Introduction
Male breast cancer is of rare occurrence compared to
female equivalent. The peak age of incidence for males is 71 years,
while for females it is 52 years (1). Although rare, male breast cancer
usually has the same common presentation as female breast cancer.
However, male breast cancer arising in ectopic axillary breast
tissue is an extremely rare malignant neoplasm that has a high
incidence of misdiagnosis. Due to the atypical location, a correct
diagnosis is often reached during the later stages of cancer. The
number of previous studies on male axillary ectopic breast cancer
is extremely low and we have found only one relevant case report
(2). In the current study, a rare
case of male breast cancer arising in ectopic axillary breast
tissue is presented, highlighting specific issues with the
diagnosis and treatment of this pathology. Written informed consent
was obtained from the patient.
Case report
Clinical presentation and diagnosis
A 51-year-old Chinese male presented with a right
axillary superficial mass that had been present for 6 months. The
lesion was slow growing and asymptomatic. A physical examination
revealed a seemingly healthy male with multiple areas of erythema
and several swollen lymph nodes in the right axilla. No mass was
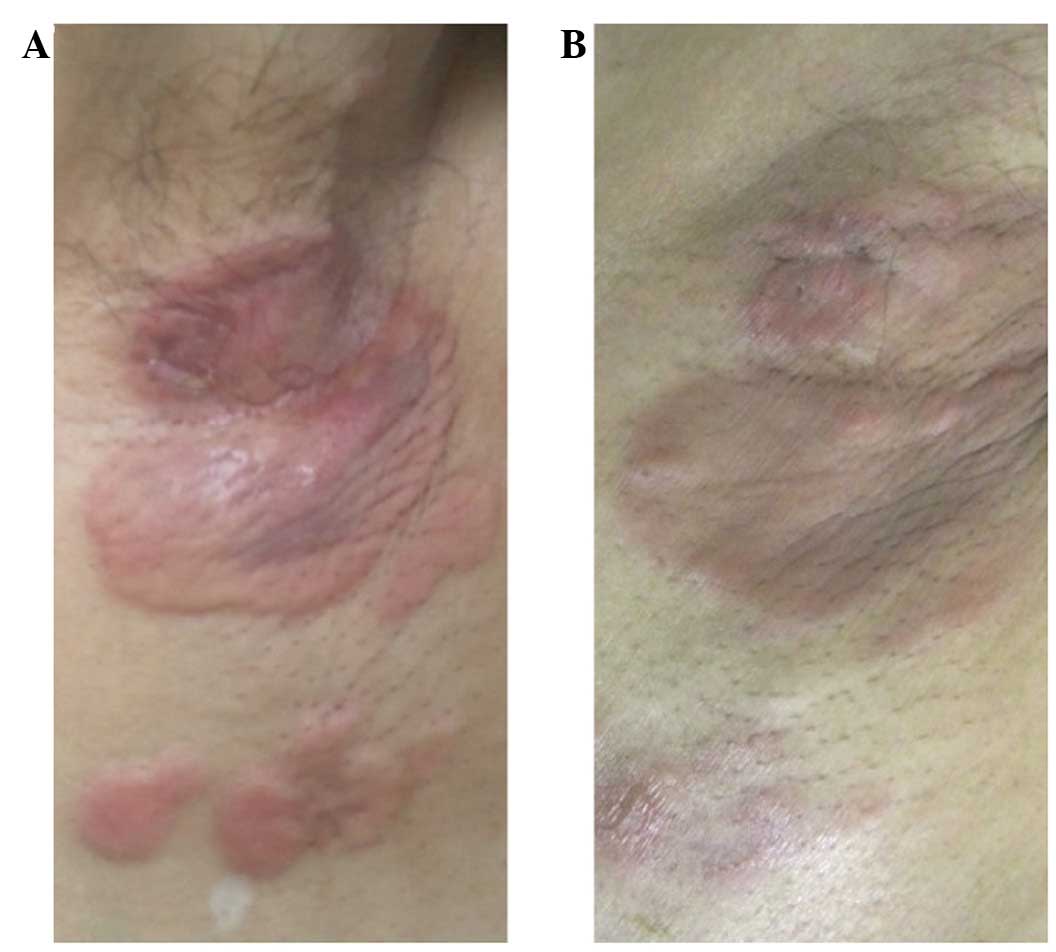
palpable inside either breast. The skin lesion was of an irregular
shape and size, with maximum dimensions of ∼6×4 cm. With the
exception of a reddish appearance, there was no ulceration,
swelling, pain or fever of the skin (Fig. 1A). The physical examination also
revealed firm, non-tender, enlarged lymph nodes in the right
axilla. No cervical, supraclavicular or contralateral axillary
swollen lymph nodes were observed. Notably, the patient underwent a
right axillary lesion biopsy prior to admission and the pathology
report revealed a poorly-differentiated adenocarcinoma. The
immunohistochemistry analysis found that the tissue sample was
positive for CK-7 and CK-Pan and negative for gross cystic disease
fluid protein 15 (GCDFP-15), mammaglobin, the estrogen and
progesterone receptors and S-100 protein, indicating that the
