Introduction
Primary osteosarcoma of the breast is a rare tumor,
which is indistinguishable from conventional osteosarcoma of the
bone and other extraskeletal sites using histological examination
(1–6). In comparison, bone-producing spindle
cell neoplasms with an epithelial origin, known as metaplastic
(sarcomatoid) carcinomas, and malignant phyllodes tumors are more
common (7). Primary breast
osteosarcomas are considered to be highly aggressive tumors that
are associated with early recurrence and a tendency for
hematogenous, instead of lymphatic, spread, most commonly to the
lungs (2,3,6,8–11).
The tumor subtype, size and mitotic figures may be predictors of
prognosis. The present study describes a case of a
chondroblastic/fibroblastic variant of this rare tumor that had a
good prognosis.
Case report
A 77-year-old Chinese woman presented to the Chengde
Central Hospital Outpatient Department with complaints of a lump in
the left breast that was self-detected a month prior to
presentation. There was no history of nipple discharge, fever and
pain. There was no history of breast trauma, prior local
irradiation and surgery, nor any other tumor history. The patient
denied using any hormonal therapy or a family history of breast
disease. A breast examination showed a 7×7×6-cm irregular, firm
mass in the lower inner quadrant of the left breast. The mass was
poorly mobile and adherent to the skin and chest wall. No axillary
lymphadenopathy was detected upon physical examination. Mammography
showed that the mass was relatively well demarcated and partially
calcified. The tumor did not invade the overlying skin and
underlying chest wall. Breast carcinoma was thus indicated. The
patient refused a needle biopsy and underwent a mastectomy.
The mastectomy specimen contained a 7-cm, relatively
well-circumscribed mass, which had a gray-white cartilaginous to
firm calcified appearance in the cross-section.
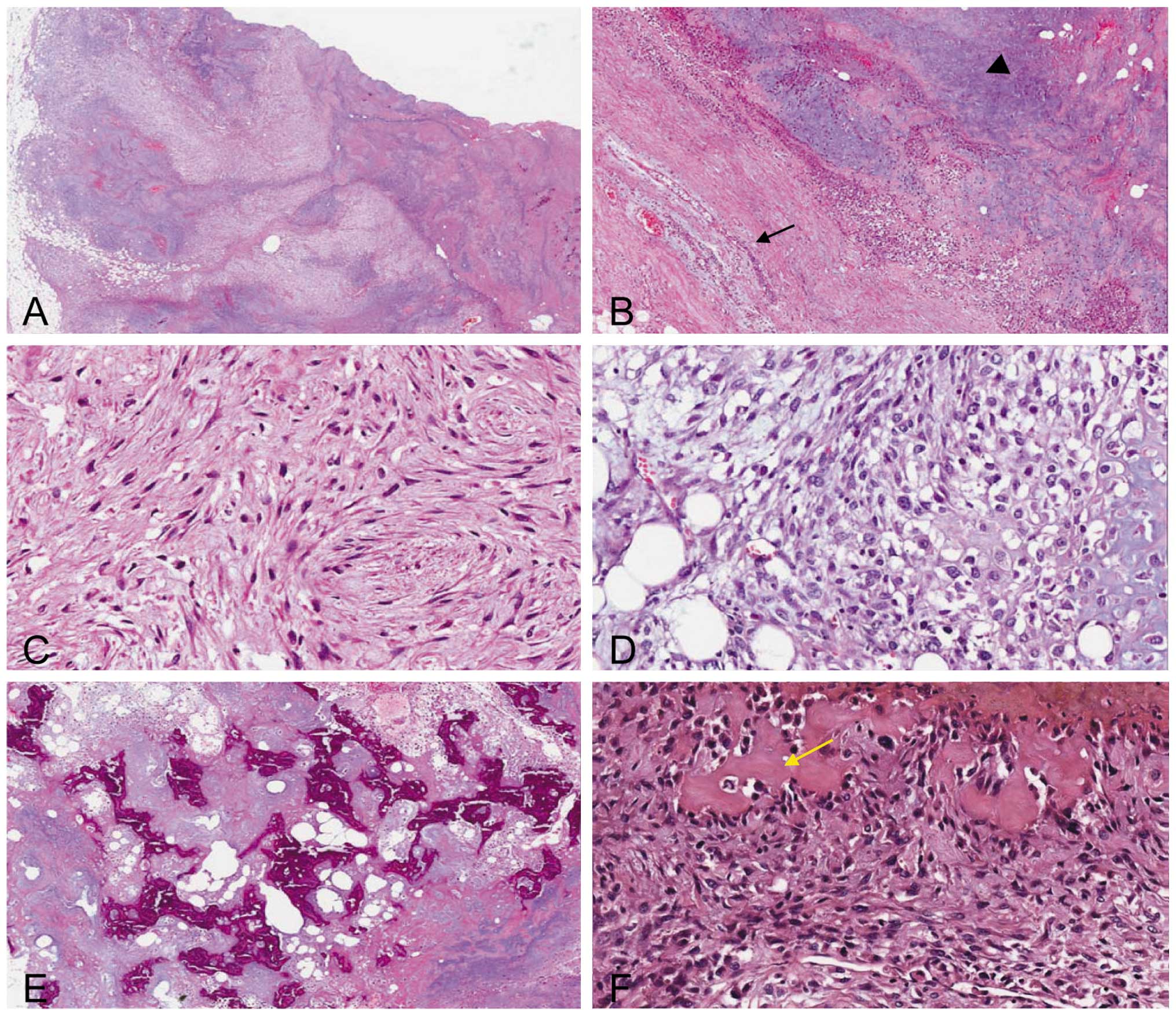
Microscopically, the tumor was slightly lobular and
relatively well demarcated, however, the adjacent fat tissue had
been invaded and the surrounding non-neoplastic breast parenchyma
revealed compressed lobular units (Fig.
1A and B). The tumor was mainly composed of cartilaginous
components. The abundant cartilaginous proliferation varied from
mature lacunar cartilage to poorly-differentiated areas displaying
myxoid changes with no lacunar arrangement. In certain areas there
was a transition from cartilaginous proliferation to fibrous cells.
More than half of the tumor cells (~60%) were spindle-like and
