, GIST, GANT,
and now GIPACT), implication of c-kit in genesis, and yet another
of the many emerging roles of the interstitial cell of Cajal in the
pathogenesis of gastrointestinal diseases? Adv Anat Pathol.
6:19–40. 1999.
|
|
9
|
Sircar K, Hewlett BR, Huizinga JD,
Chorneyko K, Berezin I and Riddel RH: Interstitial cells of Cajal
as precursors of gastrointestinal stromal tumours. Am J Surg
Pathol. 23:377–389. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lerma E, Oliva E, Tugués D and Prat J:
Stromal tumours of the gastrointestinal tract: a
clinicopathological and ploidy analysis of 33 cases. Virchows Arch.
424:19–24. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mehta RM, Sudheer VO, John AK, Nandakumar
RR, Dhar PS, Sudhindran S and Balakrishnan V: Spontaneous rupture
of giant gastric stromal tumor into gastric lumen. World J Surg
Oncol. 3:112005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dematteo RP, Heinrich MC, El-Rifai WM and
Demetri G: Clinical management of gastrointestinal stromal tumours:
before and after STI-571. Hum Pathol. 33:466–477. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nilsson B, Bümming P, Meis-Kindblom JM, et
al: Gastrointestinal stromal tumours: the incidence, prevalence,
clinical course, and prognostication in the preimatinib mesylate
era - a population-based study in western Sweden. Cancer.
103:821–829. 2005. View Article : Google Scholar
|
|
14
|
Reid R, O’Dywer P, MacDuff E, et al:
Guidelines for the management of gastrointestinal stromal tumours
(GIST) in Scotland. pp. 53–55. 2009, http://www.pathologyscotland.org/download/sgpg/guidelines/gist.pdf.
Accessed November 13, 2012.
|
|
15
|
Demetri GD, von Mehren M, Blanke CD, et
al: Efficacy and safety of imatinib mesylate in advanced
gastrointestinal stromal tumours. N Engl J Med. 347:472–480. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Blay JY, Bonvalot S, Casali P, et al: GIST
consensus meeting panelists: Consensus meeting for the management
of gastrointestinal stromal tumours. Report of the GIST Consensus
Conference of 20–21 March 2004, under the auspices of ESMO. Ann
Oncol. 16:566–578. 2005.PubMed/NCBI
|
|
17
|
Blanke CD, Demetri GD, von Mehren M, et
al: Long-term results from a randomized phase II trial of standard-
versus higher-dose imatinib mesylate for patients with unresectable
or metastatic gastrointestinal stromal tumours expressing KIT. J
Clin Oncol. 26:620–625. 2008. View Article : Google Scholar
|
|
18
|
Nathan NA, Narayan E, Smith MM and Horn
MJ: Cell block cytology. Improved preparation and its efficacy in
diagnostic cytology. Am J Clin Pathol. 114:599–606. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tuccari G, Giuffrè G, Scarfi R, Simone A,
Todaro P and Barresi G: Immunolocalization of lactoferrin in
surgically resected pigmented skin lesions. Eur J Histochem.
49:33–38. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Barresi V, Cerasoli S, Paioli G, Vitarelli
E, Giuffrè G, Guiducci G, Tuccari G and Barresi G: Caveolin-1 in
meningiomas: expression and clinico-pathological correlations. Acta
Neuropathol. 112:617–626. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jenssen C and Dietrich CF: Endoscopic
ultrasound guided fine-needle aspiration biopsy and trucut biopsy
in gastroenterology - An overview. Best Pract Res Clin
Gastroenterol. 23:743–759. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Itoi T, Tsuchiya T, Itokawa F, Sofuni A,
Kurihara T, Tsuji S and Ikeuchi N: Histological diagnosis by
Eus-guided fine-needle aspiration biopsy in pancreatic solid masses
without on-site cytopathologist: a single-center experience. Dig
Endosc. 23(Suppl 1): 34–38. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yoshinaga S, Suzuki H, Oda I and Saito Y:
Role of endoscopic ultrasound-guided fine needle aspiration
(EUS-FNA) for diagnosis of solid pancreatic masses. Dig Endosc.
23(Suppl 1): 29–33. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hoda KM, Rodriguez SA and Faigel DO:
EUS-guided sampling of suspected GI stromal tumours. Gastrointest
Endosc. 69:1218–1223. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Panizo-Santes A, Sola I, Vega F, de Alava
E, Lozano MD, Idoate MA and Pardon-Mindán J: Predicting metastatic
risk of gastrointestinal stromal tumours: role of cell
proliferation and cell cycle regulatory proteins. Int J Surg
Pathol. 8:133–144. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fletcher CD, Berman JJ, Corless C, et al:
Diagnosis of gastrointestinal stromal tumours: A consensus
approach. Hum Pathol. 33:459–465. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Koon N, Schneider-Stock R, Sarlomo-Rikala
M, Lasota J, Smolkin M, Petroni G, Zaika A, Boltze C, Meyer F,
Andersson L, Knuutila S, Miettinen M and El-Rifai W: Molecular
targets for tumour progression in gastrointestinal stromal tumours.
Gut. 53:235–240. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kim KM, Kang DW, Moon WS, et al
Gastrointestinal stromal tumor committee; The Korean
Gastrointestinal Pathology Study Group: Gastrointestinal stromal
tumours in Koreans: it’s incidence and the clinical, pathologic and
immunohistochemical findings. J Korean Med Sci. 20:977–984.
2005.
|
|
29
|
O’Sullivan B, Deshmukh N, Reynolds G, et
al: Retrospective analysis of GIST in one regional UK reference
centre. Gut. 56(S1): A72007.
|
|
30
|
Ueyama T, Guo KJ, Hashimoto H, Daimaru Y
and Enjoji M: A clinicopathologic and immunohistochemical study of
gastrointestinal stromal tumours. Cancer. 69:947–955. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumours: review on morphology, molecular pathology,
prognosis, and differential diagnosis. Arch Pathol Lab Med.
130:1466–1478. 2006.PubMed/NCBI
|