deformed cells were of epithelial origin. To exclude a metastatic
adenocarcinoma, a series of analyses were performed. A C-12
laboratory study demonstrated that the carcinoembryonic antigen
(CEA) levels were high at 73.47 ng/ml (normal level, <5 ng/ml).
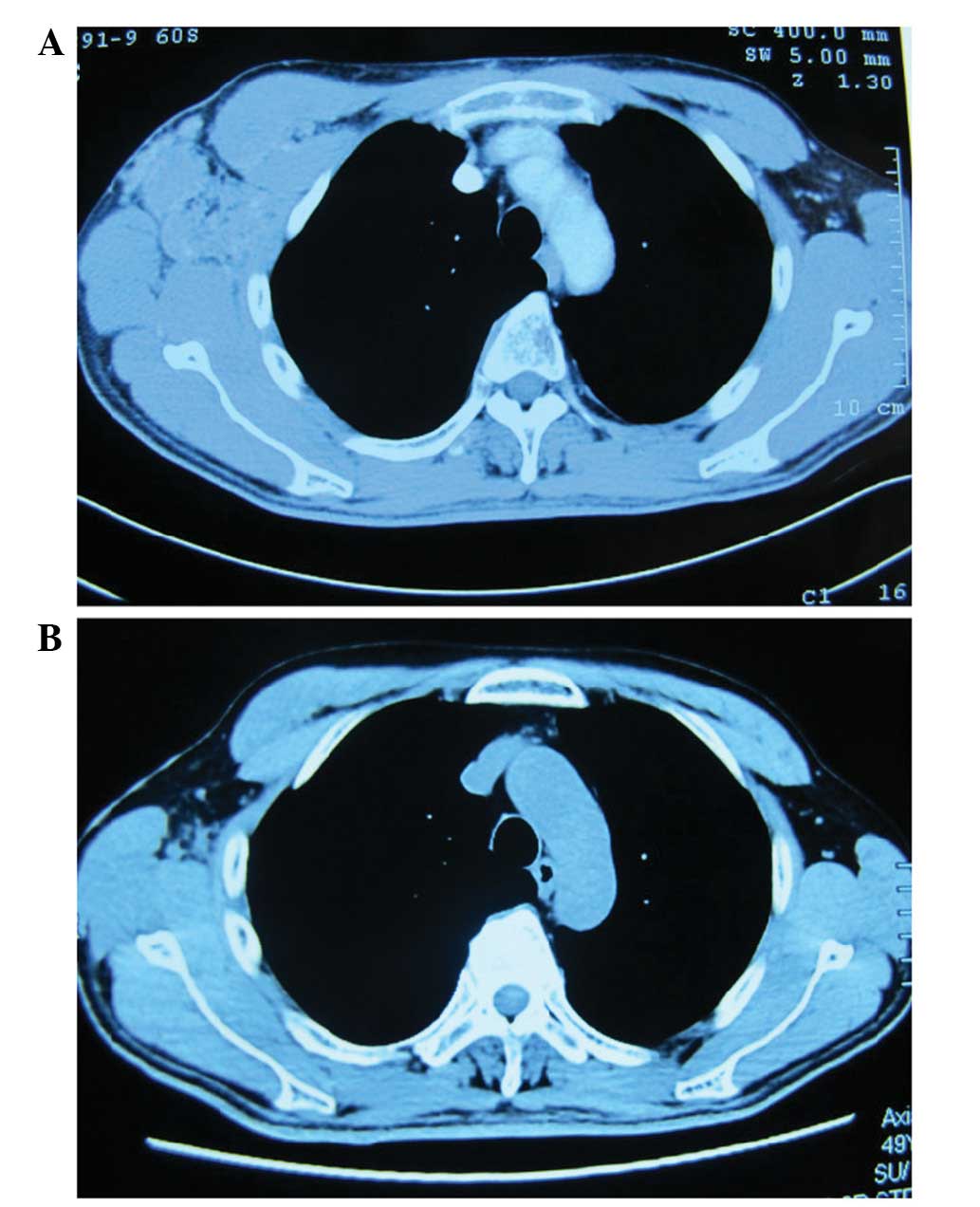
A computed tomography scan of the thorax (Fig. 2) revealed a 5.6×4.1-cm mass in the
right axilla, with enlarged adjacent lymph nodes, while the
contralateral axilla was normal. The results of a gastrointestinal
endoscopy were normal. In addition, the patient underwent positron
emission tomography-computed tomography in which the right axilla
was observed to exhibit an increase in
18F-fludeoxyglucose (18F-FDG) uptake. Based
on the clinicopathological and ancillary test results, the patient
was diagnosed with a metastatic adenocarcinoma of unknown primary
origin.
Treatment and clinical course
The patient received chemotherapy cycles of
paclitaxel (175 mg/m2) and cisplatin (75
mg/m2) every 21 days. After four cycles, the patient was
referred to the Central South University Xiangya Hospital