sparse with minimal cytological atypia, which were mainly observed
in the central portion, while the other cells (40%), which were
mainly in the periphery, were epithelioid, atypical and dense.
High-power magnification revealed low mitotic activity even in the
dense area (1 mitoses/10 high power microscopic fields; Fig. 1C and D). Neoplastic osteoid woven
bone or trabeculae were observed in the central portion (Fig. 1E and F). Hemorrhage and necrosis
foci were also observed in the central portion. No lymph-vascular
invasion or neural invasion was observed. There was no histological
evidence of an epithelial or carcinomatous component, despite
extensive sampling of the tumor. No evidence of a preexisting
malignant phyllodes tumor was present. The tumor was negative for
cytokeratin, as well as for the estrogen and progesterone receptors
and HER2. The tumor was classified as a chondroblastic/fibroblastic
variant of osteosarcoma. The 15 axillary lymph nodes studied showed
no metastasis. The patient underwent a simple mastectomy without
post-operative adjuvant chemotherapy or radiation therapy. At 60
months post-mastectomy, the patient was alive and well without
clinical evidence of local recurrence or distant metastasis.
Written informed consent was obtained from the patient for
publication of this case report and all accompanying images.
Discussion
Carcinoma is the most common malignancy of the
breast and sarcomas form a minority of breast neoplasms. Primary
osteosarcoma of the breast is rare and represents <1% of all
primary breast malignancies. However, the actual incidence of
primary osteosarcoma is difficult to determine, as a number of the
~100 previously-reported cases are likely to have included
metaplastic carcinomas, as well as osteogenic sarcomas arising in
association with a biphasic tumor, such as a phyllodes tumor or
carcinosarcoma (7). Almost every
previous reference to primary osteosarcoma of the breast in the
literature is in the form of single case reports. Silver and
Tavassoli reported a clinicopathological analysis of 50 cases
observed over a 38-year period, the largest collection of primary
breast osteogenic sarcomas to date (6). In almost all cases, the patients were
diagnosed clinically as having breast carcinoma and the final
diagnosis was established by histology. The histogenesis of primary
osteosarcoma of the breast remains unclear, but an origin from
totipotent mesenchymal cells of the breast stroma or a
transformation from a preexisting fibroadenoma or phyllodes tumor
has been suggested (1).