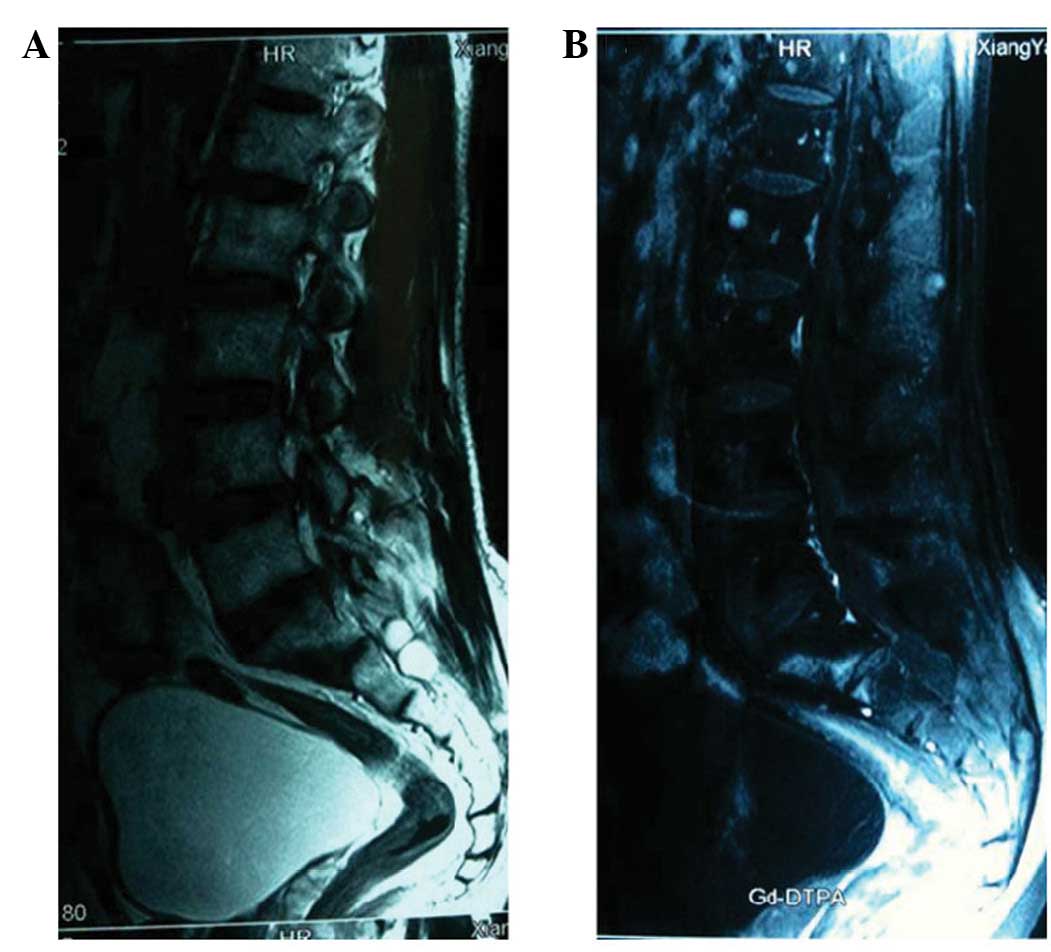
(Changsha, Hunan, China) with new lesions (Fig. 1B) and distant metastasis, as shown
by MRI (Fig. 3). Progression within
a short time may have been indicative of an initial misdiagnosis or
tumor resistance to the therapy. As a consequence, an additional
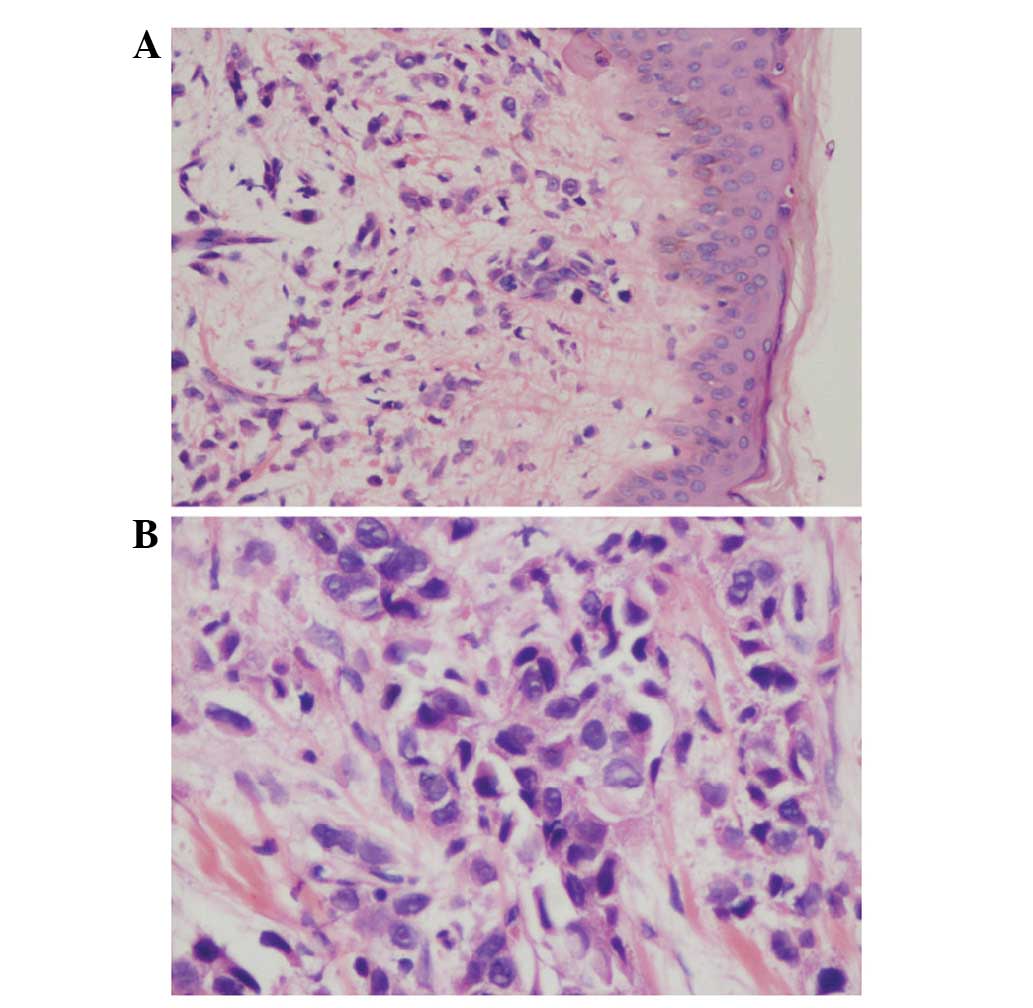
biopsy was performed. The pathological report once again diagnosed
a poorly-differentiated adenocarcinoma involving subcutaneous
tissue (Fig. 4). Macroscopically,
no tumor nests were found and no crypt-like structures were
identified in the background. The specimen consisted of skin and
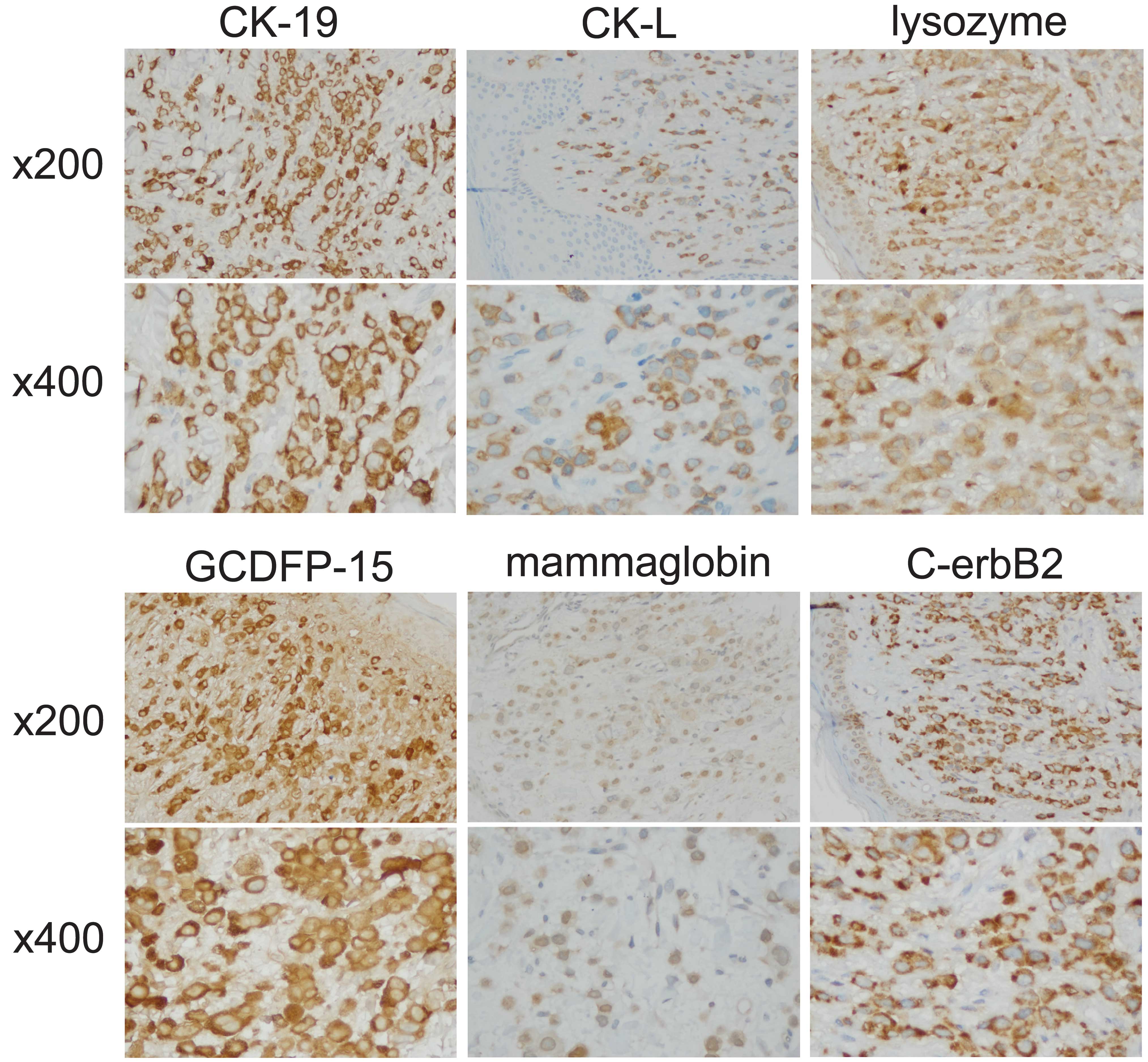
subcutaneous tissue. An immunohistochemistry analysis revealed that
the dissected tissue was positive for CK-19, CK-L, lysozyme,
GCDFP-15, mammaglobin and C-erbB2 (Fig.
5). The overexpression of C-erbB2 markedly indicated that a
breast adenocarcinoma could not yet be ruled out. The
immunohistochemical analysis of melan-A, HMB45, TG, CT, PSA, PSAP,
P504S, TTF-1, napsin, myogenin, actin, HHF35, CDX-2, P63 and
vimentin was also performed (results not shown) and the specimen
was observed to be negative for these markers. This eliminated
melanoma, thyroid gland, prostate, lung, muscle, intestine and
squamous epithelium origins, respectively. A diagnosis of carcinoma
arising in the ectopic breast tissue of the axilla was then made. A
follow-up of this case was not performed due to personal reasons
given by the patient, however, the case has been discussed here as
it is important for aiding in the improvement of clinical
performance, including forming a diagnosis and the pathological
analysis.
Discussion
Male breast cancer is extremely rare compared with
female breast cancer. Ectopic breast tissue has been identified in
a number of regions, including in the vulva (3), anal polyps (4), axilla (5,6) and
axillary lymph nodes (7), affecting
up to 6% of the general population and occurring more frequently in
females and the axillary region (8). Thus, the occurrence of male axillary
breast cancer is extremely uncommon and to the best of our
knowledge, only one case of male axillary breast cancer has been
reported (2). The presentation of
male axillary breast cancer may have a wide differential diagnosis
and, in particular, metastatic carcinoma from the breast or other
origins must be considered, as well as the diagnosis of a primary
origin (9). For the current patient
presenting with adenocarcinoma arising from axilla, the first step
of the differential diagnosis was to determine whether the mass was
a primary lesion of a metastatic epithelial neoplasm from the
breast, the gastrointestinal tract, the lung or the prostate.
Primary carcinoma arising in the axilla may be difficult to
differentiate from metastatic carcinoma of any type of origin and
from carcinoma arising in heterotopic axillary breast tissue, as
ectopic breast tissue is located in the subcutaneous tissue and
deep dermis of the skin, where it often integrates with normal skin
appendages (10). Since the
axillary region has abundant sweat and sebaceous glands, diagnoses
of cutaneous adnexal malignancies must be differentiated between.