The presentation of breast osteosarcoma usually
occurs at an advanced age, in contrast with skeletal osteosarcomas
where the patients are younger. There has been a report of a breast
osteosarcoma diagnosis at the age of 96 years, however, the usual
mean age at presentation has been reported to be ~64 years, and
cases are more frequently postmenopausal (1,6). Risk
factors for extraskeletal osteosarcomas have not been identified to
date, although certain cases have been attributed to local
irradiation, trauma or the presence of a foreign body (6). The majority of patients present with a
mobile, often large, irregular lump, without axillary metastases.
Primary osteosarcomas should be separated from malignant phyllodes
tumors with malignant heterologous differentiation. Other diagnoses
that should be excluded are: i) osteosarcomatous differentiation in
carcinoma of the breast (metaplastic carcinoma), which are likely
to be myoepithelial differentiation; ii) osteogenic sarcoma arising
from the underlying ribs or sternum; and iii) metastatic
osteosarcoma. The present patient was 77 years old with no history
of trauma or irradiation, no tumor in other sites and absence of a
biphasic image in the breast. Other diagnoses were therefore
excluded, and it was concluded that the patient had primary
osteosarcoma of the breast.
The reverse zonation pattern is observed in half of
all breast osteosarcomas (the majority of fibroblastic types)
(6). In the zonation pattern, the
bone tissue at the peripheral region is more mature than that in
the central region, which is generally the phenomenon observed in
myositis ossificans. In the reverse zonation pattern, the central
portion of the tumor was largely composed of neoplastic osteoid
woven bone or trabeculae, with sarcomatous stroma confined to the
periphery of the neoplasm, imparting a zonal pattern (the reverse
of that observed in myositis ossificans). A reverse zonation
pattern was observed in the present case. In addition, central
necrosis has been noted in 10% of all breast osteosarcomas.
Generally, central necrosis is observed in large tumors, such as
tumors with surface ulceration (6).
Areas of necrosis were identified in the center of the tumor in the
present case.
Primary breast osteosarcomas are considered to be
highly aggressive tumors associated with early recurrence and a
tendency for hematogenous, instead of lymphatic, spread, most
commonly to the lungs (2,3,6,8–11).
It has been reported that the predictive factors for
outcome in this disease are tumor size, histological grade and
subtype. Silver and Tavassoli (6)
observed that mammary osteosarcomas that were on average 4.6 cm in
diameter were associated with a significantly higher survival rate
than larger tumors. Histological differentiation is important since
fibroblastic osteosarcomas have a improved survival outcome
compared with other pathological types, in breast osteosarcomas as
well as in primary bone and soft tissue osteosarcomas. The
histological appearance of primary osteosarcoma of the breast
varies according to the cellular composition (fibroblastic,
osteoblastic and osteoclastic), as well as the type and amount of
the matrix (osteoid, osseous and chondroid). Abundant
chondrosarcomatous components are rarely observed (6,12).
Silver and Tavassoli (6) classified
primary osteosarcoma of the breast into the fibroblastic,
osteoblastic and osteoclastic types. The osteoclastic type is not
in the current World Health Organization (WHO) classification of
osteosarcomas (13). Silver and
Tavassoli (6) report that this
subtype contains abundant, multi-nucleated osteoclast giant cells
diffusely scattered within the sarcomatous stroma or surrounding
osteoid islands. The fibroblastic type constituted the majority of
cases (56%) in their study, while the osteoblastic type was the
smallest subtype (16%). Patients with osteosarcoma of the
fibroblastic subtype have a significantly improved 5-year survival
rate (67%) than those with osteosarcoma of the osteoclastic or
osteoblastic subtype (31%). Mitotic activity in osteosarcoma of the
breast ranges between 5 and >20 mitotic figures/10 high-power
fields. The osteosarcoma of the breast that has a high mitotic rate
is limited to the osteoblastic and osteoclastic variants. This may
be the reason for the different survival rates among subtypes. The
present tumor was classified into the chondroblastic/fibroblastic
variant, and the mitotic activity of this tumor was low. The
reasons for the lack of recurrence in the 5 years subsequent to the
surgery may be related to the subtype, minimal cytological atypia,
low mitotic rate and good local control due to adequate resection,
even though the tumor size was 7 cm.