In this instance, a differential diagnosis is difficult as these
two entities are often morphologically indistinguishable. In the
present case this was particularly apparent as the adenocarcinoma
was poorly-differentiated, making morphological distinction
extremely difficult. Therefore, in the present case,
immunohistochemical analysis was performed to generate a reliable
diagnosis. A previous study reported that accessory breast
carcinoma is diagnosed in the same manner as anatomical breast
carcinoma using a physical examination and ancillary tests,
followed by a pathological diagnosis via fine needle aspiration
cytology, gross excision or any other type of biopsy (11). To the best of our knowledge, a panel
of immunohistochemical markers, including the estrogen and
progesterone receptors and C-erbB2, are more useful in the
pathological diagnosis of mammary carcinoma. In addition, GCDPF-15
and mammaglobin represent significant immunomarkers of breast
cancer. Lewis et al(12)
found that mammaglobin is a more sensitive, but less specific,
marker of breast cancer compared with GCDPF-15, as mammaglobin is
not only expressed in breast carcinoma tissue but also in benign
breast epithelium, while normal breast tissue does not express
GCDPF-15. In addition, mammaglobin-A has previously been used for
the non-invasive, in vivo detection of cancerous cells in
mouse breast cancer with metastatic axillary lymph nodes and has
shown a high resolution and specificity, indicating a potential for
future translation into the provision of clinical guidance
(13). Serra et al(14) reported that lysozyme-positive male
breast cancer has an unfavorable outcome.
In the present case report, immunohistochemistry was
used to generate a diagnosis of male breast cancer arising in the
ectopic axillary breast tissues and to fully exclude other types of
origin and common presentations of breast cancer metastasis to the
axilla.
References
|
1
|
Zygogianni AG, Kyrgias G, Gennatas C, et
al: Male breast carcinoma: epidemiology, risk factors and current
therapeutic approaches. Asian Pac J Cancer Prev. 13:15–19. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schneider S and Sariego J: Male breast
cancer presenting as an axillary mass: a case report and literature
review. South Med J. 102:736–737. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dordević M, Jovanović B, Mitrović S and
Dordević G: Ectopic mammary tissue in vulva. Vojnosanit Pregl.
65:407–409. 2008.PubMed/NCBI
|
|
4
|
Chan NG, Penswick JL, Labelle E and Driman
D: Ectopic breast tissue presenting as an anal polyp. Can J Surg.
50:E23–E24. 2007.PubMed/NCBI
|
|
5
|
Evans DM and Guyton DP: Carcinoma of the
axillary breast. J Surg Oncol. 59:190–195. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ahmed M, Aurangzeb, Pervez A, et al:
Primary carcinoma of ectopic breast tissue in axilla. J Coll
Physicians Surg Pak. 22:726–727. 2012.PubMed/NCBI
|
|
7
|
Kadowaki M, Nagashima T, Sakata H, et al:
Ectopic breast tissue in axillary lymph node. Breast Cancer.
14:425–428. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Loukas M, Clarke P and Tubbs RS: Accessory
breasts: a historical and current perspective. Am Surg. 73:525–528.
2007.PubMed/NCBI
|
|
9
|
Nihon-Yanagi Y, Ueda T, Kameda N and
Okazumi S: A case of ectopic breast cancer with a literature
review. Surg Oncol. 20:35–42. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sanguinetti A, Ragusa M, Calzolari F, et
al: Invasive ductal carcinoma arising in ectopic breast tissue of
the axilla. Case report and review of the literature. G Chir.
31:383–386. 2010.PubMed/NCBI
|
|
11
|
Roorda AK, Hansen JP, Rider JA, et al:
Ectopic breast cancer: special treatment considerations in the
postmenopausal patient. Breast J. 8:286–289. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lewis GH, Subhawong AP, Nassar H, et al:
Relationship between molecular subtype of invasive breast carcinoma
and expression of gross cystic disease fluid protein 15 and
mammaglobin. Am J Clin Pathol. 135:587–591. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tafreshi NK, Enkemann SA, Bui MM, et al: A
mammaglobin-A targeting agent for noninvasive detection of breast
cancer metastasis in lymph nodes. Cancer Res. 71:1050–1059. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Serra C, Vizoso F, Alonso L, et al:
Expression and prognostic significance of lysozyme in male breast
cancer. Breast Cancer Res. 4:R162002. View
Article : Google Scholar : PubMed/NCBI
|