Treatment for localized disease should include
complete surgical removal of the tumor with an adequate margin. A
simple mastectomy may be indicated to ensure complete excision of
large tumors with cryptically infiltrative margins. Axillary lymph
node dissection is not indicated in the setting of
clinically-negative nodes, as axillary node involvement is rare.
Whereas, for metastatic disease, chemotherapy based on the classic
drugs (doxorubicine, ifosfamide, cisplatinium and methotrexate)
used for osteosarcoma is the main treatment. Distinguishing
metaplastic carcinoma and carcinosarcoma from osteosarcoma of the
breast is important, since the former requires treatment as a
primary breast cancer.
The majority of reported primary breast
osteosarcomas are considered highly aggressive tumors associated
with early recurrence and a propensity for hematogenous spread.
However, the presence of a chondroblastic/fibroblastic variant,
minimal cytological atypia, a low mitotic rate and good local
control due to adequate resection may result in a good
prognosis.
References
|
1
|
Bahrami A, Resetkova E, Ro JY, Ibanez JD
and Ayala AG: Primary osteosarcoma of the breast: report of 2
cases. Arch Pathol Lab Med. 131:792–795. 2007.PubMed/NCBI
|
|
2
|
Gull S, Patil P and Spence RA: Primary
osteosarcoma of breast. BMJ Case Rep. Aug 11–2011. View Article : Google Scholar
|
|
3
|
Middela S, Jones M and Maxwell W: Primary
osteosarcoma of the breast - a case report and review of
literature. Indian J Surg. 73:363–365. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Murakami S, Isozaki H, Shou T, et al:
Primary osteosarcoma of the breast. Pathol Int. 59:111–115. 2009.
View Article : Google Scholar
|
|
5
|
Nugent E, Wang LM, McCormack O, Jeffers M,
Rothwell J and Geraghty J: Pure primary osteosarcoma of the breast.
Breast J. 17:425–426. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Silver SA and Tavassoli FA: Primary
osteogenic sarcoma of the breast: a clinicopathologic analysis of
50 cases. Am J Surg Pathol. 22:925–933. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rakha EA, Tan PH, Shaaban A, et al: Do
primary mammary osteosarcoma and chondrosarcoma exist? A review of
a large multi-institutional series of malignant matrix-producing
breast tumours. Breast. 22:13–18. 2013. View Article : Google Scholar
|
|
8
|
Lee S, Lee MR, Lee SJ, et al: Extraosseous
osteosarcoma: single institutional experience in Korea. Asia Pac J
Clin Oncol. 6:126–129. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Saber B, Nawal A, Mohamed F and Hassan E:
Primary osteosarcoma of the breast: case report. Cases J. 1:802008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Vanhoeij M, Bourgain C and Lamote J:
Primary osteogenic sarcoma of the breast: a rare and fatal case.
Breast J. 17:97–99. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Watt AC, Haggar AM and Krasicky GA:
Extraosseous osteogenic sarcoma of the breast: mammographic and
pathologic findings. Radiology. 150:341984. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Olinici CD, Crisan D and Resiga L: Primary
chondroblastic osteosarcoma of the breast. Case report and review
of the literature. Rom J Morphol Embryol. 47:291–293.
2006.PubMed/NCBI
|
|
13
|
Fletcher CDM, Unni KK and Mertens F:
Conventional osteosarcoma. World Health Organization of Tumors.
Pathology and Genetics of Tumors of Soft Tissue and Bone. IARC
Press; Lyon: pp. 264–270. 2002
|